
The Association between COVID-19 Related Anxiety, Stress, Depression, Temporomandibular Disorders, and Headaches from Childhood to Adulthood: A Systematic Review
 , ,
, ,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
- (P) Participants consisted of patients.
- (E) The exposure consisted of patients with a diagnosis of TMD and evaluated with DC-TMD at the time of COVID
- (C) The comparison was patients in pre-COVID times with TMD.
- (O) The outcome consisted of assessing the prevalence of temporomandibular disorders in patients at the time of COVID. The secondary outcome consisted of assessing the correlation between TMD prevalence and severity during the time of COVID, compared with the time before COVID. Although the correlations between TMD, stress, and preoccupation due to the lifestyle changes from COVID were evaluated. Therefore, the secondary purpose was also to evaluate the correlation between COVID-19-related anxiety, stress, and increased TMD symptoms.
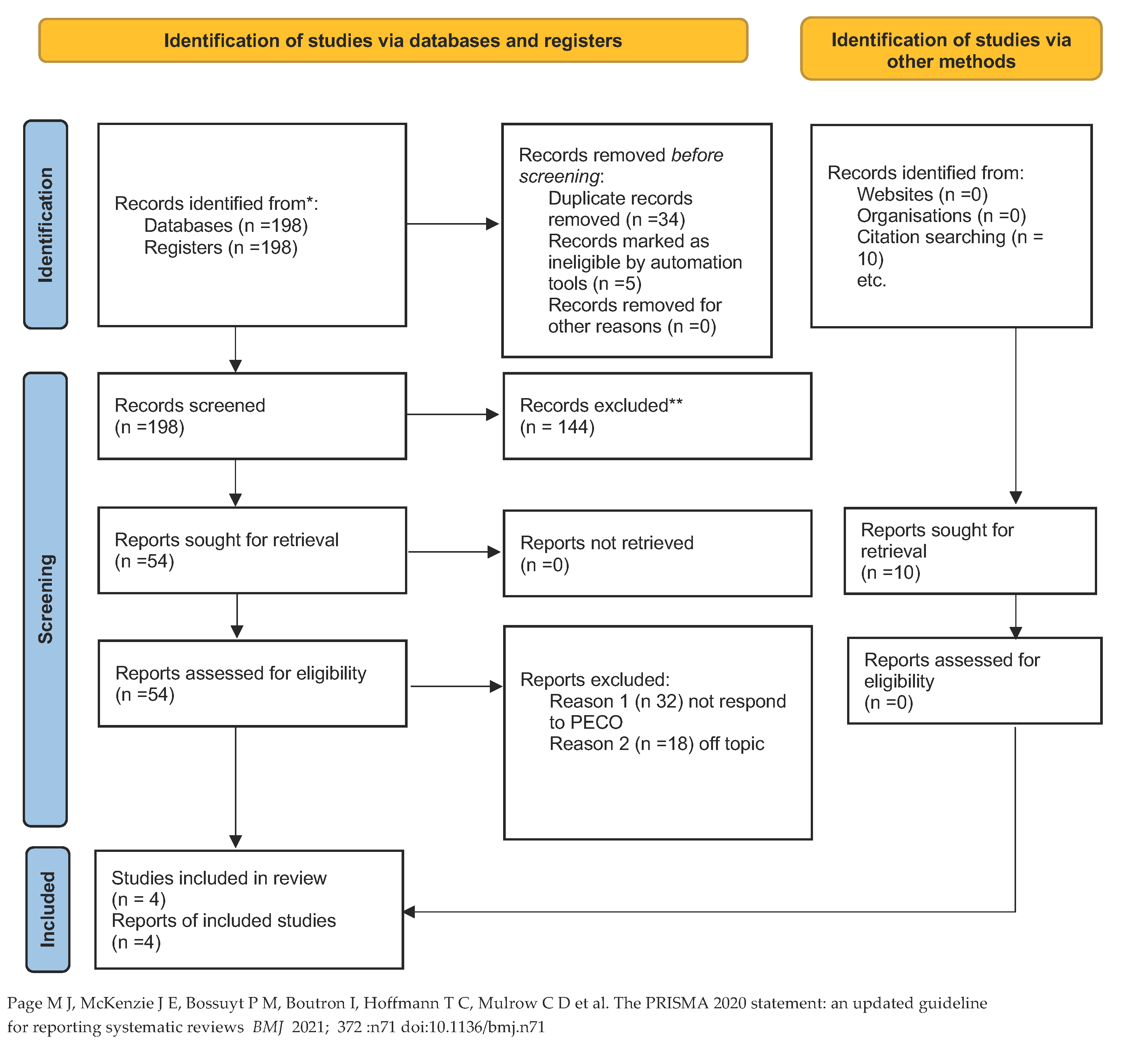
2.2. Search Strategy
2.3. Data Extraction
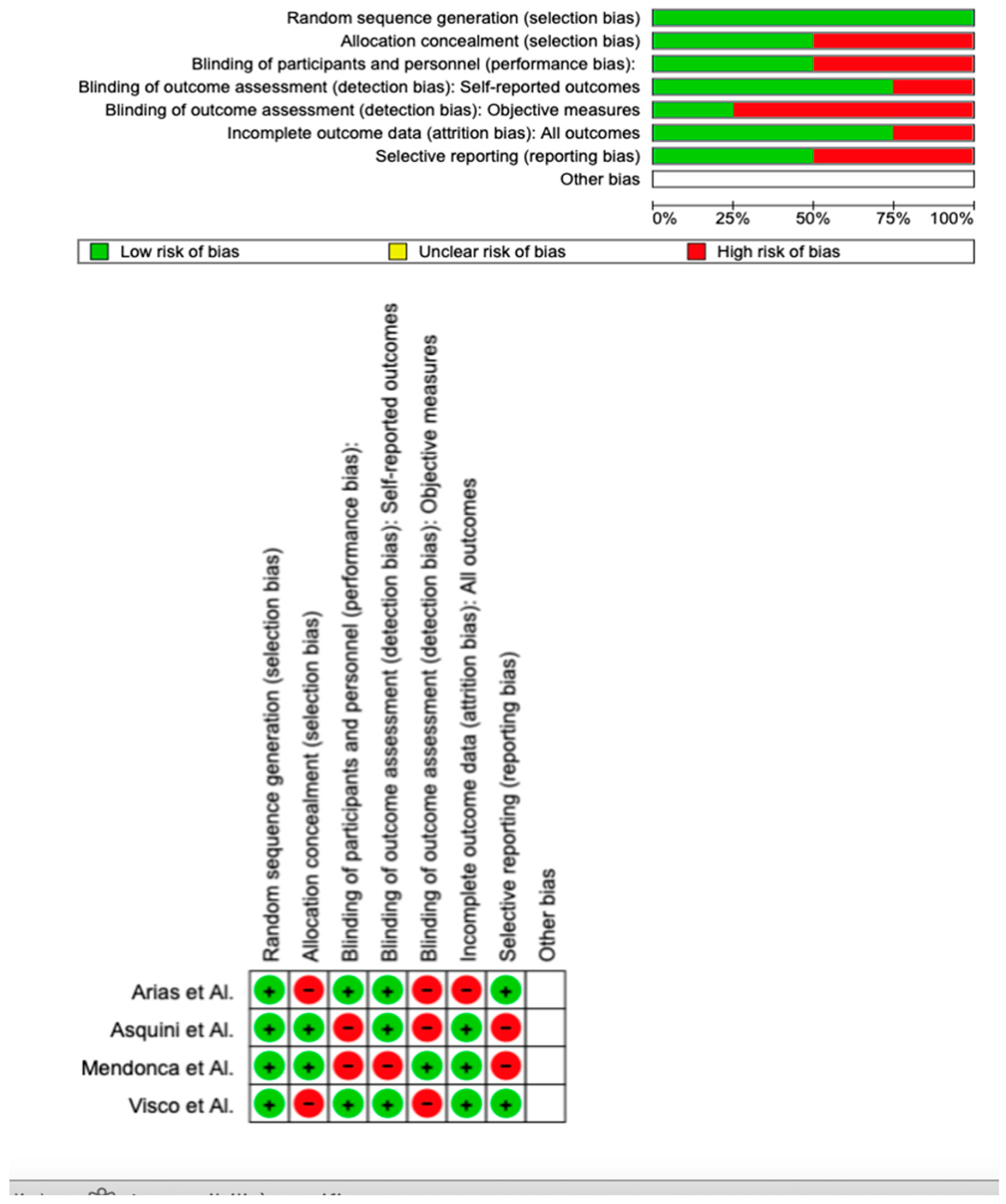
2.4. Quality Assessment
3. Results
3.1. Study Characteristics
Main Findings
3.2. Quality Assessment and Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Curci, C.; Pisano, F.; Bonacci, E.; Camozzi, D.M.; Ceravolo, C.; Bergonzi, R.; De Franceschi, S.; Moro, P.; Guarnieri, R.; Ferrillo, M.; et al. Early rehabilitation in post-acute COVID-19 patients: Data from an Italian COVID-19 rehabilitation unit and proposal of a treatment protocol. Eur. J. Phys. Rehabil. Med. 2020, 56, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Bennardo, F.; Buffone, C.; Fortunato, L.; Giudice, A. COVID-19 is a challenge for dental education—A commentary. Eur. J. Dent. Educ. 2020, 24, 822–824. [Google Scholar] [CrossRef] [PubMed]
- Badnjević, A.; Pokvić, L.G.; Džemić, Z.; Bečić, F. Risks of emergency use authorizations for medical products during outbreak situations: A COVID-19 case study. Biomed. Eng. Online 2020, 19, 1–14. [Google Scholar] [CrossRef]
- Machoň, V.; Levorová, J.; Beňo, M.; Foltán, R. The Manifestations of Covid-19 Infection. Manifestations in Patients with Temporomandibular Joint Disorders. Prague Med. Rep. 2022, 123, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Haddad, C.; Sayegh, S.M.; El Zoghbi, A.; Lawand, G.; Nasr, L. The Prevalence and Predicting Factors of Temporomandibular Disorders in COVID-19 Infection: A Cross-Sectional Study. Cureus 2022, 14, 28167. [Google Scholar] [CrossRef]
- Badnjević, A.; Cifrek, M.; Koruga, D. Integrated software suite for diagnosis of respiratory diseases. In Proceedings of the Eurocon 2013, Zagreb, Croatia, 1–4 July 2013; pp. 564–568. [Google Scholar] [CrossRef]
- Badnjevic, A.; Koruga, D.; Cifrek, M.; Smith, H.J.; Bego, T. Interpretation of pulmonary function test results in relation to asthma classification using integrated software suite. In 2013 36th International Convention on Information and Communication Technology, Electronics and Microelectronics (MIPRO); IEEE: Toulouse, France. [CrossRef]
- Granulo, E.; Bećar, L.; Gurbeta, L.; Badnjevic, A. Telemetry System for Diagnosis of Asthma and Chronical Obstructive Pulmonary Disease (COPD). In The Internet of Things Technologies for HealthCare, Västerås, Sweden, 18–19 October 2016; Lecture Notes of the Institute for Computer Sciences, Social-Informatics and Telecommunications Engineering, LNICST; Springer: Berlin/Heidelberg, Germany, 2016; pp. 113–118. [Google Scholar] [CrossRef]
- Stokes, K.; Castaldo, R.; Franzese, M.; Salvatore, M.; Fico, G.; Pokvic, L.G.; Badnjevic, A.; Pecchia, L. A machine learning model for supporting symptom-based referral and diagnosis of bronchitis and pneumonia in limited resource settings. Biocybern. Biomed. Eng. 2021, 41, 1288–1302. [Google Scholar] [CrossRef]
- Nahidh, M.; Al-Khawaja, N.F.K.; Jasim, H.M.; Cervino, G.; Cicciù, M.; Minervini, G. The Role of Social Media in Communication and Learning at the Time of COVID-19 Lockdown—An Online Survey. Dent. J. 2023, 11, 48. [Google Scholar] [CrossRef]
- de Medeiros, R.A.; Vieira, D.L.; da Silva, E.V.F.; de Rezende, L.V.M.L.; dos Santos, R.W.; Tabata, L.F. Prevalence of symptoms of temporomandibular disorders, oral behaviors, anxiety, and depression in dentistry students during the period of social isolation due to COVID-19. J. Appl. Oral Sci. 2020, 28, 1–8. [Google Scholar] [CrossRef]
- Emodi-Perlman, A.; Eli, I. One year into the COVID-19 pandemic—Temporomandibular disorders and bruxism: What we have learned and what we can do to improve our manner of treatment. Dent. Med. Probl. 2021, 58, 215–218. [Google Scholar]
- Vrbanović, E.; Alajbeg, I.Z.; Alajbeg, I. COVID-19 pandemic and Zagreb earthquakes as stressors in patients with temporomandibular disorders. Oral Dis. 2020, 27, 688–693. [Google Scholar] [CrossRef]
- La Torre, G.; Shivkumar, S.; Mehta, V.; Kumar Vaddamanu, S.; Shetty, U.A.; Hussain Alhamoudi, F.; Ali Alwadi, M.M.; Ibrahim Aldosari, L.N.; Ali Alshadidi, A.F.; Minervini, G. Surgical Protocols before and after COVID-19-A Narrative Review. Vaccines 2023, 58, 215–218. [Google Scholar]
- Bennardo, F.; Antonelli, A.; Barone, S.; Figliuzzi, M.M.; Fortunato, L.; Giudice, A. Change of Outpatient Oral Surgery during the COVID-19 Pandemic: Experience of an Italian Center. Int. J. Dent. 2020, 2020, 8893423. [Google Scholar] [CrossRef] [PubMed]
- Sycinska-Dziarnowska, M.; Maglitto, M.; Woźniak, K.; Spagnuolo, G. Oral Health and Teledentistry Interest during the COVID-19 Pandemic. J. Clin. Med. 2021, 10, 3532. [Google Scholar] [CrossRef] [PubMed]
- Campus, G.; Diaz-Betancourt, M.; Cagetti, M.; Carvalho, J.; Carvalho, T.; Cortés-Martinicorena, J.; Deschner, J.; Douglas, G.; Giacaman, R.; Machiulskiene, V.; et al. Study Protocol for an Online Questionnaire Survey on Symptoms/Signs, Protective Measures, Level of Awareness and Perception Regarding COVID-19 Outbreak among Dentists. A Global Survey. Int. J. Environ. Res. Public Health 2020, 17, 5598. [Google Scholar] [CrossRef]
- Lee, G.S.; Kim, H.K.; Kim, M.E. Relevance of sleep, pain cognition, and psychological distress with regard to pain in patients with burning mouth syndrome. Cranio J. Craniomandib. Pract. 2022, 40, 79–87. [Google Scholar] [CrossRef]
- Liu, M.; Liu, M.; Lv, K. Recommended Management of Temporomandibular Joint Dislocation During the COVID-19 Outbreak. J Craniofac. Surg. 2020, 31, e809–e810. [Google Scholar] [CrossRef]
- Cicciù, M.; Laino, L.; Fiorillo, L. Oral signs and symptoms of COVID-19 affected patients: Dental practice as prevention method. Minerva Dent. Oral Sci. 2020. [Google Scholar] [CrossRef]
- Troiano, G.; Dioguardi, M.; Giannatempo, G.; Laino, L.; Testa, N.F.; Cocchi, R.; De Lillo, A.; Muzio, L.L. Orofacial Granulomatosis: Clinical Signs of Different Pathologies. Med. Princ. Pract. 2015, 24, 117–122. [Google Scholar] [CrossRef]
- Fiorillo, L.; De Stefano, R.; Cervino, G.; Crimi, S.; Bianchi, A.; Campagna, P.; Herford, A.S.; Laino, L.; Cicciù, M. Oral and Psychological Alterations in Haemophiliac Patients. Biomedicines 2019, 7, 33. [Google Scholar] [CrossRef] [Green Version]
- Cicciù, M.; Herford, A.S.; Cervino, G.; Troiano, G.; Lauritano, F.; Laino, L. Tissue Fluorescence Imaging (VELscope) for Quick Non-Invasive Diagnosis in Oral Pathology. J. Craniofacial Surg. 2017, 28, e112–e115. [Google Scholar] [CrossRef]
- Straburzyński, M.; Nowaczewska, M.; Budrewicz, S.; Waliszewska-Prosół, M. COVID-19-related headache and sinonasal inflammation: A longitudinal study analysing the role of acute rhinosinusitis and ICHD-3 classification difficulties in SARS-CoV-2 infection. Cephalalgia 2022, 42, 218–228. [Google Scholar] [CrossRef] [PubMed]
- Daltaban, Ö.; Aytekin, Z.A. Fear and anxiety of COVID-19 in dental patients during the COVID-19 pandemic: A cross-sectional survey in Turkey. Dent. Med. Probl. 2022, 59, 150075. [Google Scholar] [CrossRef] [PubMed]
- Martina, S.; Amato, A.; Faccioni, P.; Iandolo, A.; Amato, M.; Rongo, R. The perception of COVID-19 among Italian dental patients: An orthodontic point of view. Prog. Orthod. 2021, 22, 11. [Google Scholar] [CrossRef]
- Franco, R.; Basili, M.; Venditti, A.; Chiaramonte, C.; Ottria, L.; Barlattani, A.; Bollero, P. Statistical analysis of the frequency distribution of signs and symptoms of patients with temporomandibular disorders. Oral Implant. 2016, 9, 190–201. [Google Scholar] [CrossRef]
- Emodi-Perlman, A.; Eli, I.; Smardz, J.; Uziel, N.; Wieckiewicz, G.; Gilon, E.; Grychowska, N.; Wieckiewicz, M. Temporomandibular Disorders and Bruxism Outbreak as a Possible Factor of Orofacial Pain Worsening during the COVID-19 Pandemic—Concomitant Research in Two Countries. J. Clin. Med. 2020, 9, 3250. [Google Scholar] [CrossRef] [PubMed]
- Gaş, S.; Özsoy, H.E.; Aydın, K.C. The association between sleep quality, depression, anxiety and stress levels, and temporomandibular joint disorders among Turkish dental students during the COVID-19 pandemic. Cranio® J. Craniomandib. Pract. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Rathi, S.; Chaturvedi, S.; Abdullah, S.; Rajput, G.; Alqahtani, N.M.; Chaturvedi, M.; Gurumurthy, V.; Saini, R.; Bavabeedu, S.S.; Minervini, G. Clinical Trial to Assess Physiology and Activity of Masticatory Muscles of Complete Denture Wearer Following Vitamin D Intervention. Medicina 2023, 59, 410. [Google Scholar] [CrossRef]
- Crescente, G.; Minervini, G.; Spagnuolo, C.; Moccia, S. Cannabis Bioactive Compound-Based Formulations: New Perspectives for the Management of Orofacial Pain. Molecules 2022, 28, 106. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Fiorillo, L.; Russo, D.; Lanza, A.; D’Amico, C.; Cervino, G.; Meto, A.; Di Francesco, F. Prosthodontic Treatment in Patients with Temporomandibular Disorders and Orofacial Pain and/or Bruxism: A Review of the Literature. Prosthesis 2022, 4, 253–262. [Google Scholar] [CrossRef]
- Di Francesco, F.; Lanza, A.; Di Blasio, M.; Vaienti, B.; Cafferata, E.A.; Cervino, G.; Cicciù, M.; Minervini, G. Application of Botulinum Toxin in Temporomandibular Disorders: A Systematic Review of Randomized Controlled Trials (RCTs). Appl. Sci. 2022, 12, 12409. [Google Scholar] [CrossRef]
- Minervini, G.D.; D’Amico, C.D.; Cicciù, M.D.; Fiorillo, L.D. Temporomandibular Joint Disk Displacement: Etiology, Diagnosis, Imaging, and Therapeutic Approaches. J. Craniofacial Surg. 2022, 10–1097. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Mariani, P.; Fiorillo, L.; Cervino, G.; Cicciù, M.; Laino, L. Prevalence of temporomandibular disorders in people with multiple sclerosis: A systematic review and meta-analysis. Cranio® 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.D.; Del Mondo, D.D.; Russo, D.D.; Cervino, G.D.; D’Amico, C.D.; Fiorillo, L.D. Stem Cells in Temporomandibular Joint Engineering: State of Art and Future Persectives. J. Craniofacial Surg. 2022, 33, 2181–2187. [Google Scholar] [CrossRef] [PubMed]
- Giudice, A.; Barone, S.; Muraca, D.; Averta, F.; Diodati, F.; Antonelli, A.; Fortunato, L. Can Teledentistry Improve the Monitoring of Patients during the Covid-19 Dissemination? A Descriptive Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 3399. [Google Scholar] [CrossRef]
- Chakraborty, T.; Jamal, R.; Battineni, G.; Teja, K.; Marto, C.; Spagnuolo, G. A Review of Prolonged Post-COVID-19 Symptoms and Their Implications on Dental Management. Int. J. Environ. Res. Public Health 2021, 18, 5131. [Google Scholar] [CrossRef]
- Spagnuolo, G.; De Vito, D.; Rengo, S.; Tatullo, M. COVID-19 Outbreak: An Overview on Dentistry. Int. J. Environ. Res. Public Health 2020, 17, 2094. [Google Scholar] [CrossRef] [Green Version]
- Reddy, L.K.V.; Madithati, P.; Narapureddy, B.R.; Ravula, S.R.; Vaddamanu, S.K.; Alhamoudi, F.H.; Minervini, G.; Chaturvedi, S. Personalized Medicine Perception about Health Applications (Apps) in Smartphones towards Telemedicine during COVID-19: A Cross-Sectional Study. J. Pers. Med. 2022, 12, 1920. [Google Scholar] [CrossRef]
- Qazi, N.; Pawar, M.; Padhly, P.P. 2023 Teledentistry: Evaluation of Instagram posts related to Bruxism. Technol. Health Care 2023, 1–12. [Google Scholar] [CrossRef]
- Vlăduțu, D.; Popescu, S.M.; Mercuț, R.; Ionescu, M.; Scrieciu, M.; Glodeanu, A.D.; Stănuși, A.; Rîcă, A.M.; Mercuț, V. Associations between Bruxism, Stress, and Manifestations of Temporomandibular Disorder in Young Students. Int. J. Environ. Res. Public Health 2022, 19, 5415. [Google Scholar] [CrossRef]
- Cavallo, L.; Marcianò, A.; Cicciù, M.; Oteri, G. 3D Printing beyond Dentistry during COVID 19 Epidemic: A Technical Note for Producing Connectors to Breathing Devices. Prosthesis 2020, 2, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Scarano, A.; Inchingolo, F.; Lorusso, F. Environmental Disinfection of a Dental Clinic during the Covid-19 Pandemic: A Narrative Insight. BioMed. Res. Int. 2020, 2020, 8896812. [Google Scholar] [CrossRef] [PubMed]
- Charitos, I.A.; Del Prete, R.; Inchingolo, F.; Mosca, A.; Carretta, D.; Ballini, A.; Santacroce, L. What we have learned for the future about COVID-19 and healthcare management of it? Acta Biomed. 2020, 91, 1–8. [Google Scholar]
- Colonna, A.; Guarda-Nardini, L.; Ferrari, M.; Manfredini, D. COVID-19 pandemic and the psyche, bruxism, temporomandibular disorders triangle. Cranio® J. Craniomandib. Pract. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Straburzyński, M.; Kuca-Warnawin, E.; Waliszewska-Prosół, M. COVID-19-related headache and innate immune response—A narrative review. Neurol. Neurochir. Pol. 2022, 57, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Peixoto, K.O.; de Resende, C.M.B.M.; de Almeida, E.O.; Almeida-Leite, C.M.; Conti, P.C.R.; Barbosa, G.A.S.; Barbosa, J.S. Association of sleep quality and psychological aspects with reports of bruxism and TMD in Brazilian dentists during the COVID-19 pandemic. J. Appl. Oral Sci. 2021, 29, e20201089. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Rodríguez, M.; Sillero-Arenas, M. Systematic review and meta-analysis. Med. Intensiva 2018, 42, 444–453. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow , C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar]
- Winocur-Arias, O.; Winocur, E.; Shalev-Antsel, T.; Reiter, S.; Shifra, L.; Emodi-Perlman, A.; Friedman-Rubin, P. Painful Temporomandibular Disorders, Bruxism and Oral Parafunctions before and during the COVID-19 Pandemic Era: A Sex Comparison among Dental Patients. J. Clin. Med. 2022, 11, 589. [Google Scholar] [CrossRef]
- Saccomanno, S.; Bernabei, M.; Scoppa, F.; Pirino, A.; Mastrapasqua, R.; Visco, M.A. Coronavirus Lockdown as a Major Life Stressor: Does It Affect TMD Symptoms? Int. J. Environ. Res. Public Health 2020, 17, 8907. [Google Scholar] [CrossRef]
- Mendonça, A.K.R.; Fontoura, L.P.G.; da Rocha, T.D.; Fontenele, R.C.; Nunes, T.N.B.; Regis, R.R.; Pinto-Fiamengui, L.M.S. Influence of the COVID-19 pandemic on pain and oral health-related quality of life in women with temporomandibular disorder. Dent. Press J. Orthod. 2022, 27. [Google Scholar] [CrossRef]
- Asquini, G.; Bianchi, A.E.; Borromeo, G.; Locatelli, M.; Falla, D. The impact of COVID-19-related distress on general health, oral behaviour, psychosocial features, disability and pain intensity in a cohort of Italian patients with temporomandibular disorders. PLoS ONE 2021, 16, e0245999. [Google Scholar] [CrossRef]
- Almeida-Leite, C.M.; Stuginski-Barbosa, J.; Conti, P.C.R. How psychosocial and economic impacts of COVID-19 pandemic can interfere on bruxism and temporomandibular disorders? J. Appl. Oral Sci. 2020, 28, e20200263. [Google Scholar] [CrossRef] [PubMed]
- Perrone, M.A.; Feola, A.; Pieri, M.; Donatucci, B.; Salimei, C.; Lombardo, M.; Perrone, A.; Parisi, A. The Effects of Reduced Physical Activity on the Lipid Profile in Patients with High Cardiovascular Risk during COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 8858. [Google Scholar] [CrossRef] [PubMed]
- Perrone, M.A.; Spolaore, F.; Ammirabile, M.; Romeo, F.; Caciagli, P.; Ceriotti, F.; Bernardini, S. The assessment of high sensitivity cardiac troponin in patients with COVID-19: A multicenter study. IJC Heart Vasc. 2021, 32, 100715. [Google Scholar] [CrossRef]
- Scelza, G.; Amato, A.; Rongo, R.; Nucci, L.; D’Ambrosio, F.; Martina, S. Changes in COVID-19 Perception and in TMD Prevalence after 1 Year of Pandemic in Italy. Eur. J. Dent. 2022. [Google Scholar] [CrossRef] [PubMed]
- Gębska, M.; Dalewski, B.; Pałka, Ł.; Kołodziej, Ł.; Sobolewska, E. The Importance of Type D Personality in the Development of Temporomandibular Disorders (TMDs) and Depression in Students during the COVID-19 Pandemic. Brain Sci. 2021, 12, 28. [Google Scholar] [CrossRef]
- Lee, Y.-H.; Auh, Q.-S. Clinical factors affecting depression in patients with painful temporomandibular disorders during the COVID-19 pandemic. Sci. Rep. 2022, 12, 14667. [Google Scholar] [CrossRef]
- Carrillo-Diaz, M.; Ortega-Martínez, A.R.; Romero-Maroto, M.; González-Olmo, M.J. Lockdown impact on lifestyle and its association with oral parafunctional habits and bruxism in a Spanish adolescent population. Int. J. Paediatr. Dent. 2021, 32, 185–193. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| PubMed Search: (temporomandibular disorder) AND (COVID) (“temporomandibular joint disorders” [MeSH Terms] OR (“temporomandibular” [All Fields] AND “joint” [All Fields] AND “disorders” [All Fields]) OR “temporomandibular joint disorders” [All Fields] OR (“temporomandibular” [All Fields] AND “disorder” [All Fields]) OR “temporomandibular disorder” [All Fields]) AND (“SARS-CoV-2” [MeSH Terms] OR “SARS-CoV-2” [All Fields] OR “COVID” [All Fields] OR “covid 19” [MeSH Terms] OR “COVID 19” [All Fields]) |
| Web of Science (ALL = (temporomandibular disorders)) AND ALL = (COVID) |
| Lilacs temporomandibular disorders [Palavras] and COVID [Palavras] |
| Scopus TITLE-ABS-KEY (temporomandibular AND disorders AND COVID) |
| Authors | Year | Nationality | Type of Study | Classification of TMD | Samples | Age | Type and Severity of Symptoms | Main Findings | Difference between Pre and COVID Era |
|---|---|---|---|---|---|---|---|---|---|
| Winocur-Arias et al. [51] | 2022 | Israel | Retrospective | Axis I DC/TMD | 288 patients were divided into two groups. Group 1: 108 patients pre-COVID era. Group 2: 180 patients COVID era | 35.6 yr | Evaluation of myalgia, myofascial pain, parafunction, bruxism | The results of this study showed a significant increase in parafunction in both men and women in the COVID era | Increase symptoms of TMD during COVID era |
| Visco et al. [52] | 2020 | Italy | Randomized clinical trial | Axis II RDC/TMD | A group of 182 patients | 45 yr | Evaluation of TMJ with AXIS II for evaluated TMD and stress with PSS (perceived stress scale) | A questionnaire was administered. This evaluates chronic jaw pain, the impediment of social life that follows pain, and the evaluation of psychosocial stress. 51.4% of these subjects reported that symptoms worsened following the lockdown | Increase symptoms of TMJ during COVID era |
| Mendonca et al. [53] | 2022 | Brazil | Randomized clinical trial | RDC/TMD | 41 women with temporomandibular disease. | 30 yr | The study compared pain intensity and oral health-related quality of life (OHRQoL) in women with temporomandibular disorder | The data were collected in two stages. At time T1, prior to the pandemic, and at time T2 during the pandemic period.). No statistically significant differences were found in pain (p = 0.26) and overall OHIP-14 scores | No statistical significance |
| Asquini et al. [54] | 2020 | Italy | Prospective cohort study | Axis II RDC/TMD | 45 adults before the lockdown (19 chronic, 26 acute/subacute TMD). A Covid stress scale was administered during the lockdown | 29 yr | Evaluation of TMD pre and after the lockdown with CSS to evaluate the possible stress during lockdown in the onset of TMJ | Scores on the scale were significantly higher in patients with chronic TMD (p < 0.05). In people with chronic TMD. The change in chronic pain was statistically correlated with the change in CSS scores (r = 0.59; p = 0.017) | COVID worsened pain in patients with chronic TMJ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minervini, G.; Franco, R.; Marrapodi, M.M.; Mehta, V.; Fiorillo, L.; Badnjević, A.; Cervino, G.; Cicciù, M. The Association between COVID-19 Related Anxiety, Stress, Depression, Temporomandibular Disorders, and Headaches from Childhood to Adulthood: A Systematic Review. Brain Sci. 2023, 13, 481. https://doi.org/10.3390/brainsci13030481
Minervini G, Franco R, Marrapodi MM, Mehta V, Fiorillo L, Badnjević A, Cervino G, Cicciù M. The Association between COVID-19 Related Anxiety, Stress, Depression, Temporomandibular Disorders, and Headaches from Childhood to Adulthood: A Systematic Review. Brain Sciences. 2023; 13(3):481. https://doi.org/10.3390/brainsci13030481
Chicago/Turabian StyleMinervini, Giuseppe, Rocco Franco, Maria Maddalena Marrapodi, Vini Mehta, Luca Fiorillo, Almir Badnjević, Gabriele Cervino, and Marco Cicciù. 2023. "The Association between COVID-19 Related Anxiety, Stress, Depression, Temporomandibular Disorders, and Headaches from Childhood to Adulthood: A Systematic Review" Brain Sciences 13, no. 3: 481. https://doi.org/10.3390/brainsci13030481