
Clinical Support through Telemedicine in Heart Failure Outpatients during the COVID-19 Pandemic Period: Results of a 12-Months Follow Up

 , ,
, ,
Abstract
:1. Introduction
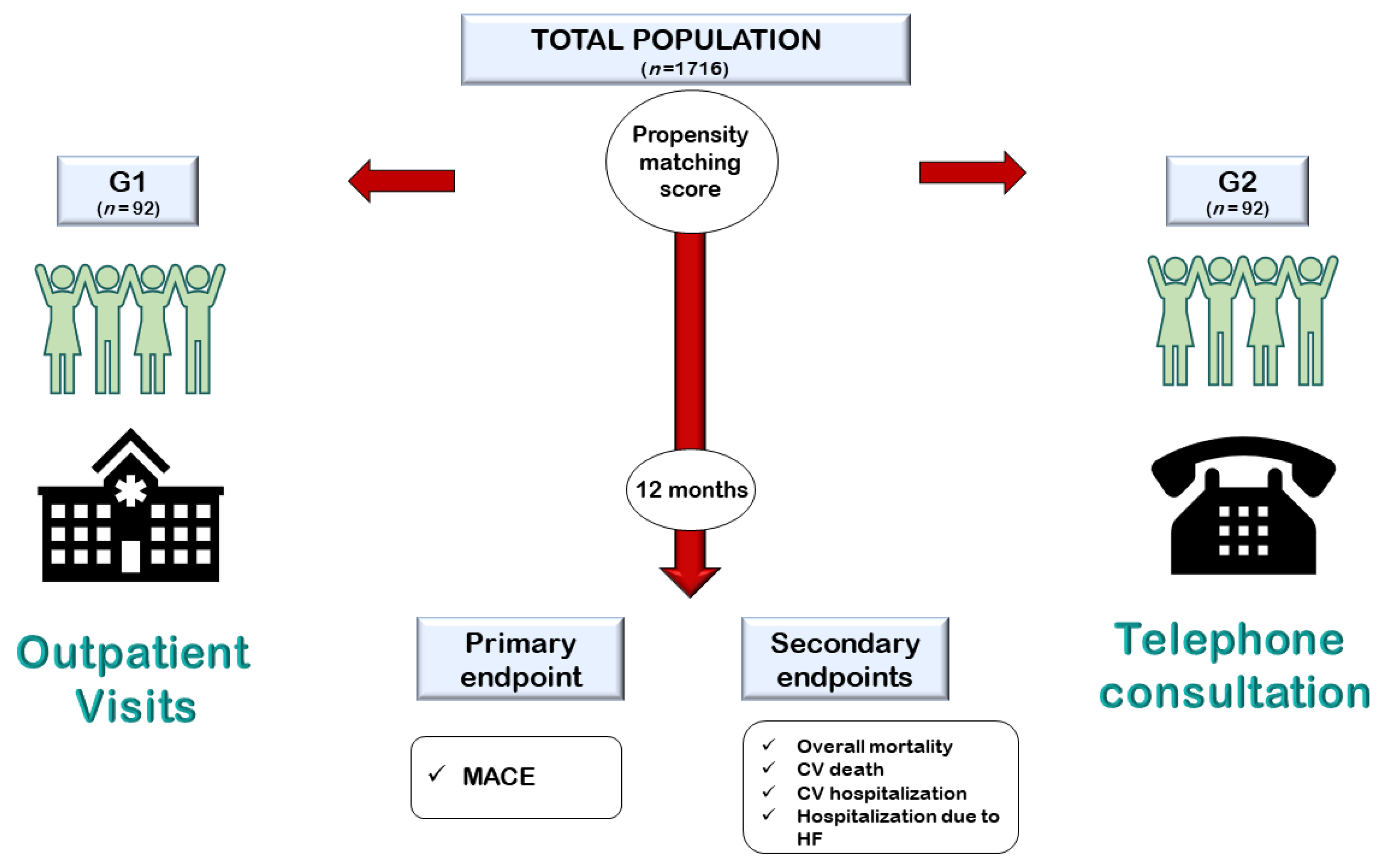
2. Methods
- Group 1 (G1): patients managed through traditional in-person visits.
- Group 2 (G2): patients managed through telephone consultations.
Statistical Analysis
3. Results
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar] [CrossRef] [PubMed]
- Pocock, S.J.; Ariti, C.A.; McMurray, J.J.; Maggioni, A.; Køber, L.; Squire, I.B.; Swedberg, K.; Dobson, J.; Poppe, K.K.; Whalley, G.A.; et al. Meta-Analysis Global Group in Chronic Heart Failure. Predicting survival in heart failure: A risk score based on 39 372 patients from 30 studies. Eur. Heart J. 2013, 34, 1404–1413. [Google Scholar] [CrossRef] [PubMed]
- Palazzuoli, A.; Evangelista, I.; Ruocco, G.; Lombardi, C.; Giovannini, V.; Nuti, R.; Ghio, S.; Ambrosio, G. Early readmission for heart failure: An avoidable or ineluctable debacle? Int. J. Cardiol. 2019, 277, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Severino, P.; D’Amato, A.; Prosperi, S.; Costi, B.; Angotti, D.; Birtolo, L.I.; Chimenti, C.; Lavalle, C.; Maestrini, V.; Mancone, M.; et al. Sodium-glucose cotransporter 2 inhibitors and heart failure: The best timing for the right patient. Heart Fail. Rev. 2021; Epub ahead of print. [Google Scholar] [CrossRef]
- DeVore, A.D.; Cox, M.; Eapen, Z.J.; Yancy, C.W.; Bhatt, D.L.; Heidenreich, P.A.; Peterson, E.D.; Fonarow, G.C.; Hernandez, A.F. Temporal Trends and Variation in Early Scheduled Follow-Up after a Hospitalization for Heart Failure: Findings from Get with the Guidelines-Heart Failure. Circ. Heart Fail. 2016, 9, e002344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Distelhorst, K.; Claussen, R.; Dion, K.; Bena, J.F.; Morrison, S.L.; Walker, D.; Tai, H.L.; Albert, N.M. Factors Associated with Adherence to 14-Day Office Appointments after Heart Failure Discharge. J. Card. Fail. 2018, 24, 407–411. [Google Scholar] [CrossRef]
- Zailinawati, A.H.; Ng, C.J.; Nik-Sherina, H. Why do patients with chronic illnesses fail to keep their appointments? A telephone interview. Asia Pac. J. Public Health 2006, 18, 10–15. [Google Scholar] [CrossRef]
- Severino, P.; D’Amato, A.; Saglietto, A.; D’Ascenzo, F.; Marini, C.; Schiavone, M.; Ghionzoli, N.; Pirrotta, F.; Troiano, F.; Cannillo, M.; et al. Reduction in heart failure hospitalization rate during coronavirus disease 19 pandemic outbreak. ESC Heart Fail. 2020, 7, 4182–4188. [Google Scholar] [CrossRef]
- Kubica, J.; Ostrowska, M.; Stolarek, W.; Kasprzak, M.; Grzelakowska, K.; Kryś, J.; Kubica, A.; Adamski, P.; Podhajski, P.; Navarese, E.P.; et al. Impact of COVID-19 pandemic on acute heart failure admissions and mortality: A multicentre study (COV-HF-SIRIO 6 study). ESC Heart Fail. 2021, 16, 721–728. [Google Scholar] [CrossRef]
- Hall, M.E.; Vaduganathan, M.; Khan, M.S.; Papadimitriou, L.; Long, R.C.; Hernandez, G.A.; Moore, C.K.; Lennep, B.W.; McMullan, M.R.; Butler, J. Reductions in Heart Failure Hospitalizations during the COVID-19 Pandemic. J. Card. Fail. 2020, 26, 462–463. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 15, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Reza, N.; DeFilippis, E.M.; Jessup, M. Secondary Impact of the COVID-19 Pandemic on Patients with HeartFailure. Circ. Heart Fail. 2020, 13, e007219. [Google Scholar] [CrossRef] [PubMed]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- Afonso Nogueira, M.; Ferreira, F.; Raposo, A.F.; Mónica, L.; Simões Dias, S.; Vasconcellos, R.; Proença, G. Impact of telemedicine on the management of heart failure patients during coronavirus disease 2019 pandemic. ESC Heart Fail. 2021, 8, 1150–1155. [Google Scholar] [CrossRef]
- Liu, P.P.; Blet, A.; Smyth, D.; Li, H. The Science Underlying COVID-19: Implications for the Cardiovascular System. Circulation 2020, 142, 68–78. [Google Scholar] [CrossRef] [Green Version]
- Palazzuoli, A.; Ruocco, G.; Tecson, K.M.; McCullough, P.A. Screening, detection, and management of heart failure in the SARS-CoV2 (COVID-19) pandemic. Heart Fail. Rev. 2021, 26, 973–979. [Google Scholar] [CrossRef]
- Palazzuoli, A.; Ruocco, G.; Gronda, E. Noncardiac comorbidity clustering in heart failure: An overlooked aspect with potential therapeutic door. Heart Fail. Rev. 2020, 8, 1–12. [Google Scholar] [CrossRef]
- Wu, J.; Mamas, M.A.; Mohamed, M.O.; Kwok, C.S.; Roebuck, C.; Humberstone, B.; Denwood, T.; Luescher, T.; de Belder, M.A.; Deanfield, J.E.; et al. Place and causes of acute cardiovascular mortality during the COVID-19 pandemic. Heart 2021, 107, 113–119. [Google Scholar] [CrossRef]
- Colivicchi, F.; Di Fusco, S.A.; Magnanti, M.; Cipriani, M.; Imperoli, G. The Impact of the Coronavirus Disease-2019 Pandemic and Italian Lockdown Measures on Clinical Presentation and Management of Acute Heart Failure. J. Card. Fail. 2020, 26, 464–465. [Google Scholar] [CrossRef]
- Andersson, C.; Gerds, T.; Fosbøl, E.; Phelps, M.; Andersen, J.; Lamberts, M.; Holt, A.; Butt, J.H.; Madelaire, C.; Gislason, G.; et al. Incidence of New-Onset and Worsening Heart Failure Before and after the COVID-19 Epidemic Lockdown in Denmark: A Nationwide Cohort Study. Circ. Heart Fail. 2020, 13, e007274. [Google Scholar] [CrossRef]
- Bollmann, A.; Hohenstein, S.; Meier-Hellmann, A.; Kuhlen, R.; Hindricks, G. Emergency hospital admissions and interventional treatments for heart failure and cardiac arrhythmias in Germany during the COVID-19 outbreak: Insights from the German-wide Helios hospital network. Eur. Heart J. Qual. Care Clin. Outcomes 2020, 6, 221–222. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.H.; Yuan, W.L.; Huang, T.C.; Zhang, H.F.; Mai, J.T.; Wang, J.F. Clinical effectiveness of telemedicine for chronic heart failure: A systematic review and meta-analysis. J. Investig. Med. 2017, 65, 899–911. [Google Scholar] [CrossRef] [PubMed]
- Salzano, A.; D’Assante, R.; Stagnaro, F.M.; Valente, V.; Crisci, G.; Giardino, F.; Arcopinto, M.; Bossone, E.; Marra, A.M.; Cittadini, A. Heart failure management during the COVID-19 outbreak in Italy: A telemedicine experience from a heart failure university tertiary referral centre. Eur. J. Heart Fail. 2020, 22, 1048–1050. [Google Scholar] [CrossRef]
- Sammour, Y.; Spertus, J.A.; Austin, B.A.; Magalski, A.; Gupta, S.K.; Shatla, I.; Dean, E.; Kennedy, K.F.; Jones, P.G.; Nassif, M.E.; et al. Outpatient Management of Heart Failure during the COVID-19 Pandemic after Adoption of a Telehealth Model. JACC Heart Fail. 2021, 9, 916–924. [Google Scholar] [CrossRef] [PubMed]
- Galinier, M.; Roubille, F.; Berdague, P.; Brierre, G.; Cantie, P.; Dary, P.; Ferradou, J.M.; Fondard, O.; Labarre, J.P.; Mansourati, J.; et al. OSICAT Investigators. Telemonitoring versus standard care in heart failure: A randomised multicentre trial. Eur. J. Heart Fail. 2020, 22, 985–994. [Google Scholar] [CrossRef]
- Wells, R.; Dionne-Odom, J.N.; Azuero, A.; Buck, H.; Ejem, D.; Burgio, K.L.; Stockdill, M.L.; Tucker, R.; Pamboukian, S.V.; Tallaj, J.; et al. Examining Adherence and Dose Effect of an Early Palliative Care Intervention for Advanced Heart Failure Patients. J. Pain Symptom Manag. 2021, 62, 471–481. [Google Scholar] [CrossRef]
- Visco, V.; Esposito, C.; Manzo, M.; Fiorentino, A.; Galasso, G.; Vecchione, C.; Ciccarelli, M. A Multistep Approach to Deal with Advanced Heart Failure: A Case Report on the Positive Effect of Cardiac Contractility Modulation Therapy on Pulmonary Pressure Measured by CardioMEMS. Front. Cardiovasc. Med. 2022, 9, 874433. [Google Scholar] [CrossRef]
- Cleland, J.G.F.; Clark, R.A.; Pellicori, P.; Inglis, S.C. Caring for people with heart failure and many other medical problems through and beyond the COVID-19 pandemic: The advantages of universal access to home telemonitoring. Eur. J. Heart Fail. 2020, 22, 995–998. [Google Scholar] [CrossRef]
- Piro, A.; Magnocavallo, M.; Della Rocca, D.G.; Neccia, M.; Manzi, G.; Mariani, M.V.; Straito, M.; Bernardini, A.; Severino, P.; Iannucci, G.; et al. Management of cardiac implantable electronic device follow-up in COVID-19 pandemic: Lessons learned during Italian lockdown. J. Cardiovasc. Electrophysiol. 2020, 31, 2814–2823. [Google Scholar] [CrossRef]
- Visco, V.; Ferruzzi, G.J.; Nicastro, F.; Virtuoso, N.; Carrizzo, A.; Galasso, G.; Vecchione, C.; Ciccarelli, M. Artificial Intelligence as a Business Partner in Cardiovascular Precision Medicine: An Emerging Approach for Disease Detection and Treatment Optimization. Curr. Med. Chem. 2021, 28, 6569–6590. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.; Hartshorne-Evans, N.; Redmond-Lyon, S.; Wilson, J.; Essa, H.; Gray, A.; Clayton, L.; Barton, C.; Ahmed, F.Z.; Cunnington, C.; et al. The impact of COVID-19 on the management of heart failure: A United Kingdom patient questionnaire study. ESC Heart Fail. 2021, 8, 1324–1332. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Coats, A.J.S.; Zheng, Z.; Adamo, M.; Ambrosio, G.; Anker, S.D.; Butler, J.; Xu, D.; Mao, J.; Khan, M.S.; et al. Management of heart failure patients with COVID-19: A joint position paper of the Chinese Heart Failure Association & National Heart Failure Committee and the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 941–956. [Google Scholar] [CrossRef] [PubMed]
- Orlando, J.F.; Beard, M.; Kumar, S. Systematic review of patient and caregivers’ satisfaction with telehealth videoconferencing as a mode of service delivery in managing patients’ health. PLoS ONE 2019, 14, e0221848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bui, A.L.; Fonarow, G.C. Home monitoring for heart failure management. J. Am. Coll. Cardiol. 2012, 59, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Dunlay, S.M.; Roger, V.L.; Redfield, M.M. Epidemiology of heart failure with preserved ejection fraction. Nat. Rev. Cardiol. 2017, 14, 591–602. [Google Scholar] [CrossRef]
- Severino, P.; D’Amato, A.; Prosperi, S.; Fanisio, F.; Birtolo, L.I.; Costi, B.; Netti, L.; Chimenti, C.; Lavalle, C.; Maestrini, V.; et al. Myocardial Tissue Characterization in Heart Failure with Preserved Ejection Fraction: From Histopathology and Cardiac Magnetic Resonance Findings to Therapeutic Targets. Int. J. Mol. Sci. 2021, 22, 7650. [Google Scholar] [CrossRef]
- Magnocavallo, M.; Bernardini, A.; Mariani, M.V.; Piro, A.; Marini, M.; Nicosia, A.; Adduci, C.; Rapacciuolo, A.; Saporito, D.; Grossi, S.; et al. Home delivery of the communicator for remote monitoring of cardiac implantable devices: A multicenter experience during the COVID-19 lockdown. Pacing Clin. Electrophysiol. 2021, 44, 995–1003. [Google Scholar] [CrossRef]
- Kędzierski, K.; Radziejewska, J.; Sławuta, A.; Wawrzyńska, M.; Arkowski, J. Telemedicine in Cardiology: Modern Technologies to Improve Cardiovascular Patients’ Outcomes—A Narrative Review. Medicina 2022, 58, 210. [Google Scholar] [CrossRef]
- Portnoy, J.M.; Waller, M.; De Lurgio, S.; Dinakar, C. Telemedicine is as effective as in-person visits for patients with asthma. Ann. Allergy Asthma Immunol. 2016, 117, 241–245. [Google Scholar] [CrossRef]
- Jeong, J.Y.; Jeon, J.H.; Bae, K.H.; Choi, Y.K.; Park, K.G.; Kim, J.G.; Won, K.C.; Cha, B.S.; Ahn, C.W.; Kim, D.W.; et al. Smart Care Based on Telemonitoring and Telemedicine for Type 2 Diabetes Care: Multi-Center Randomized Controlled Trial. Telemed. J. E-Health 2018, 24, 604–613. [Google Scholar] [CrossRef]
- Severino, P.; D’Amato, A.; Prosperi, S.; Dei Cas, A.; Mattioli, A.V.; Cevese, A.; Novo, G.; Prat, M.; Pedrinelli, R.; Raddino, R.; et al. Do the Current Guidelines for Heart Failure Diagnosis and Treatment Fit with Clinical Complexity? J. Clin. Med. 2022, 11, 857. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, A.S.; Hansen, L.; Sørensen, S.S.; Jensen, M.B.; Ehlers, L.H. Is telehealthcare for heart failure patients cost-effective? An economic evaluation alongside the Danish TeleCare North heart failure trial. BMJ Open 2020, 10, e031670. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Population n = 1716 | G1 n = 1624 | G2 n = 92 | p-Value | |
|---|---|---|---|---|
| Age (±SD) | 70.5 ± 12.9 | 70.4 ± 13 | 72.6 ± 11.5 | 0.11 |
| Female Gender, n (%) | 1149 (67) | 1118 (68.8) | 31 (33.7) | <0.001 |
| Arterial Hypertension, n (%) | 1380 (80.4) | 1308 (80.5) | 72 (78.3) | 0.59 |
| Diabetes mellitus, n (%) | 283 (16.5) | 255 (15.7) | 28 (30.4) | <0.001 |
| Dyslipidemia, n (%) | 935 (54.5) | 876 (53.9) | 59 (64.1) | 0.05 |
| Smoking habit, n (%) | 525 (30.6) | 472 (29.1) | 53 (57.6) | <0.001 |
| Familiarity for CVD, n (%) | 641 (37.4) | 594 (36.6) | 47 (51.1) | 0.01 |
| Creatinine Clearance, mL/min (±SD) | 68.9 ± 25.2 | 66.8 ± 25.4 | 68.5 ± 22.5 | 0.52 |
| LVEF, % (±SD) | 42 ± 12 | 42 ± 12 | 48 ± 10 | <0.001 |
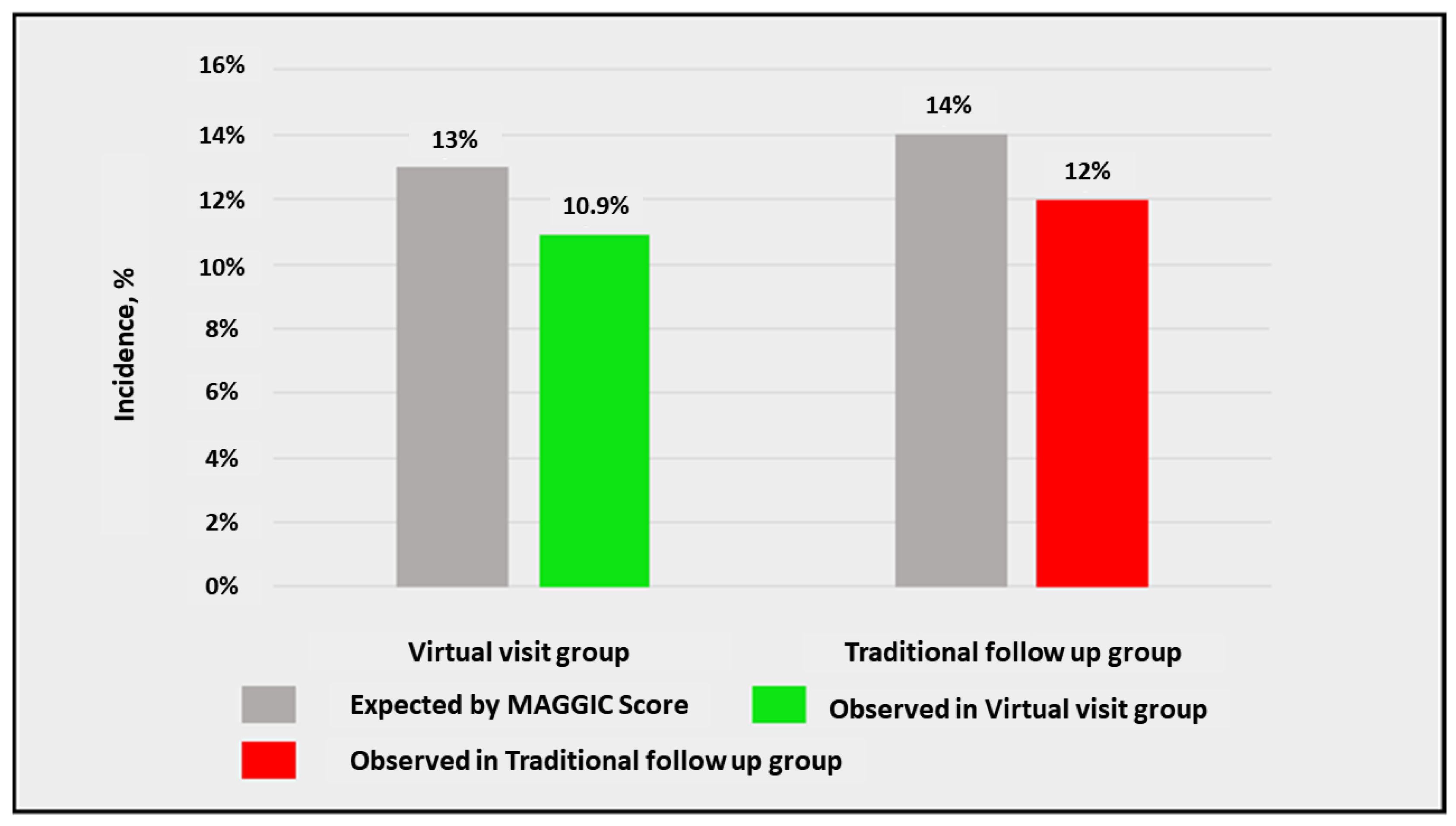
| MAGGIC Score | 21 ± 7 | 21 ± 7 | 20 ± 7.8 | 0.44 |
| G1 n = 92 | G2 n = 92 | p-Value | |
|---|---|---|---|
| Age (±SD) | 71.2 ± 13 | 72.6 ± 11.5 | 0.42 |
| Female Gender, n (%) | 27 (29.3) | 31 (33.7) | 0.53 |
| Arterial hypertension, n (%) | 73 (79.3) | 72 (78.3) | 0.85 |
| Diabetes mellitus, n (%) | 28 (30.4) | 28 (30.4) | 1 |
| Dyslipidemia, n (%) | 65 (70.7) | 59 (64.1) | 0.35 |
| Smoking habit, n (%) | 52 (56.5) | 53 (57.6) | 0.89 |
| Familiarity for CVD, n (%) | 47 (51.1) | 47 (51.1) | 1 |
| Creatinine Clearance, mL/min (±SD) | 66.6 ± 25.1 | 68.5 ± 22.5 | 0.60 |
| Ischemic HF etiology, n (%) | 46 (50) | 54 (59) | 0.30 |
| HFpEF, n (%) | 43 (47) | 48 (52) | 0.55 |
| HFmrEF, n (%) | 16 (17) | 15 (16) | 1 |
| HFrEF, n (%) | 33 (36) | 29 (32) | 0.64 |
| LV EDD, mm (±SD) | 53.3 ± 7.6 | 54 ± 6.6 | 0.5 |
| IVS, mm (±SD) | 11.35 ± 1.75 | 11.54 ± 1.72 | 0.46 |
| PW, mm (±SD) | 10.2 ±1.5 | 10 ± 1.36 | 0.34 |
| LVEF, % (±SD) | 47 ± 11 | 48 ± 10 | 0.76 |
| TAPSE, mm (±SD) | 18 ± 4 | 17 ± 4 | 0.09 |
| PAPs, mmHg (±SD) | 40 ± 11 | 37.5 ± 13 | 0.16 |
| E/e’ ratio (±SD) | 9 ± 2 | 9.5 ± 2.2 | 0.11 |
| BB, n (%) | 80 (87) | 74 (81) | 0.32 |
| ACE-i/ARBs, n (%) | 63 (68) | 66 (72) | 0.75 |
| ARNI, n (%) | 23 (25) | 13 (14) | 0.09 |
| MRAs, n (%) | 47 (51) | 52 (57) | 0.55 |
| Loop diuretics, n (%) | 64 (70) | 51 (55) | 0.07 |
| MAGGIC Score | 20 ± 7.2 | 20 ± 7.8 | 0.72 |
| Outcome | G1 n = 92 | G2 n = 92 | HR | 95% CI | p-Value |
|---|---|---|---|---|---|
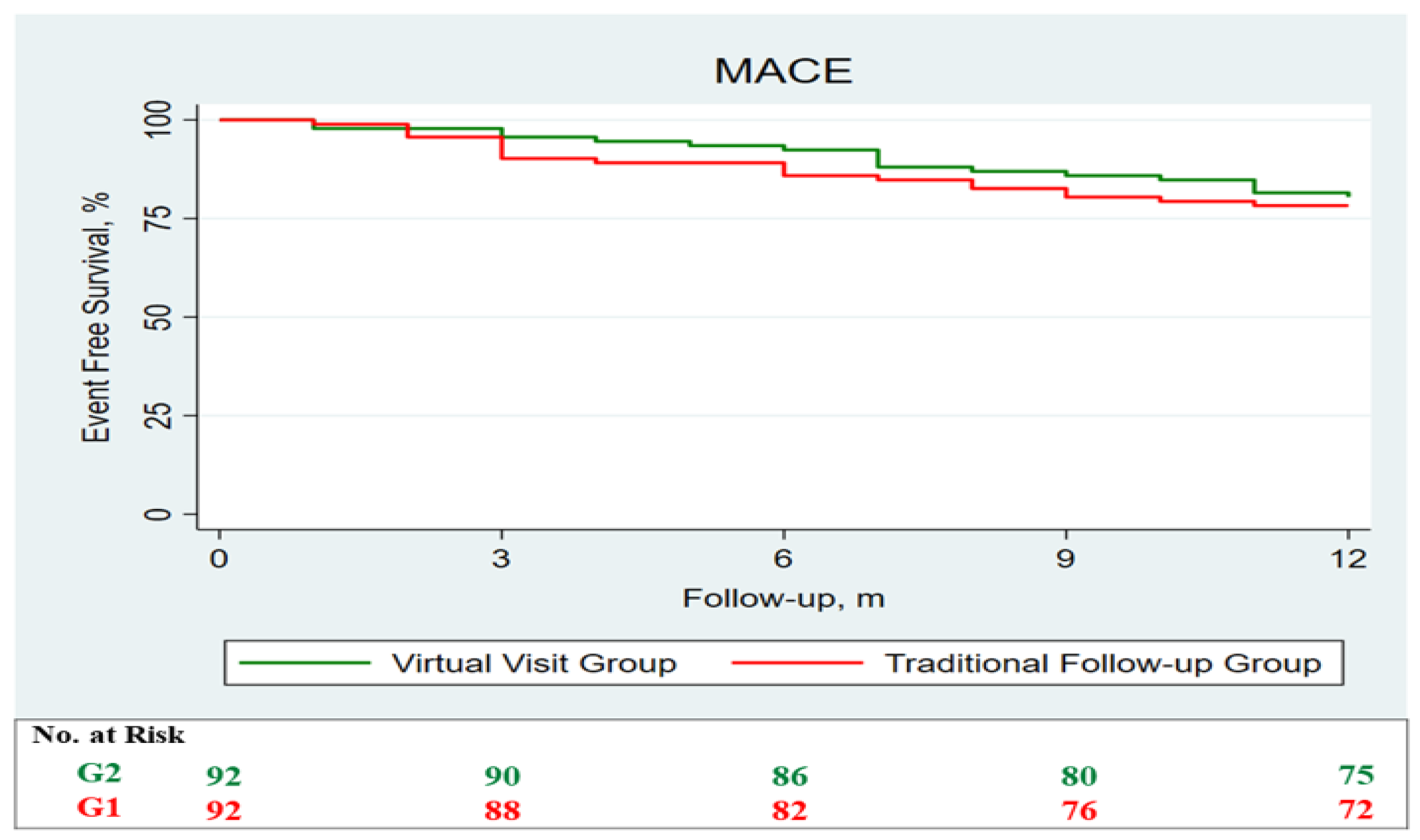
| MACE, n (%) | 20 (21.7) | 18 (19.7) | 1.15 | (0.61–2.19) | 0.65 |
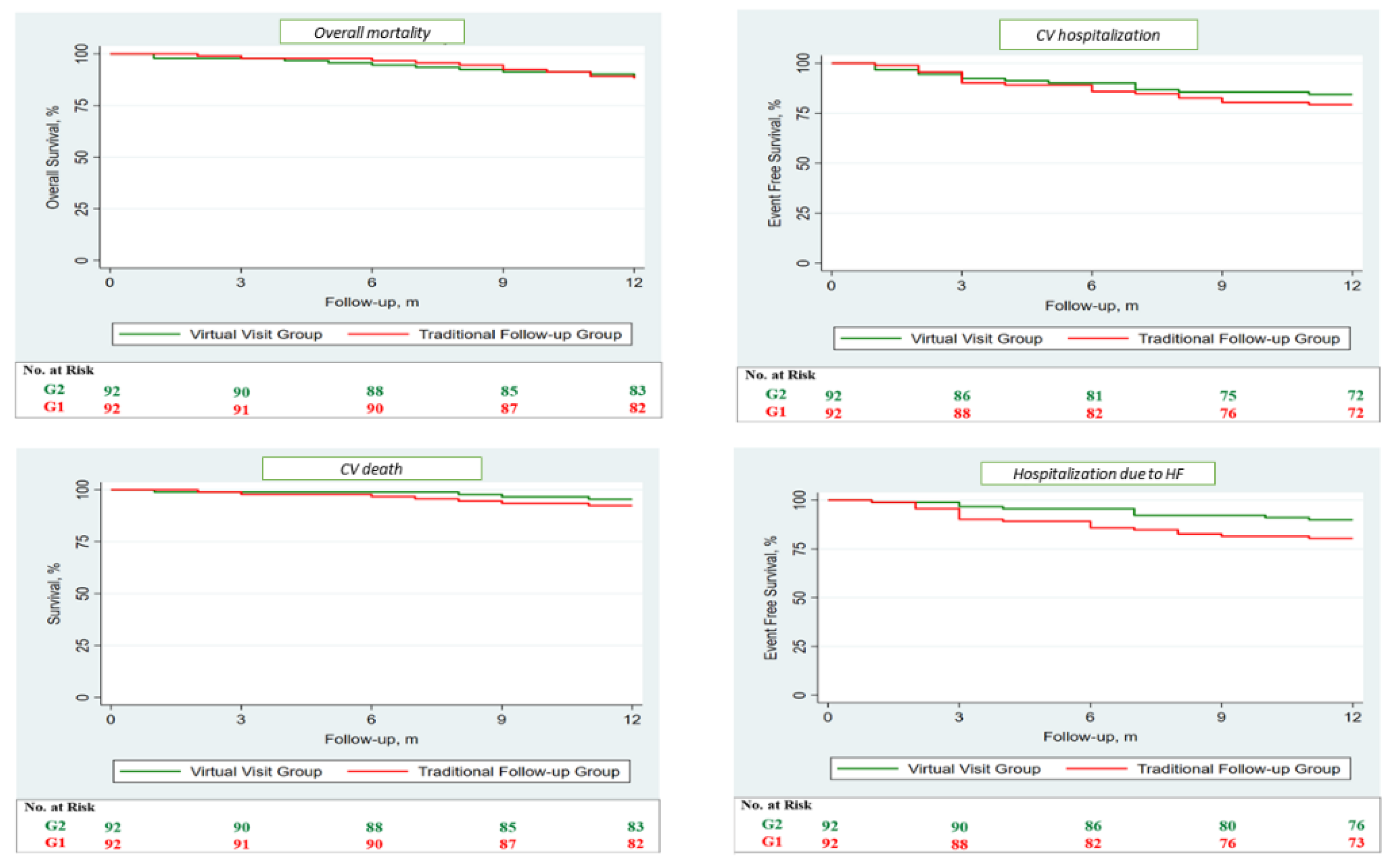
| Overall mortality, n (%) | 11 (12) | 10 (10.9) | 1.09 | (0.46–2.56) | 0.85 |
| CV death, n (%) | 7 (7.3) | 4 (4.3) | 1.72 | (0.50–5.89) | 0.39 |
| Stroke/TIA, n (%) | 1 (1.1) | 1 (1.1) | 0.99 | (0.06–15.90) | 1 |
| AMI, n (%) | 2 (2.2) | 3 (3.3) | 0.66 | (0.11–4.02) | 0.66 |
| CV Hospitalization, n (%) | 19 (20.7) | 14 (15.2) | 1.34 | (0.67–2.68) | 0.40 |
| Hospitalization due to HF, n (%) | 18 (19.6) | 9 (9.8) | 2.07 | (0.93–4.61) | 0.07 |
| Follow up, months (±SD) | 11.5 ± 1.7 | 11.3 ± 2.1 | 0.65 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Severino, P.; D’Amato, A.; Prosperi, S.; Magnocavallo, M.; Maraone, A.; Notari, C.; Papisca, I.; Mancone, M.; Fedele, F. Clinical Support through Telemedicine in Heart Failure Outpatients during the COVID-19 Pandemic Period: Results of a 12-Months Follow Up. J. Clin. Med. 2022, 11, 2790. https://doi.org/10.3390/jcm11102790
Severino P, D’Amato A, Prosperi S, Magnocavallo M, Maraone A, Notari C, Papisca I, Mancone M, Fedele F. Clinical Support through Telemedicine in Heart Failure Outpatients during the COVID-19 Pandemic Period: Results of a 12-Months Follow Up. Journal of Clinical Medicine. 2022; 11(10):2790. https://doi.org/10.3390/jcm11102790
Chicago/Turabian StyleSeverino, Paolo, Andrea D’Amato, Silvia Prosperi, Michele Magnocavallo, Annalisa Maraone, Claudia Notari, Ilaria Papisca, Massimo Mancone, and Francesco Fedele. 2022. "Clinical Support through Telemedicine in Heart Failure Outpatients during the COVID-19 Pandemic Period: Results of a 12-Months Follow Up" Journal of Clinical Medicine 11, no. 10: 2790. https://doi.org/10.3390/jcm11102790