
The Role of Von Willebrand Factor in the Pathogenesis of Pulmonary Vascular Thrombosis in COVID-19

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
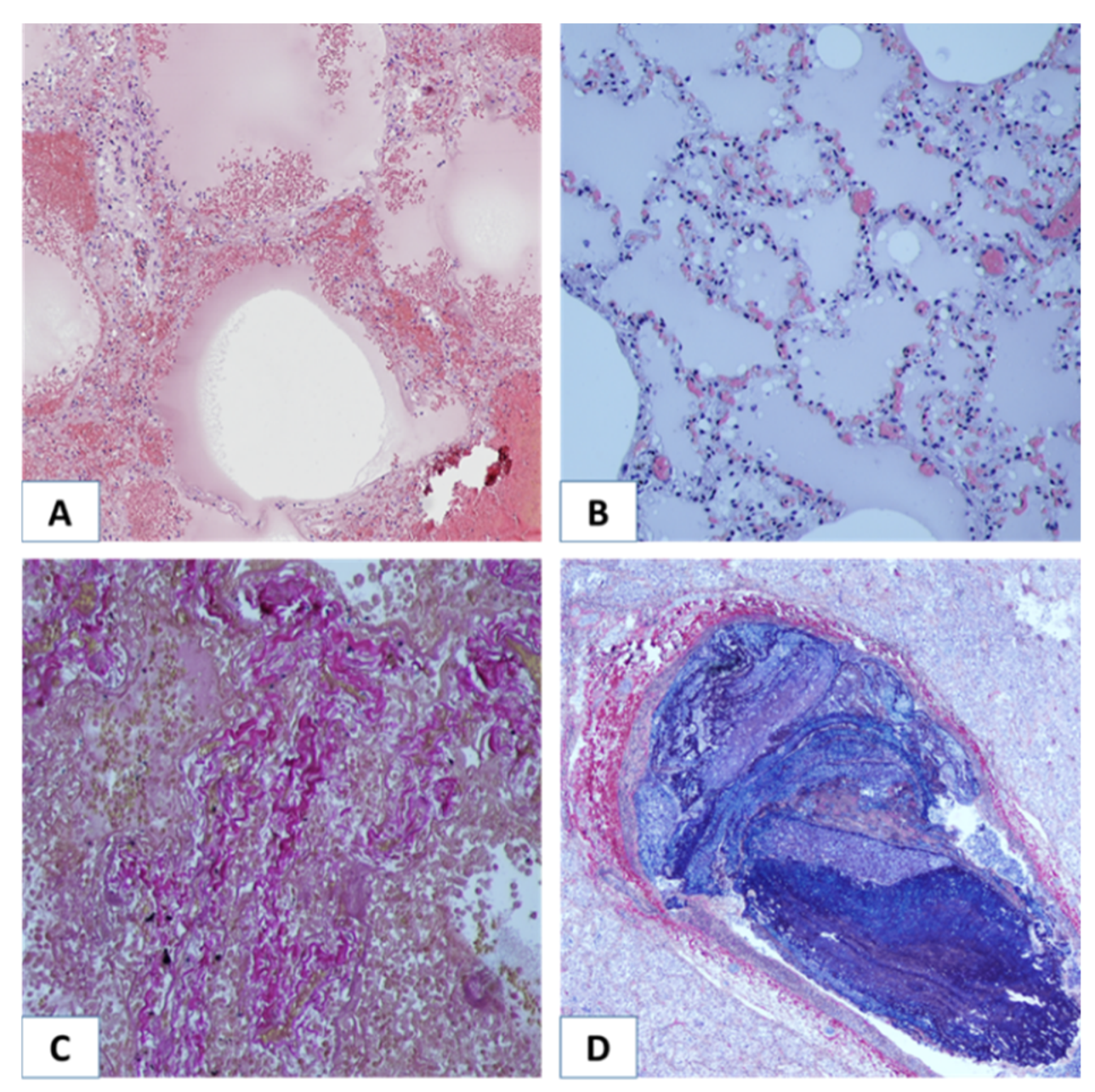
3.1. Morphological Study of the Lungs
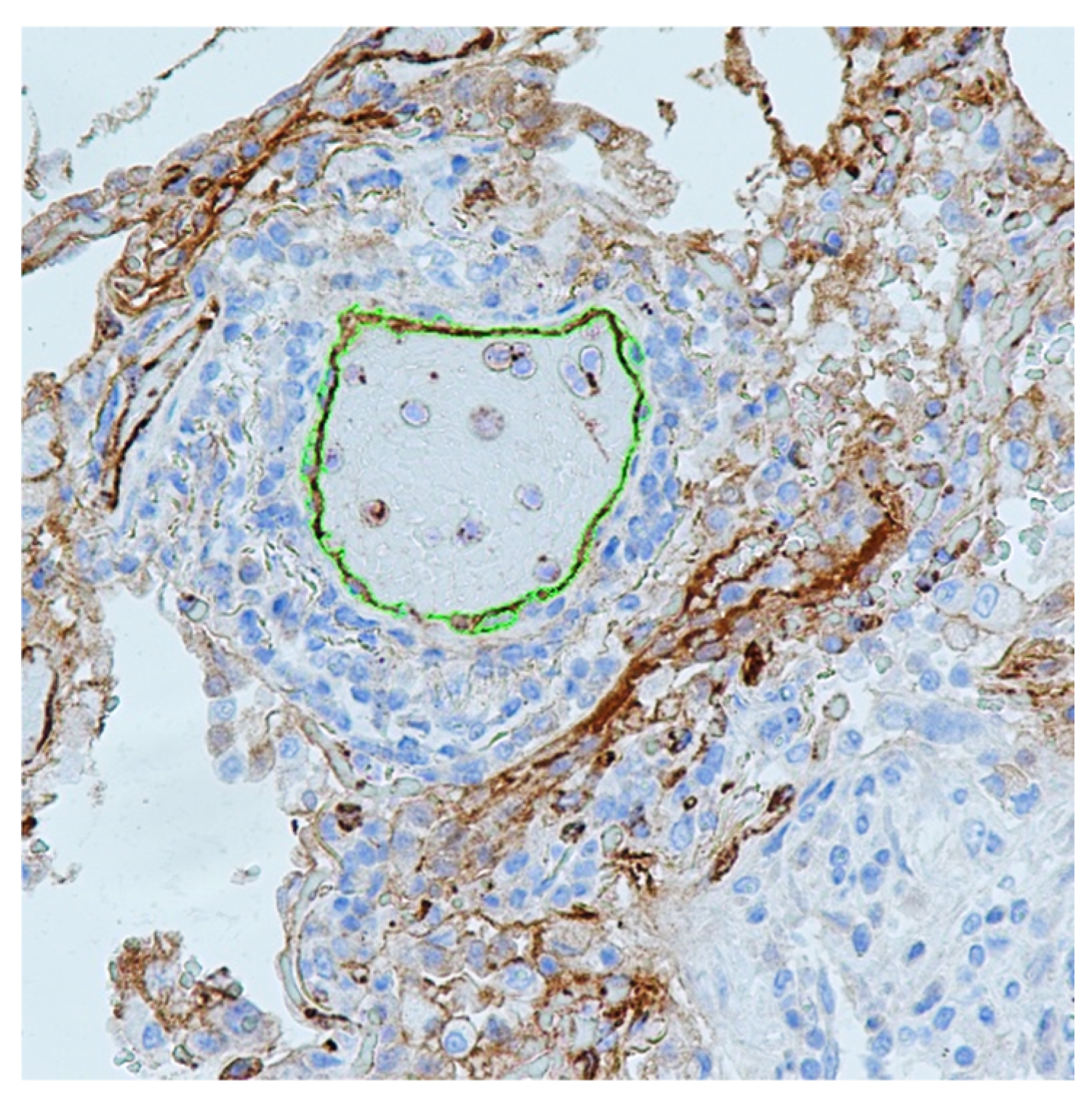
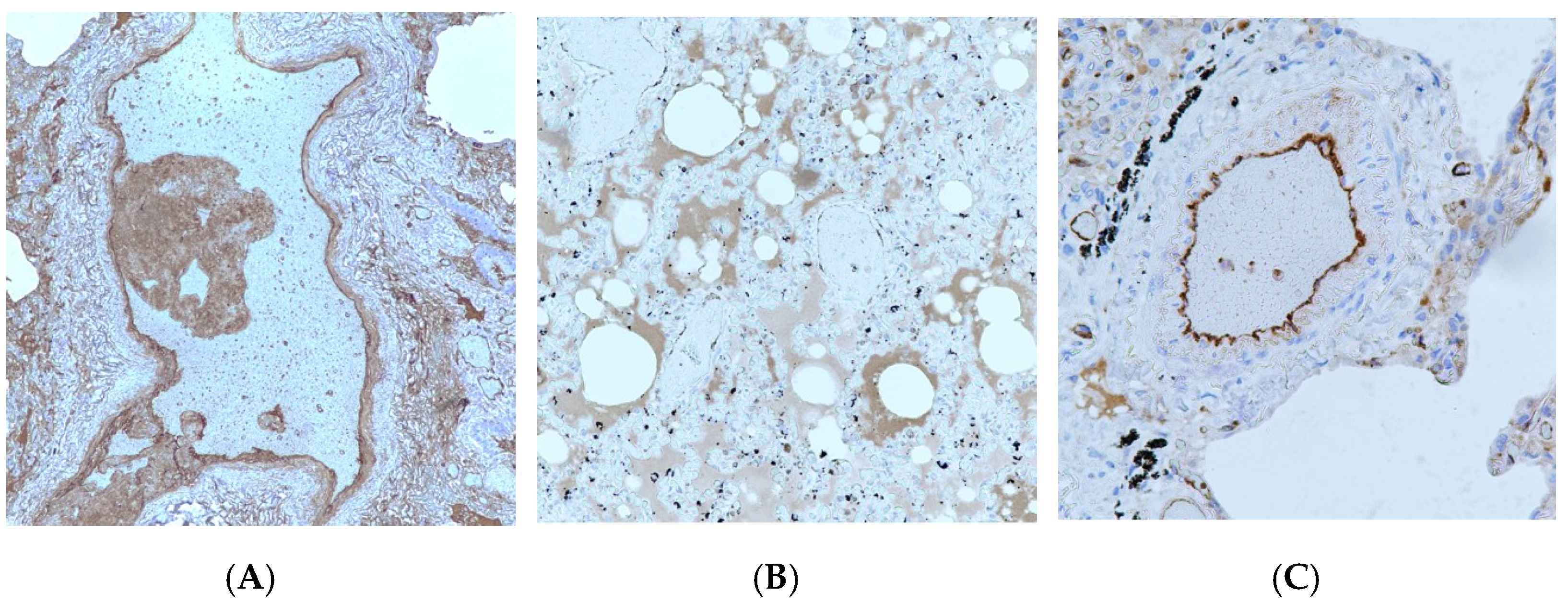
3.2. Immunohistochemistry Study of VWF in the Pulmonary Vascular Endothelium of COVID-19 Nonsuvivors
3.3. Analysis of Independent Factors Associated with an Increase in Von Willebrand Factor in Pulmonary Vascular Endothelium
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/publications/m/item/weekly-operational-updates-on-covid-19 (accessed on 11 January 2022).
- Hikmet, F.; Méar, L.; Edvinsson, Å.; Micke, P.; Uhlén, M.; Lindskog, C. The protein expression profile of ACE2 in human tissues. Mol. Syst. Biol. 2020, 16, e9610. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, J.; Gary, J.; Reagan-Steiner, S.; Estetter, L.B.; Tong, S.; Tao, Y.; Denison, A.M.; Lee, E.; DeLeon-Carnes, M.; Li, Y.; et al. Evidence of SARS-CoV-2 Replication and Tropism in the Lungs, Airways and Vascular Endothelium of Patients with Fatal COVID-19: An Autopsy Case-Series. J. Infect. Dis. 2021, 223, 752–764. [Google Scholar] [CrossRef] [PubMed]
- Hanff, T.C.; Mohareb, A.M.; Giri, J.; Cohen, J.B.; Chirinos, J.A. Thrombosis in COVID-19. Am. J. Hematol. 2020, 95, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Sisniega, D.C.; Reynolds, A.S. Severe Neurologic Complications of SARS-CoV-2. Curr. Treat. Options Neurol. 2021, 23, 14. [Google Scholar] [CrossRef] [PubMed]
- Guven, G.; Ince, C.; Topeli, A.; Caliskan, K. Cardio-Pulmonary-Renal Consequences of Severe COVID-19. Cardiorenal Med. 2021, 11, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Babkina, A.S.; Golubev, A.M.; Ostrova, I.V.; Volkov, A.V.; Kuzovlev, A.N. Brain Morphological Changes in COVID-19. Gen. Reanimatol. 2021, 17, 4–15. [Google Scholar] [CrossRef]
- Jacobs, J.L.; Bain, W.; Naqvi, A.; Staines, B.; Castanha, P.; Yang, H.; Boltz, V.F.; Barratt-Boyes, S.; Marques, E.T.; Mitchell, S.L.; et al. SARS-CoV-2 Viremia is Associated with COVID-19 Severity and Predicts Clinical Outcomes. Clin. Infect. Dis. 2021, in press. [Google Scholar] [CrossRef]
- Li, Y.; Schneider, A.M.; Mehta, A.; Sade-Feldman, M.; Kays, K.R.; Gentili, M.; Charland, N.C.; Gonye, A.L.; Gushterova, I.; Khanna, H.K.; et al. SARS-CoV-2 viremia is associated with distinct proteomic pathways and predicts COVID-19 outcomes. J. Clin. Investig. 2021, 131, e148635. [Google Scholar] [CrossRef]
- Klok, F.A.; Kruip, M.J.H.A.; Van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.A.M.P.J.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–147. [Google Scholar] [CrossRef]
- Katsaras, G.N.; Sokou, R.; Tsantes, A.G.; Konstantinidi, A.; Gialamprinou, D.; Piovani, D.; Bonovas, S.; Kriebardis, A.G.; Mitsiakos, G.; Kokoris, S.; et al. Thromboelastometry in Neonates with Respiratory Distress Syndrome: A Pilot Study. Diagnostics 2021, 11, 1995. [Google Scholar] [CrossRef]
- Oudkerk, M.; Büller, H.R.; Kuijpers, D.; van Es, N.; Oudkerk, S.F.; McLoud, T.; Gommers, D.; van Dissel, J.; Ten Cate, H.; van Beek, E.J. Diagnosis, prevention, and treatment of thromboembolic complications in COVID-19: Report of the national institute for public health of the Netherlands. Radiology 2020, 297, e216–e222. [Google Scholar] [CrossRef] [PubMed]
- Giannis, D.; Ziogas, I.A.; Gianni, P. Coagulation disorders in coronavirus infected patients: COVID-19, SARS-CoV-1, MERS-CoV and lessons from the past. J. Clin. Virol. 2020, 127, 104362. [Google Scholar] [CrossRef] [PubMed]
- Samsonova, M.V.; Chernyaev, A.L.; Omarova, Z.R.; Pershina, E.A.; Mishnev, O.D.; Zayratyants, O.V.; Mikhaleva, L.M.; Kalinin, D.V.; Varyasin, V.V.; Tishkevich10, O.A.; et al. Features of pathological anatomy of lungs at COVID-19. Pulmonologiya 2020, 30, 519–532. [Google Scholar] [CrossRef]
- Libby, P.; Lüscher, T. COVID-19 is, in the end, an endothelial disease. Eur. Heart J. 2020, 41, 3038–3044. [Google Scholar] [CrossRef]
- Spadaro, S.; Fogagnolo, A.; Campo, G.; Zucchetti, O.; Verri, M.; Ottaviani, I.; Tunstall, T.; Grasso, S.; Scaramuzzo, V.; Murgolo, F.; et al. Markers of endothelial and epithelial pulmonary injury in mechanically ventilated COVID-19 ICU patients. Crit. Care 2021, 25, 74. [Google Scholar] [CrossRef]
- Tojo, K.; Yamamoto, N.; Mihara, T.; Abe, M.; Goto, T. Distinct temporal characteristics of circulating alveolar epithelial and endothelial injury markers in ARDS with COVID-19. Crit. Care 2021, 25, 169. [Google Scholar] [CrossRef]
- Copin, M.C.; Parmentier, E.; Duburcq, T.; Poissy, J.; Mathieu, D. Lille COVID-19 ICU and Anatomopathology Group. Time to consider histologic pattern of lung injury to treat critically ill patients with COVID-19 infection. Intensive Care Med. 2020, 46, 1124–1126. [Google Scholar] [CrossRef] [Green Version]
- Pons, S.; Fodil, S.; Azoulay, E.; Zafrani, L. The vascular endothelium: The cornerstone of organ dysfunction in severe SARS-CoV-2 infection. Crit. Care 2020, 24, 353. [Google Scholar] [CrossRef]
- Nicosia, R.F.; Ligresti, G.; Caporarello, N.; Akilesh, S.; Ribatti, D. COVID-19 Vasculopathy: Mounting Evidence for an Indirect Mechanism of Endothelial Injury. Am. J. Pathol. 2021, 191, 1374–1384. [Google Scholar] [CrossRef]
- Philippe, A.; Chocron, R.; Gendron, N.; Bory, O.; Beauvais, A.; Peron, N.; Khider, L.; Guerin, C.L.; Goudot, G.; Levasseur, F.; et al. Letter in response to: Circulating von Willebrand factor and high molecular weight multimers as markers of endothelial injury predict COVID-19 in-hospital mortality. Angiogenesis 2021, 24, 413–415. [Google Scholar] [CrossRef]
- Ware, L.B.; Eisner, M.D.; Thompson, B.T.; Parsons, P.E.; Matthay, M.A. Significance of von Willebrand factor in septic and nonseptic patients with acute lung injury. Am. J. Respir. Crit. Care Med. 2004, 170, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Interim Guidelines “Prevention, Diagnosis and Treatment of New Coronavirus Infection (COVID-19)”. Version 9 (26.10.2020). Available online: https://static-0.minzdrav.gov.ru/system/attachments/attaches/000/052/548/original/%D0%9C%D0%A0_COVID-19_%28v.9%29.pdf (accessed on 11 January 2022). (In Russian)
- Goto, S. Role of von Willebrand factor for the onset of arterial thrombosis. Clin. Lab. 2001, 47, 327–334. [Google Scholar]
- Kim, D.A.; Ashworth, K.J.; Di Paola, J.; Ku, D.N. Platelet α-granules are required for occlusive high-shear-rate thrombosis. Blood Adv. 2020, 4, 3258–3267. [Google Scholar] [CrossRef]
- Franchini, M.; Lippi, G. Von Willebrand factor and thrombosis. Ann. Hematol. 2006, 85, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.L. ADAMTS13 and von Willebrand factor in thrombotic thrombocytopenic purpura. Annu. Rev. Med. 2015, 66, 211–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doevelaar, A.A.; Bachmann, M.; Hölzer, B.; Seibert, F.S.; Rohn, B.J.; Bauer, F.; Witzke, O.; Dittmer, U.; Bachmann, M.; Yilmaz, S.; et al. von Willebrand Factor Multimer Formation Contributes to Immunothrombosis in Coronavirus Disease 2019. Crit. Care Med. 2021, 49, e512–e520. [Google Scholar] [CrossRef]
- Pham, T.T.; Punsawad, C.; Glaharn, S.; De Meyer, S.F.; Viriyavejakul, P.; Van den Steen, P.E. Release of endothelial activation markers in lungs of patients with malaria-associated acute respiratory distress syndrome. Malar. J. 2019, 18, 395. [Google Scholar] [CrossRef]
- Favaloro, E.J.; Henry, B.M.; Lippi, G. Increased VWF and Decreased ADAMTS-13 in COVID-19: Creating a Milieu for (Micro)Thrombosis. Semin. Thromb. Hemost. 2021, 47, 400–418. [Google Scholar] [CrossRef]
- Philippe, A.; Chocron, R.; Gendron, N.; Bory, O.; Beauvais, A.; Peron, N.; Khider, L.; Guerin, C.L.; Goudot, G.; Levasseur, F.; et al. Circulating Von Willebrand factor and high molecular weight multimers as markers of endothelial injury predict COVID-19 in-hospital mortality. Angiogenesis 2021, 24, 505–517. [Google Scholar] [CrossRef]
- Tripodi, A.; Rossi, S.C.; Clerici, M.; Merati, G.; Scalambrino, E.; Mancini, I.; Baronciani, L.; Boscarino, M.; Monzani, V.; Peyvandi, F. Pro-coagulant imbalance in patients with community acquired pneumonia assessed on admission and one month after hospital discharge. Clin. Chem. Lab. Med. 2021, 59, 1699–1708. [Google Scholar] [CrossRef]
- Lüttge, M.; Fulde, M.; Talay, S.R.; Nerlich, A.; Rohde, M.; Preissner, K.T.; Hammerschmidt, S.; Steinert, M.; Mitchell, T.J.; Chhatwal, G.S.; et al. Streptococcus pneumoniae induces exocytosis of Weibel-Palade bodies in pulmonary endothelial cells. Cell Microbiol. 2012, 14, 210–225. [Google Scholar] [CrossRef] [PubMed]
- Golubev, A.M.; Moroz, V.V.; Lysenko, D.V.; Kuzovlev, A.N.; Ostapchenko, D.A. Artificial Ventilation-Induced Acute Lung Lesion: Experimental, Morphological Study. Gen. Reanimatol. 2006, 2, 8–12. [Google Scholar] [CrossRef] [Green Version]
- Cepkova, M.; Brady, S.; Sapru, A.; Matthay, M.A.; Church, G. Biological markers of lung injury before and after the institution of positive pressure ventilation in patients with acute lung injury. Crit. Care. 2006, 10, R126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ware, L.B.; Conner, E.R.; Matthay, M.A. von Willebrand factor antigen is an independent marker of poor outcome in patients with early acute lung injury. Crit. Care Med. 2001, 29, 2325–2331. [Google Scholar] [CrossRef] [PubMed]
- Yiming, M.T.; Lederer, D.J.; Sun, L.; Huertas, A.; Issekutz, A.C.; Bhattacharya, S. Platelets enhance endothelial adhesiveness in high tidal volume ventilation. Am. J. Respir. Cell Mol. Biol. 2008, 39, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Hegeman, M.A.; Hennus, M.P.; Heijnen, C.J.; Specht, P.A.; Lachmann, B.; Jansen, N.J.; van Vught, A.J.; Cobelens, P.M. Ventilator-induced endothelial activation and inflammation in the lung and distal organs. Crit. Care 2009, 13, R182. [Google Scholar] [CrossRef] [Green Version]
- Hwabejire, J.O.; Kaafarani, H.; Mashbari, H.; Misdraji, J.; Fagenholz, P.J.; Gartland, R.M.; Abraczinskas, D.R.; Mehta, R.S.; Paranjape, C.N.; Eng, G.; et al. Bowel Ischemia in COVID-19 Infection: One-Year Surgical Experience. Am. Surg. 2021, 87, 1893–1900. [Google Scholar] [CrossRef]
- Kondo, R.; Kawaguchi, N.; McConnell, M.J.; Sonzogni, A.; Licini, L.; Valle, C.; Bonaffini, P.A.; Sironi, S.; Alessio, M.G.; Previtali, G.; et al. Pathological characteristics of liver sinusoidal thrombosis in COVID-19 patients: A series of 43 cases. Hepatol. Res. Off. J. Jpn. Soc. Hepatol. 2021, 51, 1000–1006. [Google Scholar] [CrossRef]
- Katneni, U.K.; Alexaki, A.; Hunt, R.C.; Schiller, T.; DiCuccio, M.; Buehler, P.W.; Ibla, J.C.; Kimchi-Sarfaty, C. Coagulopathy and Thrombosis as a Result of Severe COVID-19 Infection: A Microvascular Focus. Thromb. Haemost. 2020, 120, 1668–1679. [Google Scholar] [CrossRef]
- Mojiri, A.; Nakhaii-Nejad, M.; Phan, W.L.; Kulak, S.; Radziwon-Balicka, A.; Jurasz, P.; Michelakis, E.; Jahroudi, N. Hypoxia results in upregulation and de novo activation of von Willebrand factor expression in lung endothelial cells. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1329–1338. [Google Scholar] [CrossRef] [Green Version]
- Valdivia-Mazeyra, M.F.; Salas, C.; Nieves-Alonso, J.M.; Martín-Fragueiro, L.; Bárcena, C.; Muñoz-Hernández, P.; Villar-Zarra, K.; Martín-López, J.; Ramasco-Rueda, F.; Fraga, J.; et al. Increased number of pulmonary megakaryocytes in COVID-19 patients with diffuse alveolar damage: An autopsy study with clinical correlation and review of the literature. Virchows Arch. Int. J. Pathol. 2021, 478, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Mandal, R.V.; Mark, E.J.; Kradin, R.L. Megakaryocytes and platelet homeostasis in diffuse alveolar damage. Exp. Mol. Pathol. 2007, 83, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Middleton, E.A.; Rondina, M.T.; Schwertz, H.; Zimmerman, G.A. Amicus or Adversary Revisited: Platelets in Acute Lung Injury and Acute Respiratory Distress Syndrome. Am. J. Respir. Cell Mol. Biol. 2018, 59, 18–35. [Google Scholar] [CrossRef] [PubMed]
- Samsonova, M.V.; Mikhalyova, L.M.; Zairatyants, O.V.; Varyasin, V.V.; Bykanova, A.V.; Mishnev, O.D.; Berezovsky, Y.; Tishkevitch, O.A.; Gomzikova, E.A.; Chernyayev, A.L.; et al. Lung pathology of COVID-19 in Moscow. Arkhiv Patol. 2020, 82, 32–40. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease Duration Less than 10 Days (n = 12) | Disease Duration More than 10 Days (n = 17) | p-Value (Fischer’s Exact Test) | ||
|---|---|---|---|---|
| Type of thrombotic complication | Pulmonary artery embolism | 25% (3) | 24% (4) | 0.9 |
| Pulmonary vascular thrombosis | 8% (1) | 41% (7) | 0.093 | |
| Parameter | Disease Duration Less than 10 Days | Disease Duration 10 Days and More | p-Value (Mann–Whitney U-Test) |
|---|---|---|---|
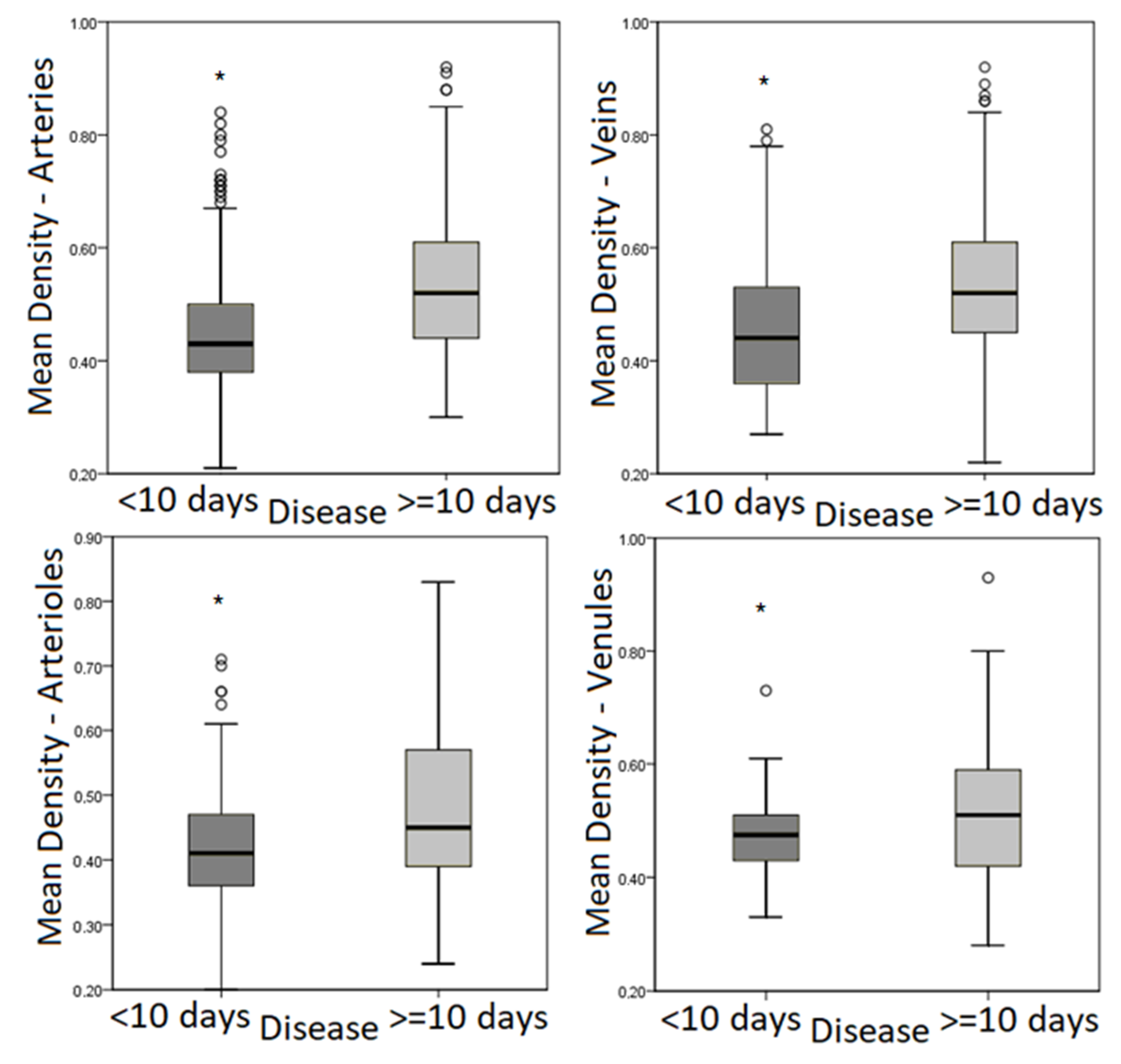
| Mean optical density in arteries | 0.43 (IQR, 0.38–0.50) | 0.52 (IQR, 0.44–0.61) | <0.001 * |
| Mean optical density in veins | 0.44 (IQR, 0.36–0.53) | 0.52 (IQR, 0.45–0.61) | <0.001 * |
| Mean optical density in arterioles | 0.41 (IQR, 0.36–0.47) | 0.45 (IQR, 0.39–0.57) | <0.001 * |
| Mean optical density in venules | 0.48 (IQR, 0.43–0.51) | 0.51 (IQR, 0.42–0.59) | 0.043 * |
| Parameter | Patients without Thrombotic Complications | Patients with Thrombotic Complications | p-Value (Mann–Whitney U-Test) |
|---|---|---|---|
| Mean optical density in arteries | 0.45 (IQR, 0.39–0.52) | 0.48 (IQR, 0.41–0.58) | <0.001 * |
| Mean optical density in veins | 0.46 (IQR, 0.39–0.56) | 0.52 (IQR, 0.45–0.61) | <0.001 * |
| Mean optical density in arterioles | 0.42 (IQR, 0.37–0.50) | 0.43 (IQR, 0.37–0.53) | 0.601 |
| Mean optical density in venules | 0.48 (IQR, 0.43–0.55) | 0.51 (IQR, 0.42–0.59) | 0.358 |
| Parameter | Patients with PE | Patients with Thrombosis | p-Value (Mann–Whitney U-Test) |
|---|---|---|---|
| Mean optical density in arteries | 0.46 (IQR, 0.39–0.53) | 0.52 (IQR, 0.43–0.60) | <0.001 * |
| Mean optical density in veins | 0.48 (IQR, 0.41–0.57) | 0.54 (IQR, 0.47–0.62) | <0.001 * |
| Mean optical density in arterioles | 0.40 (IQR, 0.35–0.47) | 0.54 (IQR, 0.44–0.62) | <0.001 * |
| Mean optical density in venules | 0.48 (IQR, 0.39–0.61) | 0.51 (IQR, 0.46–0.59) | 0.120 |
| Predictor | Adjusted Odds Ratio (Multivariable Analysis) | p-Value |
|---|---|---|
| Day 10 and more | 4.570 (95% CI, 3.416–6.114) | <0.001 * |
| Age 57 years and older | 0.790 (95% CI, 0.588–1.063) | 0.120 |
| Thrombotic complications | 2.519 (95% CI, 1.819–3.488) | <0.001 * |
| Ventilatory support | 0.381 (95% CI, 0.266–0.546) | <0.001 * |
| Bacterial pneumonia | 0.483 (95% CI, 0.361–0.647) | <0.001 * |
| Sex (female) | 1.299 (95% CI, 0.934–1.806) | 0.120 |
| Predictor | Adjusted Odds Ratio (Multivariable Analysis) | p-Value |
|---|---|---|
| Day 10 and more | 2.556 (95% CI, 1.781–3.669) | <0.001 * |
| Age 57 years and older | 1.132 (95% CI, 0.824–1.555) | 0.443 |
| Thrombotic complications | 1.544 (95% CI, 1.128–2.113) | 0.007 * |
| Ventilatory support | 1.062 (95% CI, 0.707–1.592) | 0.771 |
| Bacterial pneumonia | 0.854 (95% CI, 0.618–1.179) | 0.854 |
| Sex (female) | 3.102 (95% CI, 2.165–4.446) | <0.001 * |
| Predictor | Adjusted Odds Ratio (Multivariable Analysis) | p-Value |
|---|---|---|
| Day 10 and more | 4.188 (95% CI, 2.638–6.646) | <0.001 * |
| Age 57 years and older | 1.074 (95% CI, 0.741–1.556) | 0.706 |
| Thrombotic complications | 0.637 (95% CI, 0.423–0.958) | 0.030 * |
| Ventilatory support | 1.092 (95% CI, 0.701–1.699) | 0.697 |
| Bacterial pneumonia | 0.462 (95% CI, 0.299–0.713) | <0.001 * |
| Sex (female) | 1.433 (95% CI, 0.953–2.153) | 0.084 |
| Predictor | Adjusted Odds Ratio (Multivariable Analysis) | p-Value |
|---|---|---|
| Day 10 and more | 1.617 (95% CI, 0.907–2.880) | 0.103 |
| Age 57 years and older | 0.840 (95% CI, 0.453–1.558) | 0.581 |
| Thrombotic complications | 1.196 (95% CI, 0.652–2.194) | 0.563 |
| Ventilatory support | 1.153 (95% CI, 0.596–2.230) | 0.672 |
| Bacterial pneumonia | 3.287 (95% CI, 1.567–6.893) | 0.002 * |
| Sex (female) | 1.843 (95% CI, 1.065–3.190) | 0.029 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babkina, A.S.; Ostrova, I.V.; Yadgarov, M.Y.; Kuzovlev, A.N.; Grechko, A.V.; Volkov, A.V.; Golubev, A.M. The Role of Von Willebrand Factor in the Pathogenesis of Pulmonary Vascular Thrombosis in COVID-19. Viruses 2022, 14, 211. https://doi.org/10.3390/v14020211
Babkina AS, Ostrova IV, Yadgarov MY, Kuzovlev AN, Grechko AV, Volkov AV, Golubev AM. The Role of Von Willebrand Factor in the Pathogenesis of Pulmonary Vascular Thrombosis in COVID-19. Viruses. 2022; 14(2):211. https://doi.org/10.3390/v14020211
Chicago/Turabian StyleBabkina, Anastasiya S., Irina V. Ostrova, Mikhail Ya Yadgarov, Artem N. Kuzovlev, Andrey V. Grechko, Alexey V. Volkov, and Arkady M. Golubev. 2022. "The Role of Von Willebrand Factor in the Pathogenesis of Pulmonary Vascular Thrombosis in COVID-19" Viruses 14, no. 2: 211. https://doi.org/10.3390/v14020211