
Lung Ultrasound Patterns and Clinical-Laboratory Correlates during COVID-19 Pneumonia: A Retrospective Study from North East Italy

 , , , , , , , , , , , ,
, , , , , , , , , , , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population and Data Collection
2.2. Ultrasound Examination and Scoring
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. LUS Patterns and COVID-19 Severity
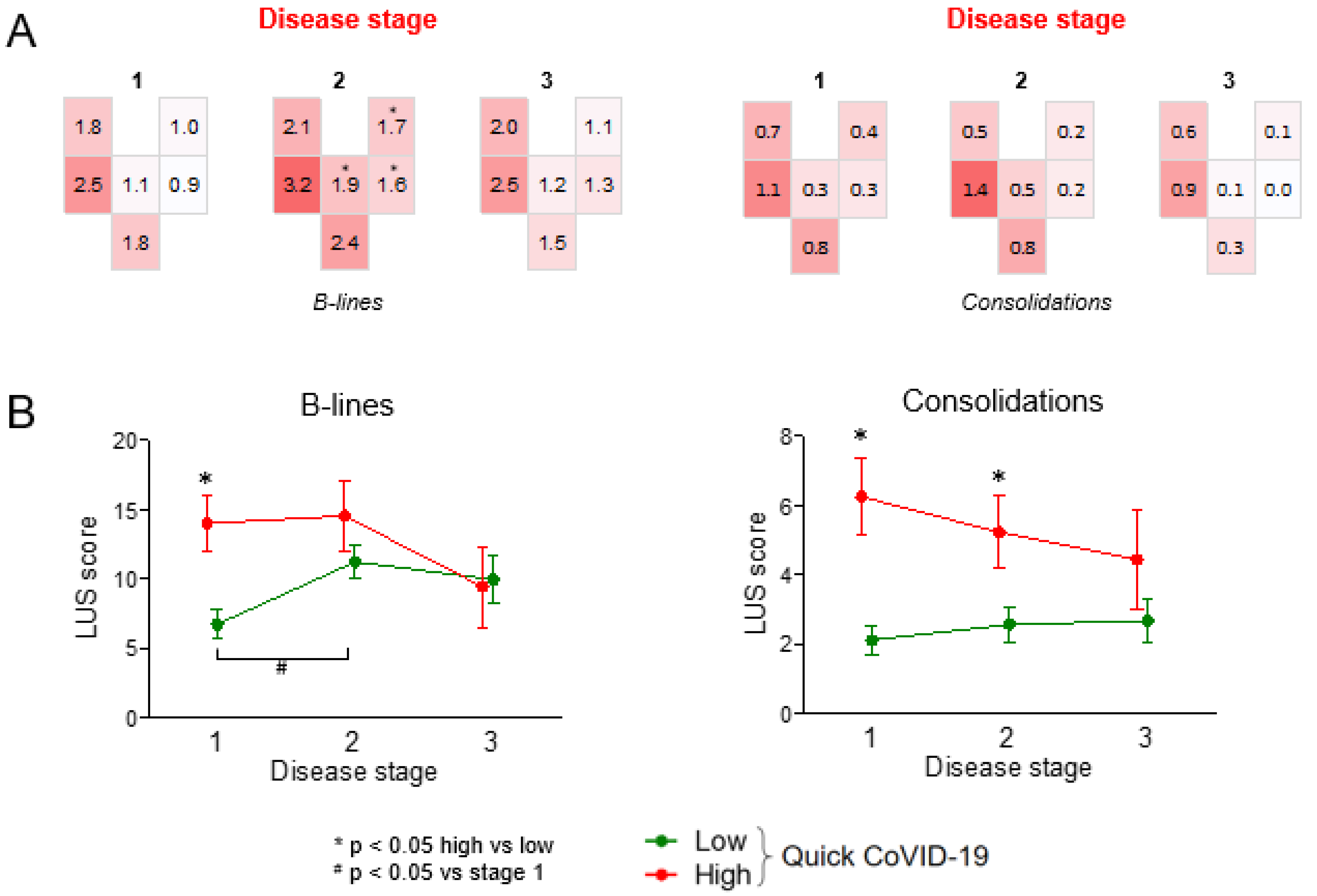
3.3. LUS Patterns According to Disease Stage
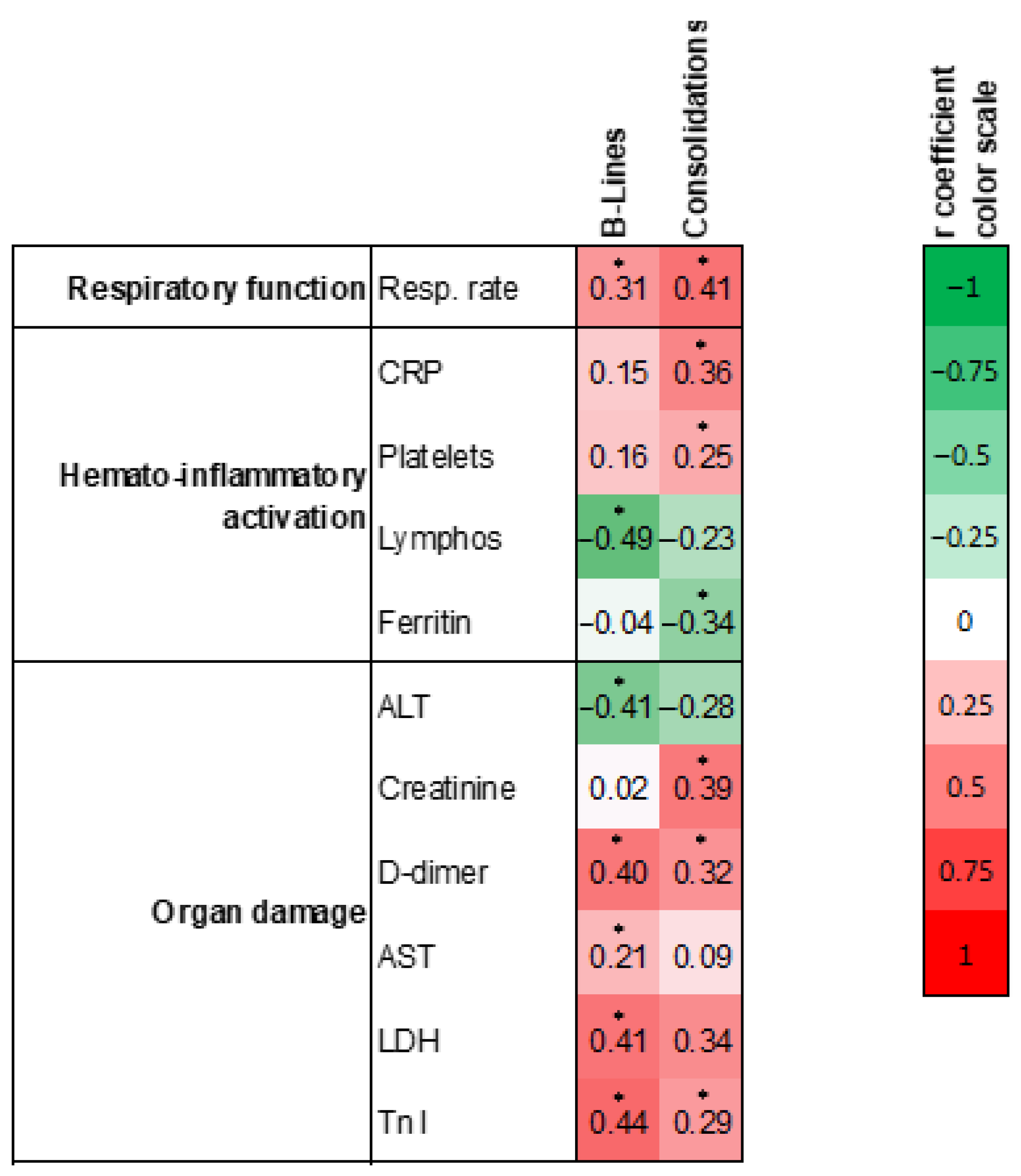
3.4. Clinical Correlates of LUS Score
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y.; et al. Extrapulmonary manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef]
- Chen, M.; Shen, W.; Rowan, N.R.; Kulaga, H.; Hillel, A.; Ramanathan, M.; Lane, A.P., Jr. Elevated ACE-2 expression in the olfactory neuroepithelium: Implications for anosmia and upper respiratory SARS-CoV-2 entry and replication. Eur. Respir. J. 2020, 56, 2001948. [Google Scholar] [CrossRef]
- Damiani, S.; Fiorentino, M.; De Palma, A.; Foschini, M.P.; Lazzarotto, T.; Gabrielli, L.; Viale, P.L.; Attard, L.; Riefolo, M.; D’Errico, A. Pathological post-mortem findings in lungs infected with SARS-CoV-2. J. Pathol. 2020, 253, 31–40. [Google Scholar] [CrossRef]
- Islam, N.; Salameh, J.P.; Leeflang, M.M.; Hooft, L.; McGrath, T.A.; van der Pol, C.B.; Frank, R.A.; Kazi, S.; Prager, R.; Hare, S.S.; et al. Thoracic imaging tests for the diagnosis of COVID-19. Cochrane Database Syst. Rev. 2020, 11, CD013639. [Google Scholar]
- Abrams, E.R.; Rose, G.; Fields, J.M.; Esener, D. Point-of-Care Ultrasound in the Evaluation of COVID-19. J. Emerg. Med. 2020, 59, 403–408. [Google Scholar] [CrossRef]
- Nouvenne, A.; Zani, M.D.; Milanese, G.; Parise, A.; Baciarello, M.; Bignami, E.G.; Odone, A.; Sverzellati, N.; Meschi, T.; Ticinesi, A. Lung Ultrasound in COVID-19 Pneumonia: Correlations with Chest CT on Hospital admission. Respiration 2020, 99, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.; Zhang, Y.; Wang, H.; Chen, L.; Yang, Z.; Peng, Z.; Liu, Y.; Feng, C.; Huang, X.; Jiang, N.; et al. Semiquantitative lung ultrasound scores in the evaluation and follow-up of critically ill patients with COVID-19: A single-center study. Acad. Radiol. 2020, 27, 1363–1372. [Google Scholar] [CrossRef]
- Colombi, D.; Petrini, M.; Maffi, G.; Villani, G.D.; Bodini, F.C.; Morelli, N.; Milanese, G.; Silva, M.; Sverzellati, N.; Michieletti, E. Comparison of admission chest computed tomography and lung ultrasound performance for diagnosis of COVID-19 pneumonia in populations with different disease prevalence. Eur. J. Radiol. 2020, 133, 109344. [Google Scholar] [CrossRef] [PubMed]
- Xing, C.; Li, Q.; Du, H.; Kang, W.; Lian, J.; Yuan, L. Lung ultrasound findings in patients with COVID-19 pneumonia. Crit. Care 2020, 24, 174. [Google Scholar] [CrossRef] [PubMed]
- Yasukawa, K.; Minami, T. Point-of-Care Lung Ultrasound Findings in Patients with COVID-19 Pneumonia. Am. J. Trop. Med. Hyg. 2020, 102, 1198–1202. [Google Scholar] [CrossRef] [Green Version]
- Peng, Q.Y.; Wang, X.T.; Zhang, L.N. Findings of lung ultrasonography of novel corona virus pneumonia during the 2019–2020 epidemic. Intensive Care Med. 2020, 46, 849–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, L.; Yu, K.; Zhao, Q.; Tian, R.; Xie, H.; Xie, L.; Deng, P.; Xie, G.; Bao, A.; Du, J. Lung Ultrasound Score in Evaluating the Severity of Coronavirus Disease 2019 (COVID-19) Pneumonia. Ultrasound Med. Biol. 2020, 46, 2938–2944. [Google Scholar] [CrossRef]
- Soldati, G.; Smargiassi, A.; Inchingolo, R.; Buonsenso, D.; Perrone, T.; Briganti, D.F.; Perlini, S.; Torri, E.; Mariani, A.; Mossolani, E.E.; et al. Proposal for International Standardization of the Use of Lung Ultrasound for Patients With COVID-19: A Simple, Quantitative, Reproducible Method. J. Ultrasound Med. 2020, 39, 1413–1419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haimovich, A.D.; Ravindra, N.G.; Stoytchev, S.; Young, H.P.; Wilson, F.P.; van Dijk, D.; Schulz, W.L.; Taylor, R.A. Development and Validation of the Quick COVID-19 Severity Index: A Prognostic Tool for Early Clinical Decompensation. Ann. Emerg. Med. 2020, 76, 442–453. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (2019-nCoV) Infection Is Suspected: Interim Guidance. Available online: https://appswhoint/iris/handle/10665/330893 (accessed on 28 January 2020).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Dargent, A.; Chatelain, E.; Kreitmann, L.; Quenot, J.P.; Cour, M.; Argaud, L. Lung ultrasound score to monitor COVID-19 pneumonia progression in patients with ARDS. PLoS ONE 2020, 15, e0236312. [Google Scholar] [CrossRef]
- Lichter, Y.; Topilsky, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Gal Oz, A.; Vine, J.; Goren, O.; Cohen, B.; et al. Lung ultrasound predicts clinical course and outcomes in COVID-19 patients. Intensive Care Med. 2020, 46, 1873–1883. [Google Scholar] [CrossRef] [PubMed]
- Zieleskiewicz, L.; Markarian, T.; Lopez, A.; Taguet, C.; Mohammedi, N.; Boucekine, M.; Baumstarck, K.; Besch, G.; Mathon, G.; Duclos, G.; et al. Comparative study of lung ultrasound and chest computed tomography scan in the assessment of severity of confirmed COVID-19 pneumonia. Intensive Care Med. 2020, 46, 1707–1713. [Google Scholar] [CrossRef]
- Gandini, O.; Criniti, A.; Gagliardi, M.C.; Ballesio, L.; Giglio, S.; Balena, A.; Caputi, A.; Angeloni, A.; Lubrano, C. Sex-disaggregated data confirm serum ferritin as an independent predictor of disease severity both in male and female COVID-19 patients. J. Infect. 2020, 82, 414–451. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Li, H.; Li, L.; Liu, C.; Yan, S.; Chen, H.; Li, Y. Ferritin in the coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. J. Clin. Lab. Anal. 2020, 34, e23618. [Google Scholar] [CrossRef]
- Samaddar, A.; Grover, M.; Nag, V.L. Pathophysiology and Potential Therapeutic Candidates for COVID-19: A Poorly Understood Arena. Front. Pharmacol. 2020, 11, 585888. [Google Scholar] [CrossRef] [PubMed]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of Covid-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Stone, J.H.; Frigault, M.J.; Serling-Boyd, N.J.; Fernandes, A.D.; Harvey, L.; Foulkes, A.S.; Horick, N.K.; Healy, B.C.; Shah, R.; Bensaci, A.M.; et al. Efficacy of Tocilizumab in Patients Hospitalized with Covid-19. N. Engl. J. Med. 2020, 383, 2333–2344. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.; Mafham, M.; Linsell, L.; Bell, J.L.; Staplin, N.; Emberson, J.R.; Wiselka, M.; Ustianowski, A.; Elmahi, E.; Prudon, B.; et al. Effect of Hydroxychloroquine in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2020, 383, 2030–2040. [Google Scholar] [PubMed]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020, 384, 693–704. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All (n = 96) | qCSI ≤ 3 (n = 69) | qCSI > 3 (n = 27) | p Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, mean (SD), years | 65.87 (15.28) | 63.56 (15.86) | 71.77 (12.04) | 0.008 |
| Male, n (%) | 56 (58.33) | 38 (55.07) | 18 (66.67) | 0.300 |
| Female, n (%) | 40 (41.67) | 31 (44.93) | 9 (33.33) | 0.300 |
| Ethnicity, % Caucasian | 89 (93.68) | 64 (94.12) | 25 (92.59) | 0.782 |
| Weight, mean (SD), kg | 78.37 (14.71) | 80.05 (15.24) | 73.25 (11.94) | 0.074 |
| Height, mean (SD), m | 1.68 (0.22) | 1.67 (0.26) | 1.69 (0.07) | 0.661 |
| Comorbidities | ||||
| Hypertension, n (%) | 41 (42.71) | 31 (44.93) | 10 (37.04) | 0.482 |
| Diabetes, n (%) | 23 (23.96) | 19 (27.54) | 4 (14.81) | 0.189 |
| Smoking, n (%) | 6 (6.25) | 4 (5.8) | 2 (7.41) | 0.769 |
| BMI > 30, n (%) | 26 (27.08) | 22 (31.88) | 4 (14.81) | 0.090 |
| Hyperlipidemia, n (%) | 19 (19.79) | 13 (18.84) | 6 (22.22) | 0.708 |
| Coronary disease, n (%) | 5 (5.21) | 2 (2.9) | 3 (11.11) | 0.103 |
| TIA/Stroke, n (%) | 6 (6.25) | 4 (5.8) | 2 (7.41) | 0.769 |
| Heart failure, n (%) | 4 (4.17) | 3 (4.35) | 1 (3.7) | 0.887 |
| Atrial Fibrillation, n (%) | 14 (14.58) | 10 (14.49) | 4 (14.81) | 0.967 |
| CKD (eGFR < 30 mL/min), n (%) | 2 (2.08) | 2 (2.9) | 0 | 0.371 |
| Previous DVT/PE, n (%) | 6 (6.25) | 4 (5.8) | 2 (7.41) | 0.769 |
| Chronic Anemia, n (%) | 4 (4.17) | 2 (2.9) | 2 (7.41) | 0.320 |
| COPD/Asthma, n (%) | 10 (10.42) | 9 (13.04) | 1 (3.7) | 0.178 |
| Cancer, n (%) | 10 (10.42) | 10 (14.49) | 0 | 0.036 |
| Liver disease, n (%) | 3 (3.13) | 3 (4.35) | 0 | 0.270 |
| Severe Cognitive impairment, n (%) | 7 (7.29) | 5 (7.25) | 2 (7.41) | 0.978 |
| Immunodepression, n (%) | 5 (5.21) | 4 (5.8) | 1 (3.7) | 0.678 |
| Administered drugs | ||||
| Hydroxychloroquine, n (%) | 63 (67.74) | 48 (71.64) | 15 (67.59) | 0.193 |
| Tocilizumab, n (%) | 40 (41.67) | 30 (43.48) | 10 (37.04) | 0.564 |
| Azithromycin, n (%) | 23 (23.96) | 18 (26.09) | 5 (18.52) | 0.434 |
| Darunavir/Cobicistat, n (%) | 7 (7.29) | 3 (4.35) | 4 (14.81) | 0.076 |
| Anticoagulants (therapeutic dose), n (%) | 21 (21.88) | 13 (18.84) | 8 (29.63) | 0.250 |
| Clinical features (at the moment of the ultrasound) | ||||
| Respiratory features | ||||
| qCSI, mean (SD) | 2.12 (2.89) | 0.5 (0.86) | 6.25 (2.01) | <0.001 |
| Respiratory rate, mean (SD), breaths/minute | 20.29 (5.26) | 18.81 (4.2) | 24.07 (5.86) | <0.001 |
| SpO2, mean (SD), % | 94.07 (4.81) | 95.42 (2.43) | 90.62 (7.22) | 0.002 |
| P/F, mean (SD), ratio | 290.89 (89.66) | 330.71 (60.3) | 199 (78.49) | <0.001 |
| pO2, mean (SD), mmHg | 75.23 (41.56) | 69.65 (12.74) | 88.11 (72.4) | 0.208 |
| Diffuse lung crepitations, n (%) | 8 (8.33) | 3 (4.41) | 5 (18.52) | 0.025 |
| Bronchostenosis, n (%) | 0 (0) | 0 | 0 | |
| Pathological chest X-ray (n = 88), n (%) | 75 (85.23) | 51 (82.26) | 24 (92.31) | 0.225 |
| Pneumothorax, n (%) | 0 (0) | 0 | 0 | |
| Pleural Effusion, n (%) | 35 (36.6) | 20 (28.99) | 15 (55.56) | 0.0150 |
| Other physical examination features | ||||
| Body temperature, mean (SD), Celsius | 36.57 (2.46) | 36.33 (2.77) | 37.18 (1.24) | 0.041 |
| SBP, mean (SD), mmHg | 132.6 (18.08) | 130.42 (16.5) | 138.18 (20.9) | 0.091 |
| Heart rate, mean (SD), beats/minute | 88.44 (17.42) | 88.31 (17.11) | 88.77 (18.52) | 0.911 |
| Dilated IVC (n = 33), n (%) | 2 (6.06) | 0 | 2 (20) | 0.026 |
| Reduced EF (n = 26), n (%) | 4 (15.38) | 3 (18.75) | 1 (10) | 0.547 |
| Laboratory tests | ||||
| Lactate (n = 69), mean (SD), mmol/L | 1.35 (0.88) | 1.31 (0.91) | 1.46 (0.82) | 0.509 |
| Hemoglobin, mean (SD), g/L | 134.71 (18.88) | 135.5 (18.9) | 132.7 (19.04) | 0.518 |
| Neutrophils, mean (SD), cells/mm3 | 4857.84 (3130.76) | 4278.75 (2474.57) | 6267.82 (4063.33) | 0.036 |
| Platelets, mean (SD), cells/mm3 | 225,555.2 (88,245.85) | 215,277.18 (81,303.13) | 251,821.25 (100,840.02) | 0.100 |
| Limphocytes, mean (SD), cells/mm3 | 1517.97 (1172.77) | 1473.14 (955.24) | 1646.25 (1730.68) | 0.706 |
| Creatinine, mean (SD), µmol/L | 78.74 (21.87) | 80.41 (22.25) | 74.47 (20.63) | 0.220 |
| D-dimer (n = 70), mean (SD), µg/L | 1680.88 (4549.48) | 732.04 (1148.74) | 4053 (7966.81) | 0.078 |
| LDH, mean (SD), U/L | 333.84 (128.73) | 308.6 (113.57) | 390.85 (144.29) | 0.012 |
| CRP, mean, (SD), mg/L | 67.56 (68.51) | 48.53 (44.93) | 117.82 (92.24) | 0.001 |
| PCT (n = 62), mean, (SD), ng/mL | 0.58 (3.18) | 0.59 (3.61) | 0.56 (1.87) | 0.963 |
| BNP (n = 51), mean, (SD), pg/mL | 888.74 (4888.88) | 1246.83 (6266.91) | 333.8 (593.76) | 0.426 |
| Troponin I (n = 73), mean, (SD), ng/L | 12.13 (14.73) | 9.96 (11.52) | 17.52 (20) | 0.116 |
| Ferritin (n = 64), mean, (SD), ng/mL | 849.03 (788.7) | 765.36 (744.74) | 1062.83 (877.35) | 0.214 |
| CPK (n = 74), mean, (SD), U/L | 151.04 (270.86) | 139.87 (273.13) | 183.36 (268.79) | 0.549 |
| ALT, mean, (SD), U/L | 46.18 (41.28) | 41.33 (28.49) | 58.5 (62.23) | 0.186 |
| AST, mean, (SD), U/L | 46.2 (28.38) | 41.34 (20.61) | 58.53 (40.08) | 0.045 |
| Clinical outcomes | ||||
| Oxygen rate flow ≥ 12 L/min, n (%) | 28 (29.16) | 14 (20.28) | 14 (51.85) | 0.002 |
| NIV/OTI, n (%) | 24 (25) | 13 (18.84) | 11 (40.74) | <0.001 |
| Death, n (%) | 8 (8.33) | 4 (5.79) | 4 (14.81) | 0.150 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Senter, R.; Capone, F.; Pasqualin, S.; Cerruti, L.; Molinari, L.; Fonte Basso, E.; Zanforlin, N.; Previato, L.; Toffolon, A.; Sensi, C.; et al. Lung Ultrasound Patterns and Clinical-Laboratory Correlates during COVID-19 Pneumonia: A Retrospective Study from North East Italy. J. Clin. Med. 2021, 10, 1288. https://doi.org/10.3390/jcm10061288
Senter R, Capone F, Pasqualin S, Cerruti L, Molinari L, Fonte Basso E, Zanforlin N, Previato L, Toffolon A, Sensi C, et al. Lung Ultrasound Patterns and Clinical-Laboratory Correlates during COVID-19 Pneumonia: A Retrospective Study from North East Italy. Journal of Clinical Medicine. 2021; 10(6):1288. https://doi.org/10.3390/jcm10061288
Chicago/Turabian StyleSenter, Riccardo, Federico Capone, Stefano Pasqualin, Lorenzo Cerruti, Leonardo Molinari, Elisa Fonte Basso, Nicolò Zanforlin, Lorenzo Previato, Alessandro Toffolon, Caterina Sensi, and et al. 2021. "Lung Ultrasound Patterns and Clinical-Laboratory Correlates during COVID-19 Pneumonia: A Retrospective Study from North East Italy" Journal of Clinical Medicine 10, no. 6: 1288. https://doi.org/10.3390/jcm10061288