
Predictors of Mortality in Hemodialyzed Patients after SARS-CoV-2 Infection

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Design
2.3. Study Population
2.4. Data Collections and Procedures
2.5. Outcome
2.6. Statistical Analyses
3. Results
3.1. Patients Demographic and Clinical Characteristic
3.2. Presentation at Admission and Outcome
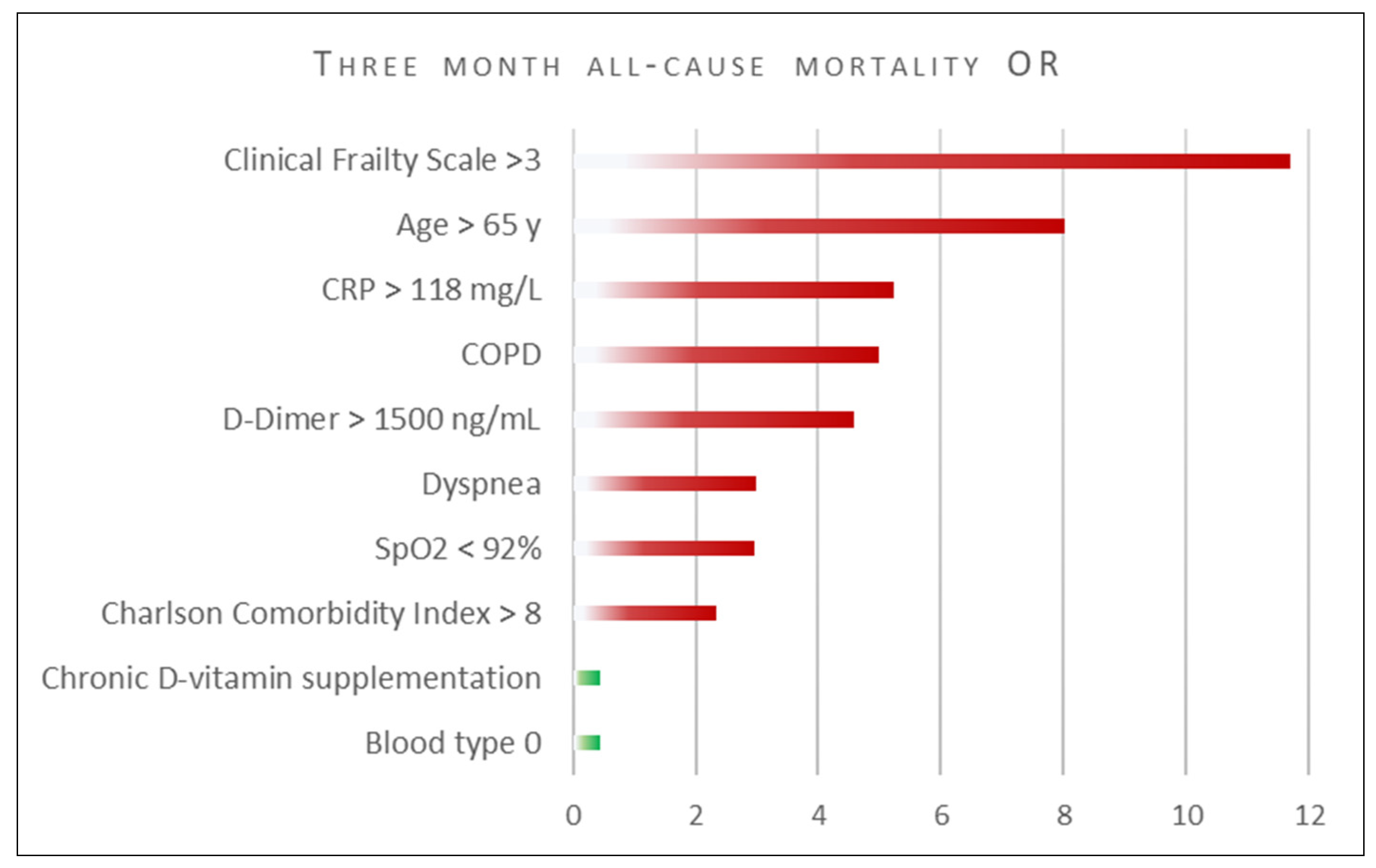
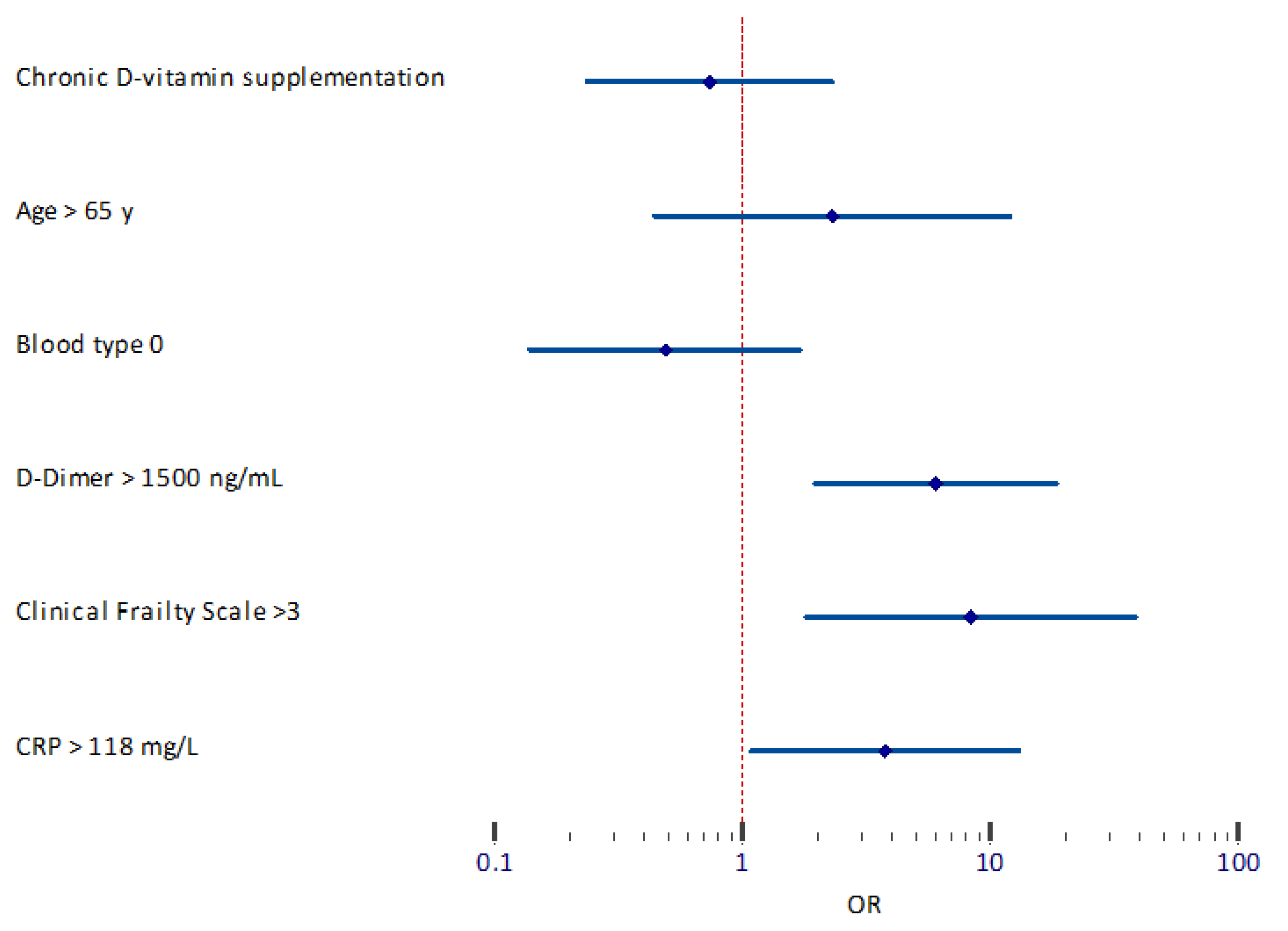
3.3. Predictors of Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vergara, A.; Molina-Van den Bosch, M.; Toapanta, N.; Villegas, A.; Sanchez-Camara, L.; Sequera, P.; Manrique, J.; Shabaka, A.; Aragoncillo, I.; Ruiz, M.C.; et al. The Impact of Age on Mortality in Chronic Haemodialysis Popu-Lation with COVID-19. J. Clin. Med. 2021, 10, 3022. [Google Scholar] [CrossRef]
- Hilbrands, L.B.; Duivenvoorden, R.; Vart, P.; Franssen, C.F.M.; Hemmelder, M.H.; Jager, K.J.; Kieneker, L.M.; Noordzij, M.; Pena, M.J.; Vries, H.; et al. COVID-19-related mortality in kidney transplant and dialysis patients: Results of the ERACODA collaboration. Nephrol. Dial. Transpl. 2020, 35, 1973–1983. [Google Scholar] [CrossRef] [PubMed]
- Puchalska-Reglińska, E.; Debska-Slizien, A.; Biedunkiewicz, B.; Tylicki, P.; Polewska, K.; Rutkowski, B.; Gellert, R.; Tylicki, L. Extremely high mortality in COVID-19 hemodialyzed patients before the anti-SARS-CoV-2 vaccination era. Large database from the North of Poland. Pol. Arch. Intern. Med. 2021, 131, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Och, A.; Tylicki, P.; Polewska, K.; Puchalska-Reglińska, E.; Parczewska, A.; Szabat, K.; Biedunkiewicz, B.; Debska Slizien, A.; Tylicki, L. Persistent post-COVID-19 syndrome in hemodialyzed patients—A longitudinal cohort study from the North of Poland. J. Clin. Med. 2021, 10, 4451. [Google Scholar] [CrossRef]
- Inciardi, R.M.; Lupi, L.; Zaccone, G.; Italia, L.; Raffo, M.; Tomasoni, D.; Cani, D.S.; Cerini, M.; Farina, D.; Gavazzi, E.; et al. Cardiac Involvement in a Patient With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 819–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tylicki, L.; Biedunkiewicz, B.; Dąbrowska, M.; Ślizień, W.; Tylicki, P.; Polewska, K.; Rosenberg, I.; Rodak, S.; Dębska-Ślizień, A. Humoral response to SARS-CoV-2 vaccination promises to improve the catastrophic prognosis of hemodialysis patients as a result of COVID-19. The COViNEPH Project. Pol. Arch. Intern. Med. 2021, 131, 797–801. [Google Scholar] [CrossRef] [PubMed]
- Biedunkiewicz, B.; Tylicki, L.; Puchalska-Reglińska, E.; Dąbrowska, M.; Ślizień, W.; Kubanek, A.; Rąbalski, Ł.; Kosiński, M.; Grzybek, M.; Renke, M.; et al. SARS-CoV-2 infection in vaccinated maintenance hemodialysis patients despite anti-spike seroconversion: A report of 3 breakthrough cases. Eur. J. Transl. Clin. Med. 2021. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Church, S.; Rogers, E.; Rockwood, K.; Theou, O. A scoping review of the Clinical Frailty Scale. BMC Geriatr. 2020, 20, 393. [Google Scholar] [CrossRef]
- Ranganathan, P.; Pramesh, C.S.; Aggarwal, R. Common pitfalls in statistical analysis: Logistic regression. Perspect. Clin. Res. 2017, 8, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Kowalska, M.; Baranski, K.; Brozek, G.; Kaleta-Pilarska, A.; Zejda, J.E. COVID-19-related risk of in-hospital death in Silesia, Poland. Pol. Arch. Intern. Med. 2021, 131, 339–344. [Google Scholar] [CrossRef]
- Nguyen, N.T.; Chinn, J.; De Ferrante, M.; Kirby, K.A.; Hohmann, S.F.; Amin, A. Male gender is a predictor of higher mortality in hospitalized adults with COVID-19. PLoS ONE 2021, 16, e0254066. [Google Scholar] [CrossRef]
- Wang, B.; Li, R.; Lu, Z.; Huang, Y. Does comorbidity increase the risk of patients with COVID-19: Evidence from meta-analysis. Aging 2020, 12, 6049–6057. [Google Scholar] [CrossRef] [PubMed]
- Castilla, J.; Guevara, M.; Miqueleiz, A.; Baigorria, F.; Ibero-Esparza, C.; Navascues, A.; Trobajo-Sanmartin, C.; Martinez-Baz, I.; Casado, I.; Burgui, C.; et al. Risk Factors of Infection, Hospitalization and Death from SARS-CoV-2: A Population-Based Cohort Study. J. Clin. Med. 2021, 10, 2608. [Google Scholar] [CrossRef] [PubMed]
- Turgutalp, K.; Ozturk, S.; Arici, M.; Eren, N.; Gorgulu, N.; Islam, M.; Uzun, S.; Sakaci, T.; Aydin, Z.; Sengul, E.; et al. Determinants of mortality in a large group of hemodialysis patients hospitalized for COVID-19. BMC Nephrol. 2021, 22, 29. [Google Scholar] [CrossRef]
- Haarhaus, M.; Santos, C.; Haase, M.; Mota Veiga, P.; Lucas, C.; Macario, F. Risk prediction of COVID-19 incidence and mortality in a large multi-national hemodialysis cohort: Implications for management of the pandemic in outpatient hemodialysis settings. Clin. Kidney J. 2021, 14, 805–813. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Tu, C.; Xiong, F.; Sun, X.; Tian, J.B.; Dong, J.W.; Wang, X.H.; Lei, C.T.; Liu, J.; Zhao, Z.; et al. Risk factors for the mortality of hemodialysis patients with COVID-19: A multicenter study from the overall hemodialysis population in Wuhan. Semin. Dial. 2021. [Google Scholar] [CrossRef]
- Scarpioni, R.; Manini, A.; Valsania, T.; De Amicis, S.; Albertazzi, V.; Melfa, L.; Ricardi, M.; Rocca, C. Covid-19 and its impact on nephropathic patients: The experience at Ospedale “Guglielmo da Saliceto” in Piacenza. G Ital. Nefrol. 2020, 37, 1–5. [Google Scholar]
- Zhang, X.M.; Jiao, J.; Cao, J.; Huo, X.P.; Zhu, C.; Wu, X.J.; Xie, X.H. Frailty as a predictor of mortality among patients with COVID-19: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 186. [Google Scholar] [CrossRef]
- Muscedere, J.; Waters, B.; Varambally, A.; Bagshaw, S.M.; Boyd, J.G.; Maslove, D.; Sibley, S.; Rockwood, K. The impact of frailty on intensive care unit outcomes: A systematic review and meta-analysis. Intensive Care Med. 2017, 43, 1105–1122. [Google Scholar] [CrossRef] [Green Version]
- Boakye, D.; Rillmann, B.; Walter, V.; Jansen, L.; Hoffmeister, M.; Brenner, H. Impact of comorbidity and frailty on prognosis in colorectal cancer patients: A systematic review and meta-analysis. Cancer Treat. Rev. 2018, 64, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Wang, L.; Ye, J.; Gu, Z.; Wang, S.; Xia, J.; Xie, Y.; Li, Q.; Xu, R.; Lin, N. Predictors of mortality in patients with coronavirus disease 2019: A systematic review and meta-analysis. BMC Infect Dis. 2021, 21, 663. [Google Scholar] [CrossRef] [PubMed]
- Tian, W.; Jiang, W.; Yao, J.; Nicholson, C.J.; Li, R.H.; Sigurslid, H.H.; Wooster, L.; Rotter, J.I.; Guo, X.; Malhotra, R. Predictors of mortality in hospitalized COVID-19 patients: A systematic review and meta-analysis. J. Med. Virol. 2020, 92, 1875–1883. [Google Scholar] [CrossRef]
- Kakkanattu, T.J.; Sankarasubbaiyan, S.; Yadav, A.K.; Kundu, M.; Gowda Bg, M.; Kumar, V.; Shah, K.; Jha, V. Outcome and Determinants of Outcome of COVID-19 Infection Among Hemodialysis Patients: Findings From a National Dialysis Network Program in India. Kidney Int. Rep. 2021, 6, 1429–1432. [Google Scholar] [CrossRef] [PubMed]
- Alberici, F.; Delbarba, E.; Manenti, C.; Econimo, L.; Valerio, F.; Pola, A.; Maffei, C.; Possenti, S.; Piva, S.; Latronico, N.; et al. Management of Patients on Dialysis and With Kidney Transplantation During the SARS-CoV-2 (COVID-19) Pandemic in Brescia, Italy. Kidney Int. Rep. 2020, 5, 580–585. [Google Scholar] [CrossRef]
- Connors, J.M.; Levy, J.H. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020, 135, 2033–2040. [Google Scholar] [CrossRef]
- Ray, J.G.; Schull, M.J.; Vermeulen, M.J.; Park, A.L. Association Between ABO and Rh Blood Groups and SARS-CoV-2 Infection or Severe COVID-19 Illness: A Population-Based Cohort Study. Ann. Intern. Med. 2021, 174, 308–315. [Google Scholar] [CrossRef]
- Kibler, M.; Dietrich, L.; Kanso, M.; Carmona, A.; Marchandot, B.; Matsushita, K.; Trimaille, A.; How-Choong, C.; Odier, A.; Gennesseaux, G.; et al. Risk and Severity of COVID-19 and ABO Blood Group in Transcatheter Aortic Valve Patients. J. Clin. Med. 2020, 9, 3796. [Google Scholar] [CrossRef]
- Dentali, F.; Sironi, A.P.; Ageno, W.; Turato, S.; Bonfanti, C.; Frattini, F.; Crestani, S.; Franchini, M. Non-O blood type is the commonest genetic risk factor for VTE: Results from a meta-analysis of the literature. Semin. Thromb. Hemost. 2012, 38, 535–548. [Google Scholar] [CrossRef]
- Campi, I.; Gennari, L.; Merlotti, D.; Mingiano, C.; Frosali, A.; Giovanelli, L.; Torlasco, C.; Pengo, M.F.; Heilbron, F.; Soranna, D.; et al. Vitamin D and COVID-19 severity and related mortality: A prospective study in Italy. BMC Infect. Dis. 2021, 21, 566. [Google Scholar] [CrossRef]
- Guven, M.; Gultekin, H. The effect of high-dose parenteral vitamin D3 on COVID-19-related inhospital mortality in critical COVID-19 patients during intensive care unit admission: An observational cohort study. Eur. J. Clin. Nutr. 2021, 75, 1383–1388. [Google Scholar] [CrossRef]
- Lakkireddy, M.; Gadiga, S.G.; Malathi, R.D.; Karra, M.L.; Raju, I.P.M.; Chinapaka, S.; Baba, K.S.; Kandakatla, M. Impact of daily high dose oral vitamin D therapy on the inflammatory markers in patients with COVID 19 disease. Sci. Rep. 2021, 11, 10641. [Google Scholar] [CrossRef]
- Stroehlein, J.K.; Wallqvist, J.; Iannizzi, C.; Mikolajewska, A.; Metzendorf, M.I.; Benstoem, C.; Meybohm, P.; Becker, M.; Skoetz, N.; Stegemann, M.; et al. Vitamin D supplementation for the treatment of COVID-19: A living systematic review. Cochrane Database Syst. Rev. 2021, 5, CD015043. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, D.C.; Winkelmayer, W.C. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int. Suppl. 2017, 7, 1–59. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; et al. 1-year outcomes in hospital survivors with COVID-19: A longitudinal cohort study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef]
- Wynants, L.; Van Calster, B.; Collins, G.S.; Riley, R.D.; Heinze, G.; Schuit, E.; Bonten, M.M.J.; Dahly, D.L.; Damen, J.A.A.; Debray, T.P.A.; et al. Prediction models for diagnosis and prognosis of covid-19: Systematic review and critical appraisal. BMJ 2020, 369, m1328. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | |
|---|---|
| n | 133 |
| Sex | |
| Male | 71 (53.38) |
| Female | 62 (46.62) |
| Age, years | 73.0 (67–79) |
| Body mass index, kg/m2 | 26.0 (22.0–29.0) |
| Dialysis vintages, months | 42.0 (17–86) |
| Dialysis dose per week, hours | 12 (12–12) |
| Past kidney transplantation | 11 (8.27) |
| Dialysis access | |
| AVF/AVG | 46 (34.59) |
| Dialysis catheter | 87 (65.41) |
| Comorbidities | |
| Diabetes | 73 (54.88) |
| Hypertension | 128 (96.24) |
| Chronic pulmonary disease | 12 (9.02) |
| Ischemic heart disease | 54 (40.60) |
| Congestive heart failure | 53 (39.85) |
| Malignancy | 15 (11.28) |
| Charlson comorbidity index (age adjusted) | 8 (6–10) |
| Frailty index | 4 (3–5) |
| COVID-19 severity on admission | |
| Asymptomatic | 34 (25.56) |
| Mild symptomatic | 63 (47.37) |
| Moderate requiring oxygen (<93%) | 36 (27.07) |
| Oxygen saturation on admission (SpO2), % | 94 (90–96) |
| Symptoms onset to hospital admission, days | 1 (0–3) |
| Hospitalization duration, days | 14.5 (9–20) |
| Died in the hospital | 44 (33.08) |
| Respiratory failure | 29 |
| Cardiovascular reasons | 9 |
| Co-infections | 4 |
| Thromboembolic complications | 1 |
| Hemorrhagic complications | 1 |
| Time from admission to hospital death, days | 8 (4–15) |
| Died during 3 months after discharge from hospital | 9 (6.8) |
| Sudden cardiac death at home | 9 (100) |
| Non survivors (died in the hospital or during 3 months) | 53 (39.08) |
| Variable | Survivors n = 80 | Non-Survivors n = 53 | p-Value |
|---|---|---|---|
| Sex | |||
| Male | 41 (51.25) | 30 (56.6) | p > 0.1 |
| Female | 39 (48.75) | 23 (43.4) | p > 0.1 |
| Age, years | 71.0 (61–77) | 75.00 (70–81) | p < 0.001 |
| Blood group: | |||
| A | 31(38.0) | 24/50 (48.0) | p > 0.1 |
| B | 13 (16.25) | 10/50 (20.0) | p > 0.1 |
| AB | 5 (6.25) | 5/50 (10.0) | p > 0.1 |
| 0 | 31 (38.75) | 11/50 (22.0) | p = 0.047 |
| Body mass index, kg/m2 | 26.0 (22.0–29.0) | 25.0 (22.0–29.0) | p > 0.1 |
| Dialysis vintages, months | 37.5 (17–90) | 47 (17–82) | p = 0.09 |
| Dialysis dose per week, hours | 12 (12–12) | 12 (12–12) | p > 0.1 |
| Past kidney transplantation | 7 (8.75) | 4 (7.55) | p > 0.1 |
| Comorbidities: | |||
| Diabetes | 42 (52.5) | 31 (53.0) | p > 0.1 |
| Hypertension | 77 (96.25) | 51 (96.25) | p > 0.1 |
| Chronic pulmonary disease | 4 (5.0) | 8 (15.09) | p = 0.046 |
| Ischemic heart disease | 29 (36.25) | 25 (47.17) | p > 0.1 |
| Congestive heart failure | 29 (36.25) | 24 (45.28) | p > 0.1 |
| Malignancy | 6 (7.5) | 9 (16.98) | p = 0.091 |
| Charlson comorbidity index | 7 (6–9) | 8 (7–10) | p = 0.023 |
| Clinical Frailty Scale (CFS) | 4 (3–5) | 5 (4–6) | p < 0.001 |
| Medications: | |||
| ACE inhibitors | 15 (18.75) | 11 (20.75) | p > 0.1 |
| ARBs | 8 (10) | 2 (3.77) | p > 0.1 |
| Calcium channel blockers | 25 (31.25) | 17 (32.07) | p > 0.1 |
| Beta-blockers | 59 (73.75) | 36 (67.9) | p > 0.1 |
| Statins | 37 (46.25) | 22 (41.51) | p > 0.1 |
| Oral anticoagulant | 6 (7.5) | 2 (3.77) | p > 0.1 |
| LMWH between dialysis days | 17 (21.25) | 15 (28.3) | p > 0.1 |
| Active oral vitamin D | 57 (71.25) | 28 (53) | p = 0.03 |
| Epoetin beta IU per week | 6000 (3500–6000) | 6000 (4000–9000) | p > 0.1 |
| Variable | Survivors n = 80 | Non-Survivors | p-Value |
|---|---|---|---|
| n = 53 | |||
| Symptoms: | |||
| Dyspnea | 23 (28.75) | 29 (54.72) | p = 0.003 |
| Fever >37.3 °C | 32 (40.0) | 21 (39.62) | p > 0.1 |
| Fatigue | 36 (45.0) | 21 (39.62) | p >0.1 |
| Chills | 13 (16.25) | 7 (13.21) | p > 0.1 |
| Cough | 25 (31.25) | 14 (26.41) | p > 0.1 |
| Decreased appetite | 4 (5.0) | 4 (7.55) | p > 0.1 |
| Diarrhea | 9 (11.25) | 4 (7.55) | p > 0.1 |
| Headache | 2 (2.5) | 3 (5.66) | p > 0.1 |
| Myalgia | 3 (3.75) | 1 (1.88) | p > 0.1 |
| Chest pain | 3 (3.75) | 1 (1.88) | p > 0.1 |
| Insomnia | 1 (1.25) | 1 (1.88) | p > 0.1 |
| Smell or taste disturbances | 4 (5.0) | 1 (1.88) | p > 0.1 |
| No symptoms | 24 (30.0) | 10 (18.87) | p = 0.15 |
| Symptoms onset to admission, days | 1 (0–3) | 1 (0–3) | p > 0.1 |
| COVID-19 disease severity: | |||
| Asymptomatic-Mild | 68 (85) | 31 (58.5) | p < 0.001 |
| Moderate-Severe | 12 (15) | 22 (41.5) | p < 0.001 |
| Findings at physical examination: | |||
| Heart rate, beats per min | 80 (73–90) | 84 (76–89) | p > 0.1 |
| Respiratory rate, breaths per min | 16 (15–17) | 15.5 (14–20) | p > 0.1 |
| Oxygen saturation, % | 95 (92–97) | 93 (86–96) | p = 0.005 |
| Systolic blood pressure, mmHg | 130 (122–152) | 132 (116–150) | p > 0.1 |
| Diastolic blood pressure, mmHg | 80 (70–90) | 75 (67–85) | p > 0.1 |
| Temperature °C | 36.7 (36.4–37) | 36.8 (36.5–37.45) | p > 0.1 |
| Laboratory findings: | |||
| White blood cell count, ×109/L | 5.12 (3.99–8.11) | 6.47 (4.71–9.08) | p = 0.05 |
| Lymphocyte count/mm3 | 0.92 (0.63–1.4) | 0.68 (0.56–0.98) | p = 0.08 |
| Hemoglobin, g/dL | 11.1 (10.0–11.6) | 10.7 (9.3–11.6) | p > 0.1 |
| Platelet count, ×109/L | 195.5 (149–239) | 171 (129–230) | p > 0.1 |
| CRP, mg/L | 34.5 (9.1–95.1) | 100.1 (38.1–174.4) | p < 0.001 |
| D-dimer, ng/mL | 1106.5 (724.9–1491.1) | 1695.66 (897.3–3793.2) | p = 0.004 |
| Procalcitonin, ng/mL | 0.35 (0.26–0.64) | 0.99 (0.69–4.22) | p > 0.1 |
| Ferritin, ng/mL | 1306 (777.9–1902.0) | 1262.5 (479.4–2145.0) | p > 0.1 |
| ALAT U/L | 20.5 (12–30) | 16 (12–28) | p > 0.1 |
| pO2, mmHg | 71.7 (54.2–87.6) | 63.2 (47.4–73.9) | p = 0.1 |
| pCO2, mmHg | 33.85 (28.6–36.9) | 34.75 (30.3–38.55) | p > 0.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tylicki, L.; Puchalska-Reglińska, E.; Tylicki, P.; Och, A.; Polewska, K.; Biedunkiewicz, B.; Parczewska, A.; Szabat, K.; Wolf, J.; Dębska-Ślizień, A. Predictors of Mortality in Hemodialyzed Patients after SARS-CoV-2 Infection. J. Clin. Med. 2022, 11, 285. https://doi.org/10.3390/jcm11020285
Tylicki L, Puchalska-Reglińska E, Tylicki P, Och A, Polewska K, Biedunkiewicz B, Parczewska A, Szabat K, Wolf J, Dębska-Ślizień A. Predictors of Mortality in Hemodialyzed Patients after SARS-CoV-2 Infection. Journal of Clinical Medicine. 2022; 11(2):285. https://doi.org/10.3390/jcm11020285
Chicago/Turabian StyleTylicki, Leszek, Ewelina Puchalska-Reglińska, Piotr Tylicki, Aleksander Och, Karolina Polewska, Bogdan Biedunkiewicz, Aleksandra Parczewska, Krzysztof Szabat, Jacek Wolf, and Alicja Dębska-Ślizień. 2022. "Predictors of Mortality in Hemodialyzed Patients after SARS-CoV-2 Infection" Journal of Clinical Medicine 11, no. 2: 285. https://doi.org/10.3390/jcm11020285