
Optimizing Strategies for Improving Mental Health in Victoria, Australia during the COVID-19 Era: A System Dynamics Modelling Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Model Structure
- A population component that models the changes in population sizes across different age groups and geographic remoteness groups as governed by birth, mortality, overseas migration, and internal migration rates;
- An education component that captures the commencement, discontinuation, and completion of post-secondary education and vocational studies;
- An employment component that models the flows between employment, underemployment, unemployment, and not participating in the labour force;
- A psychopathological vulnerability component that captures the increased risk of developmentally vulnerable children developing mental health disorders as they age into adulthood;
- A psychological distress component that models the onset of and recovery from moderate to very high psychological distress as measured by the Kessler Psychological Distress Scale (K10) [35] (score 16–50) in the population;
- A mental health services component that models the flow of psychologically distressed, help-seeking people through various services pathways, including general practitioners, psychiatrists, allied health services, hospitals, and community mental health services;
- A suicidal behaviour component that models self-harm hospitalisations and suicide deaths; and
- A COVID-19 pandemic component that models the impact of the pandemic and the resulting public health orders on labour force transitions, overseas migration, psychological distress levels, and mental health services demand and usage.
2.2. Data Sources
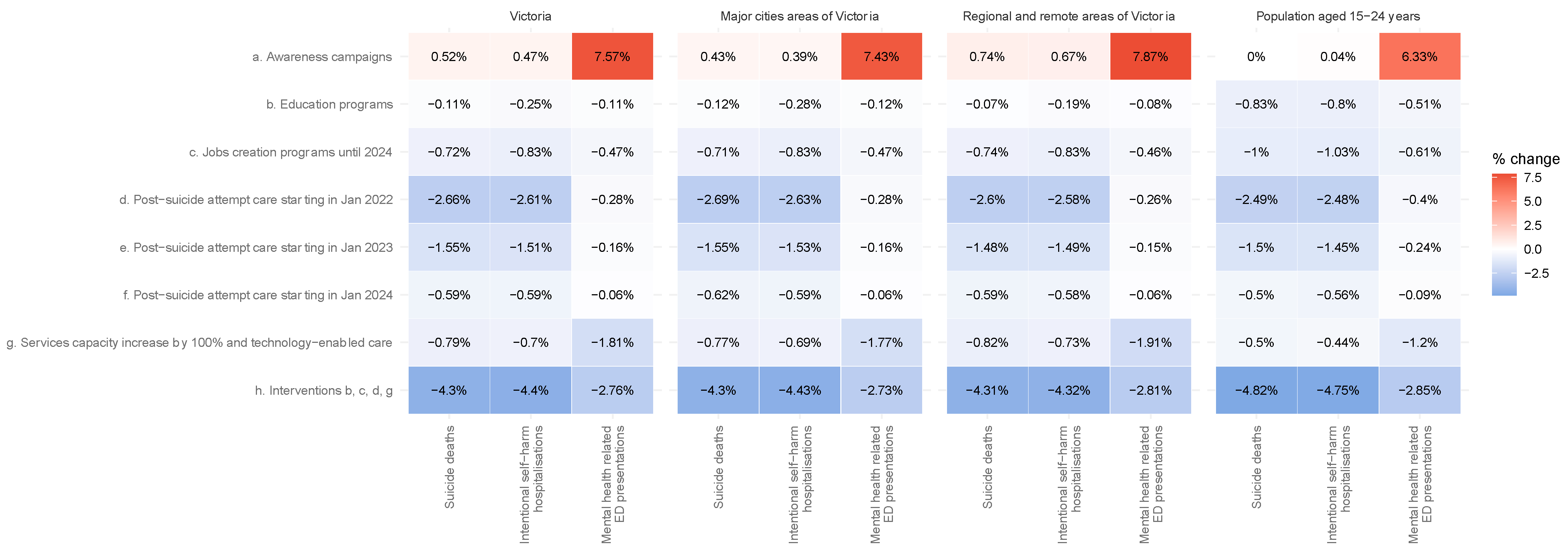
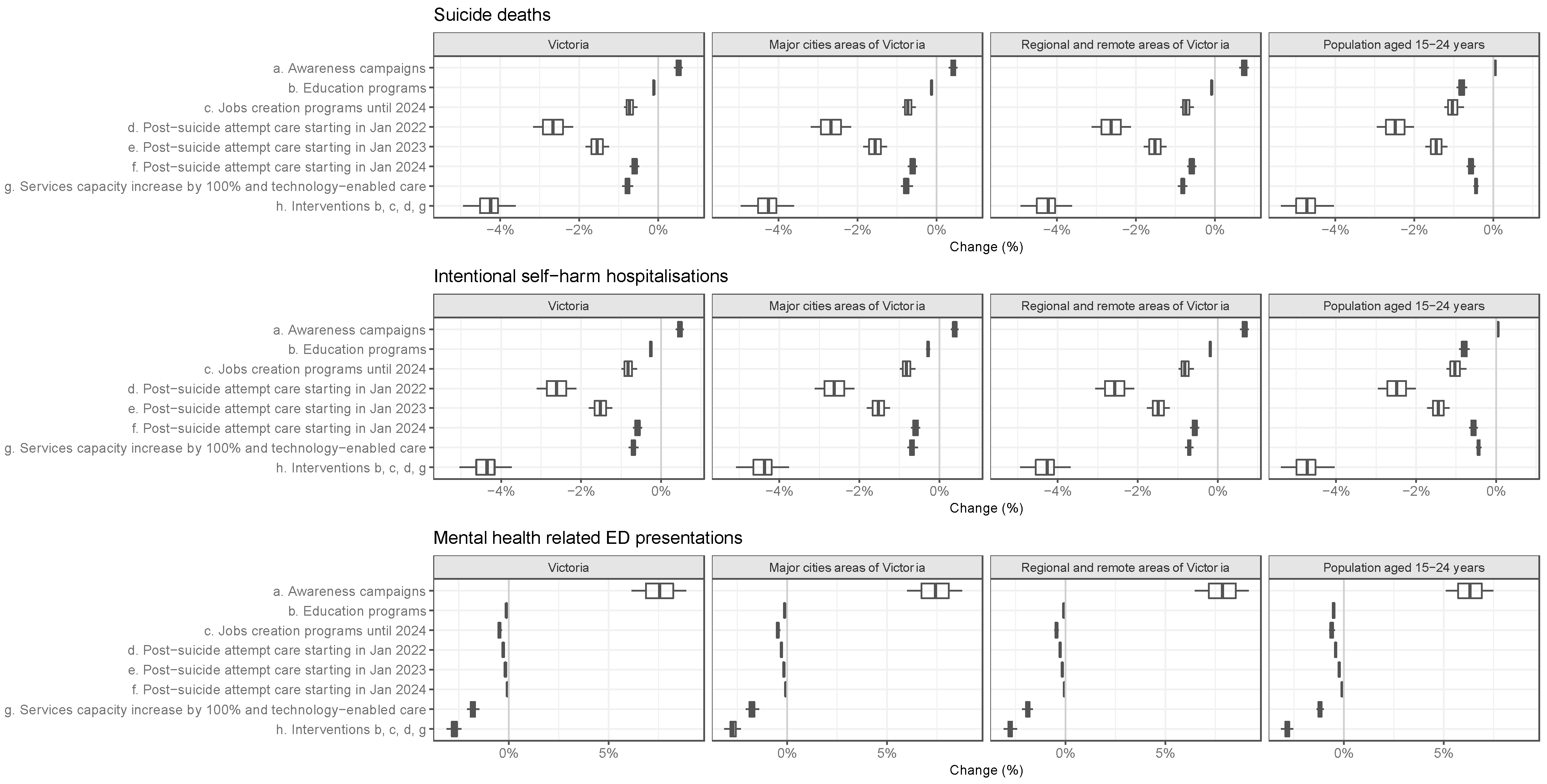
2.3. Interventions Tested
2.4. Assumptions
2.5. Projected Outcomes
2.6. Sensitivity Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- COVID-19 Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Power, E.; Hughes, S.; Cotter, D.; Cannon, M. Youth mental health in the time of COVID-19. Ir. J. Psychol. Med. 2020, 37, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, P.; Hammarstrom, A.; Janlert, U. Children of boom and recession and the scars to the mental health—A comparative study on the long term effects of youth unemployment. Int. J. Equity Health 2016, 15, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Power, E.; Clarke, M.; Kelleher, I.; Coughlan, H.; Lynch, F.; Connor, D.; Fitzpatrick, C.; Harley, M.; Cannon, M. The association between economic inactivity and mental health among young people: A longitudinal study of young adults who are not in employment, education or training. Ir. J. Psychol. Med. 2015, 32, 155–160. [Google Scholar] [CrossRef] [PubMed]
- O’Dea, B.; Glozier, N.; Purcell, R.; McGorry, P.D.; Scott, J.; Feilds, K.L.; Hermens, D.F.; Buchanan, J.; Scott, E.M.; Yung, A.R.; et al. A cross-sectional exploration of the clinical characteristics of disengaged (NEET) young people in primary mental healthcare. BMJ Open 2014, 4, e006378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- World Health Organisation: Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 1 February 2022).
- Tay, J.H.; Porter, A.F.; Wirth, W.; Duchene, S. The Emergence of SARS-CoV-2 Variants of Concern Is Driven by Acceleration of the Substitution Rate. Mol. Biol. Evol. 2022, 39, msac013. [Google Scholar] [CrossRef] [PubMed]
- Amoutzias, G.D.; Nikolaidis, M.; Tryfonopoulou, E.; Chlichlia, K.; Markoulatos, P.; Oliver, S.G. The Remarkable Evolutionary Plasticity of Coronaviruses by Mutation and Recombination: Insights for the COVID-19 Pandemic and the Future Evolutionary Paths of SARS-CoV-2. Viruses 2022, 14, 78. [Google Scholar] [CrossRef]
- Miot, E.F.; Worthington, B.M.; Ng, K.H.; de Lataillade, L.D.G.; Pierce, M.P.; Liao, Y.; Ko, R.; Shum, M.H.; Cheung, W.Y.; Holmes, E.C.; et al. Surveillance of Rodent Pests for SARS-CoV-2 and Other Coronaviruses, Hong Kong. Emerg. Infect. Dis. 2022, 28, 467–470. [Google Scholar] [CrossRef]
- Callaway, E. Beyond Omicron: What’s next for COVID’s viral evolution. Nature 2021, 600, 204–207. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. National, State and Territory Population. June 2021. Available online: https://www.abs.gov.au/statistics/people/population/national-state-and-territory-population/jun-2021#states-and-territories (accessed on 11 January 2022).
- Australian Bureau of Statistics. Regional Population. 2019–2020. Available online: https://www.abs.gov.au/statistics/people/population/regional-population/2019-20 (accessed on 11 January 2022).
- Australian Bureau of Statistics. Education and Work. May 2020. Available online: https://www.abs.gov.au/statistics/people/education/education-and-work-australia/may-2020 (accessed on 11 January 2022).
- Australian Bureau of Statistics. Labour Force. February 2022. Available online: https://www.abs.gov.au/statistics/labour/employment-and-unemployment/labour-force-australia/feb-2022#states-and-territories (accessed on 20 March 2022).
- Australian Institute of Health and Welfare. Suicide & SELF-Harm Monitoring. 2020. Available online: https://www.aihw.gov.au/suicide-self-harm-monitoring (accessed on 11 January 2022).
- Australian Bureau of Statistics. Causes of Death. 2019. Available online: https://www.abs.gov.au/statistics/health/causes-death/causes-death-australia/2019 (accessed on 15 April 2021).
- Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS): Volume 1—Main Structure and Greater Capital City Statistical Areas. July 2016. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/Lookup/1270.0.55.001Main+Features10018July%202016?OpenDocument (accessed on 12 April 2021).
- Australian Bureau of Statistics. Data by Region. 2020. Available online: https://dbr.abs.gov.au/ (accessed on 12 April 2021).
- Royal Commission into Victoria’s Mental Health System. Final Report: Summary and Recommendations. Parl Paper No. 202, Session 2018–21 (document 1 of 6). 2021. pp. 3, 8. Available online: https://finalreport.rcvmhs.vic.gov.au/wp-content/uploads/2021/02/RCVMHS_FinalReport_ExecSummary_Accessible.pdf (accessed on 10 July 2021).
- Victoria Department of Health Pandemic Order Register. Available online: https://www.health.vic.gov.au/covid-19/pandemic-order-register (accessed on 15 October 2021).
- Australian Bureau of Statistics. Labour Force. March 2021. Available online: https://www.abs.gov.au/statistics/labour/employment-and-unemployment/labour-force-australia/mar-2021 (accessed on 11 April 2021).
- Victorian Health Promotion Foundation. VicHealth Coronavirus Victorian Wellbeing Impact Survey: Follow up Survey; Victorian Health Promotion Foundation: Melbourne, Australia, 2020. [Google Scholar]
- Australian Bureau of Statistics. Household Impacts of COVID-19 Survey. June 2021. Available online: https://www.abs.gov.au/statistics/people/people-and-communities/household-impacts-covid-19-survey/latest-release (accessed on 10 July 2021).
- Australian Government. The Treasury: JobKeeper Payment. Available online: https://treasury.gov.au/coronavirus/jobkeeper (accessed on 15 April 2021).
- Australian Government. Better Access Initiative. Available online: https://www.health.gov.au/initiatives-and-programs/better-access-initiative (accessed on 15 April 2021).
- Head to Health Mental Health Service in Victoria. Available online: https://headtohealthvic.org.au/about/ (accessed on 7 May 2022).
- Head to Health Web Portal—Digital Mental Health Services. Available online: https://www.headtohealth.gov.au/ (accessed on 7 May 2022).
- Kompas, T.; Grafton, R.Q.; Che, T.N.; Chu, L.; Camac, J. Health and economic costs of early and delayed suppression and the unmitigated spread of COVID-19: The case of Australia. PLoS ONE 2021, 16, e0252400. [Google Scholar]
- Atkinson, J.A.; Song, Y.J.C.; Merikangas, K.R.; Skinner, A.; Prodan, A.; Iorfino, F.; Freebairn, L.; Rose, D.; Ho, N.; Crouse, J.; et al. The Science of Complex Systems Is Needed to Ameliorate the Impacts of COVID-19 on Mental Health. Front. Psychiatry 2020, 11, 606035. [Google Scholar] [CrossRef]
- Atkinson, J.A.; Skinner, A.; Lawson, K.; Rosenberg, S.; Hickie, I.B. Bringing new tools, a regional focus, resource-sensitivity, local engagement and necessary discipline to mental health policy and planning. BMC Public Health 2020, 20, 814. [Google Scholar] [CrossRef]
- Occhipinti, J.A.; Skinner, A.; Doraiswamy, P.M.; Fox, C.; Herrman, H.; Saxena, S.; London, E.; Song, Y.J.C.; Hickie, I.B. Mental health: Build predictive models to steer policy. Nature 2021, 597, 633–636. [Google Scholar] [CrossRef]
- Atkinson, J.A.; Skinner, A.; Hackney, S.; Mason, L.; Heffernan, M.; Currier, D.; King, K.; Pirkis, J. Systems modelling and simulation to inform strategic decision making for suicide prevention in rural New South Wales (Australia). Aust. N. Z. J. Psychiatry 2020, 54, 892–901. [Google Scholar] [CrossRef]
- Caldwell, T.M.; Jorm, A.F.; Dear, K.B. Suicide and mental health in rural, remote and metropolitan areas in Australia. Med. J. Aust. 2004, 181, S10–S14. [Google Scholar] [CrossRef]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. National, State and Territory Population. June 2020. Available online: https://www.abs.gov.au/statistics/people/population/national-state-and-territory-population/jun-2020 (accessed on 12 April 2021).
- Australian Bureau of Statistics. Labour Force, Detailed. Volume. February 2021. Available online: https://www.abs.gov.au/statistics/labour/employment-and-unemployment/labour-force-australia-detailed/feb-2021 (accessed on 12 April 2021).
- Australian Bureau of Statistics. National Health Survey: State and Territory Findings. 2017–2018. Available online: https://www.abs.gov.au/statistics/health/health-conditions-and-risks/national-health-survey-state-and-territory-findings/2017-18 (accessed on 12 April 2021).
- Australian Bureau of Statistics. Family Characteristics and Transitions. 2012–2013. Available online: https://www.abs.gov.au/statistics/people/people-and-communities/family-characteristics-and-transitions/latest-release (accessed on 12 April 2021).
- Australian Institute of Health and Welfare. Mental Health Services. 2020. Available online: https://www.aihw.gov.au/reports-data/health-welfare-services/mental-health-services/data (accessed on 10 July 2021).
- Australian Early Development Census. Data Explorer. 2020. Available online: https://www.aedc.gov.au/data/data-explorer (accessed on 12 October 2020).
- Powell, M.J.D. An efficient method for finding the minimum of a function of several variables without calculating derivatives. Comput. J. 1964, 7, 155–162. [Google Scholar] [CrossRef]
- Williamson, P.; Hope, J.; Segal, J.; Gill, L.; Orr, M.; Trevorah, B.; Garbutt, R.; Hurter, P. A critical review of the first six months of operation of a trial Hospital Outreach Post-suicidal Engagement (HOPE) service in Australia. Australas Psychiatry 2021, 29, 315–321. [Google Scholar] [CrossRef]
- Australian Government. JobTrainer. Available online: https://www.myskills.gov.au/jobtrainer (accessed on 5 May 2022).
- Charles-Edwards, E.; Wilson, T.; Bernard, A.; Wohland, P. How will COVID-19 impact Australia’s future population? A scenario approach. Appl. Geogr. 2021, 134, 102506. [Google Scholar] [CrossRef]
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 15 April 2021).
- Skinner, A.; Occhipinti, J.; Rosenberg, S.; Song, Y.J.C.; Hickie, I.B. Measuring the Scale of Underinvestment in Australia’s Mental Health Services System: A Dynamic Modelling Analysis. 2021. Available online: https://www.sydney.edu.au/content/dam/corporate/documents/brain-and-mind-centre/youth-mental-health/needs-based-services-modelling-results-may-2021.pdf (accessed on 10 February 2021).
- Varker, T.; Brand, R.M.; Ward, J.; Terhaag, S.; Phelps, A. Efficacy of synchronous telepsychology interventions for people with anxiety, depression, posttraumatic stress disorder, and adjustment disorder: A rapid evidence assessment. Psychol. Serv. 2019, 16, 621–635. [Google Scholar] [CrossRef] [PubMed]
- Fifth National Mental Health and Suicide Prevention Plan. 2017. Available online: https://www.mentalhealthcommission.gov.au/monitoring-and-reporting/fifth-plan/5th-national-mental-health-and-suicide-prevention (accessed on 15 February 2022).
- Campaign Launched by Victorian Government: ‘It’s Time to Talk about Mental Health’ 2021. Available online: https://www.mhrv.vic.gov.au/news/campaign-encourages-victorians-talk-about-mental-health (accessed on 15 February 2022).
- Coronavirus (COVID-19) Mental Health Campaign Resources. 2021. Available online: https://www.health.gov.au/resources/collections/coronavirus-covid-19-mental-health-campaign-resources (accessed on 15 February 2022).
- Dumesnil, H.; Verger, P. Public awareness campaigns about depression and suicide: A review. Psychiatr. Serv. 2009, 60, 1203–1213. [Google Scholar] [CrossRef] [PubMed]
- International Monetary Fund: G-20 Surveillance Note. 2022. Available online: https://www.imf.org/external/np/g20/021622.htm (accessed on 20 February 2022).
- OECD Economic Outlook, Interim Report March 2022: Economic and Social Impacts and Policy Implications of the War in Ukraine. 2022. Available online: https://read.oecd.org/10.1787/4181d61b-en (accessed on 20 March 2022).
- Reserve Bank of Australia: Statement by Philip Lowe, Governor: Monetary Policy Decision. 2022. Available online: https://www.rba.gov.au/media-releases/2022/mr-22-02.html (accessed on 10 February 2022).
- Achdut, N.; Refaeli, T. Unemployment and Psychological Distress among Young People during the COVID-19 Pandemic: Psychological Resources and Risk Factors. Int. J. Environ. Res. Public Health 2020, 17, 7163. [Google Scholar] [CrossRef] [PubMed]
- Graetz, B. Health consequences of employment and unemployment: Longitudinal evidence for young men and women. Soc. Sci. Med. 1993, 36, 715–724. [Google Scholar] [CrossRef]
- Rodwell, L.; Romaniuk, H.; Nilsen, W.; Carlin, J.B.; Lee, K.J.; Patton, G.C. Adolescent mental health and behavioural predictors of being NEET: A prospective study of young adults not in employment, education, or training. Psychol. Med. 2018, 48, 861–871. [Google Scholar] [CrossRef]
- Mirowsky, J.; Ross, C.E. Education, Social Status, and Health. Am. J. Sociol. 2003, 110. [Google Scholar] [CrossRef]
- Seidler, Z.E.; Rice, S.M.; Dhillon, H.M.; Cotton, S.M.; Telford, N.R.; McEachran, J.; Rickwood, D.J. Patterns of Youth Mental Health Service Use and Discontinuation: Population Data From Australia’s Headspace Model of Care. Psychiatr. Serv. 2020, 71, 1104–1113. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Business Indicators, Business Impacts of COVID-19. April 2020. Available online: https://www.abs.gov.au/statistics/economy/business-indicators/business-conditions-and-sentiments/apr-2020 (accessed on 30 May 2020).
- Badamgarav, E.; Weingarten, S.R.; Henning, J.M.; Knight, K.; Hasselblad, V.; Gano, A.; Ofman, J.J., Jr. Effectiveness of disease management programs in depression: A systematic review. Am. J. Psychiatry 2003, 160, 2080–2090. [Google Scholar] [CrossRef]
- Carroll, R.; Metcalfe, C.; Gunnell, D. Hospital presenting self-harm and risk of fatal and non-fatal repetition: Systematic review and meta-analysis. PLoS ONE 2014, 9, e89944. [Google Scholar] [CrossRef]
- Hvid, M.; Vangborg, K.; Sorensen, H.J.; Nielsen, I.K.; Stenborg, J.M.; Wang, A.G. Preventing repetition of attempted suicide—II. The Amager project, a randomized controlled trial. Nord. J. Psychiatry 2011, 65, 292–298. [Google Scholar] [CrossRef]
- Jorm, A.F.; Griffiths, K.M.; Christensen, H.; Korten, A.E.; Parslow, R.A.; Rodgers, B. Providing information about the effectiveness of treatment options to depressed people in the community: A randomized controlled trial of effects on mental health literacy, help-seeking and symptoms. Psychol. Med. 2003, 33, 1071–1079. [Google Scholar] [CrossRef]
- Woltmann, E.; Grogan-Kaylor, A.; Perron, B.; Georges, H.; Kilbourne, A.M.; Bauer, M.S. Comparative effectiveness of collaborative chronic care models for mental health conditions across primary, specialty, and behavioral health care settings: Systematic review and meta-analysis. Am. J. Psychiatry 2012, 169, 790–804. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Intervention | Description |
|---|---|
| a. Awareness programs | Population-wide mental health awareness programs aimed at reducing stigma, improving the recognition of suicide risk, and encouraging help-seeking. Default duration: 5 years. |
| b. Education programs | Programs providing financial support to post-secondary students (age 15 to 24) who have become unemployed due to the COVID-19 pandemic, enabling them to continue studying. Default duration: 5 years. |
| c. Job creation program | Programs designed to increase the per capita rate of employment initiation. Default duration: 2 years. |
| d. Post-suicide attempt care | An active outreach and contact program that aims to reduce re-admission in those presenting to services after a suicide attempt. It includes individually tailored contact, solution focused counselling, and actions to ensure adherence to follow-up treatments and continuity of contact. Default duration: till end of simulation. |
| e. Services capacity growth | GP mental health services, psychiatrist and allied services, and community mental health: multiplies (by 2 by default) the annual rate of increase in the total number of consultations that can be completed per week. Default duration: till end of simulation. |
| f. Technology-enabled, measurement-based care | Online technology to facilitate the delivery of a multidisciplinary team-based care, where medical and allied health professionals consider all treatment options, collaboratively develop an individual care plan for each patient, and measure outcomes. Default duration: till end of simulation. |
| No COVID-19 | COVID-19 Baseline | Change | % Change | |
|---|---|---|---|---|
| Victoria (all ages) | ||||
| Suicide deaths | 4361 | 4578 | 217 | 4.98% |
| Intentional self-harm hospitalisations | 35,468 | 37,528 | 2060 | 5.81% |
| Mental-health-related ED presentations | 358,580 | 365,060 | 6480 | 1.81% |
| Population aged 15–24 years | ||||
| Suicide deaths | 559 | 602 | 43 | 7.69% |
| Intentional self-harm hospitalisations | 10,782 | 11,611 | 829 | 7.69% |
| Mental-health-related ED presentations | 75,226 | 77,012 | 1786 | 2.37% |
| Major cities areas of Victoria | ||||
| Suicide deaths | 3070 | 3231 | 161 | 5.24% |
| Intentional self-harm hospitalisations | 24,878 | 26,406 | 1528 | 6.14% |
| Mental-health-related ED presentations | 246,643 | 251,965 | 5322 | 2.16% |
| Regional and remote areas of Victoria | ||||
| Suicide deaths | 1290 | 1347 | 57 | 4.42% |
| Intentional self-harm hospitalisations | 10,590 | 11,123 | 533 | 5.03% |
| Mental-health-related ED presentations | 111,937 | 113,096 | 1159 | 1.04% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vacher, C.; Ho, N.; Skinner, A.; Robinson, J.; Freebairn, L.; Lee, G.Y.; Iorfino, F.; Prodan, A.; Song, Y.J.C.; Occhipinti, J.-A.; et al. Optimizing Strategies for Improving Mental Health in Victoria, Australia during the COVID-19 Era: A System Dynamics Modelling Study. Int. J. Environ. Res. Public Health 2022, 19, 6470. https://doi.org/10.3390/ijerph19116470
Vacher C, Ho N, Skinner A, Robinson J, Freebairn L, Lee GY, Iorfino F, Prodan A, Song YJC, Occhipinti J-A, et al. Optimizing Strategies for Improving Mental Health in Victoria, Australia during the COVID-19 Era: A System Dynamics Modelling Study. International Journal of Environmental Research and Public Health. 2022; 19(11):6470. https://doi.org/10.3390/ijerph19116470
Chicago/Turabian StyleVacher, Catherine, Nicholas Ho, Adam Skinner, Jo Robinson, Louise Freebairn, Grace Yeeun Lee, Frank Iorfino, Ante Prodan, Yun Ju C. Song, Jo-An Occhipinti, and et al. 2022. "Optimizing Strategies for Improving Mental Health in Victoria, Australia during the COVID-19 Era: A System Dynamics Modelling Study" International Journal of Environmental Research and Public Health 19, no. 11: 6470. https://doi.org/10.3390/ijerph19116470