
COVID-19-Current Therapeutical Approaches and Future Perspectives
by
 , , , and
, , , and
Raluca Elisabeta Lupașcu (Moisi)
1 ,
,
Marina Ionela Ilie
1,
Bruno Ștefan Velescu
2, 
Denisa Ioana Udeanu
3,
Camelia Sultana
4,5,
Simona Ruță
4,5,* and
Andreea Letiția Arsene
1 1
Department of General and Pharmaceutical Microbiology, Faculty of Pharmacy, “Carol Davila” University of Medicine and Pharmacy, 6 Traian Vuia Street, 020956 Bucharest, Romania
2
Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, “Carol Davila” University of Medicine and Pharmacy, 6 Traian Vuia Street, 020956 Bucharest, Romania
3
Department of Clinical Laboratory and Food Safety, Faculty of Pharmacy, “Carol Davila” University of Medicine and Pharmacy, 6 Traian Vuia Street, 020956 Bucharest, Romania
4
Department of Virology, Faculty of Medicine, “Carol Davila” University of Medicine and Pharmacy, 050474 Bucharest, Romania
5
Stefan S. Nicolau Institute of Virology, 285 sos Mihai Bravu, 030304 Bucharest, Romania
*
Author to whom correspondence should be addressed.
Processes 2022, 10(6), 1053; https://doi.org/10.3390/pr10061053
Submission received: 4 May 2022
/
Revised: 23 May 2022
/
Accepted: 24 May 2022
/
Published: 25 May 2022
(This article belongs to the Special Issue Pharmaceutical Development and Bioavailability Analysis)
Abstract
:The ongoing pandemic of coronavirus disease (COVID-19) stimulated an unprecedented international collaborative effort for rapid diagnosis, epidemiologic surveillance, clinical management, prevention, and treatment. This review focuses on the current and new therapeutical approaches, summarizing the viral structure and life cycle, with an emphasis on the specific steps that can be interfered by antivirals: (a) inhibition of viral entry with anti-spike monoclonal antibodies; (b) inhibition of the RNA genome replication with nucleosidic analogs blocking the viral RNA polymerase; (c) inhibition of the main viral protease (Mpro), which directs the formation of the nonstructural proteins. An overview of the immunomodulatory drugs currently used for severe COVID-19 treatment and future therapeutical options are also discussed.
Keywords:
COVID-19; treatment; future therapy; antiviral drugs; antibodies; immunomodulators; nanobodies; interferons1. Introduction
SARS-CoV-2, an emerging zoonotic coronavirus, identified in December 2019 in Wuhan, Hubei province, China, has spread rapidly across the whole world, causing disproportionately high morbidity and mortality, along with unprecedented disruptions in the global economy and society functioning. This is the third highly pathogenic respiratory coronavirus that emerged during the last two decades, after SARS-CoV (Severe Acute Respiratory Syndrome coronavirus), which caused an important outbreak between 2002–2004, and MERS-CoV (Middle-East respiratory syndrome coronavirus), identified in 2012 and still causing sporadic infections in the Middle East [1]. Although associated with a lower fatality rate than its preceding relatives, SARS-CoV-2 caused more than 481 million infections, and more than 6.1 million deaths [2], due to its high contagiousness and ability to be transmitted during asymptomatic and pre-symptomatic infections. Exceptional measures were taken to slow down the spread of this respiratory pathogen, including lockdowns, restrictions on travel and gatherings, mask mandates, and closures of businesses and schools, all actions with a high economic and psychological burden.
A plethora of vaccines was designed, based on the rapidly advancing knowledge of the viral genome sequence and previous studies on the structure of the related highly pathogenic coronaviruses, SARS-CoV and MERS-CoV. Presently, worldwide, more than 4.5 billion persons (>57.6% of the total population) are fully vaccinated and have an important degree of protection against severe forms of the disease [2]. Nevertheless, both vaccine and infection-induced immunity seem to wane over time. In addition, SARS-CoV-2 has accumulated an important number of mutations during the last two years, a consequence of the natural evolution and adaptation processes common to all RNA viruses, caused by: (a) copying errors made by the viral RNA dependent RNA polymerase during viral genome replication; (b) recombination between different viral lineages that are co-infecting the same host; (c) host RNA-editing systems, part of the natural defense mechanisms [3,4]. Although coronaviruses have a limited intrinsic variability compared to other RNA viruses, due to their large genome and the presence of a proof-reading enzyme (the NSP14 exonuclease), the massive viral replication in a large, immunologic naïve population favored the emergence of several viral variants, with modified biologic properties, designated as variants of concern (VOCs): Alpha; Beta; Gamma; Delta; and Omicron. All of the VOCs have an enhanced binding affinity for the ACE2 receptor compared to the original strain, some of these have additional mutations that allow immune evasion (Beta, Omicron), causing reinfections and infections in vaccinated persons, others have the potential to produce more severe disease (Alpha, Delta) [5,6,7].
Since the beginning of the COVID-19 pandemic, treatment of the SARS-CoV-2 infection was a real challenge. The varying degrees of severity, as well as the uncertainty on the mechanisms underlying disease progression, led to many empirical treatment protocols. Attempts to use convalescent plasma rich in neutralizing antibodies yielded contradictory results [8,9], and several drugs with promising in vitro antiviral activity (hydroxychloroquine, lopinavir/ritonavir, nitazoxanide, oseltamivir, ivermectin) [10,11,12] have failed to demonstrate a significant impact on hospitalization and mortality rates in large clinical trials.
The development of direct antiviral agents was rather slow, surpassed by the race towards effective vaccines, and drug repurposing was the main therapeutical strategy for a long period. Currently, antiviral treatment and prevention approaches are based on a more comprehensive understanding of the pathogeny and detailed knowledge on the structure of viral proteins. The pathogeny of COVID-19 is attributed to an initial phase of intense viral replication, sometimes followed by a dysregulated immune response leading to the second phase of cytokine release storm and immune-mediated tissue damage, that contributes to disease progression, with pulmonary and multi-systemic lesions caused by endothelitis, thrombo-inflammation, and coagulopathy [13].
The main therapeutic strategies are directed toward (a) direct inhibition of the viral entry and replication and (b) immunomodulatory treatment to block the cytokine release storm that underlies COVID-19 severe evolution. Additional interventions are needed to prevent or treat the coagulopathy, lung damage, and respiratory distress syndrome seen in the most severe forms of the disease [14]. The present study is reviewing the currently approved treatments, those under rolling review, and future therapeutic directions.
2. Viral Structure, Life Cycle and Therapeutic Targets
SARS-CoV-2 is an enveloped, positive single-stranded RNA virus, member of the Coronaviridae family (named after the crown-like shape of the spike glycoproteins projections on the envelope). Phylogenetic studies demonstrated that SARS-CoV-2 belongs to genus Betacoronaviridae, subgenus Sarbecovirus, lineage 2B, is highly related to bat coronaviruses, and resembles more closely the SARS-CoV than the MERS-CoV, with genomic similarities of 79% and 50%, respectively [15,16]. The viral life cycle is initiated by SARS-CoV-2 attachment to cellular receptors (angiotensin-converting enzyme 2-ACE2), a series of host factors that promote viral penetration by fusion with the cellular or endosomal membrane. The spike (S) glycoprotein is the major antigenic component of the virus and controls viral entry in susceptible human cells, binding to the ACE2 receptor, found on epithelial cells in the respiratory tract, oral cavity (mouth and tongue), lungs, intestine, kidney, and blood vessels [16,17,18,19].
During cell attachment, the S protein is cleaved into two functional subunits: S1, which includes the receptor-binding domain (RBD); and S2, essential for membrane fusion. Activation of viral infectivity is mediated by cellular proteases: TMPRSS2 (type II transmembrane serine protease), furin (highly expressed in the lungs), and furin-like proteases, which recognize an additional polybasic PRRAR site at the S1/S2 cleavage site-specific to SARS-CoV2, thought to have played an important role in the human adaptation of the virus. Structural rearrangements of the S protein trimer are essential for the transition from a closed to an open shape of the RBD, allowing efficient cell binding and the switch from a prefusion to a post-fusion conformation [20].
Following the fusion of the virus envelope and host cell membrane, mediated by the S2 subunit containing the fusion peptide, the RNA genome is released into the cytoplasm of the host cell. The positive-sense single-stranded RNA genome is directly translated into two large polypeptides—pp1a and pp1ab—further cleaved by two important viral cysteine proteases (papain-like protease-Plpro, and the chymotrypsin-like protease-3Clpro/main protease-Mpro) to form 16 nonstructural proteins, many of which will participate in the replicase–transcriptase complex (RTC). This includes the RNA-dependent RNA polymerase (RdRP), which conducts the synthesis of the new RNA genome, together with viral and host co-factors, and the Nsp14 exonuclease, with RNA proofreading activity, that limits viral variability. A set of sub-genomic RNA (sgRNA) species are formed during the genome replication from the negative-sense RNA intermediate and serve for translation of the structural and accessory proteins [21]. Double-membrane vesicles, convoluted membranes, and open double-membrane spherules produce a protective microenvironment for viral RNA replication and transcription of sgRNA. Translated structural proteins are translocated into the endoplasmic reticulum (ER) and travel through the ER-to-Golgi intermediate compartment (ERGIC), assemble with the genomic RNA, and the progeny virions are released from the infected cells. Several steps in the viral life cycle represent important therapeutic targets: (a) viral entry interfered with anti-spike monoclonal antibodies; (b) the RNA genome replication, prematurely stopped by nucleoside analogs binding to the viral RNA polymerase; (c) synthesis of the nonstructural proteins by inhibitors of the main viral protease (Mpro).
3. Drugs Currently Used for COVID-19 Therapy
Currently, only symptomatic treatment is used for mild forms of COVID-19, while for mild to severe forms several drugs, which have proven effective both in vitro and in vivo, are recommended [16]. The therapeutic agents can be divided according to their mechanism of action and their use in inpatient or outpatient treatment (Table 1).
3.1. Entry Inhibitors and Direct-Acting Antiviral Drugs
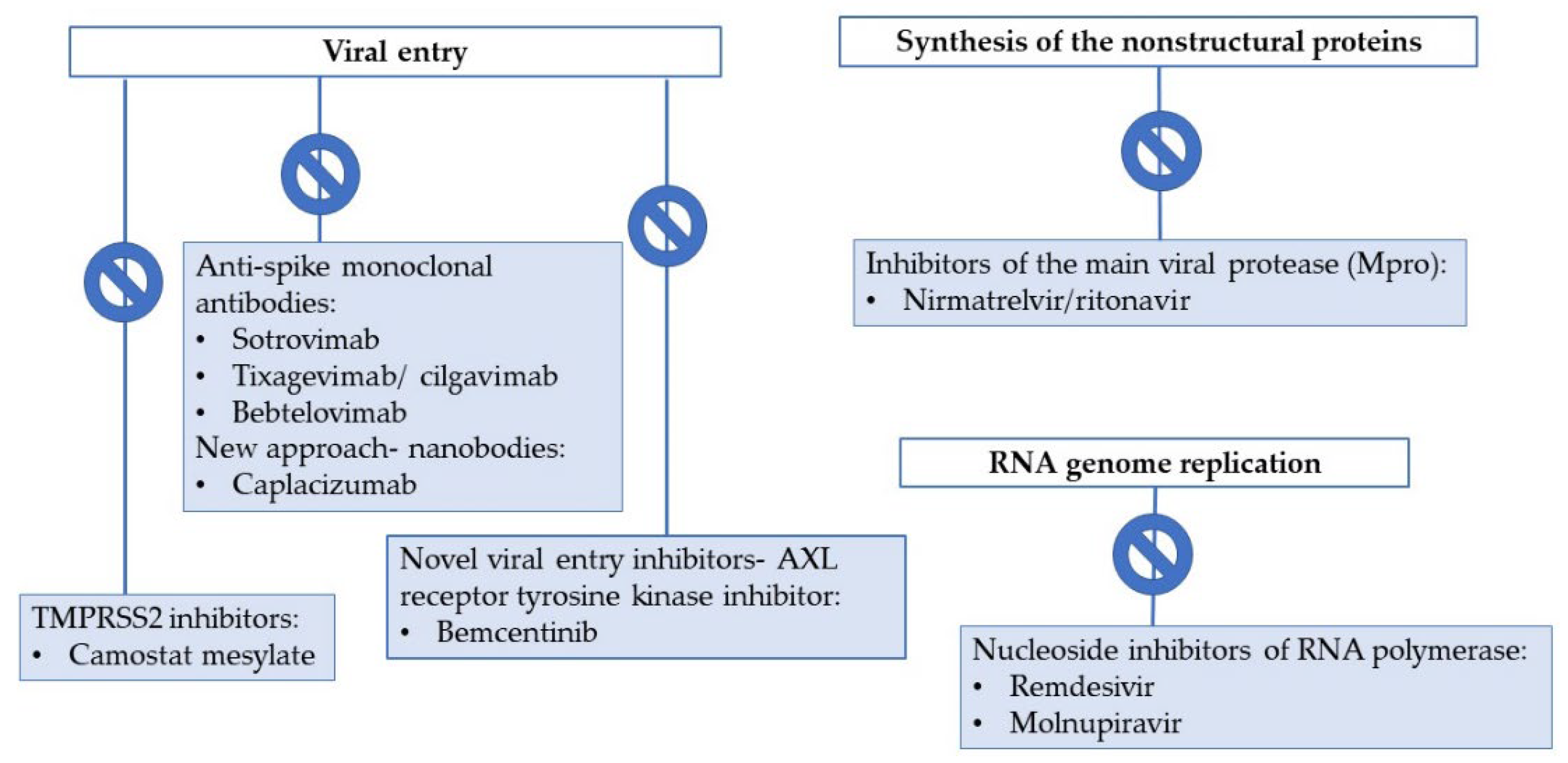
Entry inhibitors and direct-acting antiviral drugs are active during the early replicative phase, as such, they must be administered during a short therapeutic window of 3–5 days after infection, and only in patients who have significant risk factors for a severe evolution of COVID-19. Rapid testing must be available to ensure a fast diagnosis and a “test to treat” system must be implemented and maintained in the medium/long term, even during periods of low viral circulation. In immunosuppressed patients (recipients of solid organ or bone marrow transplants, those with hematologic malignancies, or who are severely B-cell depleted, HIV infected patients, etc.), SARS-CoV-2 replication may persist for weeks or months, with prolonged viral shedding and potential high variability. Early treatment of these patients with potent antiviral drugs is essential to decrease morbidity and mortality, and to prevent further selection of viral variants. Combinations of antivirals may prove beneficial, but their use requires further investigation [22,23] (Figure 1).
3.1.1. Entry Inhibitors: Anti-Spike Monoclonal Antibodies
Anti-SARS-CoV-2 monoclonal antibodies (Mab) recognize specific epitopes on the viral spike protein, blocking receptor binding and membrane fusion. Neutralizing Mab can be isolated from convalescent patients’ memory B cells, using single-cell clonal amplification or by high-throughput single-cell RNA and VDJ sequencing of antigen-binding B cells [24].
Combinations of anti-SARS-CoV-2 Mab, binding to different regions of the spike glycoprotein, can efficiently inhibit viral replication, if administered during the first 7 days after infection, leading to a lower incidence of COVID-19-related hospitalizations and deaths. Adverse reactions are rare and usually mild. Safety in pregnancy and lactation is currently unknown, therefore administration to pregnant and breastfeeding women is not recommended. However, as the anti-spike Mabs act directly on the SARS-CoV-2 specific spike protein, and given the absence of cross-reactivity with tissues involved in reproductive or fetal function, no adverse effects on the developing fetus are anticipated [22]. There are no data on anti-spike Mabs use in patients younger than 12 years [25]. In the COV-2069 study, children aged 12 to 18 years had a similar safety profile to adults. Several Mab combinations, such as casirivimab/imdevimab (REGEN-COV®, Regeneron, Tarrytown, NY, USA) [26] and bamlanivimab/etesevimab (Eli Lilly and Company, Indianapolis, IN, USA) [27] were successfully used in patients with mild to moderate forms of SARS-CoV-2 infection, who were at high risk of progression to severe COVID-19, as well as for post-exposure prevention of COVID-19 disease [26]. Nevertheless, the emergence of viral variants, especially those with high immune evasion capacity, has rendered several combinations of monoclonal antibodies futile; WHO recommends using casirivimab/imdevimab in COVID-19 only when sufficient evidence addressing its activity is available [8].The Omicron variant, which harbors a high number and unusual profile of mutations in the spike glycoprotein, is highly resistant to antibody-mediated neutralization [28], and currently, only three Mabs preserve their efficacy against this variant: Sotrovimab; Bebtelovimab; and the combination Tixagevimab/cilgavimab.
Sotrovimab (Xevudy®, GlaxoSmithKline, Brentford, UK and Vir Biotechnology, Inc, San Francisco, CA, USA) is a recombinant human IgG1 monoclonal antibody that binds to a highly conserved epitope on the receptor-binding domain of the SARS-CoV-2 spike protein, situated outside the receptor-binding motif. It harbors two Fc amino acid substitutions (M428L and N434S) that increase its half-life and its lung bioavailability and allow placental transfer [29]. In vitro studies have shown that sotrovimab preserves a broad neutralizing activity against different SARS-CoV-2 variants and multiple other Sarbecoviruses [30]. The drug is recommended for the treatment of adults and adolescents (aged > 12 years and weighing at least 40 kg) with COVID-19, who do not require supplemental oxygen and who are at increased risk of progression to a severe form of COVID-19 [26]. A phase 3, multicenter, randomized, double-blind placebo-controlled trial—COMET-ICE—reported rapid improvement in the clinical evolution and decreased hospitalization rates for high-risk, non-hospitalized adults with symptomatic COVID-19 treated with sotrovimab early during infection, with no reports of severe adverse events [31].
Tixagevimab/cilgavimab (Evusheld®, AstraZeneca, Cambridge, UK) is a long-acting combination of two new recombinant human anti-SARS-CoV-2 antibodies, with broadly neutralizing activity in vitro (including Delta, Mu, and Omicron variants of SARS-CoV-2). The Mab combination is EMA and FDA approved for the pre-exposure prophylaxis of COVID-19 in adults and adolescents aged 12 years and older, weighing at least 40 kg. The combination is particularly recommended for severe to moderate immunosuppressed patients, with a high risk of severe disease or low post-vaccinal response, reducing the risk of symptomatic disease [32,33,34].
Bebtelovimab (LY-CoV1404, Eli Lilly and Company, Indianapolis, IN, USA) is a recently FDA-approved recombinant monoclonal IgG1κ antibody, with broad neutralizing activity, unaffected by the most common mutations present in all of the known variants of concern of SARS-CoV-2, including the Omicron subvariants BA1/BA2 [35].
3.1.2. Antivirals Targeting the RNA-Dependent RNA Polymerase (RdRp)
Several nucleos(t)ide analogs bind the viral RdRP, which remains to date unaffected by the mutations developed over time in the different SARS-CoV-2 variants, and induce the accumulation of deleterious mutations during genome replication.
Remdesivir (Veklury, Gilead Sciences, Foster City, CA, USA) is a nucleotide analog that competes with intracellular nucleosides for incorporation in the viral RNA and induces premature chain termination. Remdesivir is administered as a prodrug, metabolized intracellularly to an active metabolite, an analog of ATP. Its half-life of about 35 h allows a single dose administration daily. Treatment is recommended for 5–10 days, with a higher initial loading dose (200 mg on the first day), followed by a maintenance daily dose of 100 mg to reach a stable plasma concentration [36,37]
Timing is essential for remdesivir efficacy. Initially recommended for hospitalized patients, remdesivir was proven to be more efficacious during the first 7 days of SARS-CoV-2 infection. In high-risk outpatients (age > 60 years, diabetes, obesity, hypertension), an early, short, 3 days course of remdesivir significantly decreases the rates of hospitalization [38]. Conversely, patients who are already symptomatic for more than 7 days and require oxygen support have no clinical benefit after remdesivir administration, as shown by a large phase 3, adaptive, multicentered European trial—DisCoVeRy [39].
Currently, remdesivir is administered only intravenously, but more accessible administration routes are being evaluated in experimental models, for a more targeted delivery to the respiratory mucosa. Lower doses of remdesivir, administered by nebulization in African green monkeys, have delivered similar concentrations of the active metabolite in the bronchoalveolar fluid and have reduced viral replication in the lower respiratory tract [40]. In mouse models, treatment with an oral prodrug of the remdesivir parental nucleoside (GS-621763) reduced viral load, improved pulmonary function, and had similar efficacy with an already approved oral antiviral—molnupiravir [41].
Remdesivir is EMA and FDA approved for the treatment of both hospitalized patients (with COVID-19 pneumonia, requiring supplemental oxygen) and non-hospitalized ones (with mild to moderate forms of COVID-19, but at high risk for severe disease), aged ≥ 12 years and weighing ≥ 40 kg. The initial data on remdesivir efficacy came from the WHO SOLIDARITY study, that combined data from four clinical trials, showing a decrease in symptoms’ severity in patients treated with remdesivir, and a significant increase in life expectancy in critically ill patients [22,26].
Among the side effects of remdesivir observed during clinical trials, and further reported during clinical use on the FDA or EMA websites, are gastrointestinal reactions (constipation, nausea, vomiting, diarrhea), increased prothrombin time, hypersensitivity reactions, hepato-, and renal toxicity [42]. Therefore, monitoring of liver and kidney functions is recommended before and during remdesivir administration. Remdesivir is not administered if the glomerular filtration rate is less than 30 mL per minute, due to the presence of an excipient (sulfobutyl ether beta-cyclodextrin sodium) that accumulates in the kidney, causing renal toxicity [22]. Remdesivir is not approved for the treatment of COVID-19 in pregnant women, but it was used off-label on a small number of patients, with good efficacy and minimal side effects [26]. A large study on the safety of remdesivir administration in pregnant and breastfeeding women, conducted by the National Institute of Allergy and Infectious Diseases, US, is expected to be completed in 2022 [43]. Treatment with remdesivir was available through an emergency authorization for patients younger than 12 years, due to insufficient data on the pharmacokinetics and safety of the drug in these patients. The evidence for remdesivir use in children is limited. A study done in early 2021 on 77 children (under 18 years old, with an average age of 14 years) with severe forms of COVID-19, showed improvement in the symptomatology, with good tolerance and few side effects [23,44]. In April 2022 FDA has approved remdesivir use in pediatric patients 28 days of age and older weighing at least 3 kg, based on the efficacy results in adults and on the data from a phase 2/3, single-arm, open-label clinical study of 53 pediatric patients [45].
Molnupiravir (MK-4482-002, Merck Sharp Dome/Ridgeback Biotherapeutics), is a prodrug of N4-hydroxycytidine (NHC), a nucleoside analog, converted intracellularly to the pharmacologically active form: β-D-N4-hydroxycytidine (NHC), a ribonucleoside that acts as a substrate for the viral RNA-dependent RNA-polymerase, increasing the error rate during viral replication and inducing a process of lethal mutagenesis [46]. Molnupiravir is an orally administered drug, with a broad-range of antiviral activity on many RNA viruses (including the highly pathogenic coronaviruses SARS-, MERS-, SARS-CoV-2, and the seasonal and pandemic influenza viruses).
Molnupiravir has received an Emergency Use Authorization from the FDA [23], but, as of March 2022, is still under rolling review by the EMA. It is, however, used prior to marketing authorization in several European countries, for the treatment of mild to moderate forms of COVID-19 in unvaccinated adults (≥18 years) at serious risk for severe progression, especially when there is no other therapeutic alternative, during an emergency with an increased number of cases and deaths related to SARS-CoV-2 infection.
The efficacy and safety of molnupiravir, administered during the first 5 days after symptoms onset in non-hospitalized patients, were demonstrated in phase 3, a randomized, double-blind, placebo-controlled trial—MOVe-OUT. The most common side effects observed during the study were diarrhea and bacterial pneumonia, followed by nausea and dizziness [47]. Nevertheless, further studies signaled a rather limited clinical benefit, with only a 30% reduction in the hospitalization risk. Concerns related to a potential mutagenetic risk, raised during preclinical studies and not confirmed until now in humans, preclude molnupiravir use in pediatric patients and during pregnancy. A laboratory animal study showed impaired spermatogenesis and an increased risk of embryo-fetal toxicity in pregnancy, as such, consistent use of contraception methods is recommended for the duration of treatment and 4 days after the last dose of molnupiravir, and breastfeeding is prohibited [42].
Favipiravir (Avigan®-Fujifilm, Tokyo, Japan) is a nucleoside analog, with a wide spectrum of antiviral activity in vitro, mediated by RNA polymerase inhibition. The drug was approved in 2014 in Japan for the treatment of influenza virus infections and was repurposed for use in mild/medium forms of SARS-CoV-2 infections in patients with risk factors for progression. Several systematic reviews and meta-analyses on the efficacy of favipiravir in COVID-19 patients yielded contradictory results, with possible significant improvement in symptomatology and a more rapid viral clearance [48], but without differences in the mortality rate or requirement for mechanical ventilation compared to standard of care [49]. In terms of safety, gastrointestinal adverse reactions (diarrhea, vomiting), abnormal liver function (high transaminases), low albumin levels, and high blood uric acid levels were mainly reported during the studies [48].
3.1.3. Protease Inhibitors
Nirmatrelvir/Ritonavir (Paxlovid, Pfizer, Brooklyn, NY, USA) is an orally administered combination, approved by the EMA and FDA for use in patients older than 12 years and weighing more than 40 kg, with mild/medium forms of COVID-19, who have at least one risk factor for severe disease progression [50]. Nirmatrelvir is a potent protease inhibitor, with pan-human coronavirus antiviral activity in vitro, that selectively blocks the main SARS-CoV-2 protease (Mpro or 3CLpro), via a reversible covalent mechanism, inhibiting the polyprotein cleavage and formation of nonstructural proteins, essential for viral replication [51,52].
Nirmatrelvir is administered in combination with ritonavir, a potent inhibitor of cytochrome P450 CYP 3A4, that acts as a pharmacokinetic enhancer, increasing its plasmatic concentration. Ritonavir was previously used in active antiretroviral combinations, as a pharmacologic booster for HIV protease inhibitors. Nirmatrelvir/Ritonavir treatment administered during the first 3 days of symptomatic SARS-CoV infection induced a significant decrease in the hospitalization rate in a Phase 2/3, randomized, double-blind, placebo-controlled study—EPIC-HR [53]. The combination is safe and well-tolerated, however, due to multiple potential drug-to-drug interactions, especially with drugs that are potent CYP3A inducers or that are dependent on CYP3A for clearance, a careful individual assessment and monitoring are required before treatment initiation [26]. As a CYP3A4 inhibitor, ritonavir increases the serum concentration of drugs that are metabolized by this enzyme, so that associations with such drugs are not recommended, due to a potential increase in adverse reactions. A comprehensive, updated, free resource for drug interactions, with recommendations for dose adjustments, treatment interruptions, or replacements is available online at https://www.covid19-druginteractions.org/ (accessed on 15 March 2022).
The most common side effects observed in clinical trials with Nirmatrelvir/Ritonavir are dysgeusia, diarrhea, hypertension, and myalgia [50].
No teratogenic, embryo, or fetal toxicity in females and no impairment of fertility in males were observed during preclinical studies in rats [54], but, due to limited data, the combination is not recommended during pregnancy or breastfeeding [55,56]. Several in vitro and in vivo animal model studies showed that the circulating SARS-CoV-2 VOCs preserve susceptibility to nirmatrelvir treatment [57,58].
3.2. Immunomodulators
The hyperinflammatory syndrome induced by SARS-CoV-2, derived from a dysregulated host innate immune response, contributes to the severity and mortality in COVID-19, as such, immunomodulatory drugs are recommended for hospitalized patients with severe evolution. Immunomodulatory therapy decreases the inflammation and modulates the immune response, interfering with various pathogenic mechanisms and pathways.
3.2.1. Corticosteroids
Corticosteroids decrease the COVID-19-induced systemic inflammatory response, leading to an improvement in the clinical outcomes and a reduction in the 28-day mortality (8.7% in the critically ill and 6.7% in patients with severe COVID-19 who were not critically ill). Dexamethasone is the first-choice corticosteroid, widely used throughout the pandemic, with similar oral and intravenous bioavailability.
Corticosteroids are highly effective in hospitalized patients in severe or critical conditions, requiring mechanical ventilation, while in those with mild forms of the diseases, their use is not recommended [8]. Low-dose dexamethasone used in pregnant women requiring mechanical ventilation resulted in a decrease in COVID-19-induced complications, with a low risk of fatal adverse reactions. The international treatment guidelines do not recommend the use of corticosteroids in pediatric patients, as there are insufficient data to confirm extrapolation of corticosteroid doses used in adults for patients younger than 18 years [26].
Inhaled administration of corticosteroids might be recommended in COVID-19 patients, due to an anti-inflammatory effect in the respiratory tract, that can decrease the innate immune inflammatory responses and the macrophages’ infiltration in the lung tissue. In addition, inhaled corticosteroids can interfere with the replication of SARS-CoV-2, by downregulating ACE2 receptor expression, especially in patients with chronic obstructive pulmonary disease [22,59]. Nevertheless, the COVID-19 EMA pandemic Task Force is advising that there is insufficient evidence on the benefits of inhaled corticosteroids for people with COVID-19 with normal levels of oxygen [60].
The general safety profile of corticosteroids is well known, and the main side effects (including hyperglycemia, fluid retention, increased risk of opportunistic infections, and reactivations of latent infections) are manageable.
3.2.2. IL-6 Receptor Inhibitors
Interleukin 6 (IL-6) is a pro-inflammatory cytokine with pleiotropic functions in multiple processes, from hematopoiesis and metabolic regulation to inflammation, autoimmunity, and acute phase response. Increased IL-6 levels were demonstrated during the cytokine release storm underlying severe COVID-19. Two classes of IL-6 antagonists are currently evaluated by the FDA for the treatment of COVID-19: monoclonal antibodies against the IL-6 receptor (tocilizumab, sarilumab), and monoclonal antibodies anti-IL-6 (siltuximab) [26].
The REMAP-CAP study showed the efficacy of tocilizumab and sarilumab administered in combination with dexamethasone, with improvement in survival rates and reduced need for oxygen delivery in severely ill patients, compared to other treatments [61]. The current guidelines recommend the use of tocilizumab only in combination with corticosteroids, w/wo remdesivir, in hospitalized patients requiring supplemental oxygen. Due to more limited data, sarilumab is recommended only if tocilizumab is not available, for patients in need of mechanical ventilation/ECMO [62].
Tocilizumab (Actemra®, Roche, Basel, Switzerland) (alone or in combination with methotrexate) is recommended for rheumatoid arthritis. In 2021, it was approved by the EMA and FDA for the treatment of COVID-19 disease in both adults and pediatric patients (>2 years of age) on systemic corticosteroids who require supplemental oxygen or mechanical ventilation [63]. Monotherapy with tocilizumab does not improve the evolution in severe COVID-19 cases [64]. There are insufficient data to assess the passage of tocilizumab or sarilumab across the placenta or into breast milk, so treatment of pregnant or breastfeeding women is not recommended; the efficacy in pediatric patients was not yet demonstrated, although the drug is useful in juvenile polyarthritis [26,65].
Treatment with tocilizumab increases the liver enzymes levels in a dose-dependent manner. Neutropenia with severe infections, such as tuberculosis, other bacterial or fungal infections, and thrombocytopenia, were reported as tocilizumab-specific adverse reactions. Cases of bowel perforation were also reported [26].
Siltuximab (Sylvant®, Janssen Pharmaceuticals, Inc., Belser, Belgium) is a recombinant chimeric human-mouse monoclonal antibody that binds to IL-6, used in patients with Castleman’s disease. Currently, its use in COVID-19 is not recommended outside clinical trials, but pharmacological data support its potential benefits. A retrospective study conducted in Barcelona demonstrated that siltuximab is a well-tolerated alternative to tocilizumab in high-risk patients with SARS-CoV-2-associated pneumonia and high levels of C-reactive protein [66], its main adverse reaction is skin rash [26].
3.2.3. Interleukin-1 Inhibitors
The severity of COVID-19 positively correlates with the levels of inflammatory cytokines, including IL-1, a pro-inflammatory factor, overexpressed in severe COVID-19 cases requiring intensive care and mechanical ventilation. Drugs that block the IL-1 receptor (anakinra) or drugs that block IL-1 signaling (canakinumab) are used to reduce the inflammation and hyperactivation of the immune responses associated with systemic IL-1 release [26].
Anakinra (Kineret®, Swedish Orphan Biovitrum, Stockholm, Sweden (Sobi)/Savient Pharmaceuticals, East Brunswick, NJ, USA) is an IL-1 receptor antagonist, produced by recombinant DNA technology, and approved for the treatment and prophylaxis of rheumatoid arthritis. Anakinra was approved by the EMA at the end of 2021 for the treatment of severe COVID-19 [67], following positive results in placebo-controlled clinical trials, showing attenuation of the hyper-inflammatory syndrome and a reduction in the number of patients who experience progression to severe respiratory failure or death [68]. No major safety concerns were raised during anakinra use for the treatment of COVID-19. Reported side effects included neutropenia (particularly when given concomitantly with other drugs that decrease the number of leukocytes), headache, diarrhea, and flu-like symptoms [26]. Data on pregnancy and breastfeeding are limited, and the efficacy in children under 18 years of age is not yet established [67].
Canakinumab (Ilaris®, Novartis Pharmaceuticals Corp, Basel, Switzerland) is an anti-IL-1 human monoclonal antibody used in the treatment of systemic juvenile idiopathic arthritis and Still’s disease. Due to limited available data on the use of this drug in COVID-19 patients, the treatment guidelines recommend its use only in controlled clinical trials [69]. Studies on adult patients hospitalized with COVID-19 pneumonia have shown that in those with medium forms, canakinumab administration resulted in a rapid and long-lasting improvement in oxygenation levels, without severe adverse events [70], while in those with severe forms of the disease (pneumonia, hypoxia, and systemic hyper-inflammation) there was no benefit in terms of survival without mechanical ventilation [71]. However, more data are needed to determine the optimal time for the effect of canakinumab administration and its potential benefit for COVID-19 patients with respiratory failure. No serious or increased-frequency adverse reactions were reported in patients given canakinumab [26].
3.2.4. Janus Kinase Inhibitors
Janus kinase (JAK) inhibitors interfere with one of the critical cellular pathways involved in the inflammatory response: the JAK/STAT signaling pathway, blocking phosphorylation of STAT proteins (signal transducer and activator of transcription) and preventing inflammation and immune activation [8]. JAK inhibitors can be used as supplemental therapy in hospitalized patients receiving remdesivir and/or dexamethasone, who have signs of systemic inflammation and require rapid oxygen supplementation.
Baricitinib (Olumiant®, Eli Lilly and Company, Indianapolis, IN, USA), a clinically approved drug for rheumatoid arthritis, is a selective JAK1/JAK2 inhibitor with potent anti-inflammatory activity and a potential direct antiviral effect, by inhibition of the pivotal regulators of the ACE2 receptor that mediate the clathrin-dependent viral endocytosis [72]. Three clinical trials (ACTT-2, COV-BARRIER, STOP-COVID) evaluated the efficacy of baricitinib for COVID-19 treatment, with positive results, demonstrating a decrease in hospitalization lengths, duration of mechanical ventilation, and mortality [26]. Baricitinib was administered in monotherapy or in combination with other immunomodulatory and antiviral drugs. Co-administration of baricitinib and remdesivir improved the clinical outcome, compared to remdesivir alone, with a lower frequency of adverse effects [73]. Co-administration of baricitinib and corticosteroids was associated with a significant decrease in the short and medium-term all-cause mortality, with a safety profile similar to the standard of care [74]. No serious adverse reactions were reported and the drug can also be administered to children over 2 years of age [75].
Ruxolitinib (Jakafi®, Incyte Corp, Wilmington, DE, USA/Novartis, Basel, Switzerland), a selective JAK1/JAK2 inhibitor, and Tofacitinib (Xeljanz® Pfizer, Brooklyn, NY, USA), a JAK1/JAK3 inhibitor, are recommended in combination with corticosteroids, only if baricitinib or IL-6 inhibitors cannot be used. Currently, a beneficial effect on the clinical outcomes was not fully demonstrated, therefore their use in COVID-19 treatment remains limited [8].
3.2.5. Other Potential Immunomodulatory Drugs
Fluvoxamine, a selective serotonin reuptake inhibitor, and a sigma-1 receptor agonist, involved in the regulation of mitochondrial activity, was tested in COVID-19 patients for its anti-inflammatory and anti-hypoxic capacity. Several clinical trials suggested that an early administration of fluvoxamine in high-risk outpatients has potential benefits, reducing the need for hospitalization and improving the clinical outcomes, but without effect on mortality rates [76,77].
4. New Therapeutical Approaches for COVID-19
4.1. Broadly Neutralizing Antibodies
Broadly neutralizing antibodies, active against different variants of SARS-CoV-2, including Omicron, were isolated from convalescent plasma donors or vaccinated individuals [78]. Cryo-EM studies showed antibodies that were cross-reactive between sarbeco-, merbeco- and embecoviruses, and have flexible binding modes, targeting both the “up” and “down” conformations of the RBD [79]. The development of such ultrapotent antibodies directed towards conserved viral epitopes, with broad-spectrum activity against both wild-type and mutant virus strains, is an important strategy for COVID treatment [80,81] and a step forward towards a pan-coronavirus vaccine. In addition, innovative antibody delivery techniques, such as inhaled antibodies, might offer a convenient, highly accessible method for COVID-19 prevention.
Nanobodies (Nbs) are single-domain antibodies, similar to the heavy-chain-only antibodies initially isolated from camelids and cartilaginous fish [82]. Nbs have a truncated structure, without any light chains and with a single variable domain in the two heavy chains (VHH), representing the antigen-binding region. Nbs exhibit ideal attributes for large-scale manufacture and have numerous advantages over classical human antibodies: ultra-high antigen-binding affinity, due to a very long CDR3, that can access otherwise inaccessible epitopes; recognition of a higher diversity of paratopes; good physicochemical qualities with increased solubility; good tissue penetration; and high stability, allowing for oral or inhalation administration. Bi- or multi-specific heavy chain antibodies and nanobody-drug conjugates are tested as antitumoral therapeutic strategies and can be used to prevent or treat inflammatory and infectious diseases [83].
Caplacizumab, a bivalent single-domain antibody, is the first nanobody-based medicine approved by the EMA and FDA in adults with thrombotic thrombocytopenic purpura and thrombosis in November 2018, and February 2019, respectively [84]. Due to their high antigen affinity and stability, nanobodies can be administered in oral or inhaled versions and might be beneficial for COVID-19 non-hospitalized patients, during the early stages of the disease, acquiring high pulmonary concentrations with minimal systemic adverse effects [85,86].
Nanobodies able to recognize the RBD of different variants of SARS-CoV-2 were identified using phage display libraries derived from camels and llamas immunized with SARS-CoV-2 spike protein or receptor-binding domain [87]. Engineered multivalent nanobodies constructs with superior neutralizing activity can block SARS-CoV-2 entry, either by inhibition of receptor binding or by inducing conformational modifications that prevent viral–cell fusion [88]. In experimental mice models, prophylactically administered combinations of bivalent nanobody-Fc fusions, recognizing different epitopes in SARS-CoV-2 RBD, were able to decrease viral replication [89].
Nanobodies that target chemokines or cytokines, can be customized to modify inflammatory responses in COVID-19 disease [90]. Previously, several studies using the phage display method to elicit nanobodies directed towards cytokines were published, proving higher efficacy compared to the traditional cytokine blocking antibodies [91,92].
4.2. Novel Viral Entry Inhibitors
Bemcentinib is a selective inhibitor of the AXL receptor tyrosine kinase, that mediates uptake of the apoptotic bodies, used by SARS-CoV-2 in a process of apoptotic mimicry, to adhere to and internalize into the host cells. Bemcentinib is currently tested in two phase 2b clinical trials in hospitalized COVID-19 patients. The first study recently reported the short-term efficacy results, with minor benefits in the primary trial endpoints (time to improvement by two points on the WHO ordinal scale or time to discharge), but with potentially significant clinical benefits in a key secondary endpoint (avoidance of clinical deterioration) [93].
4.3. Inhibitors of Host Transmembrane Surface Protease TMPRSS2
Camostat mesylate, an oral serine protease inhibitor, primarily used for symptomatic treatment in gastrointestinal tract disorders, is a potent inhibitor of the TMPRSS2 protease used by SARS-CoV-2 to prime and activate the spike protein. Randomized, double-blinded studies, with clinical endpoints including viral load, number of hospitalization days, and mortality, show that camostat mesylate might be a promising repurposed drug, with a very good safety profile in humans [94].
N-0385 is a small peptidomimetic molecule, an inhibitor of TMPRSS2, that shows high efficacy in vitro on several SARS-CoV-2 variants (Alpha, Beta, Gamma, Delta) at low, nanomolar concentrations. The drug demonstrated a potential prophylactic and therapeutic effect during experimental intranasal infection in a transgenic mouse model, that expresses the human ACE2 receptor driven by a keratin promoter [95]. Further studies are necessary to evaluate the efficacy of this compound on the Omicron variant, which was shown to have a decreased use of TMPRSS2 and a preference for endocytosis dependent cell entry, with altered spike processing and reduced fusogenicity [96].
4.4. Interferons
A limited and delayed interferon (IFN) response might stimulate an uncontrolled viral replication and an aberrant immune response, leading to severe forms of SARS-CoV-2 infection. Patients with errors in the type I IFN activating pathways and those with autoantibodies neutralizing type I IFN are prone to a severe course of COVID-19 [97,98].
Systemic and inhaled IFN alpha and beta were administered in hospitalized patients, either alone or in combinations with antivirals, such as remdesivir or ribavirin, without major clinical benefits [99,100].
Interferon lambda has a limited inflammatory activity, due to a more restricted distribution of its IFNLR1/IL10R2 receptors, on epithelial and immune cells [101]. Small randomized clinical trials with peginterferon lambda did not show significant clinical benefits for non-hospitalized patients [102], although an accelerated suppression of viral replication was demonstrated [103].
Interferons can inhibit cell division, as such, treatment is associated with flu-like symptoms, nausea, fatigue, weight loss, hematological toxicities, alopecia, elevated transaminases, and psychiatric problems (e.g., depression, suicidal ideation) can most often occur. Concomitant treatment with immunomodulatory drugs or chemotherapeutic agents is not recommended, due to an increased risk of toxicity. Administration in pregnancy is not safe, as congenital anomalies in the fetus or spontaneous abortion may occur. There are insufficient data for interferons’ administration in children [26].
5. Conclusions
Information related to the structure, replication, and epidemiology of zoonotic coronaviruses has slowly accumulated after SARS and MERS CoV-2 emergence, and the development of therapeutical molecules were inherently limited. Huge collaborative studies initiated during the SARS-CoV-2 pandemic spread have triggered the discovery and testing of several monoclonal antibodies’ combinations that block viral entry and of small molecules with direct antiviral activity, inhibitors of the viral RNA polymerase or the main viral protease, that can potentially change the clinical outcomes of COVID-19. A rational therapeutic use is needed to preserve their efficacy, to avoid drug-resistance, and to identify the most vulnerable patients who might benefit from early administration. New therapeutic and prophylactic strategies are warranted in order to avoid the major societal and economic disruption caused by SARS-CoV-2 variants and by other potential zoonotic coronaviruses, that might cause future viral outbreaks.
Author Contributions
All authors contributed equally in Conceptualization, methodology, validation, formal analysis, data curation, writing. All authors have read and agreed to the published version of the manuscript.
Funding
This paper was financially supported by the “Carol Davila” University of Medicine and Pharmacy Bucharest, Romania through Contract no. 33PFE/30.12.2021 funded by the Ministry of Research and Innovation within PNCDI III, Program 1-Development of the National RD system, Subprogram 1.2-Institutional Performance-RDI excellence funding projects.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hu, B.; Guo, H.; Zhou, P. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Our World in Data. Available online: https://ourworldindata.org (accessed on 30 March 2022).
- Atzrodt, C.L.; Maknojia, I.; McCarthy, D.P.; Oldfield, T.M.; Jonathan, P.; Kenny, T.L.; Stepp, H.E.; Clements, T. A Guide to COVID-19: A global pandemic caused by the novel coronavirus SARS-CoV-2. FEBS J. 2020, 287, 3633–3650. [Google Scholar] [CrossRef] [PubMed]
- Lythgoe, K.A.; Hall, M.D. Shared SARS-CoV-2 diversity suggests localized transmission of minority variants. Science 2021, 372, 1–10. [Google Scholar] [CrossRef]
- Ramanathan, M.; Ferguson, I.D.; Miao, W.; Khavari, P.A. SARS-CoV-2 B.1.1.7 and B.1.351 spike variants bind human ACE2 with increased affinity. Lancet Infect. Dis. 2021, 21, 1070. [Google Scholar] [CrossRef]
- Davies, N.G.; Jarvis, C.I.; Edmunds, W.J.; Jewell, N.P.; Diaz-Ordaz, K.; Keogh, R.H. Increased mortality in community-tested cases of SARS-CoV-2 lineage B.1.1.7. Nature 2021, 593, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy, and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Therapeutics and COVID-19: Living Guideline-World Health Organization (WHO). Available online: https://apps.who.int/iris/bitstream/handle/10665/351006/WHO-2019-nCoV-therapeutics-2022.1-eng.pdf (accessed on 26 February 2022).
- Emergency Use Authorization (EUA) of COVID-19 Convalescent Plasma for Treatment of Coronavirus Disease 2019 (COVID-19). Available online: https://www.fda.gov/media/141478/download (accessed on 27 February 2022).
- Abd-Elsalam, S.; Noor, R.A.; Badawi, R.; Khalaf, M.; Esmail, E.S.; Soliman, S.; Abd El Ghafar, M.S.; Elbahnasawy, M.; Moustafa, E.F.; Hassany, S.M.; et al. Clinical study evaluating the efficacy of ivermectin in COVID-19 treatment: A randomized controlled study. J. Med. Virol. 2021, 93, 5833–5838. [Google Scholar] [CrossRef]
- Joshi, S.; Parkar, J.; Ansari, A.; Vora, A.; Talwar, D.; Tiwaskar, M.; Patil, S.; Barkate, H. Role of favipiravir in the treatment of COVID-19. Int. J. Infect. Dis. 2021, 102, 501–508. [Google Scholar] [CrossRef]
- Buonfrate, D.; Chesini, F.; Martini, D.; Roncaglioni, M.C.; Ojeda, M.L.; Alvisi, M.F.; Ruli, E. High-dose ivermectin for early treatment of COVID-19 (COVER study): A randomized, double-blind, multicentre, phase II, dose-finding, proof-of-concept clinical trial. Int. J. Antimicrob. Agents 2022, 59, 106516. [Google Scholar] [CrossRef]
- Paludan, S.R.; Mogensen, T.H. Innate immunological pathways in COVID-19 pathogenesis. Sci. Immunol. 2022, 7, eabm5505. [Google Scholar] [CrossRef]
- Majumder, J.; Minko, T. Recent Developments on Therapeutic and Diagnostic Approaches for COVID-19. AAPS J. 2021, 23, 14. [Google Scholar] [CrossRef] [PubMed]
- Mititelu, M.; Stanciu, T.I.; Udeanu, D.I.; Popa, D.E. The Impact of COVID-19 lockdown on the lifestyle and dietary patterns among romanian population. Farmacia 2021, 69, 1. [Google Scholar] [CrossRef]
- Arsene, A.L.; Dumitrescu, B.I.; Udeanu, D.I.; Dragoi, C.M. A new era for the therapeutic management of the ongoing COVID-19 pandemic. Farmacia 2020, 68, 2. [Google Scholar] [CrossRef]
- Van Der Hoek, L.; Pyrc, K.; Jebbink, M.F.; Vermeulen-Oost, W.; Berkhout, R.J.; Wolthers, K.C.; Wertheim-van Dillen, P.M.; Kaandorp, J.; Spaargaren, J.; Berkhout, B. Identification of a new human coronavirus. Nat. Med. 2004, 10, 368–373. [Google Scholar] [CrossRef]
- Astuti, I.; Ysrafil. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): An overview of viral structure and host response. Diabetes Metab. Syndr. 2020, 14, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z. Clinical course and risk factors for mortality of adult in patients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Dubey, A.; Choudhary, S.; Kumar, P.; Tomar, S. Emerging SARS-CoV-2 Variants: Genetic Variability and Clinical Implications. Curr. Microbiol. 2021, 79, 20. [Google Scholar] [CrossRef]
- Alexandersen, S.; Chamings, A.; Bhatta, T.R. SARS-CoV-2 genomic and subgenomic RNAs in diagnostic samples are not an indicator of active replication. Nat. Commun. 2020, 11, 6059. [Google Scholar] [CrossRef]
- JHMI Clinical Recommendations for Pharmacologic Treatment of COVID-19. Available online: https://www.hopkinsguides.com/hopkins/ub?cmd=repview&type=479-1225&name=30_538747_PDF (accessed on 23 February 2022).
- Bhimraj, A.; Morgan, R.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Cheng, V. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19, IDSA Guidelines on COVID-19. Available online: https://www.idsociety.org/COVID19guidelines (accessed on 26 February 2022).
- Cao, Y.; Su, B.; Guo, X.; Sun, W.; Deng, Y.; Bao, L.; Zhu, Q.; Zhang, X.; Zheng, Y.; Geng, C.; et al. Potent Neutralizing Antibodies against SARS-CoV-2 Identified by High-Throughput Single-Cell Sequencing of Convalescent Patients’ B Cells. Cell 2020, 182, 73–84.e16. [Google Scholar] [CrossRef]
- O’Brien, M.P.; Forleo-Neto, E.; Sarkar, N. Effect of Subcutaneous Casirivimab and Imdevimab Antibody Combination vs Placebo on Development of Symptomatic COVID-19 in Early Asymptomatic SARS-CoV-2 Infection. JAMA 2022, 327, 432. [Google Scholar] [CrossRef]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 27 February 2022).
- Dougan, M.; Nirula, A.; Azizad, M.; Mocherla, B.; Gottlieb, R.L.; Chen, P.; Hebert, C.; Perry, R.; Boscia, J.; Heller, B.; et al. Bamlanivimab plus Etesevimab in Mild or Moderate COVID-19. N. Engl. J. Med. 2021, 385, 1382–1392. [Google Scholar] [CrossRef] [PubMed]
- Bamlanivimab and Etesevimab, Monoclonal Antibodies. Available online: https://www.precisionvaccinations.com/vaccines/bamlanivimab-and-etesevimab-monoclonal-antibodies (accessed on 27 February 2022).
- Heo, Y.A. Sotrovimab: First Approval. Drugs 2022, 82, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Tortorici, M.A.; Czudnochowski, N.; Starr, T.N.; Marzi, R.; Walls, A.C.; Zatta, F.; Bowen, J.E.; Jaconi, S.; Di Iulio, J.; Wang, Z.; et al. Broad sarbecovirus neutralization by a human monoclonal antibody. Nature 2021, 597, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Gonzalez-Rojas, Y.; Juarez, E.; Crespo Casal, M.; Moya, J.; Falci, D.R.; Sarkis, E.; Solis, J.; Zheng, H.; Scott, N.; et al. COMET-ICE Investigators. Early Treatment for COVID-19 with SARS-CoV-2 Neutralizing Antibody Sotrovimab. N. Engl. J. Med. 2021, 385, 1941–1950. [Google Scholar] [CrossRef] [PubMed]
- Fact Sheet for Healthcare Providers: Emergency Use Authorization for Evusheldtm (Tixagevimab Co-Packaged with Cilgavimab). Available online: https://www.fda.gov/media/154701/download (accessed on 27 February 2022).
- Levin, M.J.; Ustianowski, A.; De Wit, S. LB5. PROVENT: Phase 3 Study of Efficacy and Safety of AZD7442 (Tixagevimab/Cilgavimab) for Pre-exposure Prophylaxis of COVID-19 in Adults. Open Forum. Infect. Dis. 2021, 8 (Suppl. S1), S810. [Google Scholar] [CrossRef]
- Evusheld Long-Acting Antibody Combination Retains Neutralizing Activity Against Omicron Variant in Independent FDA study. Available online: https://www.astrazeneca.com/media-centre/press-releases/2021/evusheld-long-acting-antibody-combination-retains-neutralising-activity-against-omicron-variant-in-independent-fda-study.html (accessed on 30 March 2022).
- Westendorf, K.; Žentelis, S.; Wang, L.; Foster, D.; Vaillancourt, P.; Wiggin, M.; Lovett, E.; van der Lee, R.; Hendle, J.; Pustilnik, A.; et al. LY-CoV1404 (bebtelovimab) potently neutralizes SARS-CoV-2 variants. BioRxiv 2022, preprint. [Google Scholar] [CrossRef]
- Humeniuk, R.; Mathias, A.; Cao, H.; Osinusi, A.; Shen, G.; Chng, E.; Ling, J.; Vu, A.; German, P. Safety, Tolerability, and Pharmacokinetics of Remdesivir, An Antiviral for Treatment of COVID-19, in Healthy Subjects. Clin. Transl. Sci. 2020, 13, 896–906. [Google Scholar] [CrossRef]
- EMA Veklury RCP. Available online: https://www.ema.europa.eu/en/documents/product-information/veklury-epar-product-information_ro.pdf (accessed on 15 March 2022).
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe COVID-19 in Outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef]
- Ader, F.; Bouscambert-Duchamp, M.; Hites, M.; Peiffer-Smadja, N.; Pissy, J.; Belhadi, D. Remdesivir plus standard of care versus standard of care alone for the treatment of patients admitted to hospital with COVID-19 (DisCoVeRy): A phase 3, randomized, controlled, open-label trial. Lancet Infect. Dis. 2022, 22, 209–221. [Google Scholar] [CrossRef]
- Vermillion, M.S.; Murakami, E.; Ma, B.; Pitts, J.; Tomkinson, A.; Rautiola, D.; Babusis, D.; Irshad, H.; Siegel, D.; Kim, C.; et al. Inhaled remdesivir reduces viral burden in a nonhuman primate model of SARS-CoV-2 infection. Sci. Transl. Med. 2021, 14, eabl828. [Google Scholar] [CrossRef]
- Schäfer, A.; Martinez, D.A.; Won, J.; Meganck, R.; Moreira, F.; Brown, A.; Gully, K.; Zweigart, M.; Conrad, W. Therapeutic treatment with an oral prodrug of the remdesivir parental nucleoside is protective against SARS-CoV-2 pathogenesis in mice. Sci. Transl. Med. 2022, 14, eabm3410. [Google Scholar] [CrossRef] [PubMed]
- Mount Sinai Health System Treatment Guidance for SARS-CoV-2 Infection (COVID-19), Updated in the setting of Omicron Variant of Concern. Available online: https://www.mountsinai.org/files/MSHealth/Assets/HS/About/Coronavirus/Mount-Sinai-Health-System-Treatment-Guidelines-for-COVID-Updated.pdf (accessed on 27 February 2022).
- PK and Safety of Remdesivir for Treatment of COVID-19 in Pregnant and Non-Pregnant Women in the US. Available online: https://clinicaltrials.gov/ct2/show/record/NCT04582266 (accessed on 26 February 2022).
- Goldman, D.L.; Aldrich, M.L.; Hagmann, S.H.; Bamford, A.; Camacho-Gonzalez, A.; Lapadula, G.; Lee, P.; Bonfanti, P.; Carter, C.C.; Zhao, Y. Compassionate Use of Remdesivir in Children with Severe COVID-19. Pediatrics 2021, 147, e2020047803. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus (COVID-19) Update: FDA Approves First COVID-19 Treatment for Young Children. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-approves-first-covid-19-treatment-young-children (accessed on 1 May 2022).
- Cox, R.M.; Wolf, J.D.; Plemper, R.K. Therapeutically administered ribonucleoside analog MK-4482/EIDD-2801 blocks SARS-CoV-2 transmission in ferrets. Nat. Microbiol. 2021, 6, 11–18. [Google Scholar] [CrossRef]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of COVID-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef]
- Manabe, T.; Kambayashi, D.; Akatsu, H.; Kudo, K. Favipiravir for the treatment of patients with COVID-19: A systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 489. [Google Scholar] [CrossRef] [PubMed]
- Özlüşen, B.; Kozan, Ş.; Akcan, R.E.; Kalender, M.; Yaprak, D.; Peltek, İ.B.; Ergönül, Ö. Effectiveness of favipiravir in COVID-19: A live systematic review. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2021, 40, 2575–2583. [Google Scholar] [CrossRef] [PubMed]
- Fact Sheet for Healthcare Providers: Emergency Use Authorization for Paxlovid. Available online: https://www.fda.gov/media/155050/download (accessed on 26 February 2022).
- Eng, H.; DAntonio, A.; Kadar, E.; Obach, S.; Di, L.; Lin, J.; Patel, N.; Boras, B.; Walker, G.; Novak, J.; et al. Disposition of PF-07321332 (Nirmatrelvir), an Orally Bioavailable Inhibitor of SARS-CoV-2 3CL Protease, across Animals and Humans. Available online: https://dmd.aspetjournals.org/content/dmd/early/2022/02/13/dmd.121.000801.full.pdf (accessed on 27 February 2022).
- Owen, D.R.; Allerton, C.; Anderson, A.; Avery, M.; Berritt, S.; Cardin, R.; Zhu, Y. An oral SARS-CoV-2 Mpro inhibitor clinical candidate for the treatment of COVID-19. Science 2021, 374, 1586–1593. [Google Scholar] [CrossRef]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with COVID-19. N. Engl. J. Med. 2022, 386, NEJMoa2118542. [Google Scholar] [CrossRef]
- Hung, Y.-P.; Lee, J.-C.; Chiu, C.-W.; Lee, C.-C.; Tsai, P.-J.; Hsu, I.-L.; Ko, W.-C. Oral Nirmatrelvir/Ritonavir Therapy for COVID-19: The Dawn in the Dark? Antibiotics 2022, 11, 220. [Google Scholar] [CrossRef]
- PAXLOVID (Nirmatrelvir; Ritonavir) Product Monograph. Available online: https://covid-vaccine.canada.ca/info/pdf/paxlovid-pm-en.pdf (accessed on 26 February 2022).
- Assessing a Patient for Paxlovid (Nirmatrelvir/Ritonavir). Available online: https://www.covid19-druginteractions.org/prescribing-resources (accessed on 26 February 2022).
- Abdelnabi, R.; Foo, C.S.; Jochmans, D.; Vangeel, L.; De Jonghe, S.; Augustijns, P.; Mols, R.; Weynand, B.; Wattanakul, T.; Hoglund, R.M.; et al. The oral protease inhibitor (PF-07321332) protects Syrian hamsters against infection with SARS-CoV-2 variants of concern. Nat. Commun. 2022, 13, 719. [Google Scholar] [CrossRef]
- Ullrich, S.; Ekanayake, K.B.; Otting, G.; Nitsche, C. Main protease mutants of SARS-CoV-2 variants remain susceptible to nirmatrelvir. Bioorg. Med. Chem. Lett. 2022, 62, 128629. [Google Scholar] [CrossRef] [PubMed]
- Finney, L.J.; Glanville, N.; Farne, H.; Aniscenko, J.; Fenwick, P.; Kemp, S.V.; Trujillo-Torralbo, M.-B.; Loo, S.L.; Calderazzo, M.A.; Wedzicha, J.A.; et al. Inhaled corticosteroids downregulate the SARS-CoV-2 receptor ACE2 in COPD through suppression of type I interferon. J. Allergy Clin. Immunol. 2021, 147, 510–519.e5. [Google Scholar] [CrossRef] [PubMed]
- EMA. Insufficient Data on Use of Inhaled Corticosteroids to Treat COVID-19. Available online: https://www.ema.europa.eu/en/news/insufficient-data-use-inhaled-corticosteroids-treat-covid-19 (accessed on 15 March 2022).
- Gordon, A.C.; Mouncey, P.R.; Al-Beidh, F.; Rowan, K.M.; Nichol, A.D.; Arabi, Y.M. The REMAP-CAP Investigators, Interleukin-6 Receptor Antagonists in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 384, 1491–1502. [Google Scholar] [CrossRef]
- NIH Guidelines. Available online: https://osp.od.nih.gov/biotechnology/nih-guidelines/ (accessed on 17 March 2022).
- Fact Sheet for Healthcare Providers: Emergency Use Authorization for Actemra® (Tocilizumab). Available online: https://www.gene.com/download/pdf/actemra_eua_hcp_fact_sheet.pdf (accessed on 27 February 2022).
- Recovery Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Davidescu, E.I.; Odajiu, I.; Ilie, M.D.; Bunea, T.; Sandu, G.; Stratan, L.; Iftode, N.; Arama, V.; Popescu, B.O. Influence of Tocilizumab on the Outcome of Patients with COVID-19. Retrospective observational study. Farmacia 2020, 68, 5. [Google Scholar] [CrossRef]
- Meira, F.; Albiach, L.; Carbonell, C.; Martín-Oterino, J.Á.; Martín-Ordiales, M.; Linares, L.; Macaya, I.; Agüero, D.; Ambrosioni, J.; Bodro, M.; et al. Experience with the use of siltuximab in patients with SARS-CoV-2 infection. Rev. Española Quimioter. 2021, 34, 337. [Google Scholar] [CrossRef]
- EMA Recommends Approval for Use of Kineret in Adults with COVID-19. Available online: https://www.ema.europa.eu/en/news/ema-recommends-approval-use-kineret-adults-covid-19 (accessed on 26 February 2022).
- Kharazmi, A.B.; Moradi, O.; Haghighi, M.; Kouchek, M.; Manafi-Rasi, A.; Raoufi, M.; Shoaei, S.D.; Hadavand, F.; Nabavi, M.; Miri, M.M.; et al. A randomized controlled clinical trial on efficacy and safety of anakinra in patients with severe COVID-19. Immun. Inflamm. Dis. 2022, 10, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Katia, F.; Myriam, D.P.; Ucciferri, C. Efficacy of canakinumab in mild or severe COVID-19 pneumonia. Immun. Inflamm. Dis. 2021, 9, 399–405. [Google Scholar] [CrossRef]
- Generali, D.; Bosio, G.; Malberti, F.; Cuzzoli, A.; Testa, S.; Romanini, L.; Fioravanti, A.; Morandini, A.; Pianta, L.; Giannotti, G.; et al. Canakinumab as treatment for COVID-19-related pneumonia: A prospective case-control study. Int. J. Infect. Dis. 2021, 104, 433–440. [Google Scholar] [CrossRef]
- Caricchio, R.; Abbate, A.; Gordeev, I. Effect of Canakinumab vs. Placebo on Survival Without Invasive Mechanical Ventilation in Patients Hospitalized with Severe COVID-19: A Randomized Clinical Trial. JAMA 2021, 326, 230–239. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, Y.; Qiao, W.; Zhang, J.; Qi, Z. Baricitinib, a drug with potential effect to prevent SARS-CoV-2 from entering target cells and control cytokine storm induced by COVID-19. Int. Immunopharmacol. 2020, 86, 106749. [Google Scholar] [CrossRef] [PubMed]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.; Tomashek, K.; Wolfe, C.; Marconi, V.; Kline, S.; Tapson, V. Baricitinib plus Remdesivir for Hospitalized Adults with COVID-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef]
- Marconi, V.C.; Ramanan, A.V.; de Bono, S.; Kartman, C.E.; Krishnan, V.; Liao, R.; Piruzeli, M.L.B.; Goldman, J.D.; Alatorre-Alexander, J.; de Cassia Pellegrini, R.; et al. Efficacy and safety of baricitinib for the treatment of hospitalized adults with COVID-19 (COV-BARRIER): A randomized, double-blind, parallel-group, placebo-controlled phase 3 trial. Lancet Respir. Med. 2021, 9, 1407–1418. [Google Scholar] [CrossRef]
- Fact Sheet for Healthcare Providers Emergency Use Authorization (EUA) of Baricitinib. Available online: https://www.fda.gov/media/143823/download (accessed on 26 February 2022).
- Le Corre, P.; Loas, G. Difficulty in Repurposing Selective Serotonin Reuptake Inhibitors and Other Antidepressants with Functional Inhibition of Acid Sphingomyelinase in COVID-19 Infection. Front. Pharmacol. 2022, 13, 849095. [Google Scholar] [CrossRef] [PubMed]
- Reis, G.; dos Santos Moreira-Silva, E.A.; Silva, D.C.M.; Thabane, L.; Milagres, A.C.; Ferreira, T.S.; Dos Santos, C.V.Q.; de Souza Campos, V.H.; Nogueira, A.M.R.; de Almeida, A.P.F.G.; et al. Effect of early treatment with fluvoxamine on risk of emergency care and hospitalization among patients with COVID-19: The together randomised, platform clinical trial. Lancet Glob Health 2022, 10, e42–e51. [Google Scholar] [CrossRef]
- Cameroni, E.; Bowen, J.E.; Rosen, L.E. Broadly neutralizing antibodies overcome SARS-CoV-2 Omicron antigenic shift. Nature 2022, 602, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Vanshylla, K.; Fan, C.; Wunsch, M.; Poopalasingam, N.; Meijers, M.; Kreer, C.; Kleipass, F.; Ruchnewitz, D.; Ercanoglu, M.S.; Gruell, H.; et al. Discovery of ultrapotent broadly neutralizing antibodies from SARS-CoV-2 elite neutralizers. Cell Host Microbe 2022, 30, 69–82.e10. [Google Scholar] [CrossRef]
- Renn, A.; Fu, Y.; Hu, X.; Hall, M.D.; Simeonov, A. Fruitful neutralizing antibody pipeline brings hope to defeat SARS-CoV-2. Trends Pharmacol. Sci. 2020, 41, 815–829. [Google Scholar] [CrossRef]
- Kumar, M.; Kuroda, K.; Dhangar, K.; Mazumder, P.; Sonne, C.; Rinklebe, J.; Kitajima, M. Potential emergence of antiviral-resistant pandemic viruses via environmental drug exposure of animal reservoirs. Environ. Sci. Technol. 2020, 54, 8503–8505. [Google Scholar] [CrossRef]
- Stanfield, R.L.; Dooley, H.; Flajnik, M.F.; Wilson, I.A. Crystal structure of a shark single-domain antibody V region in complex with lysozyme. Science 2004, 305, 1770–1773. [Google Scholar] [CrossRef]
- Bannas, P.; Hambach, J.; Koch-Nolte, F. Nanobodies and Nanobody-Based Human Heavy Chain Antibodies as Antitumor Therapeutics. Front. Immunol. 2017, 8, 1603. [Google Scholar] [CrossRef] [PubMed]
- Jovcevska, I.; Muyldermans, S. The Therapeutic Potential of Nanobodies. BioDrugs 2020, 34, 11–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bessalah, S.; Jebahi, S.; Mejri, N.; Salhi, I.; Khorchani, T.; Hammadi, M. Perspective on therapeutic and diagnostic potential of camel nanobodies for coronavirus disease-19 (COVID-19). 3 Biotech 2021, 11, 89. [Google Scholar] [CrossRef] [PubMed]
- Wrapp, D.; de Vlieger, D.; Corbett, K.S.; Torres, G.M.; Wang, N.; Van Breedam, W.; Roose, K.; van Schie, L.; Hoffmann, M.; Pöhlmann, S.; et al. Structural basis for potent neutralization of betacoronaviruses by single-domain camelid antibodies. Cell 2020, 181, 1004–1015. [Google Scholar] [CrossRef] [PubMed]
- Esparza, T.J.; Martin, N.P.; Anderson, G.P. High affinity nanobodies block SARS-CoV-2 spike receptor binding domain interaction with human angiotensin converting enzyme. Sci. Rep. 2020, 10, 22370. [Google Scholar] [CrossRef]
- Koenig, P.A.; Das, H.; Liu, H.; Kümmerer, B.M.; Gohr, F.N.; Jenster, L.M.; Schiffelers, L.D.; Tesfamariam, Y.M.; Uchima, M.; Wuerth, J.D.; et al. Structure-guided multivalent nanobodies block SARS-CoV-2 infection and suppress mutational escape. Science 2021, 371, eabe6230. [Google Scholar] [CrossRef]
- Pymm, P.; Adair, A.; Chan, L.J.; Cooney, J.P.; Mordant, F.L.; Allison, C.C.; Lopez, E.; Haycroft, E.R.; O’Neill, M.T.; Tan, L.L.; et al. Nanobody cocktails potently neutralize SARS-CoV-2 D614G N501Y variant and protect mice. Proc. Natl. Acad. Sci. USA 2021, 118, e2101918118. [Google Scholar] [CrossRef]
- Wen, W.; Su, W.; Tang, H.; Le, W.; Zhang, X.; Zheng, Y.; Liu, X.; Xie, L.; Li, J.; Ye, J.; et al. Immune cell profiling of COVID-19 patients in the recovery stage by single-cell sequencing. Cell Discov. 2020, 6, 31. [Google Scholar] [CrossRef]
- Nosenko, M.A.; Atretkhany, K.N.; Mokhonov, V.V.; Efimov, G.A.; Kruglov, A.A.; Tillib, S.V.; Drutskaya, M.S.; Nedospasov, S.A. VHH-Based Bispecific Antibodies Targeting Cytokine Production. Front. Immunol. 2017, 8, 1073. [Google Scholar] [CrossRef] [Green Version]
- Coppieters, K.; Dreier, T.; Silence, K.; Lauwereys, M.; Casteels, P.; Beirnaert, E. Formatted anti-tumor necrosis factor alpha VHH proteins derived from camelids show superior potency and targeting to inflamed joints in a murine model of collagen-induced arthritis. Arthritis Rheum. 2006, 54, 1856–1866. [Google Scholar] [CrossRef]
- BerGenBio, Oslo University Hospital to Test Bemcentinib in Hospitalised COVID-19 Patients. Available online: https://www.clinicaltrialsarena.com/news/bergenbio-trial-bemcentinib-covid/ (accessed on 19 March 2022).
- Hoffmann, M.; Hofmann-Winkler, H.; Smith, J.C. Camostat mesylate inhibits SARS-CoV-2 activation by TMPRSS2-related proteases and its metabolite GBPA exerts antiviral activity. EBioMedicine 2021, 65, 103255. [Google Scholar] [CrossRef] [PubMed]
- Shapira, T.; Monreal, I.A.; Dion, S.P.; Buchholz, D.W.; Imbiakha, B.; Olmstead, A.D.; Jager, M.; Désilets, A.; Gao, G.; Martins, M.; et al. A TMPRSS2 inhibitor acts as a pan-SARS-CoV-2 prophylactic and therapeutic. Nature 2022, 605, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Meng, B.; Abdullahi, A.; Ferreira, I.A.; Goonawardane, N.; Saito, A.; Kimura, I.; Yamasoba, D.; Gerber, P.P.; Fatihi, S.; Rathore, S.; et al. Altered TMPRSS2 usage by SARS-CoV-2 Omicron impacts infectivity and fusogenicity. Nature 2022, 603, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Bastard, P.; Liu, Z.; Le Pen, J.; Moncada-Velez, M.; Chen, J. Inborn errors of type I IFN immunity in patients with life-threatening COVID-19. Science 2020, 370, eabd4570. [Google Scholar] [CrossRef] [PubMed]
- Bastard, P.; Rosen, L.B.; Zhang, Q.; Michailidis, E.; Hoffmann, H.-H.; Zhang, Y.; Dorgham, K. Autoantibodies against type I IFNs in patients with life-threatening COVID-19. Science 2020, 370, eabd4585. [Google Scholar] [CrossRef] [PubMed]
- Hung, I.F.; Lung, K.C.; Tso, E.Y. Triple combination of interferon beta-1b, lopinavir-ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: An open-label, randomised, Phase 2 trial. Lancet 2020, 395, 1695–1704. [Google Scholar] [CrossRef]
- WHO Solidarity Trial Consortium; Pan, H.; Peto, R. Repurposed antiviral drugs for COVID-19-interim WHO Solidarity Trial results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar]
- Prokunina-Olsson, L.; Alphonse, N.; Dickenson, R.E.; Durbin, J.E.; Glenn, J.S.; Hartmann, R.; Kotenko, S.V. COVID-19 and emerging viral infections: The case for interferon lambda. J. Exp. Med. 2020, 217, e20200653. [Google Scholar] [CrossRef] [Green Version]
- Jagannathan, P.; Andrews, J.R.; Bonilla, H.; Hedlin, H.; Jacobson, K.B.; Balasubramanian, V.; Purington, N. Peginterferon Lambda-1a for treatment of outpatients with uncomplicated COVID-19: A randomized placebo-controlled trial. Nat. Commun. 2021, 12, 1967. [Google Scholar] [CrossRef]
- Feld, J.J.; Kandel, C.; Biondi, M.J.; Kozak, R.A.; Zahoor, M.A.; Lemieux, C.; Borgia, S.M. Peginterferon lambda for the treatment of outpatients with COVID-19: A phase 2, placebo-controlled randomized trial. Lancet. Respir. Med. 2021, 9, 498–510. [Google Scholar] [CrossRef]
Figure 1.
Diagram of direct acting antivirals in SARS-CoV-2 infection.


{kind=link}
Table 1.
Drugs currently used for COVID-19 therapy.
| Therapeutic Agent | Pharmacological Classification | Mechanism of Action | Outpatient | Inpatient |
|---|---|---|---|---|
| Sotrovimab | Entry inhibitors-Anti-Spike Monoclonal Antibodies | Bind to the spike protein of SARS-CoV-2, inhibiting attachment to the ACE2 receptor | ✔ | ✔ ✔ |
| Tixagevimab/cilgavimab | ✔ | ✔ | ||
| Bebtelovimab Casirivimab/imdevimab * Bamlanivimab/etesevimab * | ✔ | ✔ | ||
| Remdesivir | Antivirals targeting the RNA-dependent RNA polymerase (RdRp) | Inhibition of viral genome replication | ✔ | ✔ |
| Molnupiravir | ✔ | |||
| Nirmatrelvir/Ritonavir | Protease inhibitors | Inhibit polyprotein cleavage and the formation of non-structural proteins essential for viral replication | ✔ | |
| Corticosteroids | Immunomodulators | Decrease inflammatory response | ✔ | ✔ |
| Tocilizumab | Anti-Interleukin-6 Receptor Monoclonal Antibodies | Interleukin (IL)-6 receptor antagonists, inhibition of IL-6 signaling pathway | ✔ | |
| Sarilumab | ✔ | |||
| Siltuximab | ✔ | |||
| Baricitinib | Janus kinase inhibitors | Selective JAK1/JAK2 inhibitors | ✔ | |
| Ruxolitinib | ✔ | |||
| Anakinra | Monoclonal antibody anti IL1 beta receptor | ✔ |
* low/no efficacy against SARS-CoV-2 Omicron variant.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lupașcu, R.E.; Ilie, M.I.; Velescu, B.Ș.; Udeanu, D.I.; Sultana, C.; Ruță, S.; Arsene, A.L. COVID-19-Current Therapeutical Approaches and Future Perspectives. Processes 2022, 10, 1053. https://doi.org/10.3390/pr10061053
AMA Style
Lupașcu RE, Ilie MI, Velescu BȘ, Udeanu DI, Sultana C, Ruță S, Arsene AL. COVID-19-Current Therapeutical Approaches and Future Perspectives. Processes. 2022; 10(6):1053. https://doi.org/10.3390/pr10061053
Chicago/Turabian StyleLupașcu (Moisi), Raluca Elisabeta, Marina Ionela Ilie, Bruno Ștefan Velescu, Denisa Ioana Udeanu, Camelia Sultana, Simona Ruță, and Andreea Letiția Arsene. 2022. "COVID-19-Current Therapeutical Approaches and Future Perspectives" Processes 10, no. 6: 1053. https://doi.org/10.3390/pr10061053
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.