
A COVID-19 Patient with Simultaneous Renal Infarct, Splenic Infarct and Aortic Thrombosis during the Severe Disease

Abstract
:1. Introduction
2. Case Description
Clinical Follow-Up
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Gandet, F.F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.K.; Mainbourg, S.; Friggeri, A.; Bertoletti, L.; Douplat, M.; Dargaud, Y.; Grange, C.; Lobbes, H.; Provencher, S.; Lega, J.C. Arterial and venous thromboembolism in COVID-19: A study-level meta-analysis. Thorax 2021, 76, 970–979. [Google Scholar] [CrossRef] [PubMed]
- Avila, J.; Long, B.; Holladay, D.; Gottlieb, M. Thrombotic complications of COVID-19. Am. J. Emerg. Med. 2021, 39, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Lodigiani, C.; Iapichino, G.; Carenzo, L.; Cecconi, M.; Ferrazzi, P.; Sebastian, T.; Kucher, N.; Studt, J.D.; Sacco, C.; Bertuzzi, A.; et al. Humanitas COVID-19 Task Force. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb. Res. 2020, 191, 9–14. [Google Scholar] [CrossRef]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological findings and complications of COVID-19. Am. J. Hematol. 2020, 95, 834–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Nigoghossian, C.D.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 2950–2973. [Google Scholar] [CrossRef]
- de Carranza, M.; Salazar, D.E.; Troya, J.; Alcázar, R.; Peña, C.; Aragón, E.; Domínguez, M.; Torres, J.; Muñoz-Rivas, N. Aortic thrombus in patients with severe COVID-19: Review of three cases. J. Thromb. Thrombolysis 2021, 51, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Diao, B.; Feng, Z.; Wang, C.; Wang, H.; Liu, L.; Wang, C.; Wang, R.; Liu, Y.; Liu, Y.; Wang, G.; et al. Human kidney is a target for novel severe acute respiratory syndrome coronavirus 2 infection. Nat. Commun. 2021, 12, 2506. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Reis, T. Kidney involvement in COVID-19 and rationale for extracorporeal therapies. Nat. Rev. Nephrol. 2020, 16, 308–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silversides, J.A.; Major, E.; Ferguson, A.J.; Mann, E.E.; McAuley, D.F.; Marshall, J.C.; Blackwood, B.; Fan, E. Conservative fluid management or deresuscitation for patients with sepsis or acute respiratory distress syndrome following the resuscitation phase of critical illness: A systematic review and meta-analysis. Intensive Care Med. 2017, 43, 155–170. [Google Scholar] [CrossRef] [Green Version]
- Post, A.; den Deurwaarder, E.S.; Bakker, S.J.; de Haas, R.J.; van Meurs, M.; Gansevoort, R.T.; Berger, S.P. Kidney Infarction in Patients With COVID-19. Am. J. Kidney Dis. 2020, 76, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, A.; Ghosh, R.; Furment, M.M. Case Report: COVID-19 Associated Renal Infarction and Ascending Aortic Thrombosis. Am. J. Trop. Med. Hyg. 2020, 103, 1989–1992. [Google Scholar] [CrossRef] [PubMed]
- Caravaca-Fontán, F.; Saico, S.P.; Triviño, S.E.; Álvarez, C.G.; Couto, A.G.; de las Heras, I.P.; Liaño, F. Acute renal infarction: Clinical characteristics and prognostic factors. Nefrologia 2016, 36, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Faucon, A.L.; Bobrie, G.; Jannot, A.S.; Azarine, A.; Plouin, P.F.; Azizi, M.; Amar, L. Cause of renal infarction: A retrospective analysis of 186 consecutive cases. J. Hypertens. 2018, 36, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, D.; Menes, T.; Rimon, U.; Salomon, O.; Halak, M. Acute renal artery occlusion: Presentation, treatment, and outcome. J. Vasc. Surg. 2016, 64, 1026–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besutti, G.; Bonacini, R.; Iotti, V.; Marini, G.; Riva, N.; Dolci, G.; Maiorana, M.; Spaggiari, L.; Monelli, F.; Ligabue, G.; et al. Abdominal Visceral Infarction in 3 Patients with COVID-19. Emerg. Infect. Dis. 2020, 26, 1926–1928. [Google Scholar] [CrossRef]
- O’Donnell, M.; Shatzel, J.J.; Olson, S.R.; Daughety, M.M.; Nguyen, K.P.; Hum, J.; DeLoughery, T.G. Arterial thrombosis in unusual sites: A practical review. Eur. J. Haematol. 2018, 101, 728–736. [Google Scholar] [CrossRef] [Green Version]
- Nakagami, Y.; Uchino, K.; Okada, H.; Suzuki, K.; Enomoto, M.; Mizuno, S.; Yamamoto, H.; Hanamura, I.; Nakayama, T.; Tani, H. Potential role of Howell-Jolly bodies in identifying functional hyposplenism: A prospective single-institute study. Int. J. Hematol. 2020, 112, 544–552. [Google Scholar] [CrossRef] [PubMed]
- Çora, A.R.; Çelik, E.; Karadem, K.B. Aortic Thrombosis in the Course of Covid-19 Disease; Two Rare Cases. Ann. Vasc. Surg. 2021, 73, 119–121. [Google Scholar] [CrossRef]
- Kugasia, I.R.; Ijaz, M.; Khan, A.; Jalil, B.A. A rare case of multiple aortic thromboses associated with severe COVID-19 infection. BMJ Case Rep. 2021, 14, e242196. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with Covid-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef] [PubMed]
- Hossri, S.; Shadi, M.; Hamarsha, Z.; Schneider, R.; El-Sayegh, D. Clinically significant anticardiolipin antibodies associated with COVID-19. J. Crit. Care 2020, 59, 32–34. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Time | Event |
|---|---|
| Day 0 (hospital admission) | Fever 38.5 °C, breath shortness, dry cough, oxygen saturation 86% PCR test for SARS-CoV-2 infection: positive Blood exams: 950 lymphocytes, d-dimers: 0.57 mg/L, LDH 551 U/L Enoxaparine at prophylactic dose (6.000IU once daily) Non-rebreather mask |
| Day 2 | HFNC due to clinical deterioration and presence of ARDS |
| Day 5 | Blood exams: leukocytosis (20,200 WBCs with 19,300 polmorphonuclear cells), LDH 1244 U/L, d-dimers 3.7 mg/L. Abdominal pain, localized mostly on the left upper and lower quadrant |
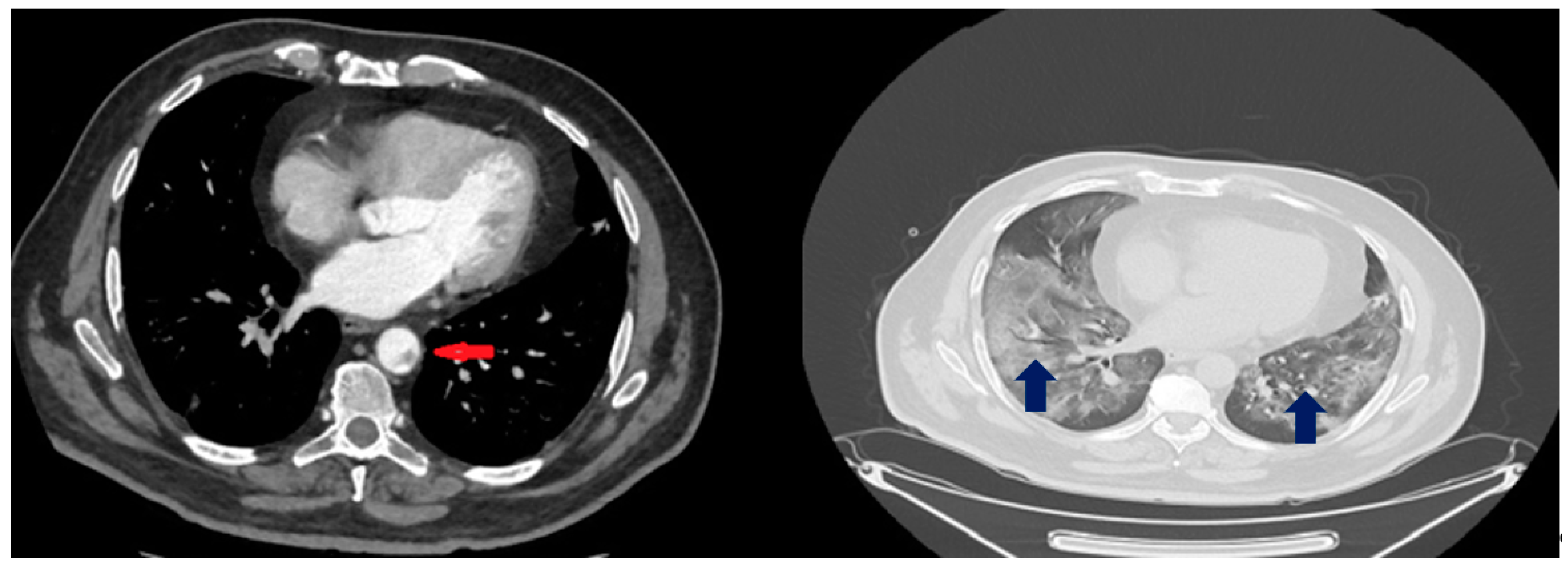
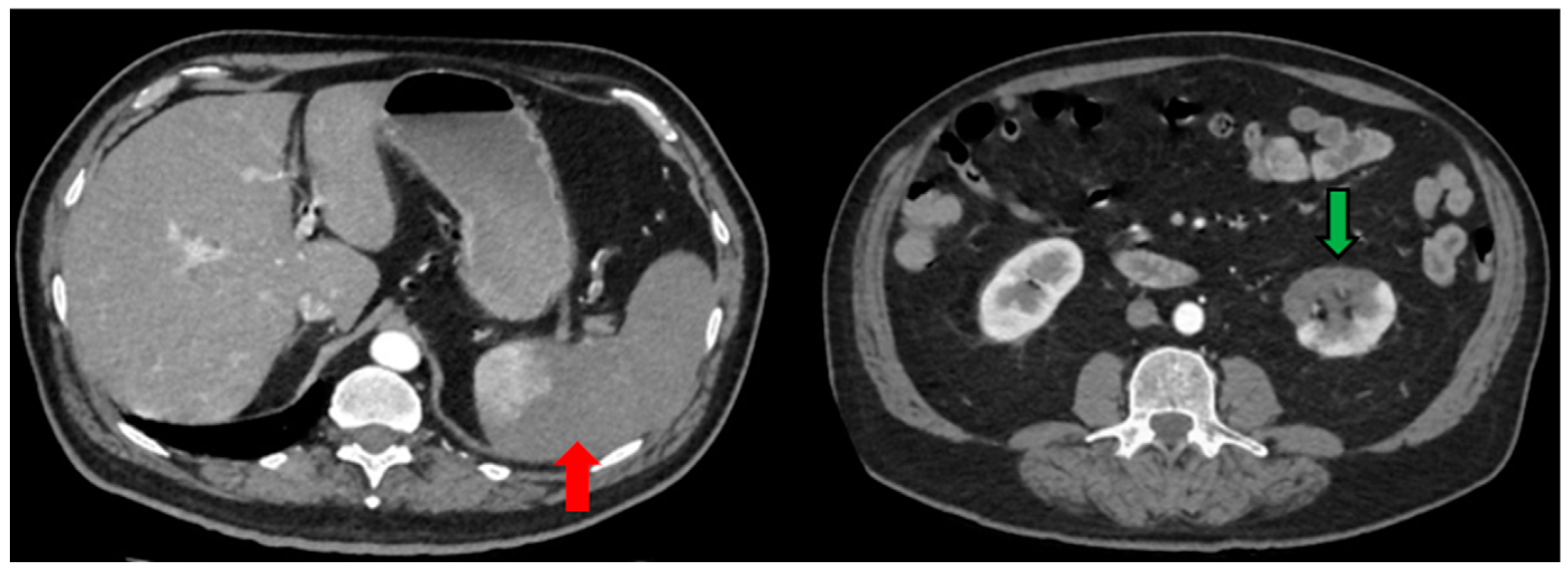
| Day 6 | Blood exams: 23,000 WBCs, LDH 1892 U/L, d-dimers 4.3 mg/L CTPA: Bilateral ground glass opacities, no evidence of pulmonary embolism, thrombi up to 5 mm in the thoracic aorta Abdominal and pelvic CT scan: Splenic infarct, thrombosis of splenic artery and vein, renal infarct at the left lower lobe. Enoxaparine at therapeutic dose (8.000 IU twice daily), acetylsalicylic acid 80 mg |
| Day 8 | Enoxaparine was replaced to sc fondaparinux 7.5 mg × 1 |
| Day 11 | Venturi mask (FiO2 50%), clinical improvement Continuing treatment with dexamethasone |
| Day 18 | Dexamethasone ceased after appropriate tapering Nasal oxygen therapy at 2 L/min |
| Day 19 | Patient without oxygen demands Discharge from hospital with the following instructions: po amoxicillin 500 mg × 2, po acetylsalicylic acid 80 mg, sc fondaparinux 7.5 mg and po omeprazole 20 mg for 6 months |
| Day 37 | Ultrasound of femoral and carotid arteries: No presence of thrombus, stenosis or significant atherosclerotic plaques |
| Day 43 | CTPA: Residual ground-glass opacity lesions, fibroatelectacic lesions at the right lower and middle lobe, traction bronchiectasis at right middle lobe and lingula of left lobe. No presence of thrombi at the thoracic aorta. Abdominal and pelvic CT scan: Splenic and renal infarct (along with renal cortical thinning) are depicted again. Re-tunelling of the splenic vein. |
| Day 51 | Ultrasonography of the lower extremities’ veins: No detection of venous chronic insufficiency or DVT. Blood exams: 10,200 WBCs, hematocrit 46.2% and hemoglobin 14.8 g/dL, detection of Howell-Jolly bodies Patient instructed to receive pneumococcal 13-valent conjugate vaccine, haemophilus influenza type b vaccine (Hib-ActHIB) as well as the meningococcal vaccine. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mavraganis, G.; Ioannou, S.; Kallianos, A.; Rentziou, G.; Trakada, G. A COVID-19 Patient with Simultaneous Renal Infarct, Splenic Infarct and Aortic Thrombosis during the Severe Disease. Healthcare 2022, 10, 150. https://doi.org/10.3390/healthcare10010150
Mavraganis G, Ioannou S, Kallianos A, Rentziou G, Trakada G. A COVID-19 Patient with Simultaneous Renal Infarct, Splenic Infarct and Aortic Thrombosis during the Severe Disease. Healthcare. 2022; 10(1):150. https://doi.org/10.3390/healthcare10010150
Chicago/Turabian StyleMavraganis, Georgios, Sofia Ioannou, Anastasios Kallianos, Gianna Rentziou, and Georgia Trakada. 2022. "A COVID-19 Patient with Simultaneous Renal Infarct, Splenic Infarct and Aortic Thrombosis during the Severe Disease" Healthcare 10, no. 1: 150. https://doi.org/10.3390/healthcare10010150