

SARS-CoV-2 and Its Variants in Thrice-Infected Health Workers: A Case Series from an Italian University Hospital
 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bastard, J.; Taisne, B.; Figoni, J.; Mailles, A.; Durand, J.; Fayad, M.; Josset, L.; Maisa, A.; van der Werf, S.; du Châtelet, I.P.; et al. Impact of the Omicron variant on SARS-CoV-2 reinfections in France, March 2021 to February 2022. Eurosurveillance 2022, 27, 2200247. [Google Scholar] [CrossRef] [PubMed]
- AlMadhi, M.; Alsayyad, A.S.; Conroy, R.; Atkin, S.; Al Awadhi, A.; Al-Tawfiq, J.A.; AlQahtani, M. Epidemiological Assessment of SARS-CoV-2 Reinfection. Int. J. Infect. Dis. 2022, 123, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Gargouri, S.; Souissi, A.; Abid, N.; Chtourou, A.; Feki-Berrajah, L.; Karray, R.; Kossentini, H.; Ben Ayed, I.; Abdelmoula, F.; Chakroun, O.; et al. Evidence of SARS-CoV-2 symptomatic reinfection in four healthcare professionals from the same hospital despite the presence of antibodies. Int. J. Infect. Dis. 2022, 117, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Mohsin, M.; Mahmud, S. Omicron SARS-CoV-2 variant of concern: A review on its transmissibility, immune evasion, reinfection, and severity. Medicine 2022, 101, e29165. [Google Scholar] [CrossRef] [PubMed]
- Brehm, T.; Pfefferle, S.; von Possel, R.; Kobbe, R.; Nörz, D.; Schmiedel, S.; Grundhoff, A.; Olearo, F.; Emmerich, P.; Robitaille, A.; et al. SARS-CoV-2 Reinfection in a Healthcare Worker Despite the Presence of Detectable Neutralizing Antibodies. Viruses 2021, 13, 661. [Google Scholar] [CrossRef] [PubMed]
- Porru, S.; Spiteri, G.; Monaco, M.G.L.; Valotti, A.; Carta, A.; Lotti, V.; Diani, E.; Lippi, G.; Gibellini, D.; Verlato, G. Post-Vaccination SARS-CoV-2 Infections among Health Workers at the University Hospital of Verona, Italy: A Retrospective Cohort Survey. Vaccines 2022, 10, 272. [Google Scholar] [CrossRef] [PubMed]
- Yahav, D.; Yelin, D.; Eckerle, I.; Eberhardt, C.S.; Wang, J.; Cao, B.; Kaiser, L. Definitions for coronavirus disease 2019 reinfection, relapse and PCR re-positivity. Clin. Microbiol. Infect. 2021, 27, 315–318. [Google Scholar] [CrossRef] [PubMed]
- ISS. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-monitoraggio-varianti (accessed on 18 September 2022).
- Swift, M.D.; Hainy, C.M.; Sampathkumar, P.; Breeher, L.E. Multiple SARS-CoV-2 Reinfections: A Case Series of Thrice-Infected Individuals. Mayo Clin. Proc. 2022, 97, 1021–1023. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No | Workers’ Characteristics (Age-yo-/Sex/Job Title/ Vaccination Dates) | Infections Details (Date, Lag in-Days-, Variant, Lineage, Cause of Swab Testing, Type of Contact) | ||
|---|---|---|---|---|
| 1st infection | 2nd infection | 3rd infection | ||
| 1 | 46 | 21/03/2020 | 25/01/2021 | 09/07/2022 |
| Female | 28 | 17 | 7 | |
| nurse | Wuhan * | Delta ** | BA.1 ** | |
| 1st dose: 07/05/2021 | Symptoms onset | Strict contact | Strict contact | |
| 2nd dose: 22/12/2021 | Occupational | Occupational | Relative/friend | |
| 2 | 30 | 07/04/2020 | 10/06/2021 | 12/02/2022 |
| male | 15 | 7 | 7 | |
| physician | Wuhan * | B.1.1.7 * | BA.1 ** | |
| 1st dose: 07/01/2021 | Screening | Screening | Screening | |
| 2nd dose: 28/01/2021 3rd dose: 09/11/2021 | Unknown | Unknown | Unknown | |
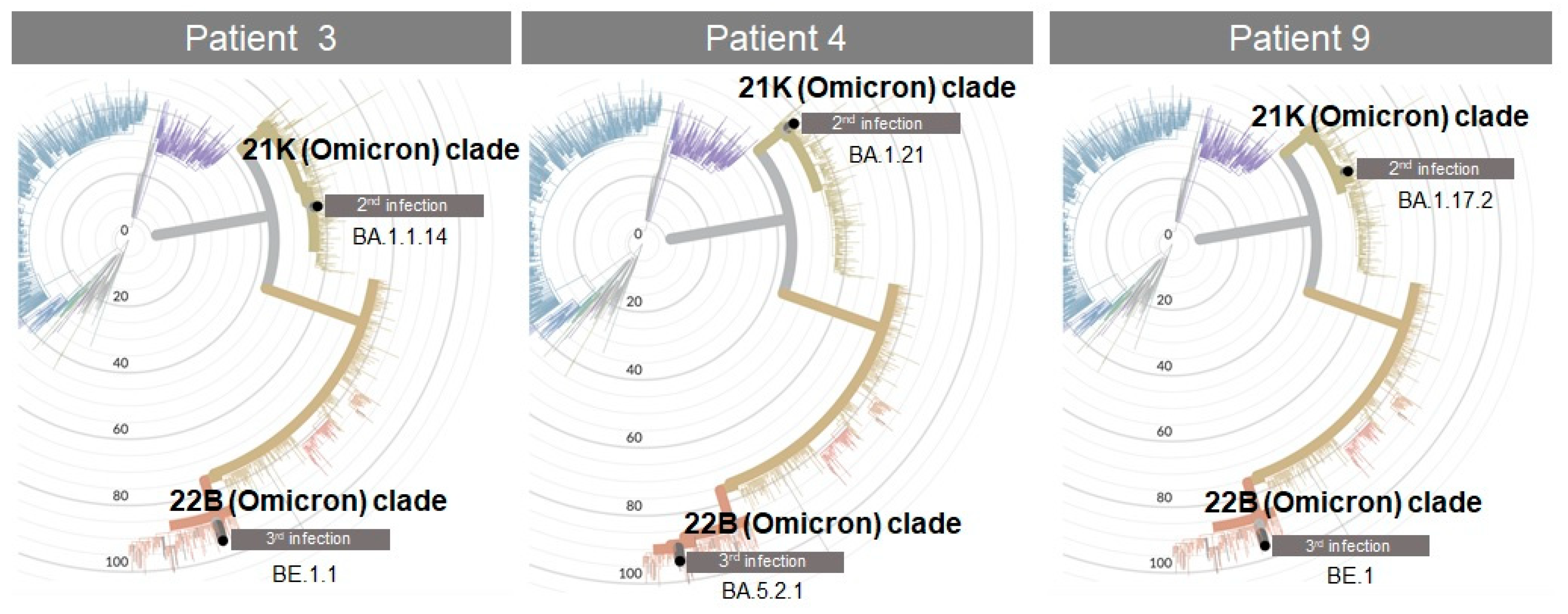
| 3 | 33 | 14/03/2020 | 12/02/2022 | 10/07/2022 |
| female | 31 | 10 | 10 | |
| nurse | Wuhan * | BA.1 ** (BA.1.1.14 †) | BA.1 ** (BE.1.1 †) | |
| 1st dose: 07/05/2021 | Strict contact | Screening | Symptoms onset | |
| 2nd dose: 28/05/2021 | Occupational | Unknown | Occupational | |
| 4 | 46 | 29/03/2021 | 16/02/2022 | 22/07/2022 |
| female | 7 | 15 | 7 | |
| nurse | B.1.1.7 * | BA.1 ** (BA.1.21 †) | BA.1 ** (BA.5.2.1 †) | |
| 1st dose: 11/02/2022 | Screening | Symptoms onset | Symptoms onset | |
| 2nd dose:03/06/2022 | Unknown | Relative/friend | Relative/friend | |
| 5 | 49 | 17/12/2020 | 04/05/2021 | 10/01/2022 |
| male | 11 | 7 | 7 | |
| physician | Wuhan * | B.1.1.7 * | Omicron * | |
| 1st dose: 05/01/2021 | Screening | Screening | Screening | |
| 2nd dose:26/01/2021 3rd dose: 09/11/2021 | Unknown | Unknown | Unknown | |
| 6 | 40 | 19/07/2021 | 01/01/2022 | 04/08/2022 |
| male | 11 | 18 | 7 | |
| nurse | B.1.617.2 * | BA.1 ** | BA.5 * | |
| 1st dose: 11/02/2021 | Screening | Symptoms onset | Symptoms onset | |
| 2nd dose: 04/03/2021 3rd dose:13/12/2021 | Relative/friend | Occupational | Occupational | |
| 7 | 48 | 27/04/2021 | 16/04/2022 | 02/08/2022 |
| female | 11 | 7 | 7 | |
| nurse | Alfa ** | BA.2 ** | BA.1 ** | |
| 1st dose: 06/01/2021 | Strict contact | Screening | Symptoms onset | |
| 2nd dose: 27/01/2021 3rd dose:09/12/2021 | Relative/friend | Occupational | Relative/friend | |
| 8 | 56 | 27/10/2020 | 13/01/2022 | 18/05/2022 |
| female | 34 | 7 | 7 | |
| nurse | Wuhan * | BA.1 ** | BA.2 ** | |
| 1st dose: 01/09/2021 | Strict contact | Strict contact | Strict contact | |
| Occupational | Occupational | Occupational | ||
| 9 | 42 | 13/11/2020 | 24/01/2022 | 29/06/2022 |
| female | 10 | 7 | 7 | |
| other HW | Wuhan * | BA.1 ** (BA.1.17.2 †) | BA.1 ** (BE.1 †) | |
| 1st dose: 11/10/2021 | Symptoms onset | Screening | Screening | |
| Occupational | Unknown | Unknown | ||
| 10 | 56 | 10/11/2020 | 10/06/2021 | 13/06/2022 |
| female | 10 | 7 | 7 | |
| nurse | Wuhan * | B.1.1.7 * | BA.2 * | |
| 1st dose: 16/03/2021 | Strict contact | Screening | Strict contact | |
| 2nd dose:09/12/2021 | Occupational | Unknown | Relative/friend | |
| 11 | 30 | 31/12/2020 | 16/12/2021 | 21/06/2022 |
| male | 16 | 7 | 7 | |
| nurse | Wuhan * | Delta ** | BA.1 ** | |
| 1st dose: 16/02/2021 | N/A | N/A | N/A | |
| 2nd dose: 10/03/2021 3rd dose:14/12/2021 | N/A | N/A | N/A | |
| 12 | 54 | 05/02/2021 | 03/01/2022 | 13/07/2022 |
| female | 10 | 7 | 9 | |
| nurse | B.1.1.7 * | Omicron * | BA.1 ** | |
| 1st dose: 05/02/2021 | Strict contact | Screening | Symptoms onset | |
| 2nd dose: 26/02/2021 3rd dose:16/12/2021 | Occupational | Relative/friend | Occupational | |
| 1st infection | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HWs no | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
| No symptoms | U | U | U | F | N/A | |||||||
| Minor symptoms | U | U | F | U | U | N/A | U | |||||
| Major symptoms | U | N/A | ||||||||||
| Hospitalisation | N/A | |||||||||||
| 2nd infection | ||||||||||||
| HWs no | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
| No symptoms | U | F | F | P | P | N/A | ||||||
| Minor symptoms | F | P | B | B | P | N/A | F | |||||
| Major symptoms | N/A | |||||||||||
| Hospitalisation | N/A | |||||||||||
| 3rd infection | ||||||||||||
| HWs no | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
| No symptoms | B | B | P | N/A | ||||||||
| Minor symptoms | F | F | F | B | B | F | N/A | B | ||||
| Major symptoms | P | N/A | ||||||||||
| Hospitalisation | N/A | |||||||||||
| No | 1st Positivity | 2nd Positivity | 3rd Positivity | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Allplex™ SARS-CoV-2 Assay (Seegene) | |||||||||
| E Gene | S Gene | N Gene | E Gene | S Gene | N Gene | E Gene | S Gene | N Gene | |
| 1 | 19.39 | 21.18 | 22.18 | 32.64 | 32.23 | 30.28 | 37.32 | 37.38 | |
| 2 | 29.95 | 31.09 | 28.49 | ||||||
| 3 | 17.63 | 18.98 | 21.50 | 26.64 | 27.19 | 24.06 | 28.34 | 30.52 | 27.70 |
| 4 | 32.76 | 34.11 | 31.57 | 28.06 | 28.08 | 26.75 | |||
| 5 | 32.75 | 32.69 | 34.03 | ||||||
| 6 | 38.13 | 38.51 | 37.60 | 35.92 | 34.30 | 21.16 | 22.13 | ||
| 7 | 26.85 | 31.28 | 33.57 | 22.41 | 23.66 | 21.34 | |||
| 8 | 23.21 | 23.45 | 20.88 | 20.34 | 20.91 | 19.69 | |||
| 9 | 25.85 | 28.64 | 24.87 | 37.00 | 37.00 | ||||
| 11 | 32.96 | 34.25 | 29.77 | 36.70 | 39.10 | ||||
| 12 | 34.39 | 36.38 | 34.62 | 22.13 | 20.22 | ||||
| EurobioPlex SARS-CoV-2 Multiplex (Eurobio Scientific) | |||||||||
| RdRp gene(Target 1) | RdRp gene(Target 2) | N gene | |||||||
| 4 | 35.00 | 35.00 | 35.00 | ||||||
| Simplexa™ COVID-19 Direct Kit (DiaSorin Molecular) | |||||||||
| Orf1ab | S gene | Orf1ab | S gene | ||||||
| 7 | 31.80 | 29.40 | |||||||
| 11 | 20.00 | 19.00 | |||||||
| TaqPath™ COVID-19 RT-PCR Kit (Applied Biosystem) | |||||||||
| Orf1ab | S gene | N gene | |||||||
| 10 | 20.70 | 20.60 | 22.20 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monaco, M.G.L.; Spiteri, G.; Caliskan, G.; Lotti, V.; Carta, A.; Gibellini, D.; Verlato, G.; Porru, S. SARS-CoV-2 and Its Variants in Thrice-Infected Health Workers: A Case Series from an Italian University Hospital. Viruses 2022, 14, 2536. https://doi.org/10.3390/v14112536
Monaco MGL, Spiteri G, Caliskan G, Lotti V, Carta A, Gibellini D, Verlato G, Porru S. SARS-CoV-2 and Its Variants in Thrice-Infected Health Workers: A Case Series from an Italian University Hospital. Viruses. 2022; 14(11):2536. https://doi.org/10.3390/v14112536
Chicago/Turabian StyleMonaco, Maria Grazia Lourdes, Gianluca Spiteri, Gulser Caliskan, Virginia Lotti, Angela Carta, Davide Gibellini, Giuseppe Verlato, and Stefano Porru. 2022. "SARS-CoV-2 and Its Variants in Thrice-Infected Health Workers: A Case Series from an Italian University Hospital" Viruses 14, no. 11: 2536. https://doi.org/10.3390/v14112536