
Lifestyle, Physical Activity and Dietary Habits of Medical Students of Wroclaw Medical University during the COVID-19 Pandemic



Abstract
:1. Introduction
2. Materials and Methods
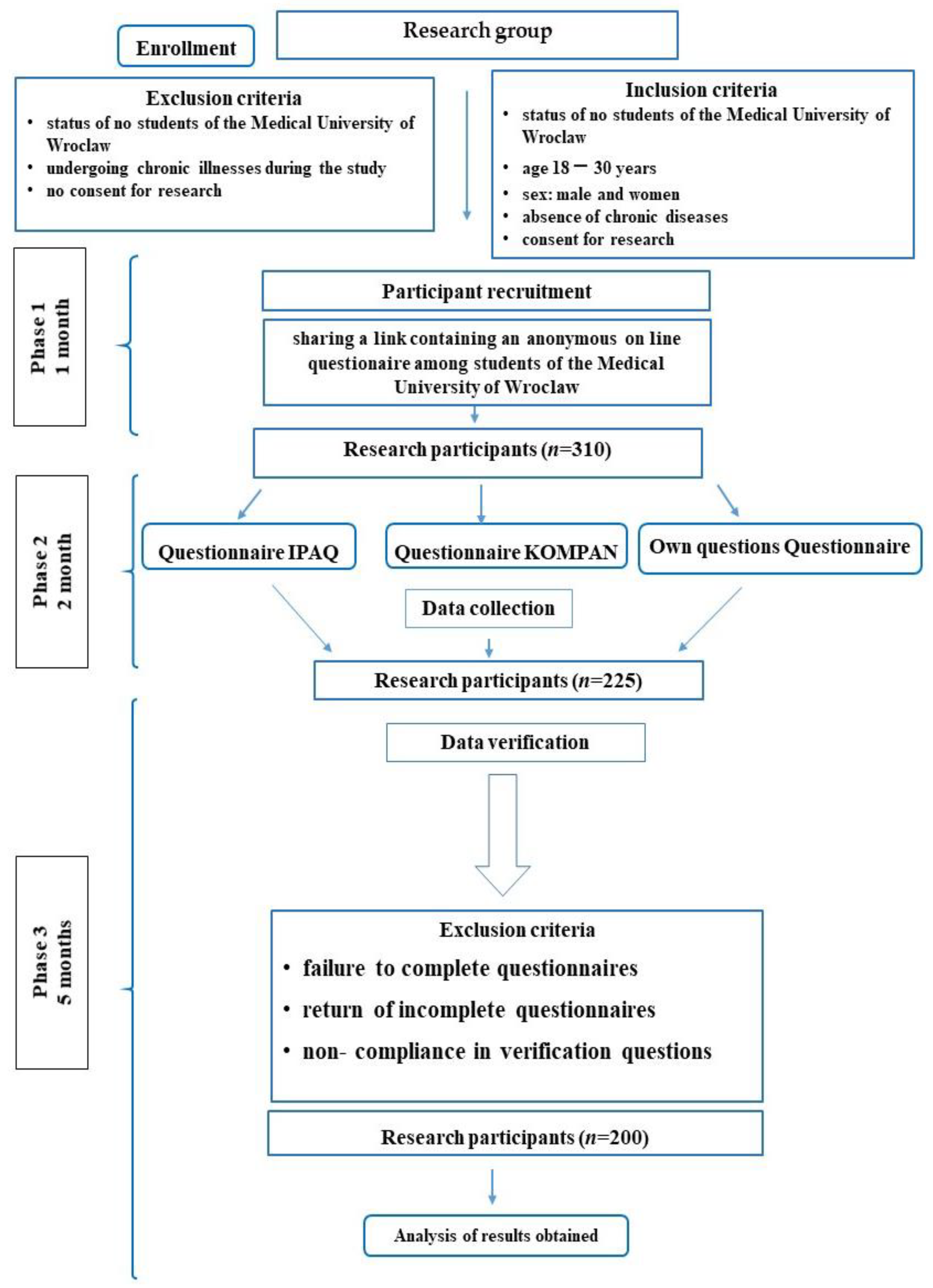
2.1. Study Design and Participants
2.2. Level of Physical Activity
2.3. Dietary Habits, Lifestyle, Diet Quality and Nutrition Knowledge
2.4. Own Questions Questionnaires
2.5. Statistical Analysis of Data
3. Results
3.1. Anthropometric Data and Place of Residence
3.2. Measurements of Physical Activity
3.3. Healthy and Unhealthy Diet Indexes, Nutritional Knowledge
3.4. Relationship between Diet Indexes and Nutritional Knowledge
3.5. Frequency of Food Consumption
3.6. Fast Food and Energy Drinks Consumption
3.7. Alcohol Consumption
3.8. Pandemic Restrictions, TV and Computer, Quality of Sleep
4. Discussion
4.1. Weight, BMI, Place of Residence
4.2. Nutritional Knowledge, Dietary Habits, Meals, Fast Food, Energy Drinks
4.3. Physical Activity
4.4. Alcohol and Cigarettes
4.5. Use of Computers, Sleep Quality and Impact of Pandemic
4.6. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hui, D.S.; Azhar, I.E.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; Mchugh, T.D.; Memish, Z.A.; Drosten, C.; et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—The latest 2019 novel coronavirus outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar] [CrossRef] [Green Version]
- Rothan, H.A.; Byrareddy, S.N. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef] [PubMed]
- Sumalla-Cano, S.; Forbes-Hernández, T.; Aparicio-Obregón, S.; Crespo, J.; Eléxpuru-Zabaleta, M.; Gracia-Villar, M.; Giampieri, F.; Elío, I. Changes in the lifestyle of the Spanish University population during confinement for COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 2210. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 13 April 2022).
- Summary Lockdown in Poland. Związek Przedsiębiorców I Pracodawców. Available online: https://zpp.net.pl/wp-content/uploads/2021/01/25.01.2021-Business-Paper-Podsumowanie-lockdownu-w-Polsce.pdf (accessed on 13 April 2022).
- Temporary Restrictions on the Operation of Institutions or Workplaces in the Period of an Epidemic Emergency. Available online: https://www.gov.pl/web/koronawirus/komunikat-w-sprawie-ograniczenia-funkcjonowania-instytucji-lub-zakladow-pracy-w-okresie-stanu-zagrozenia-epidemicznego-w-zwiazku-z-zakazeniami-wirusem-sars-cov-2 (accessed on 5 June 2022).
- Valentowitsch, J. Flattening the COVID-19 curve: The impact of contact restrictions on the infection curve in Germany. Gesundheitswesen 2020, 82, 646–648. [Google Scholar] [CrossRef] [PubMed]
- Sekulic, M.; Stajic, D.; Jurisic Skevin, A.; Kocovic, A.; Zivkovic Zaric, R.; Djonovic, N.; Vasiljevic, D.; Radmanovic, B.; Spasic, M.; Janicijevic, K.; et al. Lifestyle, physical activity, eating and hygiene habits: A comparative analysis before and during the COVID-19 pandemic in student population. Front. Public Health 2022, 10, 862816. [Google Scholar] [CrossRef]
- Gadi, N.; Saleh, S.; Johnson, J.A.; Trinidade, A. The impact of the COVID-19 pandemic on the lifestyle and behaviours, mental health and education of students studying healthcare-related courses at a British university. BMC Med. Educ. 2022, 22, 115. [Google Scholar] [CrossRef]
- Olfert, M.D.; Wattick, R.A.; Saurborn, E.G.; Hagedorn, R.L. Impact of COVID-19 on college student diet quality and physical activity. Nutr. Health 2022, 18, 2601060221086772. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary choices and habits during COVID-19 lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- Park, S.; Lee, S.H.; Yaroch, A.L.; Blanck, H.M. Reported changes in eating habits related to less healthy foods and beverages during the COVID-19 pandemic among US adults. Nutrients 2022, 14, 526. [Google Scholar] [CrossRef]
- Paltrinieri, S.; Bressi, B.; Costi, S.; Mazzini, E.; Cavuto, S.; Ottone, M.; De Panfilis, L.; Fugazzaro, S.; Rondini, E.; Giorgi Rossi, P. Beyond lockdown: The potential side effects of the SARS-CoV-2 pandemic on public health. Nutrients 2021, 13, 1600. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- El-Monshed, A.H.; Loutfy, A.; Saad, M.T.; Ali, A.S.; El-Gilany, A.H.; Soliman Mohamed, A.; Salah, M.; Zoromba, M. Satisfaction with life and psychological distress during the COVID-19 pandemic: An Egyptian online cross-sectional study. Afr. J. Prim. Health Care Fam. Med. 2022, 14, e1–e6. [Google Scholar] [CrossRef]
- Costi, S.; Paltrinieri, S.; Bressi, B.; Fugazzaro, S.; Giorgi Rossi, P.; Mazzini, E. Poor sleep during the first peak of the SARS-CoV-2 pandemic: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 306. [Google Scholar] [CrossRef]
- Fancourt, D.; Steptoe, A.; Bu, F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: A longitudinal observational study. Lancet 2021, 8, 141–149. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Jaffe, A.E.; Kumar, S.A.; Hultgren, B.A.; Smith-LeCavalier, K.N.; Garcia, T.A.; Canning, J.R.; Larimer, M.E. Meaning in life and stress-related drinking: A multicohort study of college students during the COVID-19 pandemic. Addict. Behav. 2022, 129, 107281. [Google Scholar] [CrossRef] [PubMed]
- Questionnaire. Available online: https://docs.google.com/forms/d/e/1FAIpQLSd4wz7OzFrxKpWHCPejboX6brWm05p9x6DiufFwXSs02xwzzQ/viewform?fbclid=IwAR34874vK_quYecsZBSMFg8LloJTsJ-wad6wHYnfRxv5qeDwp1x3JX7tF-I&fbzx=-569072893013937368 (accessed on 13 April 2022).
- Martínez-Mesa, J.; González-Chica, D.A.; Duquia, R.P.; Bonamigo, R.R.; Bastos, J.L. Sampling: How to select participants in my research study? An. Bras. Dermatol. 2016, 91, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Biernat, E.; Stupnicki, R.; Gajewski, A. International physical activity questionnaire (IPAQ)—Polish version. Wych. Fizyczne Sport 2007, 51, 47–54. [Google Scholar]
- IPAQ. Available online: https://sites.google.com/site/theipaq/scoring-protocol (accessed on 13 April 2022).
- Kowalkowska, J.; Wadolowska, L.; Czarnocinska, J.; Czlapka-Matyasik, M.; Galinski, G.; Jezewska-Zychowicz, M.; Bronkowska, M.; Dlugosz, A.; Loboda, D.; Wyka, J. Reproducibility of a questionnaire for dietary habits, lifestyle and nutrition knowledge assessment (KomPAN) in Polish adolescents and adults. Nutrients 2018, 10, 1845. [Google Scholar] [CrossRef] [Green Version]
- Kawalec, W.; Grenda, R.; Ziółkowska, H.; Bernatowska, E.; Chmielik, M.; Czerwionka-Szaflarska, M. Pediatria; PZWL: Warszawa, Poland, 2013; ISBN 978-83-200-4309-9. [Google Scholar]
- Demographic Situation of Poland, Report 2019–2020; The Government Population Council: Warsaw, Poland, 2020; ISBN 978-83-66466-36-4. (In Polish)
- Sánchez-Sánchez, E.; Ramírez-Vargas, G.; Avellaneda-López, Y.; Orellana-Pecino, J.I.; García-Marín, E.; Díaz-Jimenez, J. Eating habits and physical activity of the Spanish population during the COVID-19 pandemic period. Nutrients 2020, 12, 2826. [Google Scholar] [CrossRef]
- Reyes-Olavarría, D.; Latorre-Román, P.Á.; Guzmán-Guzmán, I.P.; Jerez-Mayorga, D.; Caamaño-Navarrete, F.; Delgado-Floody, P. Positive and negative changes in food habits, physical activity patterns, and weight status during COVID-19 confinement: Associated factors in the chilean population. Int. J. Environ. Res. Public Health 2020, 17, 5431. [Google Scholar] [CrossRef] [PubMed]
- Poelman, M.P.; Gillebaart, M.; Schlinkert, C.; Dijkstra, S.C.; Derksen, E.; Mensink, F.; Hermans, R.C.J.; Aardening, P.; de Ridder, D.; de Vet, E. Eating behavior and food purchases during the COVID-19 lockdown: A cross-sectional study among adults in the Netherlands. Appetite 2021, 157, 105002. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhu, W.; Kang, S.; Qiu, L.; Lu, Z.; Sun, Y. Association between physical activity and mood states of children and adolescents in social isolation during the COVID-19 epidemic. Int. J. Environ. Res. Public Health 2020, 17, 7666. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Guo, T.; Becker, B.; Yu, Q.; Chen, S.T.; Brendon, S.; Hossain, M.M.; Cunha, P.M.; Soares, F.C.; Veronese, N.; et al. Depression is associated with moderate-intensity physical activity among college students during the COVID-19 pandemic: Differs by activity level, gender and gender role. Psychol. Res. Behav. Manag. 2020, 13, 1123–1134. [Google Scholar] [CrossRef] [PubMed]
- Ashdown-Franks, G.; Sabiston, C.M.; Stubbs, B. The evidence for physical activity in the management of major mental illnesses: A concise overview to inform busy clinicians’ practice and guide policy. Curr. Opin. Psychiatry 2019, 32, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Romero-Blanco, C.; Rodríguez-Almagro, J.; Onieva-Zafra, M.D.; Parra-Fernández, M.L.; Prado-Laguna, M.d.C.; Hernández-Martínez, A. Physical activity and sedentary lifestyle in university students: Changes during confinement due to the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6567. [Google Scholar] [CrossRef] [PubMed]
- Bryl, N.; Czarnecka-Iwańczuk, M.; Romanowska, M.; Stanišić, M.-G.; Michalak, M.; Posadzy-Małaczyńska, A. Drinking alcohol as a way of coping with stress in students of medical faculties. Psychiatr. Pol. 2020, 54, 265–277. [Google Scholar] [CrossRef]
- Grossman, E.R.; Benjamin-Neelon, S.E.; Sonnenschein, S. Alcohol consumption during the COVID-19 pandemic: A cross-sectional survey of US adults. Int. J. Environ. Res. Public Health 2020, 17, 9189. [Google Scholar] [CrossRef]
- Koopmann, A.; Georgiadou, E.; Reinhard, I.; Müller, A.; Lemenager, T.; Kiefer, F.; Hillemacher, T. The effects of the lockdown during the COVID-19 pandemic on alcohol and tobacco consumption behavior in Germany. Eur. Addict. Res. 2021, 27, 242–256. [Google Scholar] [CrossRef]
- Rehm, J.; Kilian, C.; Ferreira-Borges, C.; Jernigan, D.; Monteiro, M.; Parry, C.D.H.; Sanchez, Z.M.; Manthey, J. Alcohol use in times of the COVID 19: Implications for monitoring and policy. Drug Alcohol Rev. 2020, 39, 301–304. [Google Scholar] [CrossRef]
- Tran, T.D.; Hammarberg, K.; Kirkman, M.; Nguyen, H.T.M.; Fisher, J. Alcohol use and mental health status during the first months of COVID-19 pandemic in Australia. J Affect Disord. 2020, 277, 810–813. [Google Scholar] [CrossRef] [PubMed]
- Carreras, G.; Lugo, A.; Stival, C.; Amerio, A.; Odone, A.; Pacifici, R.; Gallus, S.; Gorini, G. Impact of COVID-19 lockdown on smoking consumption in a large representative sample of Italian adults. Tob. Control. 2021. [Google Scholar] [CrossRef] [PubMed]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef] [PubMed]
- Kosendiak, A.; Król, M.; Ściskalska, M.; Kepinska, M. The changes in stress coping, alcohol use, cigarette smoking and physical activity during COVID-19 related lockdown in medical students in Poland. Int. J. Environ. Res. Public Health 2021, 19, 302. [Google Scholar] [CrossRef] [PubMed]
- Faccioli, S.; Lombardi, F.; Bellini, P.; Costi, S.; Sassi, S.; Pesci, M.C. How did italian adolescents with disability and parents deal with the COVID-19 emergency? Int. J. Environ. Res. Public Health 2021, 18, 1687. [Google Scholar] [CrossRef] [PubMed]
- Mishra, J.; Panigrahi, A.; Samanta, P.; Dash, K.; Mahapatra, P.; Behera, M.R. Sleep quality and associated factors among undergraduate medical students during COVID-19 confinement. Clin. Epidemiol. Glob. Health 2022, 15, 101004. [Google Scholar] [CrossRef]
- Katona, Z.B.; Takács, J.; Kerner, L.; Alföldi, Z.; Soós, I.; Gyömörei, T.; Podstawski, R.; Ihász, F. Physical activity and screen time among Hungarian high school students during the COVID-19 pandemic caused distance education period. Int. J. Environ. Res. Public Health 2021, 18, 13024. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Ferracuti, S.; De Giglio, O.; Caggiano, G.; Protano, C.; Valeriani, F.; Parisi, E.A.; Valerio, G.; Liguori, G.; et al. Sedentary behaviors and physical activity of Italian undergraduate students during lockdown at the time of COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6171. [Google Scholar] [CrossRef]
- Majumdar, P.; Biswas, A.; Sahu, S. COVID-19 pandemic and lockdown: Cause of sleep disruption, depression, somatic pain, and increased screen exposure of office workers and students of India. Chronobiol. Int. 2020, 37, 1191–1200. [Google Scholar] [CrossRef]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during COVID-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef] [PubMed]
- Munasinghe, S.; Sperandei, S.; Freebairn, L.; Conroy, E.; Jani, H.; Marjanovic, S.; Page, A. The impact of physical distancing policies during the COVID-19 pandemic on health and well-being among Australian adolescents. J. Adolesc. Health 2020, 67, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Savage, M.J.; James, R.; Magistro, D.; Donaldson, J.; Healy, L.C.; Nevill, M.; Hennis, P.J. Mental health and movement behaviour during the COVID-19 pandemic in UK university students: Prospective cohort study. Ment. Health Phys. Act. 2020, 19, 100357. [Google Scholar] [CrossRef]
- Schlichtiger, J.; Brunner, S.; Steffen, J.; Huber, B.C. Mental health impairment triggered by the COVID-19 pandemic in a sample population of German students. J. Investig. Med. 2020, 68, 1394–1396. [Google Scholar] [CrossRef] [PubMed]
- Chwałczyńska, A.; Andrzejewski, W. Changes in body mass and composition of the body as well as physical activity and time spent in front of the monitor by students of the Wroclaw University of Health and sport sciences during the period of COVID-19 restrictions. Int. J. Environ. Res. Public Health 2021, 18, 7801. [Google Scholar] [CrossRef] [PubMed]
- Saguem, B.N.; Nakhli, J.; Romdhane, I.; Nasr, S.B. Predictors of sleep quality in medical students during COVID-19 confinement. Encephale 2022, 48, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Bosi Bağcı, T.A.; Kanadıkırık, A.; Somyürek, E.; Gerçek, G.; Tanrıkulu, H.B.; Öntaş, E.; Uzun, S. Impact of COVID-19 on eating habits, sleeping behaviour and physical activity status of final-year medical students in Ankara, Turkey. Public Health Nutr. 2021, 24, 6369–6376. [Google Scholar] [CrossRef] [PubMed]
- Luciano, F.; Cenacchi, V.; Vegro, V.; Pavei, G. COVID-19 lockdown: Physical activity, sedentary behaviour and sleep in Italian medicine students. Eur. J. Sport Sci. 2021, 21, 1459–1468. [Google Scholar] [CrossRef] [PubMed]
- Olarte-Durand, M.; Roque-Aycachi, J.B.; Rojas-Humpire, R.; Canaza-Apaza, J.F.; Laureano, S.; Rojas-Humpire, A.; Huancahuire-Vega, S. Estado de ánimo y calidad del sueño en estudiantes de medicina peruanos durante la pandemia de COVID-19 [Mood and sleep quality in Peruvian medical students during COVID-19 pandemic]. Rev. Colomb. Psiquiatr. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Watson, N.F.; Badr, M.S.; Belenky, G.; Bliwise, D.L.; Buxton, O.; Buysse, D.; Dinges, D.F.; Gangwisch, J.; Grandner, M.A.; Kushida, C.; et al. Recommended amount of sleep for a healthy adult: A joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep 2015, 38, 843–844. [Google Scholar] [CrossRef]


{kind=link}
| Activity in School/Work | Activity in Free Time | ||
|---|---|---|---|
| Low | Moderate | High | |
| Low | Low | Low | Medium |
| Moderate | Low | Medium | Medium |
| High | Medium | Medium | High |
| March 2020 (n = 200) | October 2020 (n = 200) | p-Value | |
|---|---|---|---|
| Sex | N.A. | ||
| Male Female | 65 (32.5%) 135 (67.5%) | 65 (32.5%) 135 (67.5%) | |
| Age (years) (Mean ± SD) | 19.5 ± 0.6 | 19.9 ± 0.6 | N.A. |
| Height (centimetres) (Mean ± SD) | 171.9 ± 9 | 171.9 ± 9 | N.A. |
| Weight (kilograms) (Mean ± SD) | 63.9 ± 11.5 | 64.3 ± 11.5 | 0.068 |
| Body Mass Index (Mean ± SD) | 0.180 | ||
| <18.5 Underweight 18.5–24.9 Normal | 16 (8%) 169 (84.5%) | 13 (6.5%) 170 (85%) | |
| Weight | |||
| 25.0–29.9 | 13 (6.5%) | 14 (7%) | |
| Overweight | |||
| >29.9 Obese | 2 (1%) | 3 (1.5%) | |
| Inhabitancy | 0.001 | ||
| City > 500,000 | 38 (19%) | 52 (26%) | |
| City 500,000–100,000 | 25 (12.5%) | 25 (12.5%) | |
| Town 100,000–50,000 | 24 (12%) | 27 (13.5%) | |
| Town 50,000–20,000 | 34 (17%) | 28 (14%) | |
| Town 20,000–5000 | 15 (7.5%) | 10 (5%) | |
| Village | 64 (32%) | 58 (29%) |
| March 2020 (n = 200) | October 2020 (n = 200) | p-Value | |
|---|---|---|---|
| International Physical Activity Questionnaire (IPAQ) | 0.181 | ||
| Low | 137 (68.5%) | 158 (79%) | |
| Average | 40 (20%) | 17 (8.5%) | |
| High | 23 (11.5%) | 25 (12.5%) | |
| How much time did you average spend walking during the day? (minutes) (Mean ± SD) | 25.3 ± 62.9 | 48.3 ± 45.5 | <0.001 |
| How much time did you average spend sitting during the day? (minutes) (Mean ± SD) | 251.5 ± 507.8 | 403.4 ± 330.5 | <0.001 |
| Physical activity (from KomPAN) | 0.718 | ||
| Low | 128 (64%) | 122 (61%) | |
| Moderate | 71 (35.5%) | 72 (36%) | |
| High | 1 (0.5%) | 6 (3%) |
| March 2020 (n = 200) | October 2020 (n = 200) | p-Value | |
|---|---|---|---|
| Pro-Healthy Diet Index (pHDI-10) | 0.001 | ||
| Low | 156 (78%) | 178 (89%) | |
| Average | 44 (22%) | 22 (11%) | |
| High | 0 | 0 | |
| Non-Healthy Diet Index (nHDI-14) | 0.649 | ||
| Low | 197 (98.5%) | 196 (98%) | |
| Average | 3 (1.5%) | 4 (2%) | |
| High | 0 (0%) | 0 (0%) | |
| Level of nutritional knowledge | <0.001 | ||
| Insufficient | 9 (4.5%) | 42 (21%) | |
| Sufficient | 118 (59%) | 123 (61.5%) | |
| Good | 73 (36.5%) | 35 (17.5%) |
| March 2020 (n = 200) | October 2020 (n = 200) | p-Value | |
|---|---|---|---|
| How many meals do you usually consume daily? | 0.716 | ||
| 1 | 1 (0.5%) | 0 | |
| 2 | 13 (6.5%) | 20 (10%) | |
| 3 | 77 (38.5%) | 69 (34.5%) | |
| 4 | 78 (39%) | 81 (40.5%) | |
| 5 or more | 31 (15.5%) | 30 (15%) | |
| Do you consume meals at a regular time? | 0.435 | ||
| No | 56 (28%) | 62 (31%) | |
| Yes, but only some of them | 104 (52%) | 103 (51.5%) | |
| Yes, all of them | 40 (20%) | 35 (17.5%) | |
| How often do you snack between the meals ? | 0.061 | ||
| Never | 6 (3%) | 8 (4%) | |
| 1–3 times per month | 7 (3.5%) | 12 (6%) | |
| Once per week | 20 (10%) | 22 (11%) | |
| Few times per week | 67 (33.5%) | 75 (37.5%) | |
| Once per day | 43 (21.5%) | 37 (18.5%) | |
| Few times per day | 57 (28.5%) | 46 (23%) | |
| How often do you drink energy drinks ? | 0.019 | ||
| Never | 137 (68.5%) | 110 (55%) | |
| 1–3 times per month | 45 (22.5%) | 58 (29%) | |
| Once per week | 12 (6%) | 27 (13.5%) | |
| Few times per week | 5 (2.5%) | 4 (2%) | |
| Once per day | 0 | 1 (0.5%) | |
| Few times per day | 1 (0.5%) | 0 | |
| How often do you eat fast food ? | <0.001 | ||
| Never | 25 (12.5%) | 16 (8%) | |
| 1–3 times per month | 129 (64.5%) | 71 (35.5%) | |
| Once per week | 33 (16.5%) | 54 (27%) | |
| Few times per week | 12 (6%) | 54 (27%) | |
| Once per day | 1 (0.5%) | 4 (2%) | |
| Few times per day | 0 | 1 (0.5%) | |
| How often do you drink alcohol ? | <0.001 | ||
| Never | 44 (22%) | 107 (53.5%) | |
| 1–3 times per month | 101 (50.5%) | 60 (30%) | |
| Once per week | 39 (19.5%) | 22 (11%) | |
| Few times per week | 15 (7.5%) | 9 (4.5%) | |
| Once per day | 0 | 1 (0.5%) | |
| Few times per day | 1 (0.5%) | 1 (0.5%) | |
| Smoking (No. and %) | 0.004 | ||
| No | 189 (94.5%) | 174 (87%) | |
| Yes | 11 (5.5%) | 26 (13%) |
| Mar-20 | Oct-20 | p-Value | |
|---|---|---|---|
| (n = 200) | (n = 200) | ||
| How many hours per day do you spend on average sleeping? | 0.922 | ||
| 6 and less | 51 (25.5%) | 49 (24.5%) | |
| From 6 to 9 | 137 (68.5%) | 140 (70%) | |
| 9 and more | 12 (6%) | 11 (5.5%) | |
| How many hours per day do you spend on average watching TV or in front of a computer? | 0.801 | ||
| 2 and less | 14 (7%) | 25 (12.5%) | |
| From 2 to 4 | 45 (22.5%) | 31 (15.5%) | |
| From 4 to 6 | 59 (29.5%) | 60 (30%) | |
| From 6 to 8 | 57 (28.5%) | 57 (28.5%) | |
| From 8 to 10 | 17 (8.5%) | 21 (10.5%) | |
| 10 and more | 8 (4%) | 6 (3%) | |
| Has the pandemic situation affected you? | <0.001 | ||
| Negatively | 79 (39.5%) | 117 (58.5%) | |
| Positively | 16 (8%) | 13 (6.5%) | |
| Unaffected | 27 (13.5%) | 18 (9%) | |
| No opinion | 78 (39%) | 52 (26%) | |
| Are you subject to any pandemic restrictions? | 0.002 | ||
| No restrictions | 39 (19.5%) | 70 (35%) | |
| Only government restrictions | 155 (77.5%) | 124 (62%) | |
| Quarantine | 4 (2%) | 6 (3%) | |
| Epidemiological surveillance | 2 (1%) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosendiak, A.A.; Wysocki, M.P.; Krysiński, P.P. Lifestyle, Physical Activity and Dietary Habits of Medical Students of Wroclaw Medical University during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 7507. https://doi.org/10.3390/ijerph19127507
Kosendiak AA, Wysocki MP, Krysiński PP. Lifestyle, Physical Activity and Dietary Habits of Medical Students of Wroclaw Medical University during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(12):7507. https://doi.org/10.3390/ijerph19127507
Chicago/Turabian StyleKosendiak, Aureliusz Andrzej, Michał Piotr Wysocki, and Paweł Piotr Krysiński. 2022. "Lifestyle, Physical Activity and Dietary Habits of Medical Students of Wroclaw Medical University during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 12: 7507. https://doi.org/10.3390/ijerph19127507