
COVID-19 Impact in the Italian Reception System for Migrants during the Nationwide Lockdown: A National Observational Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, Population, and Timing
2.2. Data Collection
2.3. Data Analysis and Statistical Analysis
3. Results
3.1. Reception Centres and Hosts
3.2. Suspected and Confirmed COVID-19 Cases
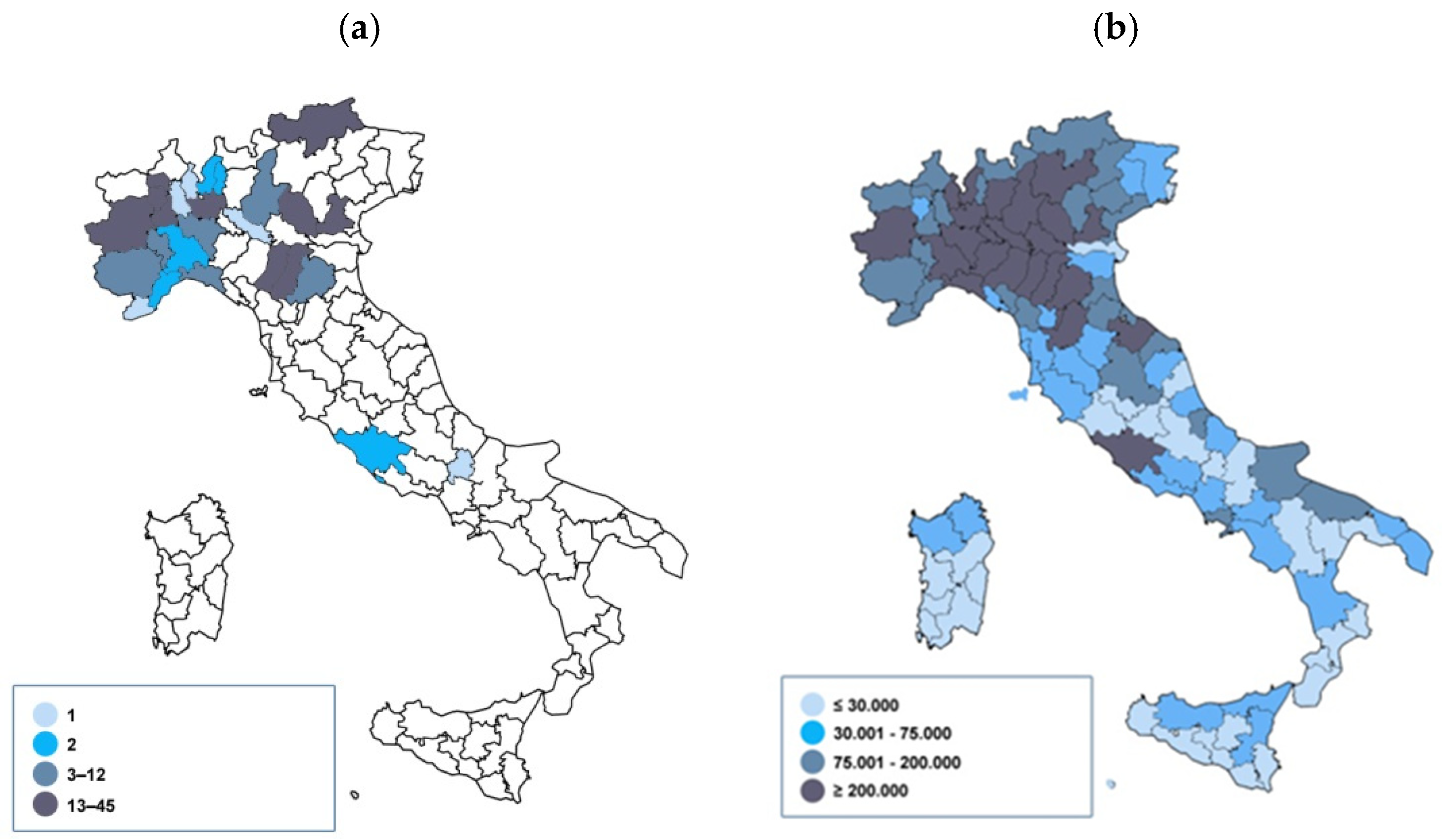
3.2.1. Geographical Distribution and Characteristics of Facilities
3.2.2. Confirmed Cases Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johns Hopkins University (JHU). COVID-19 Dashboard. Available online: https://coronavirus.jhu.edu/map.html (accessed on 27 September 2021).
- Our World in Data. Statistics and Research. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 27 September 2021).
- Saifee, J.; Franco-Paredes, C.; Lowenstein, S.R. Refugee Health During COVID-19 and Future Pandemics. Curr. Trop. Med. Rep. 2021, 16, 1–4. [Google Scholar] [CrossRef] [PubMed]
- UNHCR. Inclusion Key to Protecting Refugees and Their Hosts Amid COVID-19 Pandemic. Available online: https://www.unhcr.org/news/press/2020/11/5fa2f16b4/inclusion-key-protecting-refugees-hosts-amid-covid-19-pandemic.html (accessed on 10 September 2021).
- UNHCR. IOM and UNHCR Chiefs Stress That COVID-19 Underlines the Urgent Need for Universal Health Coverage. Available online: https://www.unhcr.org/news/press/2020/12/5fd35fc94/iom-unhcr-chiefs-stress-covid-19-underlines-urgent-need-universal-health.html (accessed on 10 September 2021).
- Lancet Migration. Leaving No One behind in the COVID-19 Pandemic: A Call for Urgent Global Action to Include Migrants & Refugees in the COVID-19 Response. Available online: https://1bec58c3-8dcb-46b0-bb2a-fd4addf0b29a.filesusr.com/ugd/188e74_b87afbfe45e44eecb13a45a5cea61209.pdf (accessed on 10 September 2021).
- Kluge, H.H.P.; Jakab, Z.; Bartovic, J.; D’Anna, V.; Severoni, S. Refugee and migrant health in the COVID-19 response. Lancet 2020, 395, 1237–1239. [Google Scholar] [CrossRef]
- UNHCR-IOM. Urgent Coordinated Response Needed to the Alarming Conditions of Migrants and Refugees Detained in Melilla. Available online: https://www.iom.int/es/node/101479 (accessed on 10 September 2021).
- ECDC. COVID-19 in Reception and Detention Centres for Migrants and Refugees. Infographic. Available online: https://www.ecdc.europa.eu/en/publications-data/covid-19-reception-and-detention-centres-migrants-and-refugees (accessed on 10 September 2021).
- ECDC. Technical Report. Guidance on Infection Prevention and Control of Coronavirus Disease (COVID-19) in Migrant and Refugee Reception and Detention Centres in the EU/EEA and the United Kingdom. Available online: https://www.ecdc.europa.eu/en/publications-data/covid-19-guidance-prevention-control-migrant-refugee-centres (accessed on 10 September 2021).
- Turunen, T.; Kontunen, K.; Sugulle, K.; Hieta, P.; Snellman, O.; Hussein, I.; Dub, T.; Melin, M.; Haveri, A.; Ekström, N.; et al. COVID-19 outbreak at a reception centre for asylum seekers in Espoo, Finland. J. Migr. Health 2021, 3, 100043. [Google Scholar] [CrossRef] [PubMed]
- ISTAT. Resident Foreigners in Italy at 1st January 2020. Available online: http://demo.istat.it/strasa2020/index_e.html (accessed on 10 September 2021).
- UNHCR Data Finder. Population Figure—Italy. Available online: https://www.unhcr.org/refugee-statistics/download/?url=E1ZxP4 (accessed on 27 September 2021).
- Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Region. A European Agenda on Migration. COM (2015) 240 Final. Brussels, 13 May 2015. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A52015DC0240 (accessed on 10 September 2021).
- Ministry of Interior. Standard Operating Procedures (Sops) Applicable to Italian Hotspots. Available online: http://www.libertaciviliimmigrazione.dlci.interno.gov.it/sites/default/files/allegati/hotspots_sops_-_english_version.pdf (accessed on 10 September 2021).
- Ministry of Interior. Immigration Centers. Available online: https://www.interno.gov.it/it/temi/immigrazione-e-asilo/sistema-accoglienza-sul-territorio/centri-limmigrazione (accessed on 10 September 2021).
- Italian Ministry of Interior—Department for Civil Liberties and Immigration Data. Statistics on the Reception System for Migrants on 15th of March 2020. Available online: http://www.libertaciviliimmigrazione.dlci.interno.gov.it/sites/default/files/allegati/cruscotto_statistico_giornaliero_15-03-2020.pdf (accessed on 10 September 2021).
- Italian Ministry of Health. COVID-19. Update of Case Definition. Available online: https://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2020&codLeg=73669&parte=1%20&serie=null. (accessed on 10 September 2021).
- Ceccarelli, G.; Lopalco, M.; D’Ettorre, G.; Ciccozzi, M. Surveillance of COVID-19 in migrant reception centres: A call for action. J. Travel Med. 2021, 28, taaa171. [Google Scholar] [CrossRef] [PubMed]
- ISTAT. Popolazione e Famiglie. 2020. Available online: https://www.istat.it/it/files/2020/12/C03.pdf (accessed on 10 November 2021).
- Kondilis, E.; Papamichail, D.; McCann, S.; Carruthers, E.; Veizis, A.; Orcutt, M.; Hargreaves, S. The impact of the COVID-19 pandemic on refugees and asylum seekers in Greece: A retrospective analysis of national surveillance data from 2020. EClinical Med. 2021, 37, 100958. [Google Scholar] [CrossRef] [PubMed]
- Italian National Institute of Health (ISS). COVID-19 National Update. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sorveglianza-integrata-COVID-19_14-maggio-2020.pdf (accessed on 10 September 2021).
- Italian National Institute of Health. COVID-19 National Update. Available online: https://www.iss.it/documents/20126/0/Bollettino+sorveglianza+integrata+COVID-19_19+marzo+2020.pdf/e56791f7-820c-555e-8b0c-750c9db2883d?t=1584724596303 (accessed on 10 September 2021).
- Italian National Institute of Health. COVID-19 National Update. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sorveglianza-integrata-COVID-19_28-aprile-2020.pdf (accessed on 10 September 2021).
- Italian National Institute of Health. COVID-19 National Update. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sorveglianza-integrata-COVID-19_16-giugno-2020.pdf (accessed on 10 September 2021).
- ECDC Technical Report. Reducing COVID-19 Transmission and Strengthening Vaccine Uptake among Migrant Populations in the EU/EEA. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-reducing-transmission-and-strengthening-vaccine-uptake-in-migrants.pdf (accessed on 10 September 2021).
- Italian Ministry of Interior—Department for Civil Liberties and Immigration. Circular 3393. Available online: https://www.asgi.it/wp-content/uploads/2020/04/Circolare-prot.3393-del-18.3.20202.pdf (accessed on 12 August 2021).
- Italian National Institute for Health, Migration, and Poverty (INMP). Interim Operating Procedures for the Management of Facilities with Persons Who Are Highly Vulnerable and at High Risk of Health and Social Care Exclusion during the COVID-19 Epidemic. First Release: July 2020—Update: October 2020. Available online: https://www.inmp.it/eng/Publications/Books/Interim-operating-procedures-for-the-management-of-facilities-with-persons-who-are-highly-vulnerable-and-at-high-risk-of-health-and-social-care-exclusion-during-the-COVID-19-epidemic (accessed on 10 September 2021).


{kind=link}
| Region/AP | Total N of Facilities | Facilities Participating in the Survey | ||
|---|---|---|---|---|
| N | % (Of the Regional Amount) | % (Of Facilities Participating in the Survey) | ||
| Piedmont | 789 | 604 | 76.55 | 11.99 |
| Aosta Valley | 17 | 15 | 88.24 | 0.30 |
| Lombardy | 995 | 749 | 75.28 | 14.87 |
| Autonomous Province of Bolzano | 53 | 43 | 81.13 | 0.85 |
| Autonomous Province of Trento | 91 | 68 | 74.73 | 1.35 |
| Veneto | 476 | 343 | 72.06 | 6.81 |
| Friuli Venezia Giulia | 299 | 149 | 49.83 | 2.96 |
| Liguria | 328 | 217 | 66.16 | 4.31 |
| Emilia-Romagna | 990 | 855 | 86.36 | 16.97 |
| Tuscany | 475 | 275 | 57.89 | 5.46 |
| Umbria | 134 | 76 | 56.72 | 1.51 |
| Marche | 198 | 175 | 88.38 | 3.47 |
| Lazio | 552 | 459 | 83.15 | 9.11 |
| Abruzzo | 86 | 67 | 77.91 | 1.33 |
| Molise | 74 | 51 | 68.92 | 1.01 |
| Campania | 289 | 156 | 53.98 | 3.10 |
| Apulia | 264 | 204 | 77.27 | 4.05 |
| Basilicata | 122 | 99 | 81.15 | 1.97 |
| Calabria | 235 | 167 | 71.06 | 3.31 |
| Sicily | 295 | 212 | 71.86 | 4.21 |
| Sardinia | 75 | 54 | 72.00 | 1.07 |
| Macro-areas | ||||
| Northern Italy | 4038 | 3043 | - | 75.36 |
| Central Italy | 1359 | 985 | - | 72.48 |
| Southern Italy and Islands | 1440 | 1010 | - | 70.14 |
| p < 0.001 | ||||
| Total | 6837 | 5038 | 73.69 | 100.00 |
| Characteristics | N (%) |
|---|---|
| Participating facilities | 5038 (73.7) |
| Geographical distribution | |
| Northern Italy | 3043 (60.4) |
| Central Italy | 985 (19.6) |
| South and Islands | 1010 (20.1) |
| Typology | |
| First reception | |
| CAS | 3750 (74.4) |
| CARA | 4 (0.1) |
| Second reception | |
| SIPROIMI | 1210 (24) |
| SIPROIMI MSNA | 33 (0.7) |
| Others/unspecified | 41 (0.8) |
| Accommodation | |
| Shared room | 3450 (68.5) |
| Single room | 507 (10.1) |
| Mixed | 1081(21.5) |
| Average n. of guests (by centre) | 11.8 |
| First reception | |
| CAS | 15.9 |
| CARA | 418.5 |
| Second reception | |
| SIPROIMI | 6.3 |
| SIPROIMI MSNA | 13.8 |
| Others/unspecified | 37.8 |
| Facilities saturation index (%) (by geographical macro-area) | |
| Northern Italy | 86.4 |
| Central Italy | 84.3 |
| Southern Italy and Islands | 66.3 |
| p < 0.001 |
| Characteristics | N (%) |
|---|---|
| N | 59,648 |
| Geographical distribution | |
| Northern Italy | 30,471 (51.1) |
| Central Italy | 11,833 (19.8) |
| Southern Italy and Islands | 17,344 (29.1) |
| Most represented nationalities | |
| Nigeria | 16,207 (27.2) |
| Pakistan | 7040 (11.8) |
| Gambia | 4669 (7.8) |
| Bangladesh | 3715 (6.2) |
| Senegal | 3512 (5.9) |
| Reception System | Italian Resident Population | |||
|---|---|---|---|---|
| Cumulative Incidence per 100,000 | 95% CI | Cumulative Incidence per 100,000 | 95% CI | |
| Northern Italy | 774.51 | 676.08–872.94 | 690.98 | 687.89–694.07 |
| Central Italy | 16.90 | 0.00–40.32 | 222.03 | 219.35–224.72 |
| Southern Italy and Islands | 5.77 | 0.00–17.07 | 95.14 | 93.80–96.49 |
| Italy | 400.68 | 349.99–451.38 | 396.21 | 394.61–397.80 |
| Type of Facility | Confirmed Cases | Total Hosts |
|---|---|---|
| CAS | 197 | 48,294 |
| CARA | 0 | 1674 |
| SIPROIMI | 18 | 7676 |
| SIPROIMI MSNA | 0 | 454 |
| Others/Unspecified | 24 | 1550 |
| Total | 239 | 59,648 |
| Characteristics | N (%) |
|---|---|
| N | 239 (0.4) |
| Sex | |
| Male | 217 (90.8) |
| Female | 22 (9.2) |
| Class Age (years) | |
| 0–4 | 4 (1.7) |
| 10–14 | 0 |
| 15–19 | 2 (0.8) |
| 20–24 | 62 (25.9) |
| 25–29 | 77 (32.2) |
| 30–34 | 54 (22.6) |
| 35–39 | 20 (8.4) |
| 40–44 | 7 (2.9) |
| 45–49 | 8 (3.4) |
| 50–54 | 4 (1.7) |
| 60–64 | 1 (0.4) |
| Clinical appearance | |
| Symptomatic | 80 (33.5) |
| Asymptomatic | 159 (66.5) |
| Comorbidities | |
| Yes | 15 (6.3) |
| No | 224 (93.7) |
| Hospitalised cases | 62 (25.9) |
| With comorbidities | 7 (11.3) |
| Without comorbidities | 55 (88.7) |
| Non-hospitalised cases | 177 (74.1) |
| With comorbidities | 8 (4.5) |
| Without comorbidities | 169 (95.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sisti, L.G.; Di Napoli, A.; Petrelli, A.; Rossi, A.; Diodati, A.; Menghini, M.; Mirisola, C.; Costanzo, G. COVID-19 Impact in the Italian Reception System for Migrants during the Nationwide Lockdown: A National Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 12380. https://doi.org/10.3390/ijerph182312380
Sisti LG, Di Napoli A, Petrelli A, Rossi A, Diodati A, Menghini M, Mirisola C, Costanzo G. COVID-19 Impact in the Italian Reception System for Migrants during the Nationwide Lockdown: A National Observational Study. International Journal of Environmental Research and Public Health. 2021; 18(23):12380. https://doi.org/10.3390/ijerph182312380
Chicago/Turabian StyleSisti, Leuconoe Grazia, Anteo Di Napoli, Alessio Petrelli, Alessandra Rossi, Alessandra Diodati, Martina Menghini, Concetta Mirisola, and Gianfranco Costanzo. 2021. "COVID-19 Impact in the Italian Reception System for Migrants during the Nationwide Lockdown: A National Observational Study" International Journal of Environmental Research and Public Health 18, no. 23: 12380. https://doi.org/10.3390/ijerph182312380