
Diagnostic Concordance between the Visual Analogue Anxiety Scale (VAS-A) and the State-Trait Anxiety Inventory (STAI) in Nursing Students during the COVID-19 Pandemic

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Measuring Instruments
2.3. Data Collection and Ethical Considerations
2.4. Data Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
6. Implications for Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, A.H.; Lee, C.T.; Espin, S. Undergraduate nursing students’ experiences of anxiety-producing situations in clinical practicums: A descriptive survey study. Nurse Educ. Today 2019, 76, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Wang, G.; Xie, C.; Hu, X.; Reinhardt, J.D. Prevalence and correlates of depression, anxiety and symptoms of stress in vocational college nursing students from Sichuan, China: A cross-sectional study. Psychol. Health Med. 2019, 24, 798–811. [Google Scholar] [CrossRef] [PubMed]
- Simpson, M.C.G.; Sawatzky, J.A.V. Clinical placement anxiety in undergraduate nursing students: A concept analysis. Nurse Educ. Today 2020, 87, 104329. [Google Scholar] [CrossRef] [PubMed]
- Wedgeworth, M. Anxiety and education: An examination of anxiety across a nursing program. J. Nurs. Educ. Pract. 2016, 6, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, A.L. Test anxiety among nursing students: A systematic review. Teach. Learn. Nurs. 2014, 9, 193–202. [Google Scholar] [CrossRef]
- Chernomas, W.M.; Shapiro, C. Stress, depression, & anxiety among undergraduate nursing students. Int. J. Nurs. Educ. Scholarsh. 2013, 10, 255–266. [Google Scholar]
- Pires Camargo, C.; Zen Tempski, P.; Freitas Busnardo, F.; Martins, M.D.A.; Gemperli, R. Online learning and COVID-19, a meta-synthesis analysis. Clinics 2020, 75, e2286. [Google Scholar] [CrossRef]
- Li, D.; Zou, L.; Zhang, Z.; Zhang, P.; Zhang, J.; Fu, W.; Mao, J.; Cao, S. The Psychological Effect of COVID-19 on Home-Quarantined Nursing Students in China. Front. Psychiatry 2021, 12, 652296. [Google Scholar] [CrossRef]
- Reverté-Villarroya, S.; Ortega, L.; Lavedán, A.; Masot, O.; Burjalés-Martí, M.D.; Ballester-Ferrando, D.; Fuentes-Pumarola, C.; Botigué, T. The influence of COVID-19 on the mental health of final-year nursing students: Comparing the situation before and during the pandemic. Int. J. Ment. Health Nurs. 2021, 30, 694–702. [Google Scholar] [CrossRef]
- Carolan, C.; Davies, C.L.; Crookes, P.; McGhee, S.; Roxburgh, M. COVID 19, Disruptive impacts and transformative opportunities in undergraduate nurse education. Nurse Educ. Pract. 2020, 46, 102807. [Google Scholar] [CrossRef]
- Suliman, W.A.; Abu-Moghli, F.A.; Khalaf, I.; Zumot, A.F.; Nabolsi, M. Experiences of nursing students under the unprecedented abrupt online learning format forced by the national curfew due to COVID-19, A qualitative research study. Nurse Educ. Today 2021, 100, 104829. [Google Scholar] [CrossRef] [PubMed]
- Haslam, M.B. What might COVID-19 have taught us about the delivery of Nurse Education, in a post-COVID-19 world? Nurse Educ. Today 2021, 97, 104707. [Google Scholar] [CrossRef] [PubMed]
- Canet-Vélez, O.; Botigué, T.; Lavedán Santamaría, A.; Masot, O.; Cemeli, T.; Roca, J. The perception of training and professional development according to nursing students as health workers during COVID-19, A qualitative study. Nurse Educ. Pract. 2021, 53, 103072. [Google Scholar] [CrossRef]
- Casafont, C.; Fabrellas, N.; Rivera, P.; Olivé-Ferrer, M.C.; Querol, E.; Venturas, M.; Prats, J.; Cuzco, C.; Frías, C.E.; Pérez-Ortega, S.; et al. Experiences of nursing students as healthcare aid during the COVID-19 pandemic in Spain: A phemonenological research study. Nurse Educ. Today 2021, 97, 104711. [Google Scholar] [CrossRef]
- De Almeida Peres, M.A.; Brandão, M.A.G.; De Sousa Aperibense, P.G.G.; Lacerda, A.C.D.; Paim, L.; Ferreira, M.D.A. Facing up COVID-19, What cannot be relativized in nursing higher education. Texto Context Enferm. 2020, 29, 1–13. [Google Scholar]
- Jimenez, C.; Navia-Osorio, P.M.; Diaz, C.V. Stress and health in novice and experienced nursing students. J. Adv. Nurs. 2010, 66, 442–455. [Google Scholar] [CrossRef] [PubMed]
- Fowler, K.; Wholeben, M. COVID-19, Outcomes for trauma-impacted nurses and nursing students. Nurse Educ. Today 2020, 93, 104525. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. Manual Cuestionario de Ansiedad Estado-Rasgo Adaptación Española; TEA Ediciones: Madrid, Spain, 2015; Volume 9. [Google Scholar]
- Spielberger, C.; Gorsuch, R.; Lushene, R.E.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory (Form Y1-Y2), 1st ed.; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Fernández-Blázquez, M.A.; Ávila-Villanueva, M.; López-Pina, J.A.; Zea-Sevilla, M.A.; Frades-Payo, B. Psychometric properties of a new short version of the State-Trait Anxiety Inventory (STAI) for the assessment of anxiety in the elderly. Neurologia 2015, 30, 352–358. [Google Scholar] [CrossRef]
- Singh, C.; Jackson, D.; Munro, I.; Cross, W. Work experiences of Nurse Academics: A qualitative study. Nurse Educ. Today 2021, 106, 105038. [Google Scholar] [CrossRef]
- Zsido, A.N.; Teleki, S.A.; Csokasi, K.; Rozsa, S.; Bandi, S.A. Development of the short version of the Spielberger state—Trait anxiety inventory. Psychiatry Res. 2020, 291, 113223. [Google Scholar] [CrossRef]
- Klimek, L.; Bergmann, K.C.; Biedermann, T.; Bousquet, J.; Hellings, P.; Jung, K.; Merk, H.; Olze, H.; Schlenter, W.; Stock, P.; et al. Visual analogue scales (VAS)—Measuring instruments for the documentation of symptoms and therapy monitoring in case of allergic rhinitis in everyday health care. Allergo J. 2017, 26, 36–47. [Google Scholar] [CrossRef]
- Bernstein, G.A.; Garfinkel, B.D. The Visual Analogue Scale for Anxiety—Revised: Psychometric properties. J. Anxiety Disord. 1992, 6, 223–239. [Google Scholar] [CrossRef]
- Boonstra, A.M.; Schiphorst Preuper, H.R.; Balk, G.A.; Stewart, R.E. Cut-off points for mild, moderate, and severe pain on the visual analogue scale for pain in patients with chronic musculoskeletal pain. Pain 2014, 155, 2545–2550. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Pedrero, E.; Paino, M.; Sierra-Baigrie, S.; Lemos-Giráldez, S.; Muñiz, J. Propiedades psicométricas del ‘Cuestionario de ansiedad estado-rasgo’ (STAI) en universitarios. Behav. Psychol. Psicol. Conduct. 2012, 20, 547–561. [Google Scholar]
- Guillén Riquelme, A.; Buela Casal, G. Validación de la Adaptación Española del State-Trait Anxiety Inventory en Diferentes Muestras Españolas; Universidad de Granada: Granada, Spain, 2014. [Google Scholar]
- Villeneuve, P.; Heale, R.; Rietze, L.; Carter, L. Exploring self-perceptions of anxiety among nursing students in the clinical setting and select demographics. Int. J. Nurs. Educ. Scholarsh. 2018, 15, 20170042. [Google Scholar] [CrossRef] [PubMed]
- Gebhart, V.; Buchberger, W.; Klotz, I.; Neururer, S.; Rungg, C.; Tucek, G.; Zenzmaier, C.; Perkhofer, S. Distraction-focused interventions on examination stress in nursing students: Effects on psychological stress and biomarker levels. A randomized controlled trial. Int. J. Nurs. Pract. 2020, 26, e12788. [Google Scholar] [CrossRef]
- Onieva-Zafra, M.D.; Fernández-Muñoz, J.J.; Fernández-Martínez, E.; García-Sánchez, F.J.; Abreu-Sánchez, A.; Parra-Fernández, M.L. Anxiety, Perceived Stress and Coping Strategies in Nursing Students: A Cross-Sectional Correlational Descriptive Study. BMC Med. Educ. 2020, 20, 370. [Google Scholar] [CrossRef]
- Rice, M.E.; Harris, G.T. Comparing effect sizes in follow-up studies: ROC area, Cohen’s d, and r. Law Hum. Behav. 2005, 29, 615–620. [Google Scholar] [CrossRef]
- Lesage, F.-X.; Berjot, S.; Deschamps, F. Clinical stress assessment using a visual analogue scale. Occup. Med. 2012, 62, 600–605. [Google Scholar] [CrossRef] [Green Version]
- Labaste, F.; Ferré, F.; Combelles, H.; Rey, V.; Foissac, J.C.; Senechal, A.; Conil, J.M.; Minville, V. Validation of a visual analogue scale for the evaluation of the postoperative anxiety: A prospective observational study. Nurs. Open 2019, 6, 1323–1330. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Palazón, J.; Fuentes-García, D.; Falcón-Araña, L.; Roca-Calvo, M.J.; Burguillos-López, S.; Doménech-Asensi, P.; Jara-Rubio, R. Assessment of Preoperative Anxiety in Cardiac Surgery Patients Lacking a History of Anxiety: Contributing Factors and Postoperative Morbidity. J. Cardiothorac. Vasc. Anesth. 2018, 32, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Abend, R.; Dan, O.; Maoz, K.; Raz, S.; Bar-Haim, Y. Reliability, validity and sensitivity of a computerized visual analog scale measuring state anxiety. J. Behav. Ther. Exp. Psychiatry 2014, 45, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Marshall, A.L.; Wolanskyj-Spinner, A. COVID-19, Challenges and Opportunities for Educators and Generation Z Learners. Mayo Clin. Proc. 2020, 95, 1135–1137. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | n | % | |
|---|---|---|---|
| Age * | 21.3 | 4.0 | |
| Sex | Men | 22 | 11.9 |
| Women | 163 | 88.1 | |
| Nursing degree year | 1st | 48 | 26.0 |
| 2nd | 40 | 21,6 | |
| 3rd | 45 | 24.3 | |
| 4th | 52 | 28.1 | |
| Health worker | No | 126 | 68.1 |
| Yes | 59 | 31.9 | |
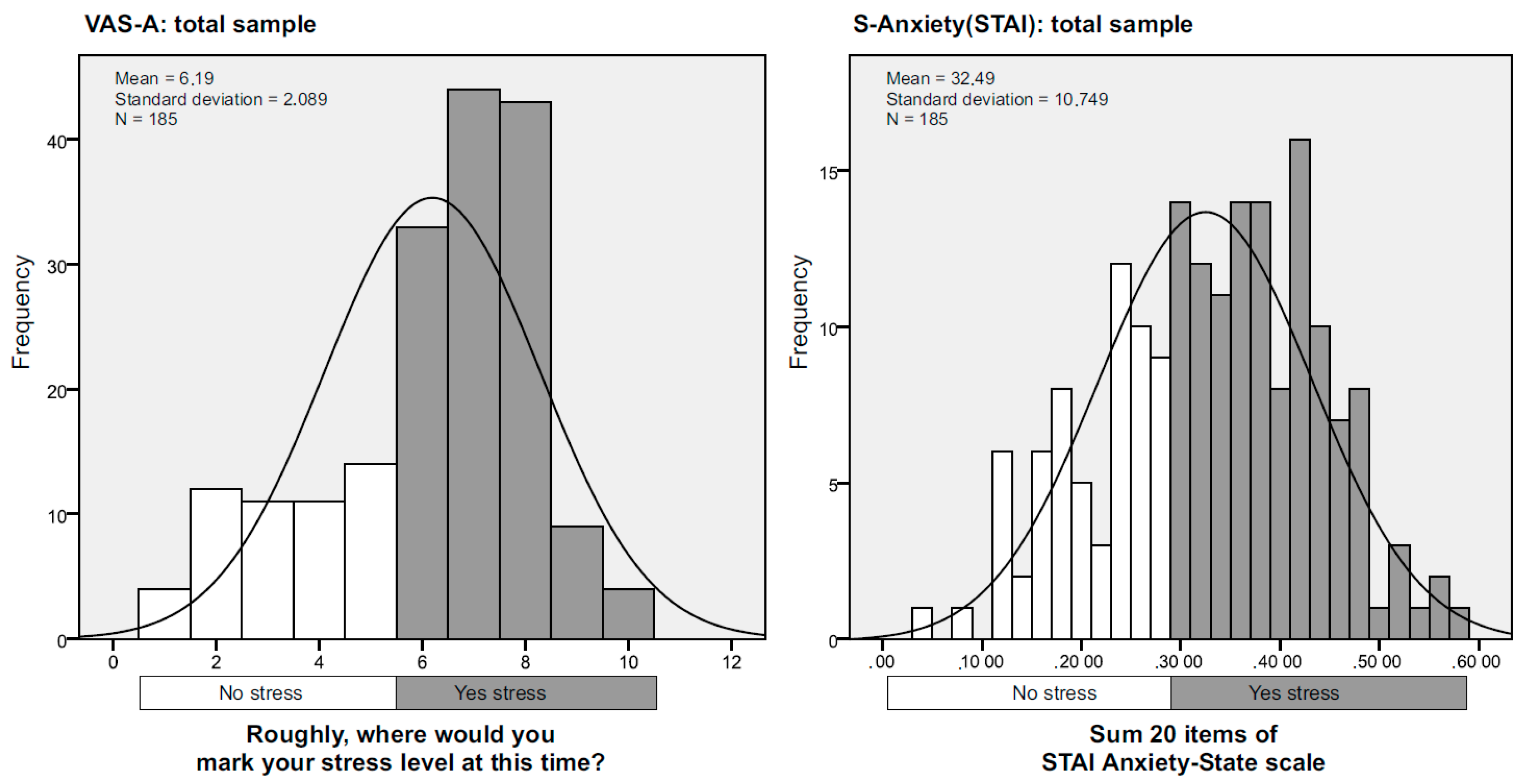
| Level of anxiety (VAS) * | 6.19 | 2.09 | |
| Level of anxiety (STAI) * | 58.43 | 18.81 | |
| S-Anxiety (STAI) * | 32.49 | 10.75 | |
| T-Anxiety (STAI) * | 25.94 | 9.97 | |
| VAS-A | S-Anxiety (STAI) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Factors | No | Yes | p | g | No | Yes | p | g | |||||
| n | % | n | % | n | % | n | % | ||||||
| Age * | 21.9 | 4.4 | 21 | 3.8 | 0.170 | 0.23 | 21.5 | 3.3 | 21.4 | 4.3 | 0.555 | 0.09 | |
| Sex ** | Man | 9 | 17.3 | 13 | 9.8 | 0.155 | 0.23 | 11 | 16.9 | 11 | 9.2 | 0.120 | 0.12 |
| Woman | 43 | 82.7 | 120 | 90.2 | 54 | 83.1 | 109 | 90.8 | |||||
| Nursing degree year ** | 1st and 2nd | 16 | 30.8 | 84 | 63.2 | 0.000 | 0.68 | 28 | 43.1 | 72 | 60 | 0.027 | 0.07 |
| 3rd and 4th | 36 | 69.2 | 49 | 36.8 | 37 | 56.9 | 48 | 40 | |||||
| Health worker ** | No | 36 | 69.2 | 90 | 67.7 | 0.838 | 0.03 | 44 | 67.7 | 82 | 68.3 | 0.929 | 0.02 |
| Yes | 16 | 30.8 | 43 | 32.3 | 21 | 32.3 | 38 | 31.7 | |||||
| Anxiety (VAS-A) | S-Anxiety (STAI) | T-Anxiety (STAI) | |
|---|---|---|---|
| VAS-A | 1 | 0.686 * | 0.417 * |
| S-anxiety (STAI) | 0.686 * | 1 | 0.648 * |
| T-anxiety (STAI) | 0.417 * | 0.648 * | 1 |
| S-Anxiety (STAI) > 30 | |||||
|---|---|---|---|---|---|
| No | Yes | n | % | ||
| VAS-A > 6 | No | 38 | 14 | 52 | 28.1 |
| Yes | 32 | 101 | 133 | 71.9 | |
| n | 70 | 115 | 185 | 100 | |
| % | 37.8 | 62.2 | 100 | ||
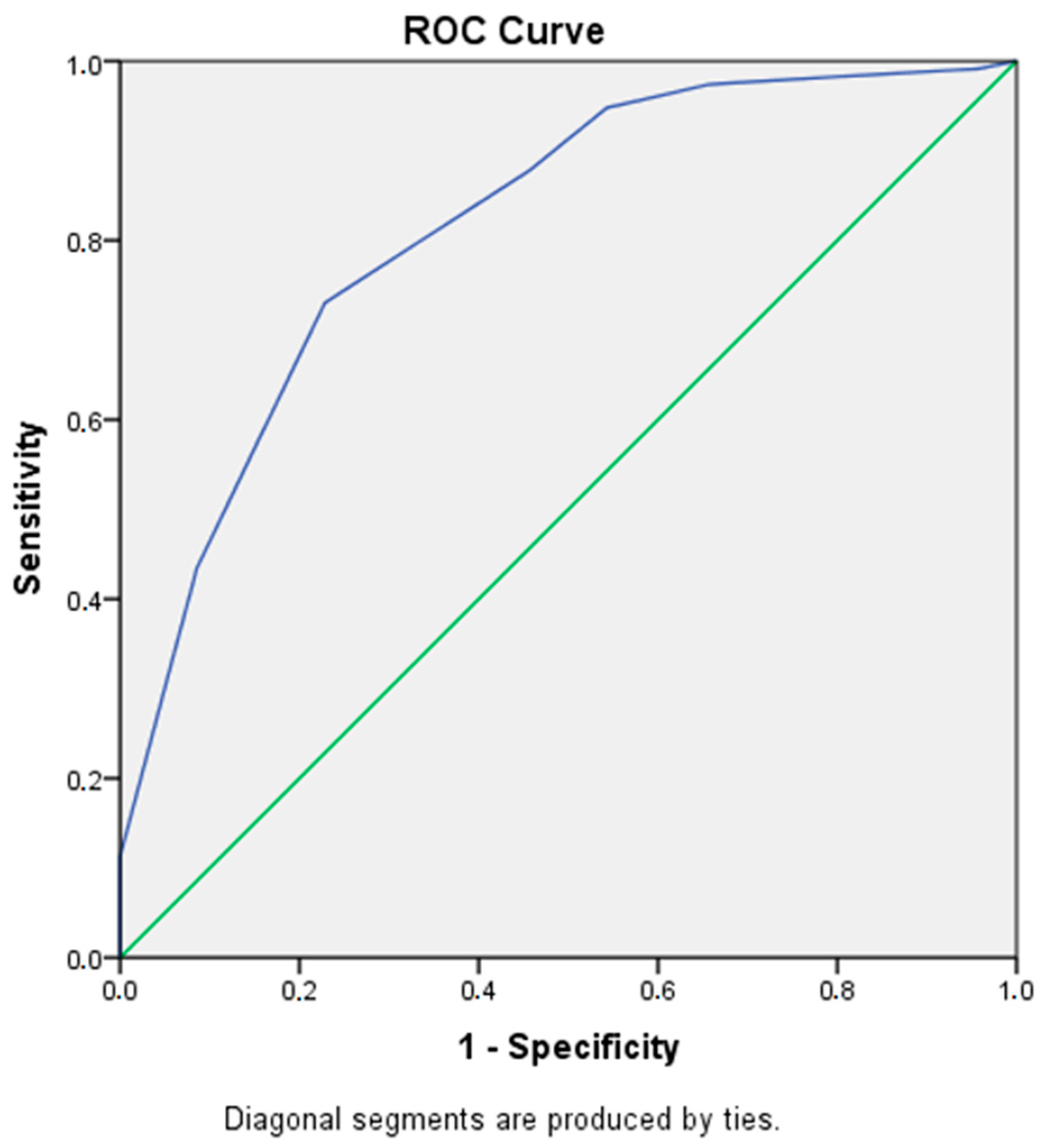
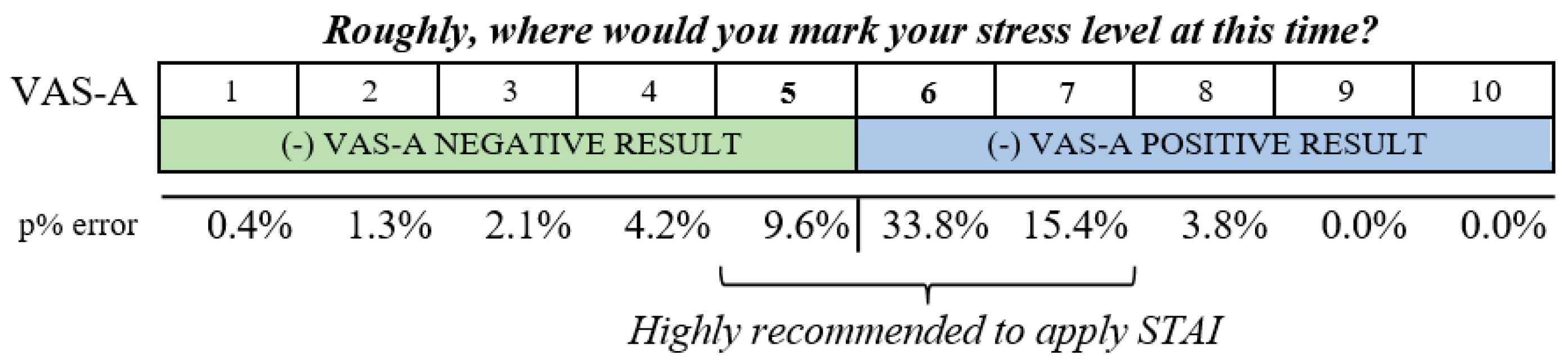
| VAS-A | Sensitivity | 1—Specificity | Probability % of Error | ||
|---|---|---|---|---|---|
| VAS-A (−) NEGATIVES | 1 | 0.991 | 0.957 | 0.4% | of false negatives (1—Sensitivity) |
| 2 | 0.983 | 0.800 | 1.3% | of false negatives (1—Sensitivity) | |
| 3 | 0.974 | 0.657 | 2.1% | of false negatives (1—Sensitivity) | |
| 4 | 0.948 | 0.543 | 4.2% | of false negatives (1—Sensitivity) | |
| 5 | 0.878 | 0.457 | 9.6% | of false negatives (1—Sensitivity) | |
| VAS-A (+) POSITIVES | 6 | 0.730 | 0.229 | 33.8% | of false positives (1—Specificity) |
| 7 | 0.435 | 0.086 | 15.4% | of false positives (1—Specificity) | |
| 8 | 0.113 | 0.000 | 3.8% | of false positives (1—Specificity) | |
| 9 | 0.035 | 0.000 | 0.0% | of false positives (1—Specificity) | |
| 10 | 0.000 | 0.000 | 0.0% | of false positives (1—Specificity) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lavedán Santamaría, A.; Masot, O.; Canet Velez, O.; Botigué, T.; Cemeli Sánchez, T.; Roca, J. Diagnostic Concordance between the Visual Analogue Anxiety Scale (VAS-A) and the State-Trait Anxiety Inventory (STAI) in Nursing Students during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 7053. https://doi.org/10.3390/ijerph19127053
Lavedán Santamaría A, Masot O, Canet Velez O, Botigué T, Cemeli Sánchez T, Roca J. Diagnostic Concordance between the Visual Analogue Anxiety Scale (VAS-A) and the State-Trait Anxiety Inventory (STAI) in Nursing Students during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(12):7053. https://doi.org/10.3390/ijerph19127053
Chicago/Turabian StyleLavedán Santamaría, Ana, Olga Masot, Olga Canet Velez, Teresa Botigué, Tània Cemeli Sánchez, and Judith Roca. 2022. "Diagnostic Concordance between the Visual Analogue Anxiety Scale (VAS-A) and the State-Trait Anxiety Inventory (STAI) in Nursing Students during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 12: 7053. https://doi.org/10.3390/ijerph19127053