 Emnet Getachew1,2*
Emnet Getachew1,2* Tsegaye Adebeta3
Tsegaye Adebeta3 Seke G. Y. Muzazu1,4Loveness Charlie1,5
Seke G. Y. Muzazu1,4Loveness Charlie1,5 Bibie Said1,6
Bibie Said1,6 Hanna Amanuel Tesfahunei1,7Catherine Lydiah Wanjiru1
Hanna Amanuel Tesfahunei1,7Catherine Lydiah Wanjiru1 Joan Acam1,8
Joan Acam1,8 Violet Dismas Kajogoo1
Violet Dismas Kajogoo1 Samrawit Solomon9
Samrawit Solomon9 Mary Gorret Atim1,10Tsegahun Manyazewal1
Mary Gorret Atim1,10Tsegahun Manyazewal1- 1Center for Innovative Drug Development and Therapeutic Trials for Africa (CDT-Africa), College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
- 2Department of Public Health, College of Health Science, Arsi University, Asella, Ethiopia
- 3Outpatient Department, Ethiopian Airlines Medical Unit, Addis Ababa, Ethiopia
- 4Enteric Diseases and Vaccines Research Unit, Centre for Infectious Disease Research in Zambia (CIDRZ), Lusaka, Zambia
- 5KNCV TB Foundation, Challenge TB Project, Blantyre, Malawi
- 6Outpatient Department, Kibong'oto National Tuberculosis Hospital, Moshi, Kilimanjaro, Tanzania
- 7Department of Public Health, Hager Biomedical Research Institute, Asmara, Eritrea
- 8Outpatient Department, Pope John's Hospital Aber, Atapara, Uganda
- 9School of Public Health, Saint Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia
- 10Soroti Regional Referral Hospital, Soroti, Uganda
COVID-19 is one of the most deadly diseases to have stricken us in recent decades. In the fight against this disease, governments and stakeholders require all the assistance they can get from various systems, including digital health interventions. Digital health technologies are supporting the tracking of the COVID-19 outbreak, diagnosing patients, expediting the process of finding potential medicines and vaccines, and disinfecting the environment, The establishment of electronic medical and health records, computerized clinical decision support systems, telemedicine, and mobile health have shown the potential to strengthen the healthcare system. Recently, these technologies have aided the health sector in a variety of ways, including prevention, early diagnosis, treatment adherence, medication safety, care coordination, documentation, data management, outbreak tracking, and pandemic surveillance. On the other hand, implementation of such technologies has questions of cost, compatibility with existing systems, disruption in patient-provider interactions, and sustainability, calling for more evidence on clinical utility and economic evaluations to help shape the next generation of healthcare. This paper argues how digital health interventions assist in the fight against COVID-19 and their opportunities, implications, and limitations.
Introduction
The World Health Organization has suggested that countries keep maximizing the opportunities for digital health interventions (DHIs) to accelerate sustainable health development and universal health coverage. DHIs are applications of smartphones, health information technology, wearable devices, telemedicine, and personalized medicine to facilitate healthcare and attain intended health outcomes (1, 2). They enhance patient care by facilitating treatment adherence and monitoring, person-centered care, laboratory diagnosis, data management, disease surveillance, drug-safety monitoring, and professional development (3–5). Healthcare institutions are looking for digital health innovations to improve care quality by integrating various technologies. However, there are impediments that countries, especially those with limited resources, face when implementing digital health, calling for a good grasp of how to develop appropriate strategies to benefit the most of digital health-enabled patient-centered health systems (5, 6).
Even though COVID-19 has caused massive problems in the healthcare system, it has forced the majority of countries to bridge the DHI gap (7). Different studies across the globe assessed the potential of DHIs in the fight against COVID-19, including their role in service delivery, health literacy, disease surveillance, treatment and vaccination, and program follow-up (7–10). At the start of the pandemic, innovative digital health-based analysis of social media data and news reports assisted in forecasting the spread of the disease. Social media platforms and features open up new avenues for educating people including hard-to-reach, recruiting participants in therapeutic trials, and remote-delivering of healthcare. However, there are several digital health implementation challenges and opportunities across countries and territories that need to be compiled to inform policy and practice as the disease is not yet over. This perspective paper argues how digital health interventions assist in the fight against COVID-19 and their opportunities, implications, and limitations.
Opportunities for implementing digital health interventions in the era of COVID-19
The COVID-19 pandemic served as a veritable testing ground for emerging digital health concepts and practices. DHIs provide enormous support in the social distancing time that interrupted healthcare service delivery. The application of telemedicine has facilitated service continuity with great potential to protect both patients and care providers (11). Hospitals' closure forced the public to seek and practice alternative digital health solutions such as smartphones to connect with their clinicians and follow-up routine care (8, 12). The use of digital health for COVID-19 screening reduced the number of visits to emergency departments while also improving healthcare system organization (13). mHealth, telemedicine, eHealth, and a variety of other mobile applications rose to prominence during lockdowns and were widely used for diagnosis, clinical care, and patient follow-up, demonstrating their potential beyond serving marginalized and underprivileged communities (14).
Virtual communication platforms facilitated remote interactions between healthcare professionals and patients, as well as the creation of operational management dashboards for optimizing workflows, resources, and patient-centered care. Several healthcare institutions have been drawn to cloud technologies in order to implement discrete COVID-19-related functionality such as testing, diagnostics, monitoring, triage, and patient consultations. large numbers of research papers accessible through the COVID-19 Open Research Database can be analyzed quickly using machine learning to extract relevant knowledge about drugs that might be beneficial for the treatment of COVID-19. By generating data summaries from multiple sources, artificial intelligence platforms enabled real-time monitoring of patients in high-risk settings for COVID-19. Insurance companies use of health-tracking reward programs that encourage the application of wearable health technologies, though implementation has been straightforward.
We have included case studies from three different countries to demonstrate how DHI has been used to support the healthcare system during the pandemic.
Case 1: China
In response to the pandemic, a hospital in China's Guangdong province that is well-known for its smart services used an existing platform to launch COVID 19 responsive services. These included information hubs, e-Consultation and screening, remote symptom monitoring, and psychological support. The system was web-based and linked users from social media sites (WeChat Facebook/Twitter equivalent), a phone App, and a website. The hospital reported that they saw a drastic drop in outpatient visits during the pandemic lockdowns but recorded high usage of the online services even at the height of the pandemic. This implies that more people had been restricted access to physical health services but they still got the healthcare services through DHIs. They also reported that the system allowed them to better triage patients who needed emergency response by providing remote care and hence, reducing the workload on clinicians and encouraging social distancing (15).
Case 2: Kenya
A provider-to-provider (P2P) asynchronous telemedicine model developed and implemented during the second year of COVID-19 in Kenya facilitated the delivery of essential health services (16). Since 2011, the Addis Clinic telemedicine platform has been providing access to specialized medical experts for frontline healthcare providers treating patients in low-resource settings. Healthcare providers heavily used this digital health platform in Kenya during the outbreak, indicating they found it very useful to them during the outbreak. Despite some of the infrastructure and network connectivity challenges present in the country, the provider-to-provider telemedicine platform was a viable option for receiving clinical recommendations from medical experts located remotely and sustaining essential health services.
Case 3: Ethiopia
A COVID-19 e-health educational intervention in Ethiopia targeting healthcare workers delivered a series of three 1-h medical seminars on COVID-19 prevention and treatment. The study collected post-seminar evaluation data from the participants using a questionnaire. The findings demonstrated the promising potential of transitioning healthcare training and delivery from an in-person to a digital medium in low-resource settings like Ethiopia (17). COVID-19 had a significant burden on patients, healthcare providers, and the healthcare system in general in Ethiopia, where the Ethiopian government and its partners intervened to sustain healthcare services (18–20).
Case 4: Vietnam
Since the beginning of the COVID-19 pandemic, seven major digital applications have been implemented in Vietnam (21). They have been classified into four categories based on their main purpose, including surveillance and contact tracing, health communication, telemedicine, and Artificial Intelligence to support diagnosis and treatment. The eCDS software was primarily focused on reporting case-based hospital admissions via an electronic system. Furthermore, two mobile apps (NCOVI and Vietnam Health Declaration) were created to record electronic health declaration forms for domestic and international travelers for case monitoring and surveillance (21).
Challenges and limitations to implementing digital health technologies
Despite a history of public health crises, data-sharing agreements and transactional standards do not exist uniformly between institutions, impeding a foundational infrastructure to meet data-sharing and integration needs for public health advancement. COVID-19 has revealed not only the need for data sharing but also the importance of serious evaluation and ethical considerations in the emerging field of digital health (22, 23). One of the main challenges in the biomedical research community and one of the contributors to international information sharing is maintaining control over the constantly generated data while simultaneously promoting their active use for generating scientific discoveries. Obtaining informed consent has been also a significant challenge in providing transparency about the kind of documents collected and which third parties able to access patient's data. Procedures were carried out remotely and/or via electronic consent during the pandemic; however, not all healthcare facilities were prepared to provide digital consent, prompting some scientists to create their own way of acquiring consent and electronic signature for participants in therapeutic trials. Issues such as potential participants' access to technology and an absence of user-friendly functionalities to interpret consent documents exacerbated the preceding problem of having complicated, lengthy, and technical consent documents in studies that used e-consent platforms.
There is a desperate need for strengthening resource capacity for effective implementation and evaluation of digital health technologies, taking into account the needs and priorities of countries (24–26). Inequalities in infrastructure and access to the internet and electricity are among the major challenges in the implementation and scale-up of DHIs in resource-limited settings. Digital health technologies were recommended to help patients adhere to their treatment; however, for optimal implementation of such technologies, trials evaluating the effectiveness of remote treatment are critically needed (19, 27–29).
Digital health literacy in the general population often determines the acceptability and adaptability of digital health solutions in a given country and this has been witnessed in the era of COVID-19. Low levels of digital health literacy were found to have a significant association with an individual's COVID-19 precautionary practices, information accuracy, vaccine hesitancy, and subjective wellbeing (30–34). The lack of qualified and skilled professionals in digital health is one of the main barriers to digital health applications, especially in resource-constrained settings (35).
In many resource-limited countries, the lack of policies and strategies, governance structures standard operating procedures, and financial resources hamper the successful deployment and implementation of DHIs (35). Sufficient and sustainable financial mechanisms are not in place for large-scale deployment of approved DHIs. Significant number of such technologies are not culturally adapted to incorporate the local context and facilitate easy understanding by patients and providers (36). The move away from traditional face-to-face care and treatment to digital health-enabled remote care and monitoring was not straightforward and the pros and cons vary by country, program, and the type of digital health technology employed (37).
Discussion
During the COVID-19 pandemic, there were a large number of patients seeking healthcare, putting a significant strain on healthcare providers. As a result, remote patient monitoring and the use of mHealth applications became an essential part of healthcare delivery. Telemedicine for remote consultation and the use of health devices such as pulse oximetry was a pivotal DHI in the COVID-19 pandemic. As mentioned in the case studies, applications designed for patient surveillance and contact tracing were crucial in reducing the pandemic's impact. The pandemic brought all stakeholders' priorities in various aspects of digital health adoption in line, including expedited regulatory approval of clinical studies. However, the widespread use of DHIs has been hampered by a lack of infrastructure, equitable access to the internet and electricity, and evidence-based digital health standards and data governance systems.
In the COVID-19 era, electronic medical records provide large amounts of data that can be used to generate research evidence, but these data require quality assurance and valid sampling procedures. Such disadvantages reduce the quality of research driven by data captured through digital health. Privacy is a concern in the digitalization of health care, where data generated by digital health must be safeguarded. It is also important to clearly explain to all stakeholders how their data will be used and protected.
DHI implementation during COVID-19 faces some unique challenges in resource-constrained settings. There were reservations and uncertainties regarding the use, adaptation, and integration of DHIs into the wider scope healthcare system before COVID-19, which slowed information dissemination and prompt responses. In these settings, insufficient financial resources, electricity supply, internet connectivity, and a trained workforce impede DHI implementation during COVID-19.
Because of their diverse nature and types, the lack of homogeneous interventions creates a major obstacle in implementing DH interventions. Such distinctions may limit model generalization and understanding of DH effectiveness (13, 78). During the pandemic, most low- and middle-income countries faced serious issues with the practicability and desirability of digital technology by care providers. This is due to a shortage of training on new technology tools, insufficient technical assistance, internet connectivity problems, and also other administrative complexities. Thus, care providers in those countries find it difficult to adopt and use digital health solutions in the healthcare system. Acknowledging that many patients need recommendations or guidance, the use of digital technologies in providing guidance services has already been previously deployed in some countries and can be adopted as an alternative to physical visits in hospitals.
We can conclude from the preceding discussion that DHIs have enabled countries to mitigate the impact of the COVID-19 pandemic, paving the way for and reshaping the next generation of healthcare. COVID-19 has aided in the massive deployment of DHIs for immediate outbreak response. To better move the DHIs momentum forward and sustainably mitigate COVID-19, equitable access to approved digital health technologies, political commitment, collaboration, stakeholder cooperation, and workforce capacity building are required. Beyond COVID-19, there may be an opportunity to set an additional focus and implement policies throughout the health system to support the potential use of DHI solutions.
The implication of this paper for policy and practice is summarized in Table 1.
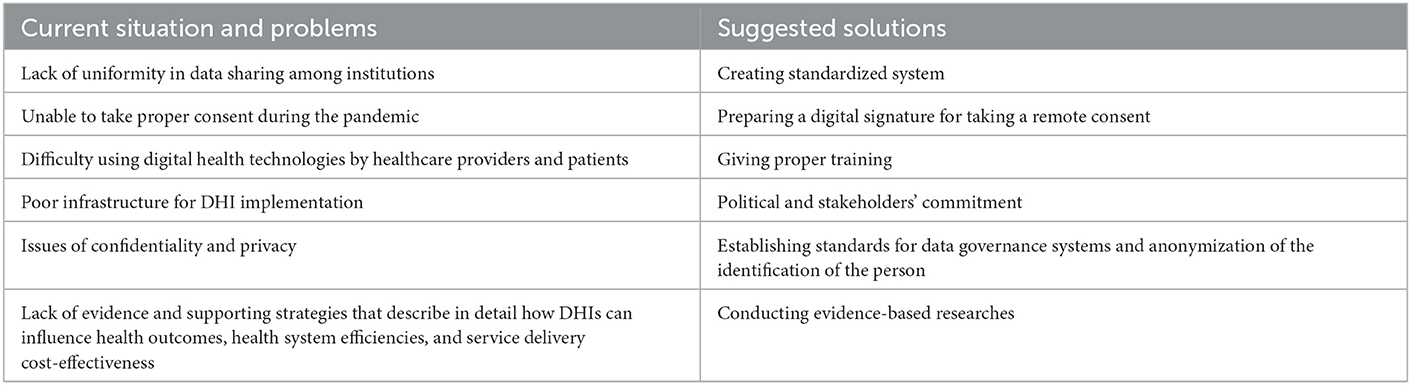
Table 1. Implications of the paper for digital health interventions policy and practice in the era of COVID-19.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://osf.io/gvm2z/.
Author contributions
Study conception, data acquisition, synthesis, and first draft of the manuscript: EG and TA. Data acquisition and synthesis: SM, CW, VK, HT, LC, JA, BS, SS, MA, and TM. Resource acquisition and critical review of the draft manuscript: TM. All authors reviewed and approved the final version for publication.
Acknowledgments
The authors would like to thank and appreciate the technical support given by the Center for Innovative Drug Development and Therapeutic Trias for Africa (CDT-Africa), College of Health Sciences, Addis Ababa University, Ethiopia.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
DHIs, digital health interventions.
References
1. Manyazewal T, Woldeamanuel Y, Blumberg HM, Fekadu A, Marconi VC. The potential use of digital health technologies in the African context: a systematic review of evidence from Ethiopia. NPJ Digit Med. (2021) 4:125. doi: 10.1038/s41746-021-00487-4
2. Sun T, He X, Song X, Shu L, Li Z. The digital twin in medicine: a key to the future of healthcare? Front Med (Lausanne). (2022) 9:907066. doi: 10.3389/fmed.2022.907066
3. Mir O, Ferrua M, Fourcade A, Mathivon D, Duflot-Boukobza A, Dumont S, et al. Digital remote monitoring plus usual care versus usual care in patients treated with oral anticancer agents: the randomized phase 3 CAPRI trial. Nat Med. (2022) 28:1224–31. doi: 10.1038/s41591-022-01788-1
4. Manyazewal T, Woldeamanuel Y, Holland DP, Fekadu A, Marconi VC. Effectiveness of a digital medication event reminder and monitor device for patients with tu berculosis (SELFTB): a multicenter randomized controlled trial. BMC Med. (2022) 20:310. doi: 10.1186/s12916-022-02521-y
5. Manyazewal T, Woldeamanuel Y, Holland DP, Fekadu A, Blumberg HM, Marconi VC. Electronic pillbox-enabled self-administered therapy versus standard directly observed therapy for tuberculosis medication adherence and treatment outcomes in Ethiopia (SELFTB): protocol for a multicenter randomized controlled trial. Trials. (2020) 21:383. doi: 10.1186/s13063-020-04324-z
6. McGuire M, de Waal A, Karellis A, Janssen R, Engel N, Sampath R, et al. Self-testing with digital supports as the new paradigm: a systematic review of global evidence (2010-2021). EClinicalMedicine. (2021) 39:101059. doi: 10.1016/j.eclinm.2021.101059
7. Budd J, Miller BS, Manning EM, Lampos V, Zhuang M, Edelstein M, et al. Digital technologies in the public-health response to COVID-19. Nat Med. (2020) 26:1183–92. doi: 10.1038/s41591-020-1011-4
8. Chereka AA, Demsash AW, Ngusie HS, Kassie SY. Digital health literacy to share COVID-19 related information and associated factors among healthcare providers worked at COVID-19 treatment centers in Amhara region, Ethiopia: a cross-sectional survey. Inform Med Unlocked. (2022) 30:100934. doi: 10.1016/j.imu.2022.100934
9. Ndayishimiye C, Lopes H, Middleton J. A systematic scoping review of digital health technologies during COVID-19: a new normal in primary health care delivery. Health Technol (Berl). (2023) 2023:1–12. doi: 10.1007/s12553-023-00725-7
10. Specht A, Sarma N, Linzbach T, Hellmund T, Hörig M, Wintel M, et al. Participatory development and implementation of inclusive digital health communication on COVID-19 with homeless people. Front Public Health. (2022) 10:1042677. doi: 10.3389/fpubh.2022.1042677
11. Bokolo AJ. Application of telemedicine and eHealth technology for clinical services in response to COVID-19 pandemic. Health Technol (Berl). (2021) 11:359–66. doi: 10.1007/s12553-020-00516-4
12. Pandit JA, Radin JM, Quer G, Topol EJ. Smartphone apps in the COVID-19 pandemic. Nat Biotechnol. (2022) 40:1013–22. doi: 10.1038/s41587-022-01350-x
13. Peek N, Sujan M, Scott P. Digital health and care in pandemic times: impact of COVID-19. BMJ Health Care Inform. (2020) 27:e100166. doi: 10.1136/bmjhci-2020-100166
14. R Niakan Kalhori S, Bahaadinbeigy K, Deldar K, Gholamzadeh M, Hajesmaeel-Gohari S, Ayyoubzadeh SM. Digital health solutions to control the COVID-19 pandemic in countries with high disease prevalence: literature review. J Med Internet Res. (2021) 23:e19473. doi: 10.2196/19473
15. Lian W, Wen L, Zhou Q, Zhu W, Duan W, Xiao X, et al. Digital health technologies respond to the COVID-19 pandemic in a tertiary hospital in China: development and usability study. J Med Internet Res. (2020) 22:e24505. doi: 10.2196/24505
16. Kim EJ, Moretti ME, Kimathi AM, Chan SY, Wootton R. Use of provider-to-provider telemedicine in Kenya during the COVID-19 pandemic. Front Public Health. (2022) 10:1028999. doi: 10.3389/fpubh.2022.1028999
17. Yudkin JS, Hodes RM, Sandler-Loeff A, Messiah SE. Needs assessment and best practices for digital trainings for health professionals in Ethiopia using the RE-AIM framework: COVID-19, case study. Disaster Med Public Health Prep. (2022) 2022:1–9. doi: 10.1017/dmp.2022.224
18. Chilot D, Woldeamanuel Y, Manyazewal T. Real-time impact of COVID-19 on clinical care and treatment of patients with tuberculosis: a multicenter cross-sectional study in <city>Addis Ababa </city>, Ethiopia. Ann Glob Health. (2021) 87:109. doi: 10.5334/aogh.3481
19. Mohammed H, Oljira L, Roba KT, Yimer G, Fekadu A, Manyazewal T. Containment of COVID-19 in Ethiopia and implications for tuberculosis care and research. Infect Dis Poverty. (2020) 9:131. doi: 10.1186/s40249-020-00753-9
20. Chilot D, Woldeamanuel Y, Manyazewal T. COVID-19 burden on HIV patients attending antiretroviral therapy in <city>Addis Ababa </city>, Ethiopia: a multicenter cross-sectional study. Front Med (Lausanne). (2022) 9:741862. doi: 10.3389/fmed.2022.741862
21. Bui LV, Ha ST, Nguyen HN, Nguyen TT, Nguyen TP, Tran K, et al. The contribution of digital health in the response to COVID-19 in Vietnam. Front Public Health. (2021) 9:672732. doi: 10.3389/fpubh.2021.672732
22. Duan Y, Luo J, Zhao L, Zhang X, Miao J, Moher D, et al. Reporting and data sharing level for COVID-19 vaccine trials: a cross-sectional study. EBioMedicine. (2022) 78:103962. doi: 10.1016/j.ebiom.2022.103962
23. Chirico F, Teixeira da Silva JA. COVID-19 health policies: the need for transparent data sharing between scientists, governments, and policymakers. Oman Med J. (2022) 37:e418. doi: 10.5001/omj.2022.63
24. Cummins N, Schuller BW. Five crucial challenges in digital health. Front Digit Health. (2020) 2:536203. doi: 10.3389/fdgth.2020.536203
25. Getachew E, Woldeamanuel Y, Manyazewal T. Capacity and readiness assessment of healthcare facilities for digital health interventions against tuberculosis and HIV in Addis Ababa, Ethiopia. Front Digit Health. (2022) 4:821390. doi: 10.3389/fdgth.2022.821390
26. Getachew E, Woldeamanuel Y, Manyazewal T. Digital health interventions in the clinical care and treatment of tuberculosis and HIV in central Ethiopia: an initial provider perceptions and acceptability study using the unified theory of acceptance and use of technology model. Int J Mycobacteriol. (2022) 11:1–9. doi: 10.4103/ijmy.ijmy_235_21
27. Manyazewal T, Woldeamanuel Y, Blumberg HM, Fekadu A, Marconi VC. The fight to end tuberculosis must not be forgotten in the COVID-19 outbreak. Nat Med. (2020) 26:811–2. doi: 10.1038/s41591-020-0917-1
28. Manyazewal T, Woldeamanuel Y, Fekadu A, Holland DP, Marconi VC. Effect of digital medication event reminder and monitor-observed therapy vs standard directly observed therapy on health-related quality of life and catastrophic costs in patients with tuberculosis: a secondary analysis of a randomized clinical trial. JAMA Netw Open. (2022) 5:e2230509. doi: 10.1001/jamanetworkopen.2022.30509
29. Manyazewal T, Woldeamanuel Y, Getinet T, Hoover A, Bobosha K, Fuad O, et al. Patient-reported usability and satisfaction with electronic medication event reminder and monitor device for tuberculosis: a multicentre, randomised controlled trial. eClinicalMedicine. (2023) 56:101820. doi: 10.1016/j.eclinm.2022.101820
30. Marzo RR, Su TT, Ismail R, Htay MNN, Essar MY, Chauhan S, et al. Digital health literacy for COVID-19 vaccination and intention to be immunized: a cross sectional multi-country study among the general adult population. Front Public Health. (2022) 10:998234. doi: 10.3389/fpubh.2022.998234
31. Quansah F, Ankomah F, Agormedah EK, Abieraba RSK, Srem-Sai M, Hagan JE Jr, et al. COVID-digital health literacy and subjective well-being of students in Ghana: mediation-moderation analyses. Health Sci Rep. (2022) 5:e916. doi: 10.1002/hsr2.916
32. Atim MG, Kajogoo VD, Amare D, Said B, Geleta M, Muchie Y, et al. COVID-19 and health sector development plans in Africa: the impact on maternal and child health outcomes in Uganda. Risk Manag Healthc Policy. (2021) 14:4353–60. doi: 10.2147/RMHP.S328004
33. Umer A, Abdella K, Tekle Y, Debebe A, Manyazewal T, Yuya M, et al. Community engagement in the fight against COVID-19: knowledge, attitude, and prevention practices among Dire Dawa Residents, Eastern Ethiopia. Front Public Health. (2021) 9:753867. doi: 10.3389/fpubh.2021.753867
34. Mussie KM, Setchell J, Elger BS, Kaba M, Memirie ST, Wangmo T. Care of older persons in Eastern Africa: a scoping review of Ethical issues. Front Public Health. (2022) 10:923097. doi: 10.3389/fpubh.2022.923097
35. Mason C, Lazenby S, Stuhldreher R, Kimball M, Bartlein R. Lessons learned from implementing digital health tools to address COVID-19 in LMICs. Front Public Health. (2022) 10:859941. doi: 10.3389/fpubh.2022.859941
36. Dettori M, Castiglia P. COVID-19 and digital health: evolution, perspectives and opportunities. Int J Environ Res Public Health. (2022) 19:8519. doi: 10.3390/ijerph19148519
Keywords: digital health, technology, DHIs, COVID-19, pandemic
Citation: Getachew E, Adebeta T, Muzazu SGY, Charlie L, Said B, Tesfahunei HA, Wanjiru CL, Acam J, Kajogoo VD, Solomon S, Atim MG and Manyazewal T (2023) Digital health in the era of COVID-19: Reshaping the next generation of healthcare. Front. Public Health 11:942703. doi: 10.3389/fpubh.2023.942703
Received: 12 July 2022; Accepted: 26 January 2023;
Published: 15 February 2023.
Edited by:
Anthony Bokolo Jr, Institute for Energy Technology, NorwayReviewed by:
Ajaya Bhattarai, Tribhuvan University, NepalSong Niu, Shanghai International Studies University, China
Copyright © 2023 Getachew, Adebeta, Muzazu, Charlie, Said, Tesfahunei, Wanjiru, Acam, Kajogoo, Solomon, Atim and Manyazewal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emnet Getachew,  emnet.getachew@aau.edu.et
emnet.getachew@aau.edu.et