
“Stay-at-Home” Lifestyle Effect on Weight Gain during the COVID-19 Outbreak Confinement in China

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Survey Development and Content
2.2.1. Sociodemographic Information
2.2.2. Diet
- (1)
- Change of dietary intake before and during the epidemic, including 10 categories: total intake, staple foods, vegetables, dairies, legumes or products, livestock/poultry meats, fished or fishery products, eggs, fruits, snacks/beverages;
- (2)
- Six psychological emotions on dietary behavior before and during the epidemic: dysphoria, anxiety, sadness, nervous, loneliness, depression; and
- (3)
- Dietary restriction, overeating, and storing food behavior during the epidemic.
2.2.3. Physical Activity
- (1)
- Physical activity time, sedentary time, outdoor exercise time, and average daily steps before and during the epidemic;
- (2)
- Time spent using mobile phones and computers and doing housework during the epidemic; and
- (3)
- Weekly frequency of vigorous exercise and moderate exercise, as well as going out and walking during the epidemic.
2.2.4. Sleep
- (1)
- The time to go to bed, fall asleep, and get up; the length of sleep; the quality of sleep before and during the epidemic;
- (2)
- Factors affecting sleep during the epidemic: disturbance in respiration, cough or snore, feeling cold or hot, having a nightmare; pain or ache; and
- (3)
- Feeling sleepy and undynamic during the epidemic.
2.3. Statistical Analysis
3. Results
3.1. Changes in Food Intake, Physical Activity, and Sleep Compared to before the COVID-19 Outbreak
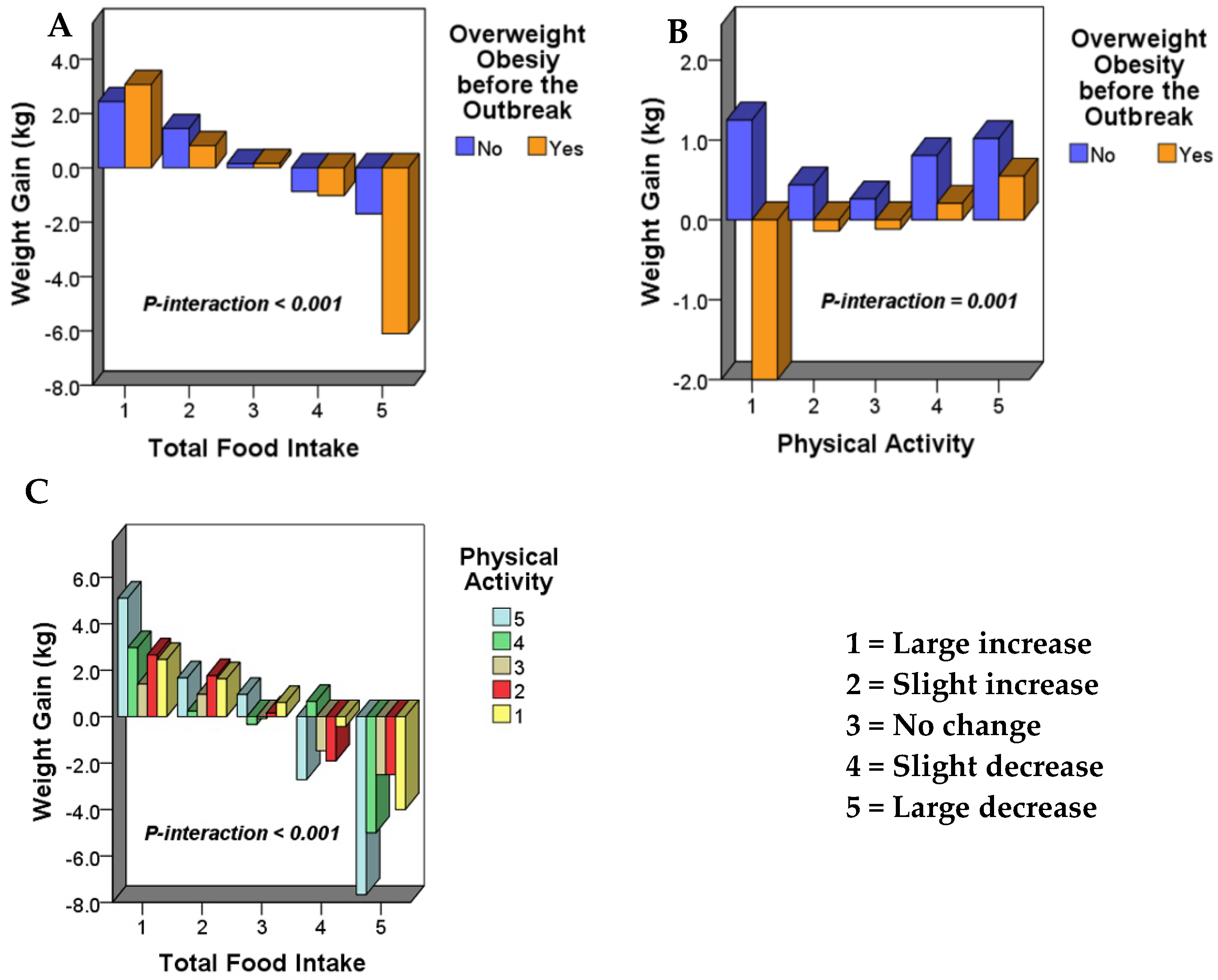
3.2. Analysis of Factors Affecting Weight Gain during the “Stay-at-Home” Lifestyle Caused by COVID-19 Outbreak
- (1)
- “Changes in total food intake * whether or not overweight/obesity before the outbreak” had a significant interaction effect on weight gain (p-interaction < 0.001) (Figure 1A).
- (2)
- “Changes in physical activity * whether or not overweight/obesity before the outbreak” had a significant interaction effect on weight gain (p-interaction = 0.001) (Figure 1B).
- (3)
- “Changes in total food intake * changes of physical activity” had a significant interaction effect on weight gain (p-interaction < 0.001) (Figure 1C).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Director-General’s Remarks at the Media Briefing on 2019-nCoV on 11 February 2020. 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020 (accessed on 11 April 2020).
- Guo, Y.-R.; Cao, Q.-D.; Hong, Z.-S.; Tan, Y.-Y.; Chen, S.-D.; Jin, H.-J.; Tan, K.-S.; Wang, D.-Y.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak—An update on the status. Mil. Med. Res. 2020, 7, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xinhua Net. The Wuhan Health and Fitness Commission Reported That Many Cases of Pneumonia Were Found to Be Viral Pneumonia and no Obvious Human-to-Human Transmission Was Found. Available online: http://www.hb.xinhuanet.com/2019-12/31/c_1125409171.htm (accessed on 9 April 2020).
- World Health Organization. Director-General’s Statement on IHR Emergency Committee on Novel Coronavirus (2019-nCoV). Available online: https://www.who.int/zh/dg/speeches/detail/who-director-general-s-statement-on-ihr-emergency-committee-on-novel-coronavirus-(2019-ncov) (accessed on 9 April 2020).
- World Health Organization. Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 28 June 2020).
- Han, Q.; Lin, Q.; Jin, S.; You, L. Coronavirus 2019-nCoV: A brief perspective from the front line. J. Infect. 2020, 80, 373–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellewell, J.; Abbott, S.; Gimma, A.; Bosse, N.I.; Jarvis, C.I.; Russell, T.W.; Munday, J.D.; Kucharski, A.J.; Edmunds, W.J.; Sun, F.; et al. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob. Health 2020, 8, e488–e496. [Google Scholar] [CrossRef] [Green Version]
- National Health Commission of the PRC. Notice Concerning the Issuance of the Recent Work Plan for the Prevention and Control of Pneumonia Caused by Novel Coronavirus. Available online: http://www.nhc.gov.cn/tigs/s7848/202001/808bbf75e5ce415aa19f74c78ddc653f.shtml (accessed on 9 April 2020).
- World Health Organization. Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV). Available online: https://www.who.int/zh/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 10 April 2020).
- Centers for Disease Control and Prevention. Interim Guidelines for the Prevention of Coronavirus Disease 2019 (COVID-19) in Households and Residential Communities. Available online: https://www.cdc.gov/coronavirus/2019-ncov/guidance-prevent-spread-chinese.html (accessed on 10 April 2020).
- Lau, H.; Khosrawipour, V.; Kocbach, P.; Mikolajczyk, A.; Schubert, J.; Bania, J.; Khosrawipour, T. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, C.R.; Sah, P.; Moghadas, S.M.; Pandey, A.; Shoukat, A.; Wang, Y.; Wang, Z.; Meyers, L.A.; Singer, B.H.; Galvani, A.P. Impact of international travel and border control measures on the global spread of the novel 2019 coronavirus outbreak. Proc. Natl. Acad. Sci. USA 2020, 117, 7504–7509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhutani, S.; Cooper, J.A. COVID-19–related home confinement in adults: Weight gain risks and opportunities. Obesity 2020, 28, 1576–1577. [Google Scholar] [CrossRef]
- Owen, N.; Sparling, P.B.; Healy, G.N.; Dunstan, D.W.; Matthews, C.E. Sedentary behavior: Emerging evidence for a new health risk. Mayo Clin. Proc. 2010, 85, 1138–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lippi, G.; Henry, B.M.; Bovo, C.; Sanchis-Gomar, F. Health risks and potential remedies during prolonged lockdowns for coronavirus disease 2019 (COVID-19). Diagnosis 2020, 7, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Changzheng, Y.; Manson, J.E.; Yuan, C.; Liang, M.H.; Grodstein, F.; Stampfer, M.J.; Willett, W.C.; Hu, F.B. Associations of weight gain from early to middle adulthood with major health outcomes later in life. JAMA 2017, 318, 255–272. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 1–15. [Google Scholar] [CrossRef]
- Zachary, Z.; Brianna, F.; Brianna, L.; Garrett, P.; Jade, W.; Alyssa, D.; Mikayla, K. Self-quarantine and weight gain related risk factors during the COVID-19 pandemic. Obes. Res. Clin. Pract. 2020, 14, 210–216. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary choices and habits during COVID-19 lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef] [PubMed]
- Ghosal, S.; Arora, B.; Dutta, K.; Ghosh, A.; Sinha, B.; Misra, A. Increase in the risk of type 2 diabetes during lockdown for the COVID19 pandemic in India: A cohort analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 949–952. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Simith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Hoare, E.; Milton, K.; Foster, C.; Allender, S. The associations between sedentary behaviour and mental health among adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearl, R.L. Weight Stigma and the “Quarantine-15”. Obesity 2020, 28, 1180–1181. [Google Scholar] [CrossRef]
- Sominsky, L.; Spencer, S.J. Eating behavior and stress: A pathway to obesity. Front. Psychol. 2014, 5, 434. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S. Central effects of stress hormones in health and disease: Understanding the protective and damaging effects of stress and stress mediators. Eur. J. Pharmacol. 2008, 583, 174–185. [Google Scholar] [CrossRef] [Green Version]
- Lupien, S.J.; McEwen, B.S.; Gunnar, M.R.; Heim, C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci. 2009, 10, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Santana, P.; Akana, S.F.; Hanson, E.S.; Strack, A.M.; Sebastian, R.J.; Dallman, M.F. Aldosterone and dexamethasone both stimulate energy acquisition whereas only the glucocorticoid alters energy storage. Endocrinology 1995, 136, 2214–2222. [Google Scholar] [CrossRef]
- Pecoraro, N.; Reyes, F.; Gomez, F.; Bhargava, A.; Dallman, M.F. Chronic stress promotes palatable feeding, which reduces signs of stress: Feedforward and feedback effects of chronic stress. Endocrinology 2004, 145, 3754–3762. [Google Scholar] [CrossRef] [PubMed]
- Foster, M.T.; Warne, J.P.; Ginsberg, A.B.; Horneman, H.F.; Pecoraro, N.C.; Akana, S.F.; Dallman, M.F. Palatable foods, stress, and energy stores sculpt corticotropin-releasing factor, adrenocorticotropin, and corticosterone concentrations after restraint. Endocrinology 2008, 150, 2325–2333. [Google Scholar] [CrossRef] [PubMed]
- Kaviani, S.; van Dellen, M.; Cooper, J.A. Daily self-weighing to prevent holiday-associated weight gain in adults. Obesity 2019, 27, 908–916. [Google Scholar] [CrossRef]
- Stevenson, J.L.; Krishnan, S.; Stoner, M.A.; Goktas, Z.E.Y.N.P.; Cooper, J.A. Effects of exercise during the holiday season on changes in body weight, body composition and blood pressure. Eur. J. Clin. Nutr. 2013, 67, 944–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhutani, S.; Wells, N.; Finlayson, G.; Schoeller, D.A. Change in eating pattern as a contributor to energy intake and weight gain during the winter holiday period in obese adults. Int. J. Obes. 2020, 44, 1586–1595. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.A.; Tokar, T. A prospective study on vacation weight gain in adults. Physiol. Behav. 2016, 156, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Schoeller, D.A. The effect of holiday weight gain on body weight. Physiol. Behav. 2014, 134, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.T.; Yuan, W.; Song, W.K. Changes in nutrition and health behavior in different age groups during COVID-19. J. Public Health Prev. Med. 2020, 31, 25–28. [Google Scholar]
- Nielsen. COVID-19: Tracking the Impact 2020. Available online: https://www.nielsen.com/us/en/ (accessed on 12 April 2020).
- Rodríguez-Pérez, C.; Molina-Montes, E.; Verardo, V.; Artacho, R.; García-Villanova, B.; Guerra-Hernández, E.J.; Ruíz-López, M.D. Changes in dietary behaviours during the COVID-19 outbreak confinement in the Spanish COVIDiet Study. Nutrients 2020, 12, 1730. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M.; Sanchis-Gomar, F. Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID-19). Eur. J. Prev. Cardiol. 2020, 27, 906–908. [Google Scholar] [CrossRef]
- Castrogiovanni, P.; Trovato, F.M.; Szychlinska, M.A.; Nsir, H.; Imbesi, R.; Musumeci, G. The importance of physical activity in osteoporosis. From the molecular pathways to the clinical evidence. Histol. Histopathol. 2016, 31, 1183–1194. [Google Scholar] [PubMed]
- Bhaskarabhatla, K.V.; Birrer, R. Physical activity and diabetes mellitus. Compr. Ther. 2005, 31, 291–298. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-Gomar, F. An Estimation of the worldwide epidemiologic burden of physical inactivity-related ischemic heart disease. Cardiovasc. Drugs Ther. 2020, 34, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Gomar, F.; Lucia, A.; Yvert, T.P.; Ruiz-Casado, A.; Pareja-Galeano, H.; Santos-Lozano, A.; Luces, M.D.C.F.; Garatachea, N.; Lippi, G.; Bouchard, C.; et al. Physical inactivity and low fitness deserve more attention to alter cancer risk and prognosis. Cancer Prev. Res. 2015, 8, 105–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J. The relationship between physical activity and dementia: A systematic review and meta-analysis of prospective cohort studies. J. Gerontol. Nurs. 2018, 44, 22–29. [Google Scholar] [CrossRef]
- Mok, A.; Khaw, K.-T.; Luben, R.; Wareham, N.; Brage, S. Physical activity trajectories and mortality: Population based cohort study. BMJ 2019, 365, l2323. [Google Scholar] [CrossRef] [Green Version]
- Djalalinia, S.; Qorbani, M.; Peykari, N.; Kelishadi, R. Health impacts of obesity. Pak. J. Med. Sci. 2015, 31, 239–242. [Google Scholar] [PubMed]
- He, L.; Gao, Y.; Gao, X.; Lei, X. Sleep patterns and physical and mental health of residents during coVID-19: Susceptibility factors and coping strategies. J. Southwest Univ. 2020, 42, 11–20. [Google Scholar]
- Moore, S.A.; Faulkner, G.; Rhodes, R.E.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.J.; Mitra, R.; O’Reilly, N.; Spence, J.C.; Vanderloo, L.M.; et al. Impact of the COVID-19 virus outbreak on movement and play behaviours of Canadian children and youth: A national survey. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–11. [Google Scholar] [CrossRef]


{kind=link}
| Large Increase | Slight Increase | No Change | Slight Decrease | Large Decrease | |
| Total food intake | 87 (9.8) | 260 (29.2) | 428 (48.1) | 96 (10.8) | 18 (2.0) |
| Snacks and drinks intake | 104 (11.7) | 263 (29.6) | 378 (42.5) | 65 (7.3) | 79 (8.9) |
| Fruits intake | 84 (9.4) | 303 (34.1) | 385 (43.3) | 86 (9.7) | 31 (3.5) |
| Vegetable intake | 81 (9.1) | 228 (25.6) | 502 (56.5) | 63 (7.1) | 15 (1.7) |
| Eggs intake | 75 (8.4) | 275 (30.9) | 494 (55.6) | 34 (3.8) | 11 (1.2) |
| Livestock/poultry meat intake | 66 (7.4) | 280 (31.5) | 418 (47.0) | 88 (9.9) | 37 (4.2) |
| Dairy intake | 62 (7.0) | 191 (21.5) | 497 (55.9) | 91 (10.2) | 48 (5.4) |
| Staple food intake | 60 (6.7) | 175 (19.7) | 531 (59.7) | 97 (10.9) | 26 (2.9) |
| Aquatic products intake | 48 (5.4) | 266 (29.9) | 441 (49.6) | 85 (9.6) | 49 (5.5) |
| Legumes intake | 36 (4.0) | 250 (28.1) | 526 (59.2) | 55 (6.2) | 22 (2.5) |
| Physical activity | 31 (3.5) | 111 (12.5) | 259 (29.1) | 208 (23.4) | 280 (31.5) |
| Sleep duration | 169 (19.0) | 205 (23.1) | 392 (44.1) | 75 (8.4) | 48 (5.4) |
| Significantly Better | Slightly Better | No Change | Significantly Worse | Slightly Worse | |
| Sleep quality | 96 (10.8) | 111 (12.5) | 533 (60.0) | 110 (12.4) | 39 (4.4) |
| Overeating Because of | Completely Consistent | Basically Consistent | Basically Not Consistent | Completely Not Consistent |
|---|---|---|---|---|
| Loneliness | 34 (3.8) | 253 (28.5) | 362 (40.7) | 240 (27.0) |
| Agitation | 31 (3.5) | 225 (25.3) | 375 (42.2) | 258 (29.0) |
| Anxiety | 25 (2.8) | 192 (21.6) | 401 (45.1) | 271 (30.5) |
| Tension | 20 (2.2) | 146 (16.4) | 428 (48.1) | 295 (33.2) |
| Sadness | 19 (2.1) | 134 (15.1) | 440 (49.5) | 296 (33.3) |
| Depression | 14 (1.6) | 190 (21.4) | 391 (44.0) | 294 (33.1) |
| Day | How Many Days a Week Do Strenuous Physical Activity | How Many Days a Week Do Moderate Physical Activity | How Many Days a Week Go for a Walk (10 min or More at a Time) |
|---|---|---|---|
| 0 | 399 (44.9) | 216 (24.3) | 241 (27.1) |
| 1 | 231 (26.0) | 206 (23.2) | 144 (16.2) |
| 2 | 129 (14.5) | 174 (19.6) | 172 (19.3) |
| 3 | 50 (5.6) | 107 (12.0) | 113 (12.7) |
| 4 | 29 (3.3) | 59 (6.6) | 65 (7.3) |
| 5 | 24 (2.7) | 53 (6.0) | 63 (7.1) |
| 6 | 10 (1.1) | 15 (1.7) | 23 (2.6) |
| 7 | 17 (1.9) | 59 (6.6) | 68 (7.6) |
| Numerical Continues Variables | Before the Outbreak | During the Outbreak | Difference Value of during and before | Paired t-Test p-Value |
|---|---|---|---|---|
| Body weight (kg) | 61.9 ± 11.6 | 62.4 ± 11.6 | 0.5 ± 2.8 | <0.001 |
| Step number per day | 6427 ± 4374 | 2714 ± 3542 | −3713 ± 4450 | <0.001 |
| Outdoor activities duration (min/d) | 48.1 ± 51.6 | 22.8 ± 38.0 | −25.3 ± 48.7 | <0.001 |
| Sedentary duration (h/d) | 5.3 ± 2.7 | 6.6 ± 3.1 | 1.3 ± 2.6 | <0.001 |
| Actual sleep duration (h/night) | 7.6 ± 2.9 | 8.0 ± 1.4 | 0.5 ± 1.3 | <0.001 |
| The time it takes to fall asleep (min) | 23.5 ± 24.7 | 31.9 ± 38.4 | 8.5 ± 28.9 | <0.001 |
| Total Food Intake | Weight Gain 1 (kg) | Whether Overweight/Obese before the Outbreak | Weight Gain 2 (kg) | Physical Activity | Weight Gain 3 (kg) |
|---|---|---|---|---|---|
| Large increase | 2.55 ± 3.97 | Normal weight | 0.68 ± 2.37 | Large increase | 0.10 ± 4.77 |
| (n = 87) | (n = 661) | (n = 31) | |||
| Slight increase | 1.31 ± 2.40 | Overweight/obesity | 0.07 ± 3.61 | Slight increase | 0.31 ± 2.66 |
| (n = 260) | (n = 228) | (n = 111) | |||
| No change | 0.16 ± 1.96 | p-Value for ANCOVA | No change | 0.16 ± 2.38 | |
| (n = 428) | 1p-Ancova < 0.001 2 p-Ancova < 0.001 3 p-Ancova = 0.024 | (n = 259) | |||
| Slight decrease | −0.92 ± 2.97 | Slight decrease | 0.66 ± 2.27 | ||
| (n = 96) | (n = 208) | ||||
| Large decrease | −4.14 ± 3.76 | Large decrease | 0.90 ± 3.08 | ||
| (n = 18) | (n = 280) | ||||
| Main Factors on Weight Gain | Score Assignment | ||||
|---|---|---|---|---|---|
| Large Increase | Slight Increase | No Change | Slight Decrease | Large Decrease | |
| Total food intake | 1 | 2 | 3 | 4 | 5 |
| Physical activity | 5 | 4 | 3 | 2 | 1 |
| Overweight/obesity before the outbreak | No | Yes | |||
| 1 | 2 | ||||
| Total Score of the Main Factors | Weight Gain (kg) | ||||
| Min = 3, Max = 12, Mean = 6.25, SD = 1.56 | Min = −16.0, Max = 20.0, Mean = 0.53, SD = 2.75 | ||||
| Linear Regression Equation of Weight Gain and Total Score of the Main Factors | |||||
| * Weight gain (kg) = −0.58 * Total score + 4.148, p-coefficient < 0.001 | |||||
| Variables Correlated with Weight Gain | Correlation Coefficient * | p-Coefficient |
|---|---|---|
| Increase in total food intake * | 0.406 | <0.001 |
| Staple food intake | 0.344 | <0.001 |
| Snacks and drinks intake | 0.259 | <0.001 |
| Livestock/poultry meat intake | 0.242 | <0.001 |
| Eggs intake | 0.236 | <0.001 |
| Fruits intake | 0.219 | <0.001 |
| Dairy intake | 0.207 | <0.001 |
| Aquatic products intake | 0.158 | <0.001 |
| Vegetable intake | 0.130 | <0.001 |
| Legumes intake | 0.116 | <0.001 |
| Increased food intake for psychological factors * | ||
| Agitation | 0.168 | <0.001 |
| Loneliness | 0.156 | <0.001 |
| Tension | 0.122 | <0.001 |
| Anxiety | 0.117 | <0.001 |
| Depression | 0.108 | <0.001 |
| Sadness | 0.106 | 0.001 |
| BMI before the outbreak | −0.161 | 0.001 |
| Decreased physical activity * | 0.102 | 0.002 |
| Decreased step number * | 0.095 | 0.005 |
| Decreased outdoor activity * | 0.091 | 0.006 |
| Increased sedentary time * | 0.075 | 0.025 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, Q.; Li, M.; Ji, Y.; Shi, Y.; Zhou, J.; Li, Q.; Qin, R.; Zhuang, X. “Stay-at-Home” Lifestyle Effect on Weight Gain during the COVID-19 Outbreak Confinement in China. Int. J. Environ. Res. Public Health 2021, 18, 1813. https://doi.org/10.3390/ijerph18041813
Zhu Q, Li M, Ji Y, Shi Y, Zhou J, Li Q, Qin R, Zhuang X. “Stay-at-Home” Lifestyle Effect on Weight Gain during the COVID-19 Outbreak Confinement in China. International Journal of Environmental Research and Public Health. 2021; 18(4):1813. https://doi.org/10.3390/ijerph18041813
Chicago/Turabian StyleZhu, Qi, Min Li, Yu Ji, Youpeng Shi, Jie Zhou, Qianyue Li, Ruoyu Qin, and Xun Zhuang. 2021. "“Stay-at-Home” Lifestyle Effect on Weight Gain during the COVID-19 Outbreak Confinement in China" International Journal of Environmental Research and Public Health 18, no. 4: 1813. https://doi.org/10.3390/ijerph18041813