
Attitudes of Patients with Cancer towards Vaccinations—Results of Online Survey with Special Focus on the Vaccination against COVID-19

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Statistical Analysis
3. Results
3.1. Study Population
3.2. General Attitudes and Opinions about Vaccinations
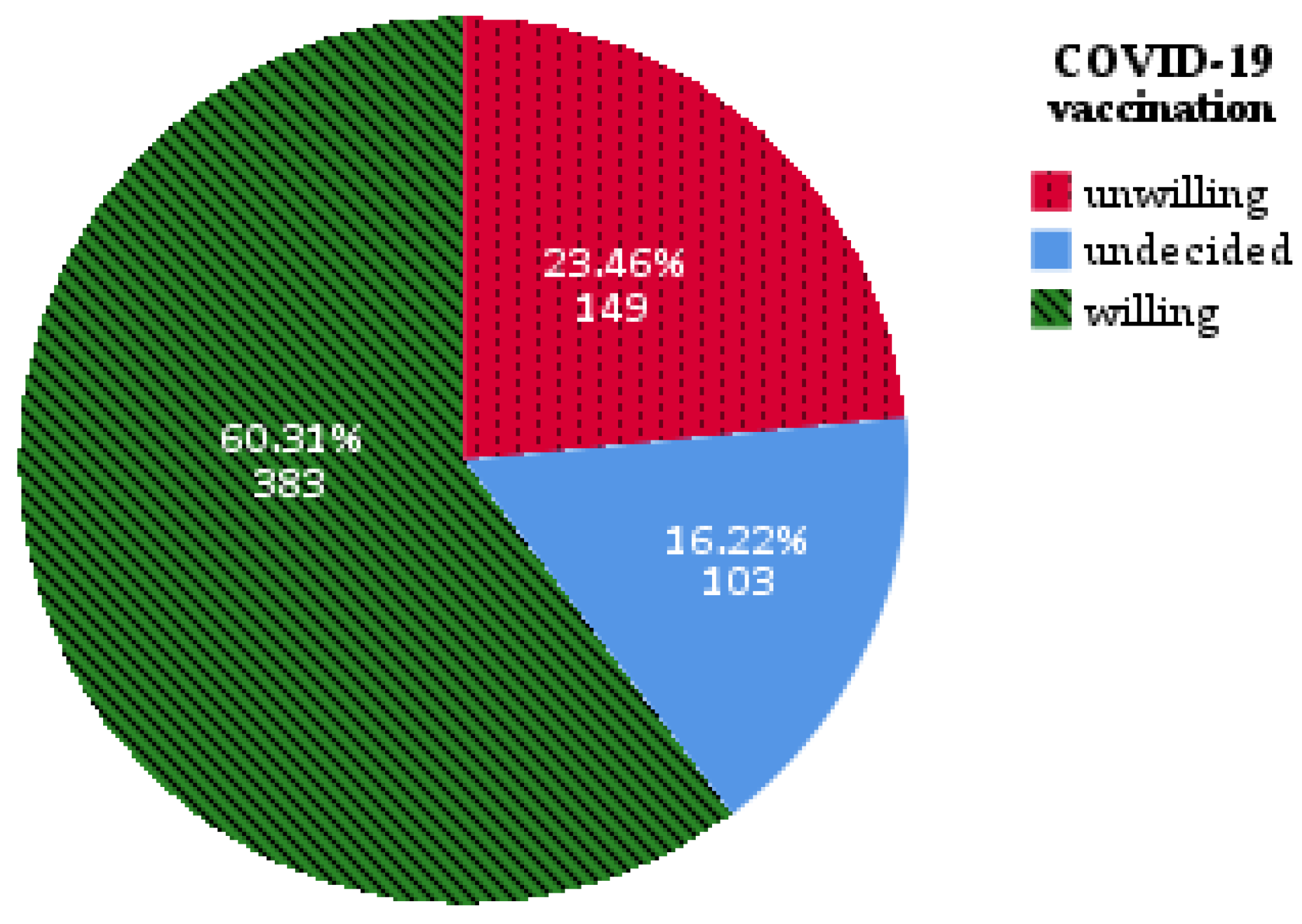
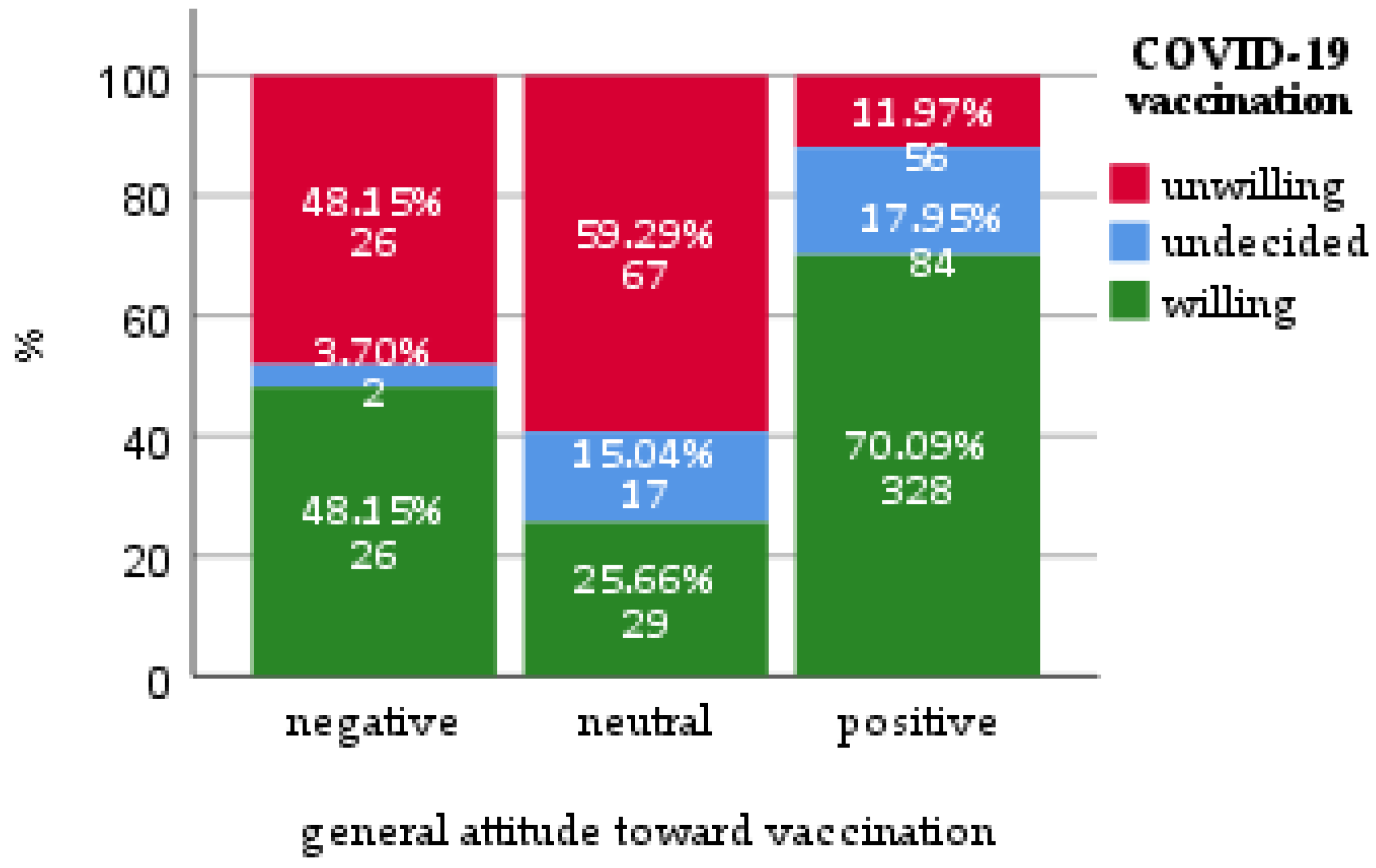
3.3. Attitudes and Opinions about COVID-19 Vaccination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Glatter, K.A.; Finkelman, P. History of the Plague: An Ancient Pandemic for the Age of COVID-19. Am. J. Med. 2021, 134, 176–181. [Google Scholar] [CrossRef]
- Riedel, S. Edward Jenner and the history of smallpox and vaccination. Proc. Bayl. Univ. Med. Cent. 2005, 18, 21–25. [Google Scholar] [CrossRef]
- Greenwood, B. The contribution of vaccination to global health: Past, present and future. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2014, 369, 20130433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaorsky, N.G.; Churilla, T.M.; Egleston, B.L.; Fisher, S.G.; Ridge, J.A.; Horwitz, E.M.; Meyer, J.E. Causes of death among cancer patients. Ann. Oncol. 2017, 28, 400–407. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Preliminary Recommendations of the NCCN COVID-19 Vaccination Advisory Committee* Version 2.0 3/10/2021. Available online: https://www.nccn.org/covid-19/pdf/COVID-19_Vaccination_Guidance_V2.0.pdf (accessed on 22 March 2021).
- Patt, D.; Gordan, L.; Diaz, M.; Okon, T.; Grady, L.; Harmison, M.; Markward, N.; Sullivan, M.; Peng, J.; Zhou, A. Impact of COVID-19 on Cancer Care: How the Pandemic Is Delaying Cancer Diagnosis and Treatment for American Seniors. JCO Clin. Cancer Inform. 2020, 4, 1059–1071. [Google Scholar] [CrossRef]
- Alzaid, E.H.; Alsaad, S.S.; Alshakhis, N.; Albagshi, D.; Albesher, R.; Aloqaili, M. Prevalence of COVID-19-related anxiety among healthcare workers: A cross-sectional study. J. Fam. Med. Prim. Care 2020, 9, 4904–4910. [Google Scholar] [CrossRef]
- Sigorski, D.; Sobczuk, P.; Osmola, M.; Kuc, K.; Walerzak, A.; Wilk, M.; Ciszewski, T.; Kopec, S.; Hryn, K.; Rutkowski, P.; et al. Impact of COVID-19 on anxiety levels among patients with cancer actively treated with systemic therapy. ESMO Open 2020, 5, e000970. [Google Scholar] [CrossRef]
- Bandyopadhyay, S.; Baticulon, R.E.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y.; Kamath, A.; Parepalli, S.A.; Brown, G.; Iharchane, S.; et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob. Health 2020, 5. [Google Scholar] [CrossRef]
- Wysocki, P.J.; Kwinta, Ł.; Potocki, P.; Konopka, K.; Streb, J.; Wojtukiewicz, M.Z.; Radecka, B.; Tomczak, P.; Jarząb, M.; Kawecki, A.; et al. Systemic treatment of patients with solid tumors during the COVID-19 (SARS-CoV-2) pandemic—Comprehensive recommendations of the Polish Society of Clinical Oncology. Oncol. Clin. Pract. 2020, 16, 41–51. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.; Gainor, J.F.; Hegde, A.; Schram, A.M.; Curigiliano, G.; Pal, S.; Liu, S.V.; Halmos, B.; Groisberg, R.; Grande, E.; et al. COVID-19 vaccine guidance for patients with cancer participating in oncology clinical trials. Nat. Rev. Clin. Oncol. 2021, 15, 1–7. [Google Scholar] [CrossRef]
- Saini, K.S.; Tagliamento, M.; Lambertini, M.; McNally, R.; Romano, M.; Leone, M.; Curigliano, G.; de Azambuja, E. Mortality in patients with cancer and coronavirus disease 2019: A systematic review and pooled analysis of 52 studies. Eur. J. Cancer 2020, 139, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Grivas, P.; Khaki, A.R.; Wise-Draper, T.M.; French, B.; Hennessy, C.; Hsu, C.Y.; Shyr, Y.; Li, X.; Choueiri, T.K.; Painter, C.A.; et al. Association of Clinical Factors and Recent Anti-Cancer Therapy with COVID-19 Severity among Patients with Cancer: A Report from the COVID-19 and Cancer Consortium. Ann. Oncol. 2021, 19. [Google Scholar] [CrossRef]
- Ribas, A.; Sengupta, R.; Locke, T.; Zaidi, S.K.; Campbell, K.M.; Carethers, J.M.; Jaffee, E.M.; Wherry, E.J.; Soria, J.C.; D’Souza, G.; et al. Priority COVID-19 Vaccination for Patients with Cancer while Vaccine Supply Is Limited. Cancer Discov. 2021, 11, 233–236. [Google Scholar] [CrossRef]
- Marra, A.; Generali, D.; Zagami, P.; Cervoni, V.; Gandini, S.; Venturini, S.; Morganti, S.; Passerini, R.; Orecchia, R.; Curigliano, G. Seroconversion in patients with cancer and oncology health care workers infected by SARS-CoV-2. Ann. Oncol. 2021, 32, 113–119. [Google Scholar] [CrossRef]
- Garassino, M.C.; Vyas, M.; de Vries, E.G.E.; Kanesvaran, R.; Giuliani, R.; Peters, S.; European Society for Medical Oncology. The ESMO Call to Action on COVID-19 vaccinations and patients with cancer: Vaccinate. Monitor. Educate. Ann. Oncol. 2021, 32, 579–581. [Google Scholar] [CrossRef]
- Smith, L.E.; Amlot, R.; Weinman, J.; Yiend, J.; Rubin, G.J. A systematic review of factors affecting vaccine uptake in young children. Vaccine 2017, 35, 6059–6069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobson, R.M.; St Sauver, J.L.; Rutten, L.J.F. Vaccine Hesitancy. Mayo Clin. Proc. 2015, 90, 1562–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalski, J.; Marchlewska, M.; Molenda, Z.; Gorska, P.; Gaweda, L. Adherence to safety and self-isolation guidelines, conspiracy and paranoia-like beliefs during COVID-19 pandemic in Poland—Associations and moderators. Psychiatry Res. 2020, 294, 113540. [Google Scholar] [CrossRef]
- Freeman, D.; Waite, F.; Rosebrock, L.; Petit, A.; Causier, C.; East, A.; Jenner, L.; Teale, A.L.; Carr, L.; Mulhall, S.; et al. Coronavirus conspiracy beliefs, mistrust, and compliance with government guidelines in England. Psychol. Med. 2020, 1–13. [Google Scholar] [CrossRef]
- Kelkar, A.H.; Blake, J.A.; Cherabuddi, K.; Cornett, H.; McKee, B.L.; Cogle, C.R. Vaccine Enthusiasm and Hesitancy in Cancer Patients and the Impact of a Webinar. Healthcare 2021, 9, 351. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- McAteer, J.; Yildirim, I.; Chahroudi, A. The VACCINES Act: Deciphering Vaccine Hesitancy in the Time of COVID-19. Clin. Infect. Dis. 2020, 71, 703–705. [Google Scholar] [CrossRef] [PubMed]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to vaccination: A critical review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Health Eur. 2021, 1. [Google Scholar] [CrossRef]
- Barriere, J.; Gal, J.; Hoch, B.; Cassuto, O.; Leysalle, A.; Chamorey, E.; Borchiellini, D. Acceptance of SARS-CoV-2 vaccination among French patients with cancer: A cross-sectional survey. Ann. Oncol. 2021, 32, 673–674. [Google Scholar] [CrossRef] [PubMed]
- Ariza-Heredia, E.J.; Azzi, J.; Shah, D.P.; Nesher, L.; Ghantoji, S.S.; Michailidis, L.; Marsh, L.; Chemaly, R.F. Influenza vaccination in patients with cancer: Factors associated with vaccination practices for patients and their household members. Infect Control Hosp. Epidemiol. 2015, 36, 1239–1241. [Google Scholar] [CrossRef]
- Loulergue, P.; Mir, O.; Alexandre, J.; Ropert, S.; Goldwasser, F.; Launay, O. Low influenza vaccination rate among patients receiving chemotherapy for cancer. Ann. Oncol. 2008, 19, 1658. [Google Scholar] [CrossRef]
- Poeppl, W.; Lagler, H.; Raderer, M.; Sperr, W.R.; Zielinski, C.; Herkner, H.; Burgmann, H. Influenza vaccination perception and coverage among patients with malignant disease. Vaccine 2015, 33, 1682–1687. [Google Scholar] [CrossRef]
- Vollaard, A.; Schreuder, I.; Slok-Raijmakers, L.; Opstelten, W.; Rimmelzwaan, G.; Gelderblom, H. Influenza vaccination in adult patients with solid tumours treated with chemotherapy. Eur. J. Cancer 2017, 76, 134–143. [Google Scholar] [CrossRef]
- Vinograd, I.; Baslo, R.; Eliakim-Raz, N.; Farbman, L.; Taha, A.; Sakhnini, A.; Lador, A.; Stemmer, S.M.; Gafter-Gvili, A.; Fraser, D.; et al. Factors associated with influenza vaccination among adult cancer patients: A case-control study. Clin. Microbiol. Infect. 2014, 20, 899–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akin, S.; Dizdar, O.; Karakas, Y.; Ozisik, L.; Tanriover, M.D.; Kamisli, S.; Erman, M.; Hayran, M. Vaccination perception and attitudes among patients with cancer receiving chemotherapy. Ann. Oncol. 2016, 27, vi514. [Google Scholar] [CrossRef]
- Soares, P.; Rocha, J.V.; Moniz, M.; Gama, A.; Laires, P.A.; Pedro, A.R.; Dias, S.; Leite, A.; Nunes, C. Factors Associated with COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef] [PubMed]
- Urun, Y.; Akbulut, H.; Demirkazik, A.; Senler, F.C.; Utkan, G.; Onur, H.; Icli, F. Perception about influenza and pneumococcal vaccines and vaccination coverage among patients with malignancies and their family members. J. BUON 2013, 18, 511–515. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Parameter | Study Population n (%), n = 635 |
|---|---|---|
| Age | Median years (range) | 53 (18–89) |
| Gender | Male | 124 (19.5) |
| Female | 509 (80.2) | |
| Do not want to provide information | 2 (0.3) | |
| Place of residence | Village | 141 (22.2) |
| City < 50,000 inhabitants | 182 (28.7) | |
| City 50,000–100,000 inhabitants | 73 (11.5) | |
| City > 100,000 inhabitants | 239 (37.6) | |
| Education | Primary | 13(2.0) |
| Vocational | 65 (10.2) | |
| Secondary | 253(39.8) | |
| Higher | 296 (46.8) | |
| Do not want to provide information | 8 (1.3) | |
| Occupational situation | Professionally active | 295 (46.5) |
| Retired | 181 (28.5) | |
| On a disability pension | 77 (12.1) | |
| Unemployed | 54 (8.5) | |
| Student | 15 (2.4) | |
| Do not want to provide information | 13 (2.0) | |
| Marital status | In a relationship | 452 (71.2) |
| Single | 61 (9.6) | |
| Divorced | 58 (9.1) | |
| Widow/widower | 58 (7.1) | |
| Do not want to provide information | 16 (2.5) | |
| Cancer type | Breast cancer | 295 (46.5) |
| Gastrointestinal cancers | 71 (11.2) | |
| Urogenital cancers | 56 (8.8) | |
| Hematological | 51 (8.0) | |
| Gynecological | 49 (7.7) | |
| Sarcoma | 38 (6.0) | |
| Thoracic tumors | 38 (6.0) | |
| Head and neck cancers | 18 (2.8) | |
| Melanoma | 11 (1.7) | |
| Other | 8 (1.3) | |
| Active anti-cancer treatment | 393 (61.9) | |
| How do you evaluate your health in comparison to your peers? | Very good | 73 (11.5) |
| Good | 264 (41.6) | |
| Medium | 227 (35.7) | |
| Bad | 63 (9.9) | |
| Very bad | 8 (1.3) | |
| Comorbidities | Overall | 388 (61.1) |
| Comobidities | Cardiovascular diseases | 233 (36.7) |
| Respiratory tract disease | 61 (9.6) | |
| Autoimmune diseases | 86 (13.5) | |
| Neurological diseases | 28 (4.4), | |
| Allergies | 171 (26.9) | |
| History of COVID-19 infection | 100 (15.7) | |
| COVID-19 hospitalization | 5 (0.9%) | |
| Know someone who suffered from COVID-19 | 317 (49.9) | |
| Know someone who died of COVID-19 | 98 (15.4) | |
| Wearing mask or face shield | 610 (96.1) | |
| Pandemic recommendations compliance (washing hands etc.) | 612 (96.4) | |
| The main source of information about the world: | Websites | 281 (44.3) |
| TV and radio | 230 (36.2) | |
| Social media | 54 (8.5) | |
| Professional literature | 47 (7.4) | |
| Press | 14 (2.2) | |
| Friends and family | 9 (1.4) | |
| Source of information about vaccinations (multiple choice): | TV and radio | 316 (49.8) |
| Websites | 286 (45.0) | |
| Social media | 134 (21.1) | |
| Physician | 122 (20.9) | |
| Scientific Guidelines | 125 (19.7) | |
| Professional literature | 109 (17.2) | |
| Friends/family | 78 (12.3) | |
| Press | 63 (9.9) | |
| Patient’s organizations articles | 58 (9.1) | |
| TV use | I do not watch TV | 100 (15.7) |
| Less than one hour | 99 (15.6) | |
| Between 1 and 2 h | 195 (30.7) | |
| Between 2 and 4 h | 167 (26.3) | |
| More than 4 h | 74 (11.7) | |
| Internet use | I do not use the Internet | 51 (8.0) |
| Less than one hour | 87 (13.7) | |
| Between 1 and 2 h | 262 (41.3) | |
| Between 2 and 4 h | 175 (27.6) | |
| More than 4 h | 60 (9.4) | |
| Social media use | Yes, everyday | 432 (68.0) |
| Yes, several times a week | 88 (13.9) | |
| Yes, but less than once a week | 19 (3.0) | |
| No | 96 (15.1) | |
| Question | Answer n (%), n = 635 | ||
|---|---|---|---|
| Disagree (Likert Scale 1–2) | Neither Disagree Nor Agree (Likert Scale 3) | Agree (Likert Scale 4–5) | |
| Thanks to preventive vaccinations many dangerous diseases are practically non-existent today. | 43 (6.8) | 59 (9.3) | 533 (83.9) |
| Vaccinations are the most effective way to protect against serious infectious diseases. | 48 (7.6) | 59 (9.3) | 528 (83.1) |
| Vaccinations are safe. | 66 (10.4) | 117 (18.4) | 452 (71.2) |
| Before vaccination, patients are adequately informed about the side effects. | 171 (26.9) | 162 (25.5) | 302 (47.6) |
| Vaccinations are promoted not because they are really needed but because it is in the interests of pharmaceutical companies. | 334 (52.6) | 147 (23.1) | 154 (24.3) |
| Vaccinations in children can cause serious developmental disorders, e.g., autism. | 368 (58.0) | 134 (21.1) | 133 (20.9) |
| Vaccinations have more advantages than disadvantages. | 76 (12.0) | 109 (17.2) | 450 (70.9) |
| Factor | Negative Attitude towards Vaccination | Neutral Attitude towards Vaccination | ||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Female (ref. male) | 3.69 | 0.83–16.33 | 2.24 | 0.92–5.43 |
| Age (ref. ≤44) | ||||
| 45–64 | 0.93 | 0.32–2.73 | 0.74 | 0.38–1.44 |
| 65+ | 0.17 | 0.03–1.12 | 0.42 | 0.11–1.61 |
| Education (ref. secondary) | ||||
| primary | 14.09 | 1.29–153.61 | 3.20 | 0.68–15.06 |
| basic vocational | 1.97 | 0.55–7.11 | 1.17 | 0.47–2.91 |
| higher | 0.26 | 0.10–0.68 | 0.78 | 0.43–1.40 |
| Place of living (ref. village) | ||||
| city < 50,000 inhabitants | 1.91 | 0.65–5.61 | 0.88 | 0.45–1.71 |
| city 50,000–100,000 inhabitants | 0.71 | 0.14–3.71 | 0.68 | 0.28–1.61 |
| city > 100,000 inhabitants | 1.19 | 0.39–3.64 | 0.29 | 0.14–0.59 |
| Marital status (re. single) | ||||
| in a relationship | 2.48 | 0.67–10.77 | 1.08 | 0.49–2.35 |
| widow/widower | 3.27 | 0.42–25.62 | 2.33 | 0.67–8.16 |
| divorced | 4.48 | 0.74–27.28 | 1.93 | 0.63–5.85 |
| Occupational status (ref. professionally active) | ||||
| retired | 2.30 | 0.65–8.01 | 0.53 | 0.19–1.53 |
| on a disability pension | 1.22 | 0.34–4.36 | 1.07 | 0.47–2.45 |
| unemployed | 3.51 | 1.06–11.62 | 2.21 | 0.93–5.21 |
| studying | 0.57 | 0.4–8.2 | 2.67 | 0.66–10.80 |
| Main source of information (ref. radio and TV) | ||||
| Internet services | 1.95 | 0.65–5.90 | 1.21 | 0.59–2.47 |
| Social media | 1.36 | 0.30–6.18 | 1.25 | 0.43–3.63 |
| Friends and family | 4.84 | 0.22–107.29 | 1.12 | 0.11–11.20 |
| Specialistic literature | 16.00 | 2.77–92.44 | 3.60 | 1.11–11.63 |
| Time spent watching TV (ref. 1–2 h) | ||||
| I do not watch TV | 1.13 | 0.34–3.78 | 1.85 | 0.83–4.12 |
| Less than one hour | 0.55 | 0.17–1.81 | 0.75 | 0.35–1.61 |
| Between 2 and 4 h | 0.57 | 0.19–1.72 | 0.51 | 0.25–1.03 |
| More than 4 h | 0.45 | 0.1–2.06 | 0.33 | 0.12–0.96 |
| Time spent surfing the Internet (ref. 1–2 h) | ||||
| I do not watch TV | 4.60 | 0.34–62.02 | 1.26 | 0.33–4.75 |
| Less than one hour | 1.02 | 0.28–3.75 | 0.92 | 0.43–2.00 |
| Between 2 and 4 h | 0.62 | 0.24–1.61 | 0.59 | 0.31–1.15 |
| More than 4 h | 0.97 | 0.24–3.95 | 1.30 | 0.51–3.30 |
| Use of social media (ref. few times a week) | ||||
| everyday | 1.04 | 2.95–3.69 | 0.68 | 0.32–1.43 |
| less than once a week | 0.38 | 0.02–6.31 | 1.10 | 0.24–5.04 |
| no | 0.25 | 0.02–3.32 | 1.00 | 0.33–3.05 |
| Use of articles from patients’ organizations as a source of information about vaccinations (ref. No) | 1.17 | 0.26–5.16 | 0.67 | 0.24–1.88 |
| Use of radio and TV as a source of information about vaccinations (ref. No) | 0.68 | 0.25–1.85 | 0.95 | 0.48–1.89 |
| Use of Internet about vaccinations (ref. No) | 1.20 | 0.52–2.78 | 0.68 | 0.38–1.20 |
| Physician as a source of information about vaccinations (ref. No) | 0.14 | 0.03–0.61 | 0.34 | 0.16–0.74 |
| Scientific Literature as a source of information about vaccinations (ref. No) | 0.97 | 0.31–3.06 | 0.43 | 0.19–1.01 |
| Guidelines as a source of information about vaccinations (ref. No) | 0.14 | 0.03–0.60 | 0.4 | 0.19–0.86 |
| Friends and family as a source of information about vaccinations (ref. No) | 1.00 | 0.23–4.26 | 2.27 | 1.08–4.80 |
| Social media as a source of information about vaccinations (ref. No) | 2.60 | 1.02–6.64 | 0.89 | 0.44–1.78 |
| Press as a source of information about vaccinations (ref. No) | 0.66 | 0.10–4.24 | 1.02 | 0.39–2.66 |
| General assessment of personal health (ref. very good) | ||||
| Good | 1.12 | 0.33–3.81 | 0.98 | 0.43–2.22 |
| Medium | 0.76 | 0.21–2.80 | 0.74 | 0.31–1.75 |
| Bad | 1.46 | 0.31–6.90 | 0.49 | 0.15–1.56 |
| Very bad | 1.53 | 0.10–23.8 | 0.76 | 0.06–9.00 |
| Concomitant diseases (ref. No) | 0.65 | 0.28–1.52 | 0.95 | 0.55–1.64 |
| Active anticancer treatment (ref. No) | 1.27 | 0.54–2.99 | 1.10 | 0.62–1.95 |
| Cancer type (Ref. gastrointestinal) | ||||
| Melanoma and skin cancer | 0.96 | 0.08–11.62 | 1.44 | 0.21–9.70 |
| Sarcoma | 2.90 | 0.44–19.10 | 1.84 | 0.50–6.75 |
| Gynecological | 0.95 | 0.16–5.59 | 0.70 | 0.19–2.53 |
| Head and neck | NA | NA | 0.39 | 0.06–2.45 |
| Hematological | 1.17 | 0.17–8.23 | 0.70 | 0.18–2.69 |
| Genitourinary | 0.53 | 0.06–4.43 | 1.18 | 0.39–3.60 |
| Respiratory tract | 1.24 | 0.20–7.48 | 0.76 | 0.19–3.01 |
| Breast | 0.36 | 0.08–1.64 | 0.68 | 0.25–1.86 |
| Other | 1.72 | 0.05–64.21 | 1.27 | 0.09–17.74 |
| Question | Answer n (%), n = 635 | ||
|---|---|---|---|
| Disagree (Likert Scale 1–2) | Neither Disagree Nor Agree (Likert Scale 3) | Agree (Likert Scale 4–5) | |
| I am afraid of the vaccine’s side effects. | 198 (31.2) | 153 (24.1) | 284 (44.7) |
| I have concerns about the effectiveness of the vaccine. | 235 (37.0) | 118 (18.6) | 282 (44.4) |
| I am afraid of the composition of the vaccine. | 284 (44.7) | 112 (17.6) | 239 (37.6) |
| The vaccine was developed too rapidly. | 239 (37.6) | 102 (16.1) | 294 (46.3) |
| The vaccine contains bodies of aborted children. | 502 (79.1) | 84 (13.2) | 49 (7.7) |
| Religious reasons prevent me from vaccination. | 592 (93.2) | 23 (3.6) | 20 (3.1) |
| Coronavirus does not exist, so I do not need to get vaccinated. | 541 (85.2) | 52 (8.2) | 42 (6.6) |
| I do not need to get vaccinated because I believe that the risk of getting sick in my case is low because I adhere to the recommendations of isolation and have no contact with other people. | 470 (74.0) | 92 (14.5) | 73 (11.5) |
| I believe that patients in active cancer treatment should get vaccinated first. | 109 (17.2) | 101 (15.9) | 425 (66.9) |
| I believe that COVID-19 vaccination should be mandatory. | 232 (36.5) | 113 (17.8) | 290 (45.7) |
| I am sufficiently informed about the possibilities and safety of the vaccination in cancer patients. | 243 (38.3) | 130 (20.5) | 262 (41.3) |
| I believe that cancer patients should not get vaccinated against COVID-19 | 419 (66.0) | 122 (19.2) | 94 (14.8) |
| Factor | Unwilling to Vaccinate against COVID-19 | Undecided to Vaccinate against COVID-19 | ||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Female (ref. male) | 2.62 | 1.01–6.80 | 0.93 | 0.39–2.22 |
| Age (ref. ≤44) | ||||
| 45–64 | 0.58 | 0.28–1.18 | 0.54 | 0.25–1.15 |
| 65+ | 0.22 | 0.06–0.82 | 0.27 | 0.07–1.04 |
| Education (ref. secondary) | ||||
| primary | 0.76 | 0.08–7.29 | 1.72 | 0.37–7.97 |
| basic vocational | 1.32 | 0.55–3.15 | 0.33 | 0.11–1.01 |
| higher | 0.45 | 0.24–0.83 | 0.75 | 0.40–1.41 |
| Place of living (ref. village) | ||||
| city < 50,000 inhabitants | 2.01 | 0.96–4.20 | 0.70 | 0.33–1.51 |
| city 50,000–100,000 inhabitants | 0.69 | 0.25–1.95 | 0.84 | 0.34–2.06 |
| city > 100,000 inhabitants | 1.16 | 0.54–2.47 | 0.83 | 0.41–1.71 |
| Marital status (re. single) | ||||
| in a relationship | 0.44 | 0.19–1.00 | 0.51 | 0.21–1.26 |
| widow/widower | 0.23 | 0.06–0.89 | 0.40 | 0.10–1.57 |
| divorced | 0.20 | 0.06–0.66 | 0.11 | 0.02–0.48 |
| Occupational status (ref. professionally active) | ||||
| retired | 1.39 | 0.54–3.57 | 0.95 | 0.35–2.59 |
| on a disability pension | 0.75 | 0.31–1.79 | 0.82 | 0.34–1.97 |
| Unemployed | 0.77 | 0.31–1.94 | 0.38 | 0.12–1.18 |
| studying | 0.40 | 0.07–2.21 | NA | NA |
| Main source of information (ref. radio and TV) | ||||
| Internet services | 0.95 | 0.45–2.00 | 0.73 | 0.35–1.54 |
| social media | 0.52 | 0.18–1.51 | 0.57 | 0.18–1.84 |
| Friends and family | 0.70 | 0.06–8.50 | 0.44 | 0.03–5.78 |
| Specialistic literature | 2.45 | 0.76–8.16 | 0.95 | 0.26–3.46 |
| Press | 0.76 | 0.10–5.96 | 1.29 | 0.25–6.52 |
| Time spent watching TV (ref. 1–2 h) | ||||
| I do not watch TV | 1.28 | 0.53–3.08 | 0.36 | 0.13–0.99 |
| Less than one hour | 2.13 | 0.92–4.94 | 0.78 | 0.34–1.82 |
| Between 2 and 4 h | 2.54 | 1.19–5.42 | 0.80 | 0.40–1.60 |
| More than 4 h | 1.73 | 0.61–4.90 | 0.88 | 0.35–2.21 |
| Time spent surfing the Internet (ref. 1–2 h) | ||||
| I do not watch TV | 0.40 | 0.08–1.84 | 1.72 | 0.47–2.27 |
| Less than one hour | 0.66 | 0.27–1.60 | 1.08 | 0.45–2.61 |
| Between 2 and 4 h | 0.81 | 0.41–1.56 | 1.02 | 0.53–1.97 |
| More than 4 h | 0.73 | 0.28–1.87 | 0.78 | 0.26–2.35 |
| Use of social media (ref. few times a week) | ||||
| everyday | 1.06 | 0.46–2.44 | 1.69 | 0.71–4.01 |
| less than once a week | 0.89 | 0.16–4.90 | 0.52 | 0.08–3.42 |
| No | 0.89 | 0.26–3.10 | 1.04 | 0.32–3.35 |
| Use of articles from patients’ organizations as a source of information about vaccinations (ref. No) | 0.85 | 0.31–2.36 | 0.66 | 0.29–2.17 |
| Use of radio and TV as a source of information about vaccinations (ref. No) | 0.74 | 0.36–1.50 | 0.92 | 0.45–1.88 |
| Use of Internet about vaccinations (ref. No) | 1.19 | 0.66–2.14 | 1.05 | 0.57–1.94 |
| Physician as a source of information about vaccinations (ref. No) | 0.80 | 0.37–1.71 | 0.98 | 0.49–1.96 |
| Scientific Literature as a source of information about vaccinations (ref. No) | 0.51 | 0.22–1.18 | 0.55 | 0.23–1.32 |
| Guidelines as a source of information about vaccinations (ref. No) | 0.91 | 0.68–3.53 | 1.00 | 0.46–2.17 |
| Friends and family as a source of information about vaccinations (ref. No) | 1.55 | 0.68–3.53 | 1.90 | 0.85–4.25 |
| Social media as a source of information about vaccinations (ref. No) | 1.42 | 0.72–2.80 | 1.06 | 0.52–2.19 |
| Press as a source of information about vaccinations (ref. No) | 0.99 | 0.36–2.77 | 0.61 | 0.24–1.57 |
| General assessment of personal health (ref. very good) | ||||
| Good | 0.66 | 0.28–1.55 | 1.59 | 0.60–4.20 |
| Medium | 1.25 | 0.52–3.02 | 1.83 | 0.67–5.00 |
| Bad | 0.80 | 0.25–2.54 | 3.54 | 1.08–11.55 |
| Very bad | 1.92 | 0.24–15.57 | NA | NA |
| Concomitant diseases (ref. No) | 1.10 | 0.62–1.97 | 1.14 | 0.65–2.00 |
| Active anticancer treatment (ref. No) | 0.83 | 0.45–1.53 | 0.38 | 0.21–0.71 |
| Cancer type (Ref. gastrointestinal) | ||||
| Melanoma and skin cancer | 0.67 | 0.08–5.52 | 1.91 | 0.23–16.24 |
| Sarcoma | 1.06 | 0.26–4.27 | 0.59 | 0.12–2.83 |
| Gynecological | 0.34 | 0.10–1.18 | 0.50 | 0.12–2.05 |
| Head and neck | 0.42 | 0.06–3.17 | 1.30 | 0.27–6.32 |
| Hematological | 0.36 | 0.09–1.42 | 0.55 | 0.13–2.22 |
| Genitourinary | 0.66 | 0.19–2.32 | 0.98 | 0.32–2.97 |
| Respiratory tract | 1.15 | 0.30–3.38 | 2.47 | 0.76–8.04 |
| Breast | 0.45 | 0.17–1.20 | 0.67 | 0.24–1.86 |
| Other | NA | NA | 0.26 | 0.02–4.46 |
| Had COVID-19 infection (Ref. No) | 2.03 | 0.99–4.11 | 0.83 | 0.36–1.9– |
| Know somebody who had COVID-19 infection (Ref. No) | 0.69 | 0.37–1.32 | 0.50 | 0.26–0.96 |
| Know somebody who died of COVID-19 (Ref. No) | 1.53 | 0.69–3.40 | 1.30 | 0.57–2.98 |
| Vaccination against influenza (Ref. never) | ||||
| regularly every year | 0.28 | 0.09–0.91 | 0.46 | 0.18–1.17 |
| not regularly | 0.36 | 0.19–0.70 | 0.61 | 0.33–1.11 |
| General attitude towards vaccination (Ref. positive) | ||||
| Negative | 3.25 | 1.41–7.50 | 0.28 | 0.06–1.38 |
| Neutral | 13.34 | 6.80–26.17 | 1.99 | 0.90–4.39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brodziak, A.; Sigorski, D.; Osmola, M.; Wilk, M.; Gawlik-Urban, A.; Kiszka, J.; Machulska-Ciuraj, K.; Sobczuk, P. Attitudes of Patients with Cancer towards Vaccinations—Results of Online Survey with Special Focus on the Vaccination against COVID-19. Vaccines 2021, 9, 411. https://doi.org/10.3390/vaccines9050411
Brodziak A, Sigorski D, Osmola M, Wilk M, Gawlik-Urban A, Kiszka J, Machulska-Ciuraj K, Sobczuk P. Attitudes of Patients with Cancer towards Vaccinations—Results of Online Survey with Special Focus on the Vaccination against COVID-19. Vaccines. 2021; 9(5):411. https://doi.org/10.3390/vaccines9050411
Chicago/Turabian StyleBrodziak, Anna, Dawid Sigorski, Małgorzata Osmola, Michał Wilk, Angelika Gawlik-Urban, Joanna Kiszka, Katarzyna Machulska-Ciuraj, and Paweł Sobczuk. 2021. "Attitudes of Patients with Cancer towards Vaccinations—Results of Online Survey with Special Focus on the Vaccination against COVID-19" Vaccines 9, no. 5: 411. https://doi.org/10.3390/vaccines9050411