
The Effects of Vitamin D Supplementation in COVID-19 Patients: A Systematic Review
 ,
,  and
and
Abstract
:1. Introduction
1.1. Background
1.2. Role of Vitamin D in SARS-CoV-2 Infection
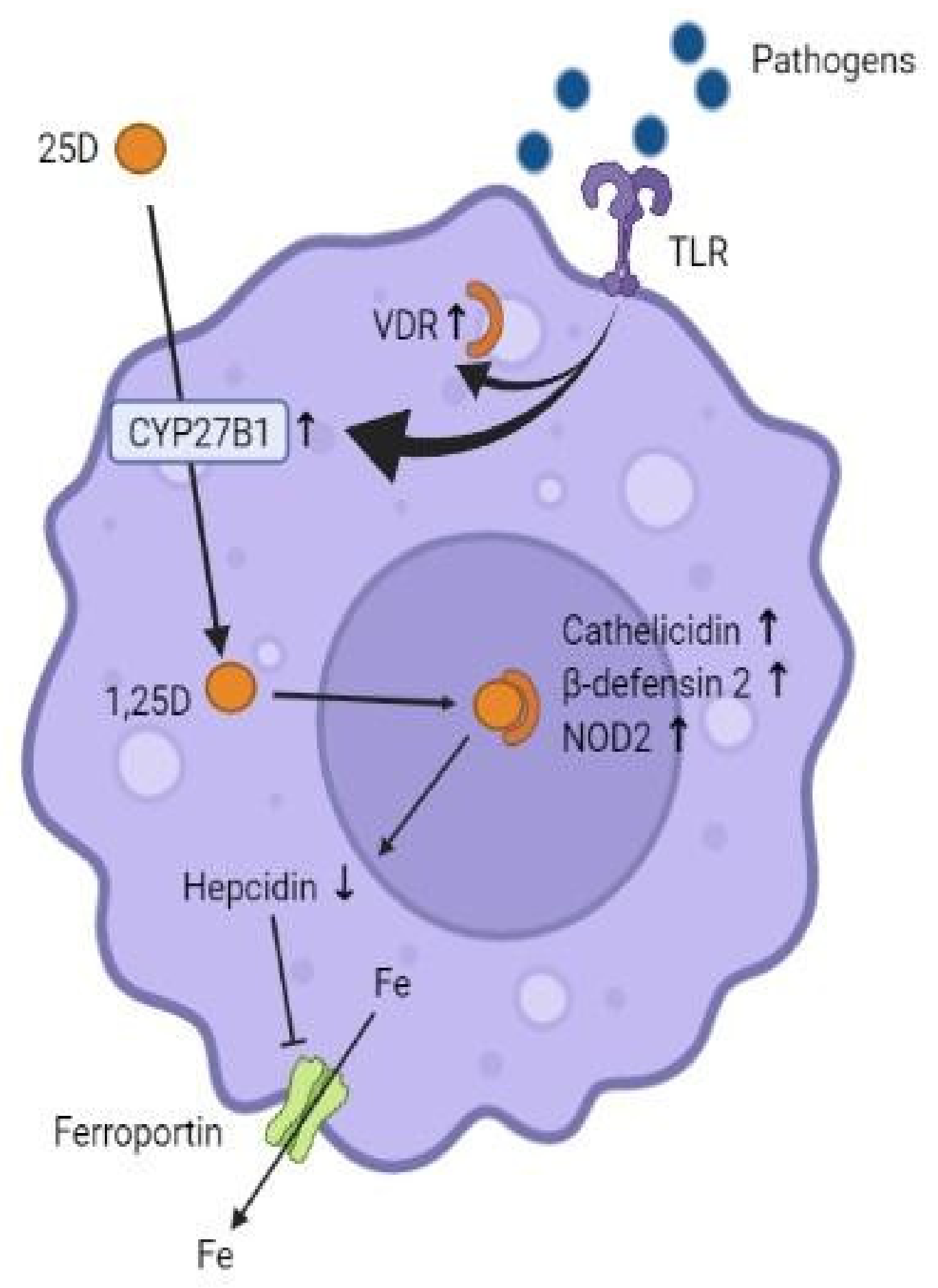
1.3. Mechanism of Action of Vitamin D with Regard to Its Immunomodulatory Role
1.4. Vitamin D Deficiency—A Risk Factor in COVID-19?
1.5. Justification and Aim
2. Methodology
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Aglipay, M.; Birken, C.S.; Parkin, P.C.; Loeb, M.B.; Thorpe, K.; Chen, Y.; Laupacis, A.; Mamdani, M.; MacArthur, C.; Hoch, J.S.; et al. Effect of High-Dose vs Standard-Dose Wintertime Vitamin D Supplementation on Viral Upper Respiratory Tract Infections in Young Healthy Children. JAMA 2017, 318, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Bergman, P.; Lindh, Å.U.; Björkhem-Bergman, L.; Lindh, J.D. Vitamin D and Respiratory Tract Infections: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2013, 8, e65835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martineau, A.R.; Forouhi, N.G. Vitamin D for COVID-19: A case to answer? Lancet Diabetes Endocrinol. 2020, 8, 735–736. [Google Scholar] [CrossRef]
- Charan, J.; Goyal, J.P.; Saxena, D.; Yadav, P. Vitamin D for prevention of respiratory tract infections: A systematic review and meta-analysis. J. Pharmacol. Pharmacother. 2012, 3, 300–303. [Google Scholar] [CrossRef] [Green Version]
- Pascual, A.L.C.; Torrejón, M.J. Vitamin D and its “non-classical” effects. Revista Española Salud Pública 2012, 83, 453–459. [Google Scholar]
- Sanz, J.M.; Gómez Lahoz, A.M.; Martín, R.O. Role of the immune system in SARS-CoV-2 infection: Immunopathology of COVID-19. Medicine 2021, 13, 1917–1931. [Google Scholar]
- Bilezikian, J.P.; Bikle, D.; Hewison, M.; Lazaretti-Castro, M.; Formenti, A.M.; Gupta, A.; Madhavan, M.V.; Nair, N.; Babalyan, V.; Hutchings, N.; et al. Mechanisms in Endocrinology: Vitamin D and COVID-19. Eur. J. Endocrinol. 2020, 183, R133–R147. [Google Scholar] [CrossRef]
- Baeke, F.; Takiishi, T.; Korf, H.; Gysemans, C.; Mathieu, C. Vitamin D: Modulator of the immune system. Curr. Opin. Pharmacol. 2010, 10, 482–496. [Google Scholar] [CrossRef]
- Ao, T.; Kikuta, J.; Ishii, M. The Effects of Vitamin D on Immune System and Inflammatory Diseases. Biomolecules 2021, 11, 1624. [Google Scholar] [CrossRef]
- Mao, J.; Lin, E.; He, L.; Yu, J.; Tan, P.; Zhou, Y. Autophagy and Viral Infection. Adv. Exp. Med. Biol. 2019, 1209, 55–78. [Google Scholar] [CrossRef]
- Pérez Castrillón, J.; Casado, E.; Corral Gudino, L.; Gómez Alonso, C.; Peris, P.; Riancho, J. COVID-19 and Vitamin D. Position paper of the Spanish Society for Bone and Mineral Metabolism Research (SEIOMM). Rev. Osteoporos. Metab. Miner. 2020, 12, 155–159. [Google Scholar] [CrossRef]
- Annweiler, C.; Beaudenon, M.; Gautier, J.; Simon, R.; Dubée, V.; Gonsard, J.; Parot-Schinkel, E.; Aidoud, A.; Albaret, G.; Audemard-Verger, A.; et al. COVID-19 and high-dose VITamin D supplementation TRIAL in high-risk older patients (COVIT-TRIAL): Study protocol for a randomized controlled trial. Trials 2020, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Peng, M.-Y.; Liu, W.-C.; Zheng, J.-Q.; Lu, C.-L.; Hou, Y.-C.; Zheng, C.-M.; Song, J.-Y.; Lu, K.-C.; Chao, Y.-C. Immunological Aspects of SARS-CoV-2 Infection and the Putative Beneficial Role of Vitamin-D. Int. J. Mol. Sci. 2021, 22, 5251. [Google Scholar] [CrossRef] [PubMed]
- Bergman, P. The link between vitamin D and COVID-19: Distinguishing facts from fiction. J. Intern. Med. 2020, 289, 131–133. [Google Scholar] [CrossRef] [PubMed]
- Maghbooli, Z.; Sahraian, M.A.; Ebrahimi, M.; Pazoki, M.; Kafan, S.; Tabriz, H.M.; Hadadi, A.; Montazeri, M.; Nasiri, M.; Shirvani, A.; et al. Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection. PLoS ONE 2020, 15, e0239799. [Google Scholar] [CrossRef]
- Carpagnano, G.E.; Di Lecce, V.; Quaranta, V.N.; Zito, A.; Buonamico, E.; Capozza, E.; Palumbo, A.; Di Gioia, G.; Valerio, V.N.; Resta, O. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J. Endocrinol. Investig. 2020, 44, 765–771. [Google Scholar] [CrossRef]
- Merzon, E.; Tworowski, D.; Gorohovski, A.; Vinker, S.; Cohen, A.G.; Green, I.; Frenkel-Morgenstern, M. Low plasma 25(OH) vitamin D level is associated with increased risk of COVID-19 infection: An Israeli population-based study. FEBS J. 2020, 287, 3693–3702. [Google Scholar] [CrossRef]
- De Smet, D.; De Smet, K.; Herroelen, P.; Gryspeerdt, S.; Martens, G.A. Serum 25(OH)D Level on Hospital Admission Associated With COVID-19 Stage and Mortality. Am. J. Clin. Pathol. 2020, 155, 381–388. [Google Scholar] [CrossRef]
- Jain, A.; Chaurasia, R.; Sengar, N.S.; Singh, M.; Mahor, S.; Narain, S. Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers. Sci. Rep. 2020, 10, 20191. [Google Scholar] [CrossRef]
- Panagiotou, G.; Tee, S.A.; Ihsan, Y.; Athar, W.; Marchitelli, G.; Kelly, D.; Boot, C.S.; Stock, N.; Macfarlane, J.; Martineau, A.R.; et al. Low serum 25-hydroxyvitamin D (25[OH]D) levels in patients hospitalised with COVID-19 are associated with greater disease severity: Results of a local audit of practice. Clin. Endocrinol. 2020, 93, 508–511. [Google Scholar] [CrossRef]
- Alsafar, H.; Grant, W.B.; Hijazi, R.; Uddin, M.; Alkaabi, N.; Tay, G.; Mahboub, B.; Al Anouti, F. COVID-19 disease severity and death in relation to vitamin D status among SARS-CoV-2-positive UAE residents. Nutrients 2021, 13, 1714. [Google Scholar] [CrossRef] [PubMed]
- Borsche, L.; Glauner, B.; von Mendel, J. COVID-19 Mortality Risk Correlates Inversely with Vitamin D3 Status, and a Mortality Rate Close to Zero Could Theoretically Be Achieved at 50 ng/mL 25(OH)D3: Results of a Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3596. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroehlein, J.K.; Wallqvist, J.; Iannizzi, C.; Mikolajewska, A.; Metzendorf, M.-I.; Benstoem, C.; Meybohm, P.; Becker, M.; Skoetz, N.; Stegemann, M.; et al. Vitamin D supplementation for the treatment of COVID-19: A living systematic review. Cochrane Database Syst. Rev. 2021, 2021, CD015043. [Google Scholar] [CrossRef]
- Vimaleswaran, K.S.; Forouhi, N.G.; Khunti, K. Vitamin D and covid-19. BMJ 2021, 372, n544. [Google Scholar] [CrossRef]
- Walsh, J.B.; McCartney, D.M.; Laird, É.; McCarroll, K.; Byrne, D.G.; Healy, M.; O’Shea, P.M.; Kenny, R.A.; Faul, J.L. Understanding a Low Vitamin D State in the Context of COVID-19. Front. Pharmacol. 2022, 13, 835480. [Google Scholar] [CrossRef]
- Saponaro, F.; Franzini, M.; Okoye, C.; Antognoli, R.; Campi, B.; Scalese, M.; Neri, T.; Carrozzi, L.; Monzani, F.; Zucchi, R.; et al. Is There a Crucial Link Between Vitamin D Status and Inflammatory Response in Patients With COVID-19? Front. Immunol. 2022, 12, 745713. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Urrútia, G.; Bonfilll, X. La declaración prisma: Un paso adelante en la mejora de las publicaciones de la revista Española de salud pública. Rev. Española Salud Pública 2013, 87, 99–102. [Google Scholar] [CrossRef] [Green Version]
- Caballero-García, A.; Pérez-Valdecantos, D.; Guallar, P.; Caballero-Castillo, A.; Roche, E.; Noriega, D.C.; Córdova, A. Effect of Vitamin D Supplementation on Muscle Status in Old Patients Recovering from COVID-19 Infection. Medicina 2021, 57, 1079. [Google Scholar] [CrossRef]
- Entrenas Castillo, M.E.; Entrenas Costa, L.M.E.; Vaquero Barrios, J.M.V.; Alcalá Díaz, J.F.A.; López Miranda, J.L.; Bouillon, R.; Quesada Gomez, J.M.Q. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef] [PubMed]
- Elamir, Y.M.; Amir, H.; Lim, S.; Rana, Y.P.; Lopez, C.G.; Feliciano, N.V.; Omar, A.; Grist, W.P.; Via, M.A. A randomized pilot study using calcitriol in hospitalized COVID-19 patients. Bone 2021, 154, 116175. [Google Scholar] [CrossRef] [PubMed]
- Cannata-Andía, J.B.; Díaz-Sottolano, A.; Fernández, P.; Palomo-Antequera, C.; Herrero-Puente, P.; Mouzo, R.; Carrillo-López, N.; Panizo, S.; Ibañez, G.H.; Cusumano, C.A.; et al. A single-oral bolus of 100,000 IU of cholecalciferol at hospital admission did not improve outcomes in the COVID-19 disease: The COVID-VIT-D—A randomised multicentre international clinical trial. BMC Med. 2022, 20, 83. [Google Scholar] [CrossRef] [PubMed]
- Murai, I.H.; Fernandes, A.L.; Sales, L.P.; Pinto, A.J.; Goessler, K.F.; Duran, C.S.C.; Silva, C.B.R.; Franco, A.S.; Macedo, M.B.; Dalmolin, H.H.H.; et al. Effect of a Single High Dose of Vitamin D3 on Hospital Length of Stay in Patients with Moderate to Severe COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, A.L.; Murai, I.H.; Reis, B.Z.; Sales, L.P.; Santos, M.D.; Pinto, A.J.; Goessler, K.F.; Duran, C.S.C.; Silva, C.B.R.; Franco, A.S.; et al. Effect of a single high dose of vitamin D3 on cytokines, chemokines, and growth factor in patients with moderate to severe COVID-19. Am. J. Clin. Nutr. 2022, 115, 790–798. [Google Scholar] [CrossRef]
- Murai, I.H.; Fernandes, A.L.; Antonangelo, L.; Gualano, B.; Pereira, R.M.R. Effect of a single high-dose vitamin D3 on the length of hospital stay of severely 25-hydroxyvita-min D-deficient patients with COVID-19. Clinics 2021, 76, 3549. [Google Scholar] [CrossRef]
- Pal, R.; Banerjee, M. Spurious undermining of the adjuvant role of vitamin D in COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102230. [Google Scholar] [CrossRef]
- Lakkireddy, M.; Gadiga, S.G.; Malathi, R.; Karra, M.L.; Raju, I.P.M.; Chinapaka, S.; Kss, S.B.; Kandakatla, M. Effect of Short Term High Dose Oral Vitamin D Therapy on the Inflammatory Markers in Patients with COVID 19 Disease. Arch. Clin. Biomed. Res. 2022, 6, 623–630. [Google Scholar] [CrossRef]
- Maghbooli, Z.; Sahraian, M.A.; Jamalimoghadamsiahkali, S.; Asadi, A.; Zarei, M.A.; Zendehdel, A.; Varzandi, T.; Mohammadnabi, S.; Alijani, N.; Karimi, M.; et al. Treatment With 25-Hydroxyvitamin D3 (Calcifediol) Is Associated With a Reduction in the Blood Neutrophil-to-Lymphocyte Ratio Marker of Disease Severity in Hospitalized Patients With COVID-19: A Pilot Multicenter, Randomized, Placebo-Controlled, Double-Blinded Clinical Trial. Endocr. Pract. 2021, 27, 1242–1251. [Google Scholar] [CrossRef]
- Huang, W.; Berube, J.; McNamara, M.; Saksena, S.; Hartman, M.; Arshad, T.; Bornheimer, S.J.; O’Gorman, M. Lymphocyte Subset Counts in COVID-19 Patients: A Meta-Analysis. Cytometry A 2020, 97, 772–776. [Google Scholar] [CrossRef]
- Rastogi, A.; Bhansali, A.; Khare, N.; Suri, V.; Yaddanapudi, N.; Sachdeva, N.; Puri, G.D.; Malhotra, P. Short term, high-dose vitamin D supplementation for COVID-19 disease: A randomised, placebo-controlled, study (SHADE study). Postgrad. Med. J. 2022, 98, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.R.; Abdelaziz, T.S.; Fathy, A. Impact of Vitamin D Therapy on the Progress COVID-19: Six Weeks Follow-Up Study of Vitamin D Deficient Elderly Diabetes Patients. Proc. Singap. Health 2021, 31, 20101058211041405. [Google Scholar] [CrossRef]
- Griffin, G.; Hewison, M.; Hopkin, J.; Kenny, R.A.; Quinton, R.; Rhodes, J.; Subramanian, S.; Thickett, D. Perspective: Vitamin D supplementation prevents rickets and acute respiratory infections when given as daily maintenance but not as intermittent bolus: Implications for COVID-19. Clin. Med. 2021, 21, e144–e149. [Google Scholar] [CrossRef] [PubMed]
- Villasis-Keever, M.A.; López-Alarcón, M.G.; Miranda-Novales, G.; Zurita-Cruz, J.N.; Barrada-Vázquez, A.S.; González-Ibarra, J.; Martínez-Reyes, M.; Grajales-Muñiz, C.; Santacruz-Tinoco, C.E.; Martínez-Miguel, B.; et al. Efficacy and Safety of Vitamin D Supplementation to Prevent COVID-19 in Frontline Healthcare Workers. A Randomized Clinical Trial. Arch. Med. Res. 2022, 53, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Ling, S.F.; Broad, E.; Murphy, R.; Pappachan, J.M.; Pardesi-Newton, S.; Kong, M.F.; Jude, E.B. High-Dose Cholecalciferol Booster Therapy is Associated with a Reduced Risk of Mortality in Patients with COVID-19: A Cross-Sectional Multi-Centre Observational Study. Nutrients 2020, 12, 3799. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PICO Algorithm | ||
|---|---|---|
| P | Patient | patient with active COVID-19, regardless of severity status and serum vitamin D level |
| I | Intervention | with vitamin D |
| C | Comparison | with or without placebo plus treatment as usual |
| O | Results | muscle status, need for ICU admission, mortality, length of hospitalisation, inflammatory markers, arterial O2 saturation |
| Sample | Methodology | Results | |
|---|---|---|---|
| Caballero-García et al., 2021 [28] | 30 healthy older male patients who suffered COVID-19 infection and no comorbidities Spain | Double blind study: I (n = 15): oral cholecalciferol (2000 IU/day) C (n = 15): placebo For 6 weeks from PCR+ 9 weeks | Respiratory function physical state: no statistically significant improvement ↓significant increase in circulating CK levels in I |
| Entrenas Castillo et al., 2020 [29] | 76 patients hospitalised for SARS-CoV-2 infection Spain | Electronic randomisation: I (n = 50): Oral calcifediol (days 1, 3, 7 and weekly until discharge) C (n = 26): usual treatment Data not available | Significant reduction in the need for ICU admission in the intervention group |
| Elamir et al., 2022 [30] | 50 patients hospitalised for SARS-CoV-2 infection USA | Open randomised trial: I (n = 25): calcitriol 0.5 µg daily for 14 days or until hospital discharge C (n = 25): usual treatment Data not available | Arterial oxygen saturation higher in I than in C at discharge compared to admission No significant changes in length of stay, ICU, endotracheal intubation, hospital readmission, or mortality |
| Cannata-Andía et al., 2022 [31] | 543 patients hospitalised for moderate to severe COVID-19 Multicentre international. Coordinated by Spain and carried out in 12 centres from four countries (Spain, Argentina, Guatemala and Chile) | Open randomised trial: I (n = 274): single dose of 100,000 IU of cholecalciferol on the first day of hospitalisation C (n = 269): usual treatment 1 year | No statistically significant differences in length of hospital stay, ICU admissions, or mortality ↑calcifediol levels (>25 ng/mL) at admission were associated with better evolution |
| Murai et al., 2021 [32] | 237 patients hospitalised for moderate to severe COVID-19 Multicentre, Brazil | Randomised double blind: I (n = 119): single dose of 200,000 IU of cholecalciferol C (n = 118): placebo 5 months | No significant reduction in length of hospital stay, mortality, ICU admission, or requirement or duration of mechanical ventilation, despite significantly higher calcifediol levels. ↑ in the I |
| Murai et al., 2022 [33] | 200 patients hospitalised for moderate to severe COVID-19 Brazil | Randomised double blind: I (n = 101): single dose of 200,000 IU of cholecalciferol C (n = 99): placebo 5 months | Does not improve the status of systemic pro-inflammatory cytokines, chemokines and growth factors |
| Murai et al., 2021 [34] | 32 patients with severe 25-OH cholecalciferol deficiency (<10 ng/mL) and moderate to severe COVID-19 disease Brazil | Randomised double blind: I (n = 16): single dose of 200,000 IU with cholecalciferol C (n = 16): placebo 5 months | No significant reduction in length of hospital stay, mortality, ICU admission, or requirement for mechanical ventilation despite significantly higher calcifediol levels. ↑ in the I |
| Lakkireddy et al., 2021 [36] | 87 patients with hypovitaminosis (vit. D <30 ng/mL) and mild to moderate COVID-19 disease India | Open randomised trial: I (n = 44): 60,000 IU of vitamin D orally daily for 8 or 10 days depending on BMI C (n = 43): usual treatment Data not available | Significant ↓ inflammatory markers of COVID-19 (INL, CRP, LDH, IL6, Ferritin) in I |
| Maghbooli et al., 2021 [37] | 106 patients with plasma levels of calcifediol <30 ng/mL and COVID-19 Iran | Randomised double blind: I (n = 53): 25 µg oral calcifediol daily C (n = 53): usual treatment 5 months | ↑ significant of the % lymphocyte and INL ↓ ↓ INL significantly associated with ↓ length of ICU stay and ↓ mortality |
| Rastogi et al., 2020 [39] | 40 patients with vitamin D deficiency (calcifediol <20 ng/mL) and asymptomatic or mildly symptomatic COVID-19 infection India | Randomised study: I (n = 16): 60,000 IU cholecalciferol orally for 7 days C (n = 24): placebo Data not available | ↑ 41.7% in the PCR negative on day 21 in I Significant ↓ of fibrinogen levels in I, without significant changes in D-dimer, procalcitonin and CRP |
| Soliman et al., 2021 [40] | 56 patients >60 years old with DM2 and vitamin D deficiency (<20 ng/mL) with COVID-19 Egypt | Randomised study: I (n = 40): single IM injection (200,000 IU) of cholecalciferol C (n = 16): single IM injection with placebo 2 months | No significant differences in mortality or in the need for intubation 6 weeks after diagnosis |
| Mean Serum Vitamin D Level after Supplementation (ng/mL) | |
|---|---|
| Cannata-Andía et al. [33] | 29.00 |
| Murai et al. [34] | 44.40 |
| Murai et al. [35] | 44.60 |
| Murai et al. [36] | 31.70 |
| Lakkireddy et al. [38] | 89.00 |
| Maghbooli et al. [39] | 59.60 |
| Rastogi et al. [41] | 51.70 |
| Soliman et al. [42] | 20.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feiner Solís, Á.; Avedillo Salas, A.; Luesma Bartolomé, M.J.; Santander Ballestín, S. The Effects of Vitamin D Supplementation in COVID-19 Patients: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 12424. https://doi.org/10.3390/ijms232012424
Feiner Solís Á, Avedillo Salas A, Luesma Bartolomé MJ, Santander Ballestín S. The Effects of Vitamin D Supplementation in COVID-19 Patients: A Systematic Review. International Journal of Molecular Sciences. 2022; 23(20):12424. https://doi.org/10.3390/ijms232012424
Chicago/Turabian StyleFeiner Solís, Ángela, Ana Avedillo Salas, María José Luesma Bartolomé, and Sonia Santander Ballestín. 2022. "The Effects of Vitamin D Supplementation in COVID-19 Patients: A Systematic Review" International Journal of Molecular Sciences 23, no. 20: 12424. https://doi.org/10.3390/ijms232012424