
Relation between Vitamin D and COVID-19 in Aged People: A Systematic Review

 , , ,
, , ,
Abstract
:1. Introduction
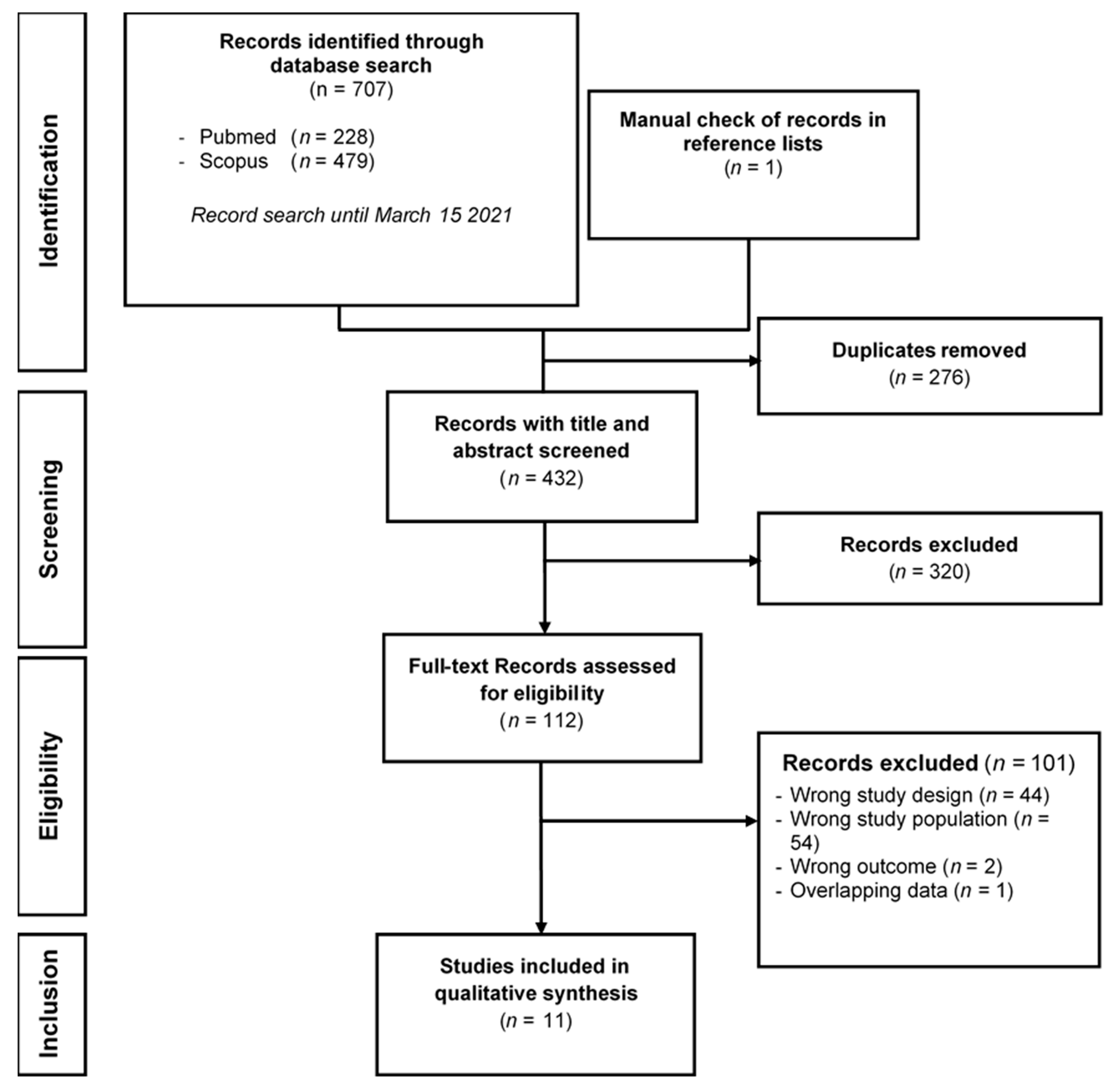
2. Methods
2.1. Search Strategy
2.2. Study Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Author, Year | N | Vitamin D Group Cut-Offs | ||
|---|---|---|---|---|
| Insufficiency | Deficiency | Severe Deficiency | ||
| Baktash V, 2020 [19] | 105 | Not defined | ≤30 nmol/L (≤12 ng/mL) | Not defined |
| Carpagnano GE, 2020 [20] | 27 | 20–30 ng/mL (50–75 nmol/L) | 10–20 ng/mL (25–50 nmol/L) | <10 ng/mL (<25 nmol/L) |
| Cereda E, 2020 [21] | 106 | 20–30 ng/mL (50–75 nmol/L) | 10–20 ng/mL (25–50 nmol/L) | <10 ng/mL (<25 nmol/L) |
| Hars M, 2020 [23] | 160 | Not defined | <20 ng/mL (<50 nmol/L) | Not defined |
| Macaya F, 2020 [24] | 55 | Not defined | <20 ng/mL (<50 nmol/L) | Not defined |
| Radujkovic A, 2020 [25] | 185 | 12–20 ng/mL (30–50 nmol/L) | <12 ng/mL (<30 nmol/L) | Not defined |
| Sulli A, 2021 [26] | 130 | 20–30 ng/mL (50–75 nmol/L) | 10–20 ng/mL (25–50 nmol/L) | <10 ng/mL (<25 nmol/L) |
References
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT Findings in Coronavirus Disease-19 (COVID-19): Relationship to Duration of Infection. Radiology 2020, 295, 200463. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet. Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Lian, J.; Jin, X.; Hao, S.; Cai, H.; Zhang, S.; Zheng, L.; Jia, H.; Hu, J.; Gao, J.; Zhang, Y.; et al. Analysis of Epidemiological and Clinical Features in Older Patients With Coronavirus Disease 2019 (COVID-19) Outside Wuhan. Clin. Infect. Dis 2020, 71, 740–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, K.; Chen, Y.; Lin, R.; Han, K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J. Infect. 2020, 80, e14–e18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; He, W.; Yu, X.; Hu, D.; Bao, M.; Liu, H.; Zhou, J.; Jiang, H. Coronavirus disease 2019 in elderly patients: Characteristics and prognostic factors based on 4-week follow-up. J. Infect. 2020, 80, 639–645. [Google Scholar] [CrossRef]
- Liu, F.; Li, L.; Xu, M.; Wu, J.; Luo, D.; Zhu, Y.; Li, B.; Song, X.; Zhou, X. Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. J. Clin. Virol. 2020, 127, 104370. [Google Scholar] [CrossRef]
- Silberstein, M. Correlation between premorbid IL-6 levels and COVID-19 mortality: Potential role for Vitamin D. Int. Immunopharmacol. 2020, 88. [Google Scholar] [CrossRef]
- Ye, Q.; Wang, B.; Mao, J. The pathogenesis and treatment of the ‘Cytokine Storm’ in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Fiorino, S.; Gallo, C.; Zippi, M.; Sabbatani, S.; Manfredi, R.; Moretti, R.; Fogacci, E.; Maggioli, C.; Travasoni Loffredo, F.; Giampieri, E.; et al. Cytokine storm in aged people with CoV-2: Possible role of vitamins as therapy or preventive strategy. Aging Clin. Exp. Res. 2020, 32, 2115–2131. [Google Scholar] [CrossRef] [PubMed]
- Daneshkhah, A.; Agrawal, V.; Eshein, A.; Subramanian, H.; Roy, H.K.; Backman, V. Evidence for possible association of vitamin D status with cytokine storm and unregulated inflammation in COVID-19 patients. Aging Clin. Exp. Res. 2020, 32, 2141–2158. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B.; Giovannucci, E. The possible roles of solar ultraviolet-B radiation and vitamin D in reducing case-fatality rates from the 1918-1919 influenza pandemic in the United States. Dermatoendocrinol 2009, 1, 215–219. [Google Scholar] [CrossRef]
- Mamani, M.; Muceli, N.; Ghasemi Basir, H.R.; Vasheghani, M.; Poorolajal, J. Association between serum concentration of 25-hydroxyvitamin D and community-acquired pneumonia: A case-control study. Int. J. Gen. Med. 2017, 10, 423–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 25 November 2020).
- Annweiler, C.; Hanotte, B.; Grandin de l’Eprevier, C.; Sabatier, J.M.; Lafaie, L.; Celarier, T. Vitamin D and survival in COVID-19 patients: A quasi-experimental study. J. Steroid Biochem. Mol. Biol. 2020, 204, 105771. [Google Scholar] [CrossRef]
- Annweiler, G.; Corvaisier, M.; Gautier, J.; Dubee, V.; Legrand, E.; Sacco, G.; Annweiler, C. Vitamin D Supplementation Associated to Better Survival in Hospitalized Frail Elderly COVID-19 Patients: The GERIA-COVID Quasi-Experimental Study. Nutrients 2020. [Google Scholar] [CrossRef] [PubMed]
- Baktash, V.; Hosack, T.; Patel, N.; Shah, S.; Kandiah, P.; Van den Abbeele, K.; Mandal, A.K.J.; Missouris, C.G. Vitamin D status and outcomes for hospitalised older patients with COVID-19. Postgrad Med. J. 2020. [Google Scholar] [CrossRef]
- Carpagnano, G.E.; Di Lecce, V.; Quaranta, V.N.; Zito, A.; Buonamico, E.; Capozza, E.; Palumbo, A.; Di Gioia, G.; Valerio, V.N.; Resta, O. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J. Endocrinol. Investig. 2021, 44, 765–771. [Google Scholar] [CrossRef]
- Cereda, E.; Bogliolo, L.; Klersy, C.; Lobascio, F.; Masi, S.; Crotti, S.; De Stefano, L.; Bruno, R.; Corsico, A.G.; Di Sabatino, A.; et al. Vitamin D 25OH deficiency in COVID-19 patients admitted to a tertiary referral hospital. Clin. Nutr. 2020. [Google Scholar] [CrossRef]
- Giannini, S.; Passeri, G.; Tripepi, G.; Sella, S.; Fusaro, M.; Arcidiacono, G.; Torres, M.O.; Michielin, A.; Prandini, T.; Baffa, V.; et al. Effectiveness of In-Hospital Cholecalciferol Use on Clinical Outcomes in Comorbid COVID-19 Patients: A Hypothesis-Generating Study. Nutrients 2021. [Google Scholar] [CrossRef]
- Hars, M.; Mendes, A.; Serratrice, C.; Herrmann, F.R.; Gold, G.; Graf, C.; Zekry, D.; Trombetti, A. Sex-specific association between vitamin D deficiency and COVID-19 mortality in older patients. Osteoporos. Int. A J. Establ. Result Coop. Eur. Found. Osteoporos. Natl. Osteoporos. Found. USA 2020, 31, 2495–2496. [Google Scholar] [CrossRef]
- Macaya, F.; Espejo Paeres, C.; Valls, A.; Fernandez-Ortiz, A.; Gonzalez Del Castillo, J.; Martin-Sanchez, F.J.; Runkle, I.; Rubio Herrera, M.A. Interaction between age and vitamin D deficiency in severe COVID-19 infection. Nutr. Hosp. 2020, 37, 1039–1042. [Google Scholar] [CrossRef]
- Radujkovic, A.; Hippchen, T.; Tiwari-Heckler, S.; Dreher, S.; Boxberger, M.; Merle, U. Vitamin D Deficiency and Outcome of COVID-19 Patients. Nutrients 2020. [Google Scholar] [CrossRef]
- Sulli, A.; Gotelli, E.; Casabella, A.; Paolino, S.; Pizzorni, C.; Alessandri, E.; Grosso, M.; Ferone, D.; Smith, V.; Cutolo, M. Vitamin D and Lung Outcomes in Elderly COVID-19 Patients. Nutrients 2021. [Google Scholar] [CrossRef]
- Tan, C.W.; Ho, L.P.; Kalimuddin, S.; Cherng, B.P.Z.; Teh, Y.E.; Thien, S.Y.; Wong, H.M.; Tern, P.J.W.; Chandran, M.; Chay, J.W.M.; et al. Cohort study to evaluate the effect of vitamin D, magnesium, and vitamin B12 in combination on progression to severe outcomes in older patients with coronavirus (COVID-19). Nutrition 2020, 79–80, 111017. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, D.O.; Best, T.J.; Zhang, H.; Vokes, T.; Arora, V.; Solway, J. Association of Vitamin D Status and Other Clinical Characteristics With COVID-19 Test Results. JAMA Netw. Open 2020, 3, e2019722. [Google Scholar] [CrossRef] [PubMed]
- Im, J.H.; Je, Y.S.; Baek, J.; Chung, M.H.; Kwon, H.Y.; Lee, J.S. Nutritional status of patients with COVID-19. Int. J. Infect. Dis. 2020, 100, 390–393. [Google Scholar] [CrossRef]
- Manios, Y.; Moschonis, G.; Lambrinou, C.P.; Tsoutsoulopoulou, K.; Binou, P.; Karachaliou, A.; Breidenassel, C.; Gonzalez-Gross, M.; Kiely, M.; Cashman, K.D. A systematic review of vitamin D status in southern European countries. Eur. J. Nutr. 2018, 57, 2001–2036. [Google Scholar] [CrossRef]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenner, H.; Holleczek, B.; Schottker, B. Vitamin D Insufficiency and Deficiency and Mortality from Respiratory Diseases in a Cohort of Older Adults: Potential for Limiting the Death Toll during and beyond the COVID-19 Pandemic? Nutrients 2020. [Google Scholar] [CrossRef]
- Ye, K.; Tang, F.; Liao, X.; Shaw, B.A.; Deng, M.; Huang, G.; Qin, Z.; Peng, X.; Xiao, H.; Chen, C.; et al. Does Serum Vitamin D Level Affect COVID-19 Infection and Its Severity?-A Case-Control Study. J. Am. Coll. Nutr. 2020. [Google Scholar] [CrossRef]
- Maghbooli, Z.; Sahraian, M.A.; Ebrahimi, M.; Pazoki, M.; Kafan, S.; Tabriz, H.M.; Hadadi, A.; Montazeri, M.; Nasiri, M.; Shirvani, A.; et al. Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection. PLoS ONE 2020, 15, e0239799. [Google Scholar] [CrossRef]
- Wang, L.; Amin, A.K.; Khanna, P.; Aali, A.; McGregor, A.; Bassett, P.; Gopal Rao, G. An observational cohort study of bacterial co-infection and implications for empirical antibiotic therapy in patients presenting with COVID-19 to hospitals in North West London. J. Antimicrob. Chemother. 2021, 76, 796–803. [Google Scholar] [CrossRef]
- Haroon, A.; Higa, F.; Fujita, J.; Watanabe, A.; Aoki, N.; Niki, Y.; Kadota, J.; Yanagihara, K.; Kaku, M.; Hori, S.; et al. Pulmonary computed tomography findings in 39 cases of Streptococcus pneumoniae pneumonia. Intern. Med. 2012, 51, 3343–3349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coomes, E.A.; Haghbayan, H. Interleukin-6 in Covid-19: A systematic review and meta-analysis. Rev. Med. Virol. 2020, 30, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Aranow, C. Vitamin D and the immune system. J. Investig. Med. 2011, 59, 881–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greiller, C.L.; Martineau, A.R. Modulation of the immune response to respiratory viruses by vitamin D. Nutrients 2015, 7, 4240–4270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giustina, A.; Adler, R.A.; Binkley, N.; Bollerslev, J.; Bouillon, R.; Dawson-Hughes, B.; Ebeling, P.R.; Feldman, D.; Formenti, A.M.; Lazaretti-Castro, M.; et al. Consensus statement from 2(nd) International Conference on Controversies in Vitamin D. Rev. Endocr. Metab. Disord. 2020, 21, 89–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Entrenas Castillo, M.; Entrenas Costa, L.M.; Vaquero Barrios, J.M.; Alcalá Díaz, J.F.; López Miranda, J.; Bouillon, R.; Quesada Gomez, J.M. “Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study”. J. Steroid Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef] [PubMed]
- Ginde, A.A.; Blatchford, P.; Breese, K.; Zarrabi, L.; Linnebur, S.A.; Wallace, J.I.; Schwartz, R.S. High-Dose Monthly Vitamin D for Prevention of Acute Respiratory Infection in Older Long-Term Care Residents: A Randomized Clinical Trial. J. Am. Geriatr. Soc. 2017, 65, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Cesareo, R.; Attanasio, R.; Caputo, M.; Castello, R.; Chiodini, I.; Falchetti, A.; Guglielmi, R.; Papini, E.; Santonati, A.; Scillitani, A.; et al. Italian Association of Clinical Endocrinologists (AME) and Italian Chapter of the American Association of Clinical Endocrinologists (AACE) Position Statement: Clinical Management of Vitamin D Deficiency in Adults. Nutrients 2018. [Google Scholar] [CrossRef] [Green Version]
- Cereda, E.; Bogliolo, L.; Lobascio, F.; Barichella, M.; Zecchinelli, A.L.; Pezzoli, G.; Caccialanza, R. Vitamin D supplementation and outcomes in coronavirus disease 2019 (COVID-19) patients from the outbreak area of Lombardy, Italy. Nutrition 2021, 82, 111055. [Google Scholar] [CrossRef] [PubMed]
- Ssentongo, P.; Ssentongo, A.E.; Heilbrunn, E.S.; Ba, D.M.; Chinchilli, V.M. Association of cardiovascular disease and 10 other pre-existing comorbidities with COVID-19 mortality: A systematic review and meta-analysis. PLos ONE 2020, 15, e0238215. [Google Scholar] [CrossRef]
- Rosenthal, N.; Cao, Z.; Gundrum, J.; Sianis, J.; Safo, S. Risk Factors Associated With In-Hospital Mortality in a US National Sample of Patients With COVID-19. Jama Netw Open 2020, 3, e2029058. [Google Scholar] [CrossRef] [PubMed]

| Author, Year | Setting | Study Design | N | Female Sex | Age (Years) | COVID-19+ Patients | Comparison |
|---|---|---|---|---|---|---|---|
| Annweiler C, 2020 [17] | NH | Retrospective cohort | 66 | 77.3% | 88 ± 9 * | 100% | Supplementation |
| Annweiler G, 2020 [18] | ACU | Retrospective cohort | 77 | 49.4% | 88 ± 5 * | 100% | Supplementation |
| Giannini S, 2021 [22] | ED | Retrospective cohort | 77 | 49.4% | 78 ± 10 * | 100% | Supplementation |
| Tan CW, 2020 [27] | Hospital | Prospective cohort | 20 | 50.0% | 66 ± 4 * | 100% | Supplementation |
| Baktash V, 2020 [19] | ED | Prospective cohort | 105 | 45.7% | 81 (65–102) † | 67% | Deficiency |
| Carpagnano GE, 2020 [20] | ICU | Retrospective cohort | 27 | 29.6% | 72 ± 9 * | 100% | Deficiency |
| Cereda E, 2020 [21] | Hospital | Prospective cohort | 106 | 49.0% | 78 ± 9 * | 100% | Deficiency |
| Hars M, 2020 [23] | ACU | Retrospective cohort | 160 | 59.4% | 86 ± 7 * | 100% | Deficiency |
| Macaya F, 2020 [24] | ED | Retrospective cohort | 55 | 56.4% | 75 ± 10 * | 100% | Deficiency |
| Radujkovic A, 2020 [25] | ACU and community | Prospective cohort | 185 | 42.3% | 71 ± 8 * | 100% | Deficiency |
| Sulli A, 2021 [26] | Hospital and community | Retrospective case control | 130 | 53.8% | 76 ± 13 * | 50% | Deficiency |
| Author, Year | N | Supplementation | Outcome | Results | Death | |||
|---|---|---|---|---|---|---|---|---|
| Products | Regimen | Primary | Secondary | Primary | Secondary | |||
| Annweiler C, 2020 [17] | 66 | Vitamin D3 | Group 1: oral bolus of 80 kIU in the week following suspicion or diagnosis of COVID-19 | Death during follow-up | Severe COVID-19 (OSCI score ≥5) | Group 1: 17.5% | Group 1: 21.1% | 22.7% |
| Group 2: no supplementation | Group 2: 55.6% | Group 2: 66.7% | ||||||
| Annweiler G, 2020 [18] | 77 | Vitamin D3 | Group 1: oral bolus of 50 kIU per month, or 80 or 100 kIU every 2–3 months over the preceding year | 14-day death | Severe COVID-19 (OSCI score ≥5) | Group 1: 6.9% | Group 1: 10.3% | 19.5% |
| Group 2: single oral bolus of 80 kIU within a few hours after COVID-19 diagnosis | Group 2: 18.8% | Group 2: 25.0% | ||||||
| Group 3: No supplementation | Group 3: 31.3% | Group 3: 31.3% | ||||||
| Giannini S, 2021 [22] | 77 | Vitamin D3 | Group 1: oral 400 kIU vitamin D (2*100 kIU daily for two consecutive days) | Death and/or ICU support | Death | Group 1: 43.3% | Group 1: 33.3% | 28.6% |
| Group 2: no supplementation | Group 2: 57.4% | Group 2: 25.5% | ||||||
| Tan CW, 2020 [27] | 20 | Vitamin D3, B12, magnesium, | Group 1: single daily dose 1 kIU for ≤14 days | Oxygen therapy requirement and/or ICU support | Oxygen therapy requirement but no ICU support | Group 1: 25.0% | Group 1: 12.5% | 0.0% |
| Group 2: no supplementation | Group 2: 58.3% | Group 2: 16.7% | ||||||
| Author, Year | N | Serum Vitamin D Level (ng/mL) | Serum Vitamin D Level in COVID-19+ Patients (ng/mL) | Serum Vitamin D Level in COVID-19- Patients (ng/mL) | Subjects with Vitamin D Deficiency |
|---|---|---|---|---|---|
| Baktash V, 2020 [19] | 105 | 14.3 ± * | 10.8 ± 8.8 ¶ | 20.8 ± 16.0 ¶ | 45.7% |
| Carpagnano GE, 2020 [20] | 27 | 16.1 ± 14.0 † | 16.1 ± 14.0 † | NA | 37.0% |
| Cereda E, 2020 [21] | 106 | 13.9 ± 11.7 | 13.9 ± 11.7 | NA | 74.5% |
| Hars M, 2020 [23] | 160 | 24.0 ± 15.2 ¶ | 24.0 ± 15.2 ¶ | NA | 36.9% |
| Macaya F, 2020 [24] | 55 | 17.0 ± 22.0 ¶ | 16.7 ± 22.0 ¶ | NA | 52.7% |
| Radujkovic A, 2020 [25] | 185 | 19.7 ± 12.4 † | 19.7 ± 12.4 † | NA | 63.7% |
| Sulli A, 2021 [26] | 130 | 12.1 ± 17.0 ¶ | 7.9 ± 15.0 ¶ | 16.3 ± 19.0 ¶ | 83.8% |
| Author, Year | N | Outcome | Results | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Primary | Secondary | Primary | Secondary | Deaths | ||||||
| Overall | Deficiency | No Deficiency | Overall | Deficiency | No Deficiency | |||||
| Baktash V, 2020 [19] | 105 | In-hospital death ‡ | Composite ‡,§ | 14.3% | 15.4% | 12.9% | 48.6% | 59.0% | 35.5% | 14.3% |
| Carpagnano GE, 2020 [20] | 42 | 10-day death | 18.5% | 30.0% | 11.8% | 18.5% | ||||
| Cereda E, 2020 [21] | 106 | Prevalence of deficit | Composite || | 74.5% | 100.0% | 0.0% | 90.6% | 92.4% | 85.2% | 31.1% |
| Hars M, 2020 [23] | 160 | In-hospital death | 25.0% | 32.2% | 20.8% | 25.0% | ||||
| Macaya F, 2020 [24] | 80 | Composite ¶ | 43.6% | 44.8% | 42.34% | 21.3% | ||||
| Radujkovic A, 2020 [25] | 97 | IMV and/or death | Death | 24.7% | 57.7% | 12.7% | 15.5% | 46.2% | 4.2% | 15.5% |
| Sulli A, 2021 [26] | 65 # | In-hospital death | 15.4% | 17.6% | 7.1% | 15.4% | ||||
| Study First Author, Month Year | Selection | Comparability | Outcome | Total Score | Quality Rating |
|---|---|---|---|---|---|
| Annweiler C, September 2020 [17] | ** | * | *** | 6 | Moderate |
| Annweiler G, November 2020 [18] | *** | * | *** | 7 | High |
| Giannini S, January 2021 [22] | *** | ** | *** | 8 | High |
| Tan CW, December 2020 [27] | **** | ** | *** | 9 | High |
| Baktash V, August 2020 [19] | **** | * | *** | 8 | High |
| Carpagnano GE, August 2020 [20] | **** | * | *** | 8 | High |
| Cereda E, October 2020 [21] | **** | ** | *** | 9 | High |
| Hars M, October 2020 [23] | **** | ** | *** | 9 | High |
| Macaya F, October 2020 [24] | **** | ** | *** | 9 | High |
| Radujkovic A, September 2020 [25] | *** | * | *** | 7 | High |
| Sulli A, February 2021 [26] | **** | ** | *** | 9 | High |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dramé, M.; Cofais, C.; Hentzien, M.; Proye, E.; Coulibaly, P.S.; Demoustier-Tampère, D.; Destailleur, M.-H.; Lotin, M.; Cantagrit, E.; Cebille, A.; et al. Relation between Vitamin D and COVID-19 in Aged People: A Systematic Review. Nutrients 2021, 13, 1339. https://doi.org/10.3390/nu13041339
Dramé M, Cofais C, Hentzien M, Proye E, Coulibaly PS, Demoustier-Tampère D, Destailleur M-H, Lotin M, Cantagrit E, Cebille A, et al. Relation between Vitamin D and COVID-19 in Aged People: A Systematic Review. Nutrients. 2021; 13(4):1339. https://doi.org/10.3390/nu13041339
Chicago/Turabian StyleDramé, Moustapha, Cécilia Cofais, Maxime Hentzien, Emeline Proye, Pécory Souleymane Coulibaly, David Demoustier-Tampère, Marc-Henri Destailleur, Maxime Lotin, Eléonore Cantagrit, Agnès Cebille, and et al. 2021. "Relation between Vitamin D and COVID-19 in Aged People: A Systematic Review" Nutrients 13, no. 4: 1339. https://doi.org/10.3390/nu13041339