
Impact of Different Transportation Modes on the Transmission of COVID-19: Correlation and Strategies from a Case Study in Wuhan, China
 , , ,
, , ,
Abstract
:1. Introduction
2. Literature Review
3. Materials and Methods
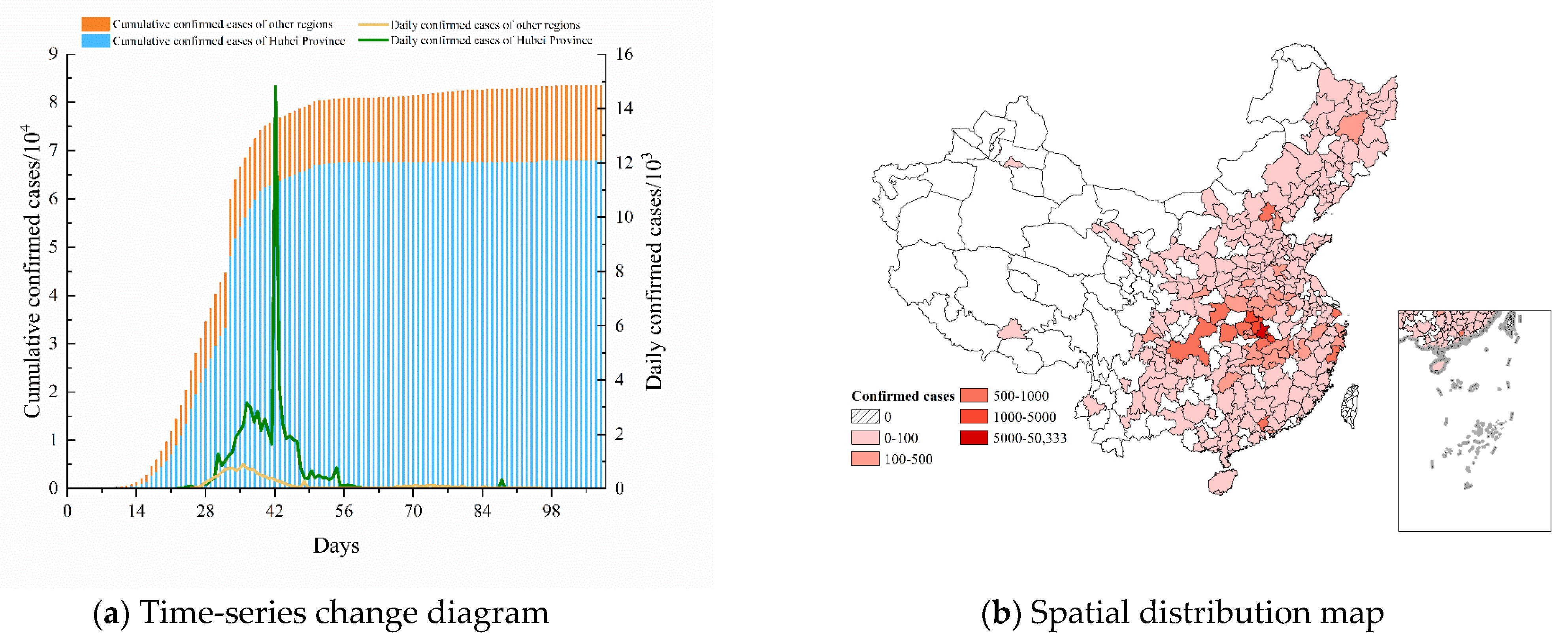
3.1. Research Region
3.2. Data Sources
3.3. Definition of Epidemic Transmission Patterns Indicators
- (1)
- Transmission speed: the number of days between the announcement of the first confirmed case of COVID-19 in Wuhan (11 January 2020) and the first confirmed case in that city (Equation (1));
- (2)
- Transmission severity: the cumulative number of confirmed cases in a given city (until the end of February 2020) (Equation (2)).
3.4. Classification of Transportation Facilities and Inspection Methods
- (1)
- K-means clustering algorithm
- (2)
- Mann–Whitney U test
3.5. Modelling the Impact of Transportation Modes on the Epidemic Transmission
3.5.1. Epidemic Transmission Patterns
- (1)
- Transmission speed
- (2)
- Transmission severity
3.5.2. Regression Modelling of the Transmission Speed and Severity
- (1)
- Quantile regression
- (2)
- Negative binomial regression
4. Results
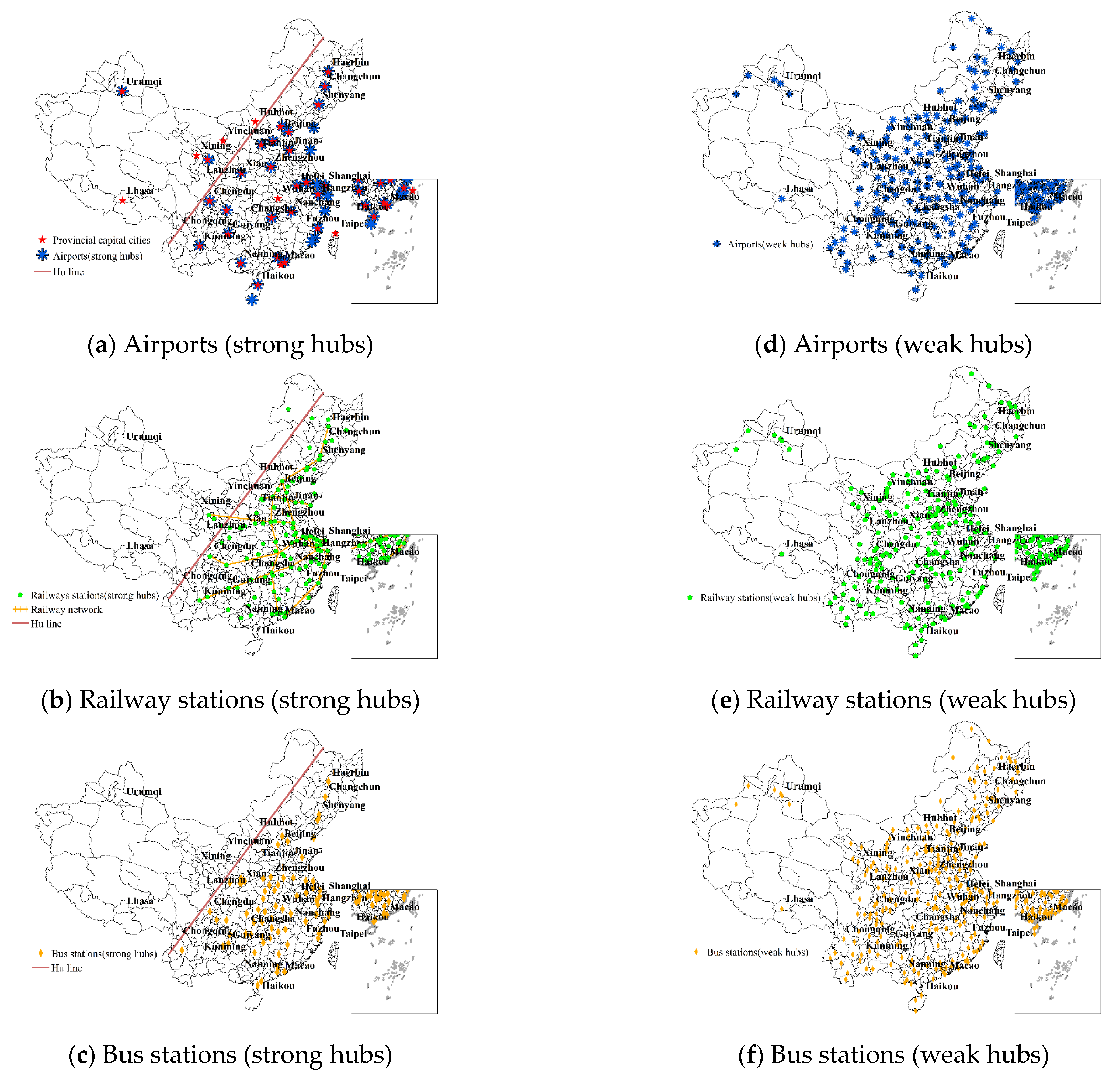
4.1. Division of Transportation Hubs
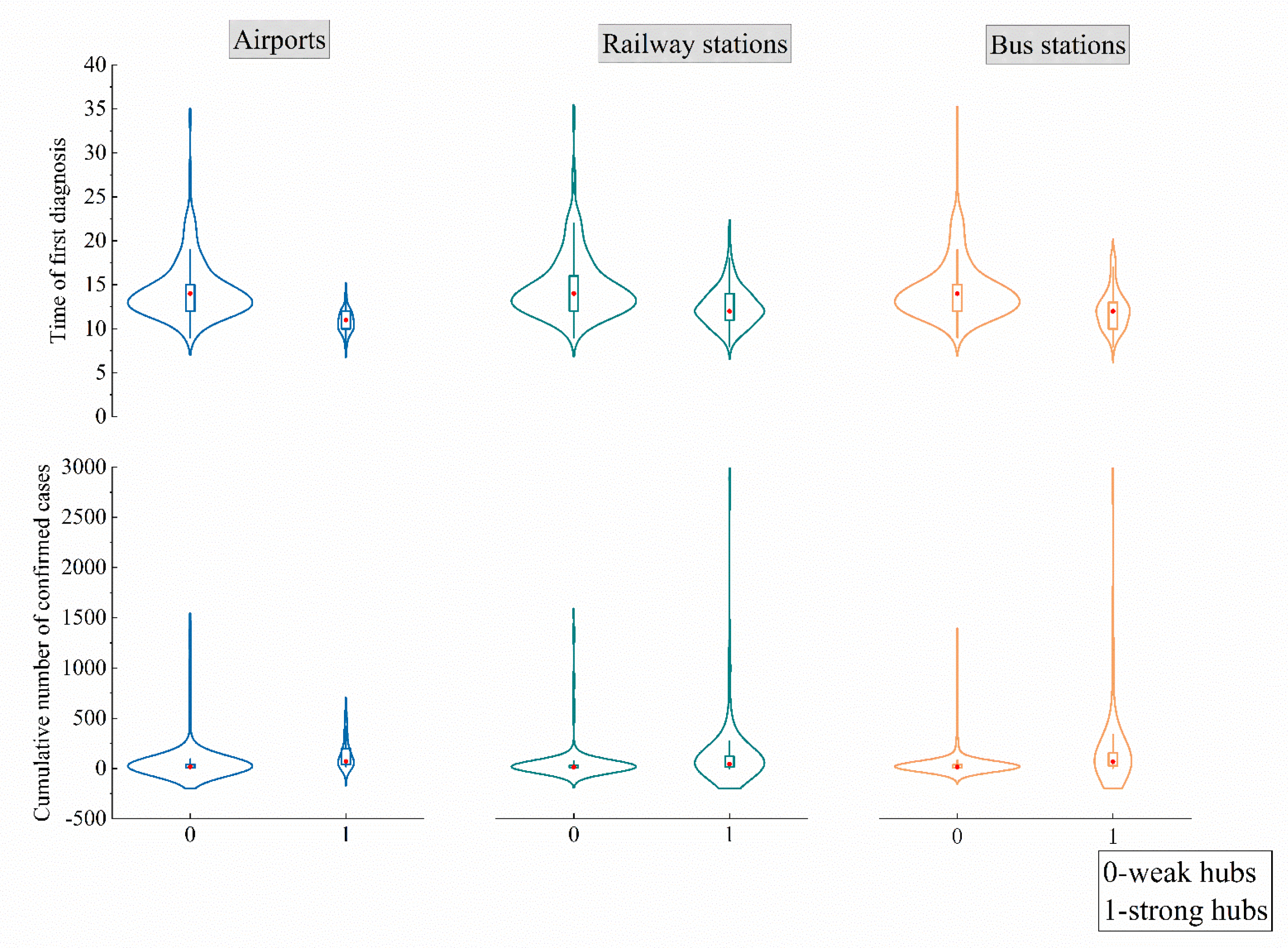
4.2. The Role of Transportation Hubs in the Epidemic Transmission
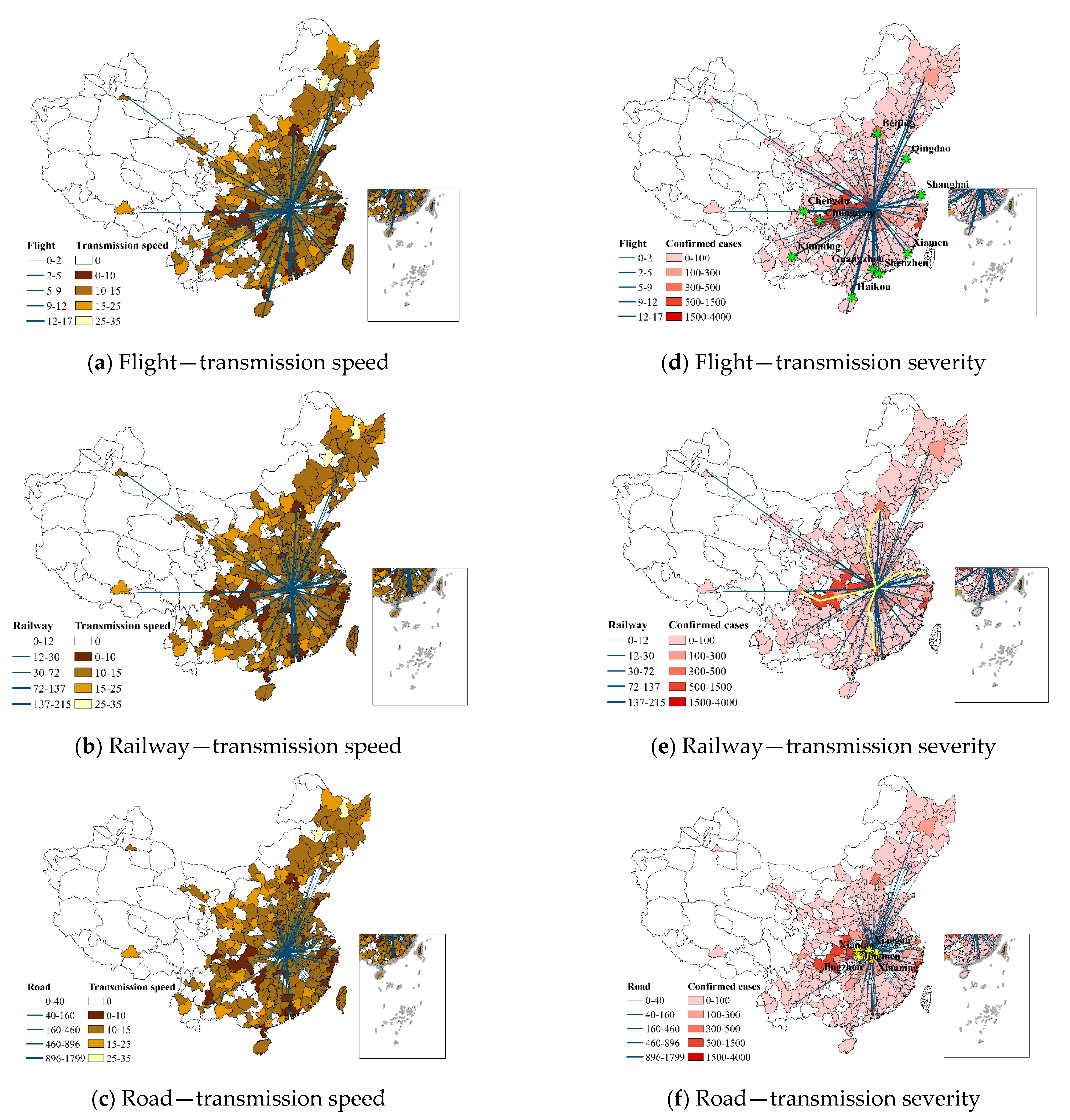
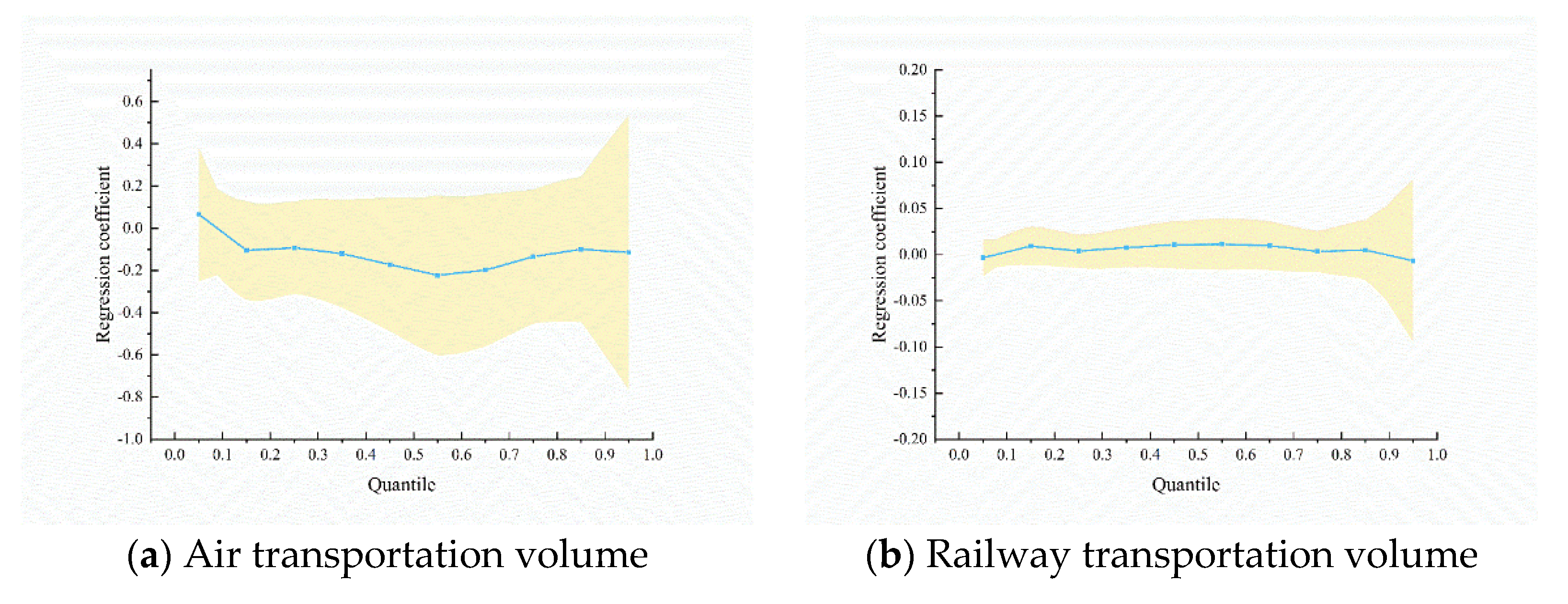
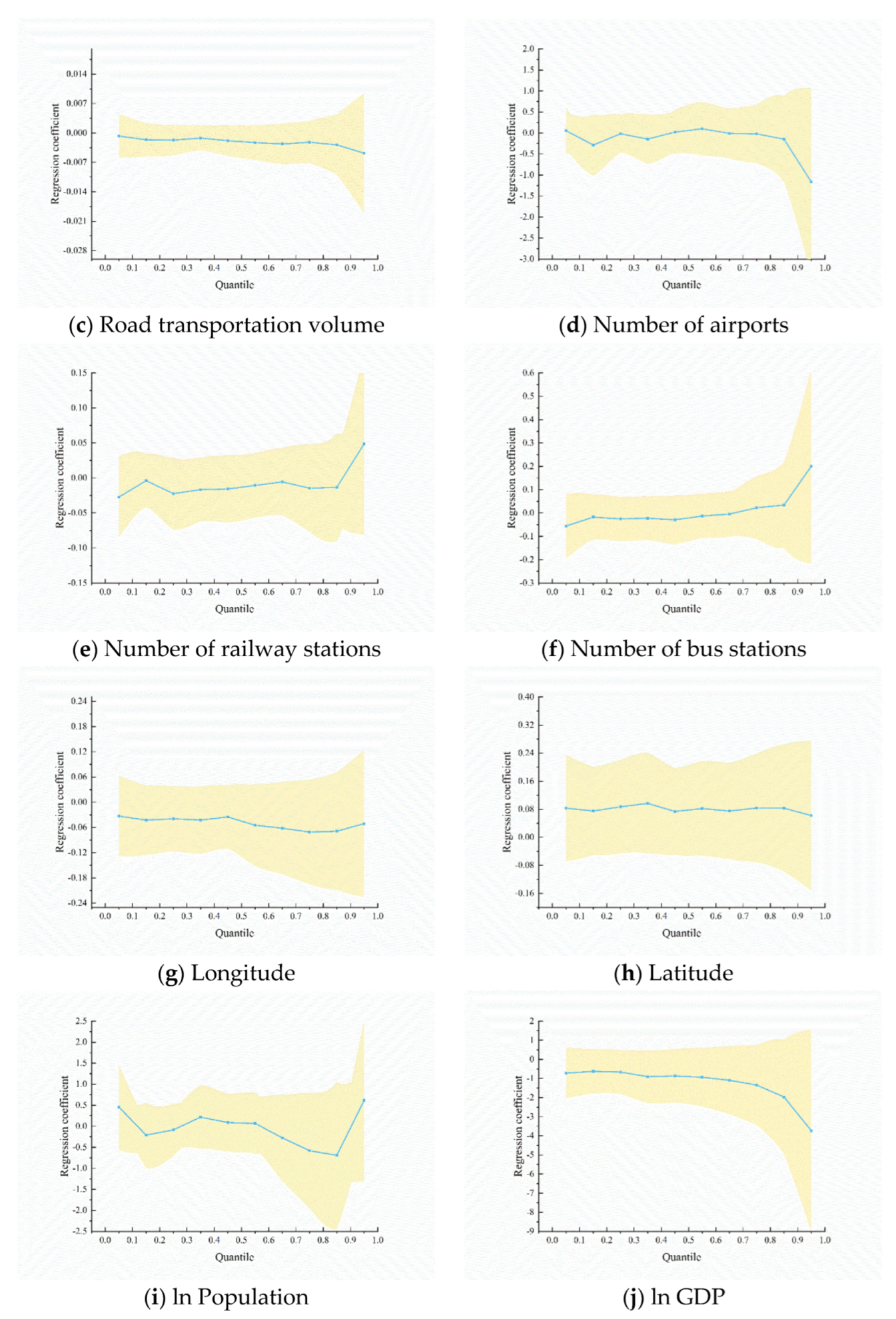
4.3. Influence of Transportation Modes on Epidemic Transmission
- (1)
- Transmission speed
- (2)
- Transmission severity
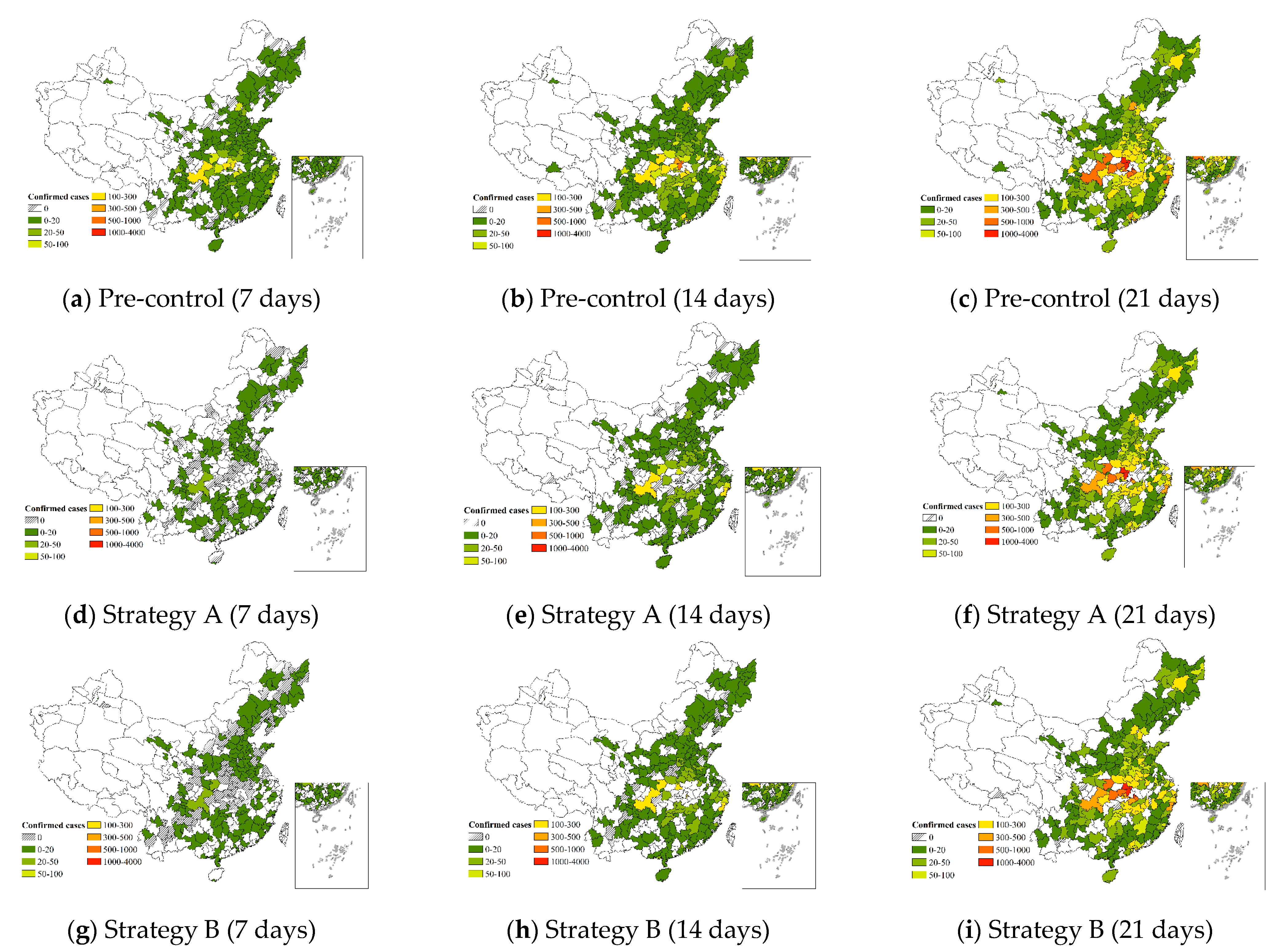
5. Evaluation of Different Prevention Strategies
- (1)
- Strategy A
- (2)
- Strategy B
- (3)
- Comparison of control effects
6. Discussion
6.1. Impact of Transportation Hubs on the Epidemic Transmission
- Transmission speed
- Transmission severity
6.2. The Role of Transportation Modes in the Epidemic Transmission
6.3. Suggestions Regarding Prevention Strategies
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, Y.; Zhang, A.; Wang, J. Exploring the roles of high-speed train, air and coach services in the spread of COVID-19 in China. Transp. Policy 2020, 94, 34–42. [Google Scholar] [CrossRef]
- Ai, S.; Zhu, G.; Tian, F.; Li, H.; Gao, Y.; Wu, Y.; Liu, Q.; Lin, H. Population Movement, City Closure and Spatial Transmission of the 2019-nCoV Infection in China. medRxiv 2020. [Google Scholar] [CrossRef]
- Liu, T.; Jin, Y.A. Human Mobility and Spatio—Temporal Dynamics of COVID-19 in China: Comparing Survey Data and Big Data. Popul. Res. 2020, 44, 44–59. [Google Scholar]
- Bowen, J.T.; Laroe, C. Airline networks and the international diffusion of severe acute respiratory syndrome (SARS). Geogr. J. 2006, 172, 130–144. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.; Kim, Y.R.; O’Connell, J.F. COVID-19 and the aviation industry: The interrelationship between the spread of the COVID-19 pandemic and the frequency of flights on the EU market. Ann. Tour. Res. 2021, 91, 103298. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.C. Epidemic Spreading and Suppression on Temporal Chinese Aviation Network; Beijing Jiaotong University: Beijing, China, 2019. [Google Scholar]
- Zhao, S.; Zhuang, Z.; Ran, J. The association between domestic train transportation and novel coronavirus outbreak in China, from 2019 to 2020: A data-driven correlational report. Travel Med. Infect. Dis. 2020, 33, 101568. [Google Scholar] [CrossRef] [PubMed]
- Chen, X. and Yan G.H. Spreading Simulation Analysis of Infectious Disease Incident in Cities Network System of Northeast China. Geomat. World 2021, 28, 82–88. [Google Scholar]
- Wan, L.Y.; Wan, Q. The High-speed Railway Network and the Cross-town Transmission of Epidemics: Evidence from Chinese COVID-19. Rev. Ind. Econ. 2020, 114, 37–48. [Google Scholar]
- Cai, J.; Xu, B.; Chan, K.K.Y.; Zhang, X.; Zhang, B.; Chen, Z.; Xu, B. Roles of Different Transport Modes in the Spatial Spread of the 2009 Influenza A(H1N1) Pandemic in Mainland China. Int. J. Environ. Res. Public Health 2019, 16, 222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.; Cao, C.; Wang, Q.; Chen, Y.; Cao, Z.; Zhang, H.; Dong, L.; Zhao, J.; Xu, M.; Gao, M.; et al. The novel H1N1 influenza A global airline transmission and early warning without travel containments. Chin. Sci. Bull. 2010, 55, 1128–1133. [Google Scholar] [CrossRef]
- Fang, L.-Q.; Wang, L.-P.; de Vlas, S.J.; Liang, S.; Tong, S.-L.; Li, Y.-L.; Li, Y.-P.; Qian, Q.; Yang, H.; Zhou, M.-G.; et al. Distribution and Risk Factors of 2009 Pandemic Influenza A (H1N1) in Mainland China. Am. J. Epidemiol. 2012, 175, 890–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Kortoçi, P.; Motlagh, N.H.; Nurmi, P.; Tarkoma, S. A Survey of COVID-19 in Public Transportation Transmission Risk, Mitigation and Prevention. Multimodal Transp. 2022, 2022, 100030. [Google Scholar] [CrossRef]
- Oztig, L.I.; Askin, O.E. Human mobility and coronavirus disease 2019 (COVID-19): A negative binomial regression analysis. Public Health 2020, 185, 364–367. [Google Scholar] [CrossRef] [PubMed]
- Colizza, V.; Barrat, A.; Barthélemy, M.; Vespignani, A. The Role of the Airline Transportation Network in the Prediction and Predictability of Global Epidemics. Proc. Natl. Acad. Sci. USA 2006, 103, 2015–2020. [Google Scholar] [CrossRef] [Green Version]
- Zhu, P.; Guo, Y. The role of high-speed rail and air travel in the spread of COVID-19 in China. Travel Med. Infect. Dis. 2021, 42, 102097. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Lin, A.; Jiang, C.; Zhang, A.; Yang, Z. Influence of transportation network on transmission heterogeneity of COVID-19 in China. Transp. Res. Part C Emerg. Technol. 2021, 129, 103231. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.T.; Cai, W.X. Virus at the Gates: An Estimation of the Impact of Traffic Control in the Prevention of COVID-19. Rev. Ind. Econ. 2020, 4, 59–74. [Google Scholar]
- Yan, C.X.; Wang, B.; Chen, L.; Xiang, W.; Wang, Y.; Yan, X.D. Impacts of COVID-19 Traffic Control Policy on Population Flows in Changsha. J. Transp. Syst. Eng. Inf. Technol. 2021, 21, 190–197. [Google Scholar]
- Browne, A.; Ahmad, S.S.-O.; Beck, C.R.; Nguyen-Van-Tam, J.S. The roles of transportation and transportation hubs in the propagation of influenza and coronaviruses: A systematic review. J. Travel Med. 2016, 23, tav002. [Google Scholar] [CrossRef] [Green Version]
- Xu, F.; McCluskey, C.C.; Cressman, R. Spatial spread of an epidemic through public transportation systems with a hub. Math. Biosci. 2013, 246, 164–175. [Google Scholar] [CrossRef]
- Gaskin, D.J.; Zare, H.; Delarmente, B.A. Geographic disparities in COVID-19 infections and deaths: The role of transportation. Transp. Policy 2021, 102, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Kutela, B.; Combs, T.; Mwekh’iga, R.J.; Langa, N. Insights into the long-term effects of COVID-19 responses on transportation facilities. Transp. Res. Part D 2022, 111, 103463. [Google Scholar] [CrossRef]
- Wang, X.J.; Li, Q.S. Quantile Regression Analysis of Interannual Variation Characteristics of Landing Tropical Cyclones in China Under the Influence of ENSO Events. J. Trop. Meteorol. 2022, 38, 11–22. [Google Scholar]
- Dai, H.D.; Zhang, X.Y. Zero-Velocity Detection Algorithm for Inertial Pedestrian Navigation Based on Improved K-Means Clustering. Chin. J. Sens. Actuators 2022, 35, 115–121. [Google Scholar]
- Yang, X.S.; Wang, Q. Research on Hub Airport Evaluation Based on Cluster Analysis and DEA. Aeronaut. Comput. Tech. 2017, 47, 5–8. [Google Scholar]
- Tai, K.Y.; Dhaliwal, J.; Balasubramaniam, V. Leveraging Mann—Whitney U test on large-scale genetic variation data for analysing malaria genetic markers. Malar. J. 2022, 21, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Cui, M.; Yao, X.; Fang, H.; Zhang, Y.; Yang, D.; Pei, T. Spatial and Temporal Transmission Differences between SARS and COVID-19 and Analysis of Influence Factors. J. Geo-Inf. Sci. 2021, 23, 1910–1923. [Google Scholar]
- Koenker, R.; Bassett, E.G. Regression Quantiles. J. Econom. Soc. 1978, 1, 33–50. [Google Scholar] [CrossRef]
- Sajadi, M.M.; Habibzadeh, P.; Vintzileos, A.; Shokouhi, S.; Miralles-Wilhelm, F.; Amoroso, A. Temperature, humidity, and latitude analysis to predict potential spread and seasonality for COVID-19. Soc. Sci. Res. Netw. 2020. [Google Scholar] [CrossRef]
- Xu, Y.F. Statistical Diagnosis of the Negative Binomial Regression Model; Yangzhou University: Yangzhou, China, 2014. [Google Scholar]
- Sun, L.; Shang, Z.; Hu, H. Application of a Poisson Model and a Negative Binomial Regression Model in the Forest Fire Forecasting. Sci. Silvae Sin. 2012, 48, 126–129. [Google Scholar]
- Ni, D. How Wenzhou, 900 km From Wuhan, Went Into Total Lockdown. 2020. Available online: https://www.sixthtone.com/news/1005197/how-wenzhou%2C-900-km-from-wuhan%2C-went-into-total-lockdown (accessed on 15 April 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categories | Subjects | Epidemic | Findings | References |
|---|---|---|---|---|
| Influence of transportation modes on epidemic transmission | Air transportation | SARS |
| [4,6] |
| H1N1 | The results confirmed that there was a definite relationship between H1N1 and air travel. Additionally, the prevention measures were effective in containing the spread of virus. | [11] | ||
| COVID-19 |
| [5,13,14] | ||
| Railway transportation | COVID-19 |
| [8,9] | |
| Air, railway and road transportation | H1N1 |
| [10,12] | |
| COVID-19 |
| [1,7,15,16] | ||
| The role of transportation facilities in epidemic transmission | Airports | SARS | Airports were highly susceptible to the epidemic, from overall findings. | [20] |
| Transit stops | COVID-19 | Areas closer to transit stops had higher case numbers and fatality rates. | [22] | |
| All transportation facilities | The findings showed that responses instituted for economic recovery and public health were less likely to be long-term. | [23] |
| Iteration | Change of Clustering Center | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| K = 2 | K = 3 | K = 4 | |||||||
| 1 | 2 | 1 | 2 | 3 | 1 | 2 | 3 | 4 | |
| 1 | 282.861 | 472.872 | 197.474 | 190.283 | 223.367 | 126.837 | 44.238 | 72.258 | 157.254 |
| 2 | 16.424 | 119.873 | 2.135 | 25.949 | 87.703 | 11.968 | 94.562 | 3.557 | 43.450 |
| 3 | 9.339 | 58.619 | 5.356 | 22.958 | 22.871 | 0.907 | 47.560 | 3.904 | 44.634 |
| 4 | 1.674 | 11.558 | 6.477 | 28.990 | 44.285 | 0.000 | 37.307 | 7.528 | 23.667 |
| 5 | 4.910 | 32.456 | 6.246 | 21.258 | 19.936 | 0.907 | 26.226 | 6.446 | 22.286 |
| 6 | 3.243 | 19.649 | 3.064 | 7.354 | 0.000 | 0.876 | 26.038 | 6.098 | 19.781 |
| 7 | 0.000 | 0.000 | 3.008 | 12.162 | 20.092 | 0.881 | 33.784 | 15.498 | 0.000 |
| 8 | / | / | 2.974 | 11.754 | 18.702 | 1.739 | 9.610 | 7.484 | 0.000 |
| 9 | / | / | 1.971 | 4.409 | 0.000 | 1.690 | 5.149 | 4.876 | 0.000 |
| 10 | / | / | 1.965 | 4.312 | 0.000 | 2.520 | 0.000 | 4.035 | 0.000 |
| Variable | Sample Size | Symbols | Average Value | Standard Deviation | Minimum Value | Maximum Value |
|---|---|---|---|---|---|---|
| Population | 310 | 15.06 | 0.73 | 12.51 | 17.35 | |
| GDP | 310 | 25.95 | 0.96 | 23.03 | 28.97 | |
| Air transportation volume | 310 | 0.95 | 2.70 | 0 | 17 | |
| Railway transportation volume | 310 | 7.78 | 27.08 | 0 | 215 | |
| Road transportation volume | 310 | 37.48 | 178.34 | 0 | 1799 | |
| Number of airports | 310 | 0.65 | 0.67 | 0 | 4 | |
| Number of railway stations | 310 | 9.38 | 10.52 | 0 | 83 | |
| Number of bus stations | 310 | 7.59 | 5.51 | 1 | 52 | |
| Longitude | 310 | 113.17 | 7.97 | 80.27 | 131.16 | |
| Latitude | 310 | 32.80 | 6.82 | 18.25 | 52.34 | |
| Time of first diagnosis | 310 | 13.89 | 3.55 | 8 | 34 | |
| Cumulative number of confirmed cases | 310 | 97.41 | 316.70 | 1 | 3427 |
| Sample Size | Average | Variance | O-Value | p-Value |
|---|---|---|---|---|
| 310 | 97.4065 | 100,295.7954 | 12,786.0753 | 0.000 |
| Indicators | Type | Classification | Median | 25% Quantile | 75% Quantile | U-Value | z-Value | p-Value |
|---|---|---|---|---|---|---|---|---|
| v | Airport | 1 | 11 | 10 | 12 | 1032.5 | −7.6324 | 0.000 *** |
| 0 | 14 | 12 | 15 | |||||
| Railway station | 1 | 12 | 11 | 14 | 6445 | −6.1305 | 0.000 *** | |
| 0 | 14 | 12 | 16 | |||||
| Bus station | 1 | 12 | 10 | 13 | 4918.5 | −5.4228 | 0.000 *** | |
| 0 | 14 | 12 | 15 | |||||
| s | Airport | 1 | 71 | 39 | 197 | 1673 | −6.2875 | 0.000 *** |
| 0 | 17 | 7 | 42 | |||||
| Railway station | 1 | 44 | 17 | 120 | 5906 | −6.7931 | 0.000 *** | |
| 0 | 14 | 6 | 34 | |||||
| Bus station | 1 | 66 | 26 | 155 | 4067 | −6.6629 | 0.000 *** | |
| 0 | 15 | 7 | 38 |
| Variables | 0.05 (10 Days) | 0.25 (12 Days) | 0.55 (14 Days) | 0.85 (17 Days) |
|---|---|---|---|---|
| Population | 0.4547 | −0.0849 | 0.0688 | −0.6891 |
| GDP | −0.7139 ** | −0.6634 *** | −0.936 *** | −1.9686 *** |
| Air transportation volume | 0.0663 | −0.0924 ** | −0.2222 *** | −0.0996 |
| Railway transportation volume | −0.0034 | 0.0039 | 0.0115 | 0.0051 |
| Road transportation volume | −0.0007 | −0.0017 * | −0.0023 ** | −0.0028 |
| Number of airports | 0.0566 | −0.0192 | 0.1001 | −0.1466 |
| Number of railway stations | −0.0273 * | −0.0224 | −0.0106 | −0.0132 |
| Number of bus stations | −0.0558 | −0.0253 | −0.0126 | 0.034 |
| Longitude | −0.033 | −0.0393 ** | −0.0547 ** | −0.0688 * |
| Latitude | 0.0833 ** | 0.087 *** | 0.0821 *** | 0.0833 * |
| R2 | 0.1297 | 0.1558 | 0.1774 | 0.2390 |
| Variables | ||||
|---|---|---|---|---|
| OR Value | OR Value | |||
| Population | 0.2064 (1.6001) | 1.2293 | 0.1935 (1.4179) | 1.2135 |
| GDP | 0.4684 *** (4.0841) | 1.5975 | 0.5187 *** (4.3070) | 1.6798 |
| Air transportation volume | 0.0210 (0.6920) | 1.0212 | 0.0194 (0.6303) | 1.0196 |
| Railway transportation volume | 0.0105 *** (3.3774) | 1.0106 | 0.0113 *** (3.5985) | 1.0113 |
| Road transportation volume | 0.0065 *** (17.8622) | 1.0065 | 0.0050 *** (13.5560) | 1.005 |
| Number of airports | 0.0643 (0.6083) | 1.0664 | 0.0311 (0.2793) | 1.0316 |
| Number of railway stations | −0.0085 (−1.2351) | 0.9915 | −0.0081 (−1.1043) | 0.9919 |
| Number of bus stations | −0.0111 (−0.7008) | 0.9889 | −0.0085 (−0.5214) | 0.9915 |
| Longitude | 0.0331 *** (3.8528) | 1.0337 | 0.0254 *** (2.7176) | 1.0257 |
| Latitude | −0.0275 *** (2.6051) | 0.9729 | −0.0465 *** (4.1733) | 0.9546 |
| Infection Level | Prevention Level | Number of Infected Cities before Control | Number of Infected Cities after Control | Cumulative Number of Cases before Control | Cumulative Number of Cases after Control | Decline Percentage |
|---|---|---|---|---|---|---|
| 0–100 | High | 265 | 245 | 6287 | 4959 | 21.12% |
| Medium | 254 | 5337 | 15.11% | |||
| 100–300 | High | 26 | 26 | 4276 | 3113 | 27.20% |
| Medium | 26 | 3549 | 17.00% | |||
| 300–500 | High | 5 | 5 | 1977 | 1119 | 43.40% |
| Medium | 5 | 1440 | 27.16% | |||
| 500–1000 | High | 8 | 7 | 5950 | 3132 | 47.36% |
| Medium | 8 | 4164 | 30.02% | |||
| 1000–4000 | High | 6 | 6 | 11706 | 6947 | 40.65% |
| Medium | 6 | 8732 | 25.41% |
| Infection Level | Prevention Level | Number of Infected Cities before Control | Number of Infected Cities after Control | Cumulative Number of Cases before Control | Cumulative Number of Cases after Control | Decline Percentage |
|---|---|---|---|---|---|---|
| 0–100 | High | 265 | 253 | 6287 | 5248 | 16.53% |
| Medium | 256 | 5474 | 12.93% | |||
| 100–300 | High | 26 | 26 | 4276 | 3317 | 22.43% |
| Medium | 26 | 3607 | 15.65% | |||
| 300–500 | High | 5 | 5 | 1977 | 1248 | 36.87% |
| Medium | 5 | 1519 | 23.17% | |||
| 500–1000 | High | 8 | 8 | 5950 | 4295 | 27.82% |
| Medium | 8 | 4761 | 19.98% | |||
| 1000–4000 | High | 6 | 6 | 11706 | 7181 | 38.66% |
| Medium | 6 | 8878 | 24.16% |
| Prevention Strategies | Prevention Level | Cumulative Number of Cases before Control | Cumulative Number of Cases after Control | Decline Percentage | Control Efficiency |
|---|---|---|---|---|---|
| A | High | 30,196 | 19,271 | 36.18% | 0.181 |
| Medium | 23,223 | 23.09% | 0.184 | ||
| B | High | 21,288 | 29.50% | 0.236 | |
| Medium | 24,239 | 19.73% | 0.235 | ||
| C | High | 19,156 | 36.56% | 0.152 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bao, D.; Yin, L.; Tian, S.; Lv, J.; Wang, Y.; Wang, J.; Liao, C. Impact of Different Transportation Modes on the Transmission of COVID-19: Correlation and Strategies from a Case Study in Wuhan, China. Int. J. Environ. Res. Public Health 2022, 19, 15705. https://doi.org/10.3390/ijerph192315705
Bao D, Yin L, Tian S, Lv J, Wang Y, Wang J, Liao C. Impact of Different Transportation Modes on the Transmission of COVID-19: Correlation and Strategies from a Case Study in Wuhan, China. International Journal of Environmental Research and Public Health. 2022; 19(23):15705. https://doi.org/10.3390/ijerph192315705
Chicago/Turabian StyleBao, Danwen, Liping Yin, Shijia Tian, Jialin Lv, Yanjun Wang, Jian Wang, and Chaohao Liao. 2022. "Impact of Different Transportation Modes on the Transmission of COVID-19: Correlation and Strategies from a Case Study in Wuhan, China" International Journal of Environmental Research and Public Health 19, no. 23: 15705. https://doi.org/10.3390/ijerph192315705