
A Retrospective Analysis of the Challenges of Urothelial Cancer Management during the COVID-19 Pandemic at a Single Academic Center in Romania

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design and Ethical Considerations
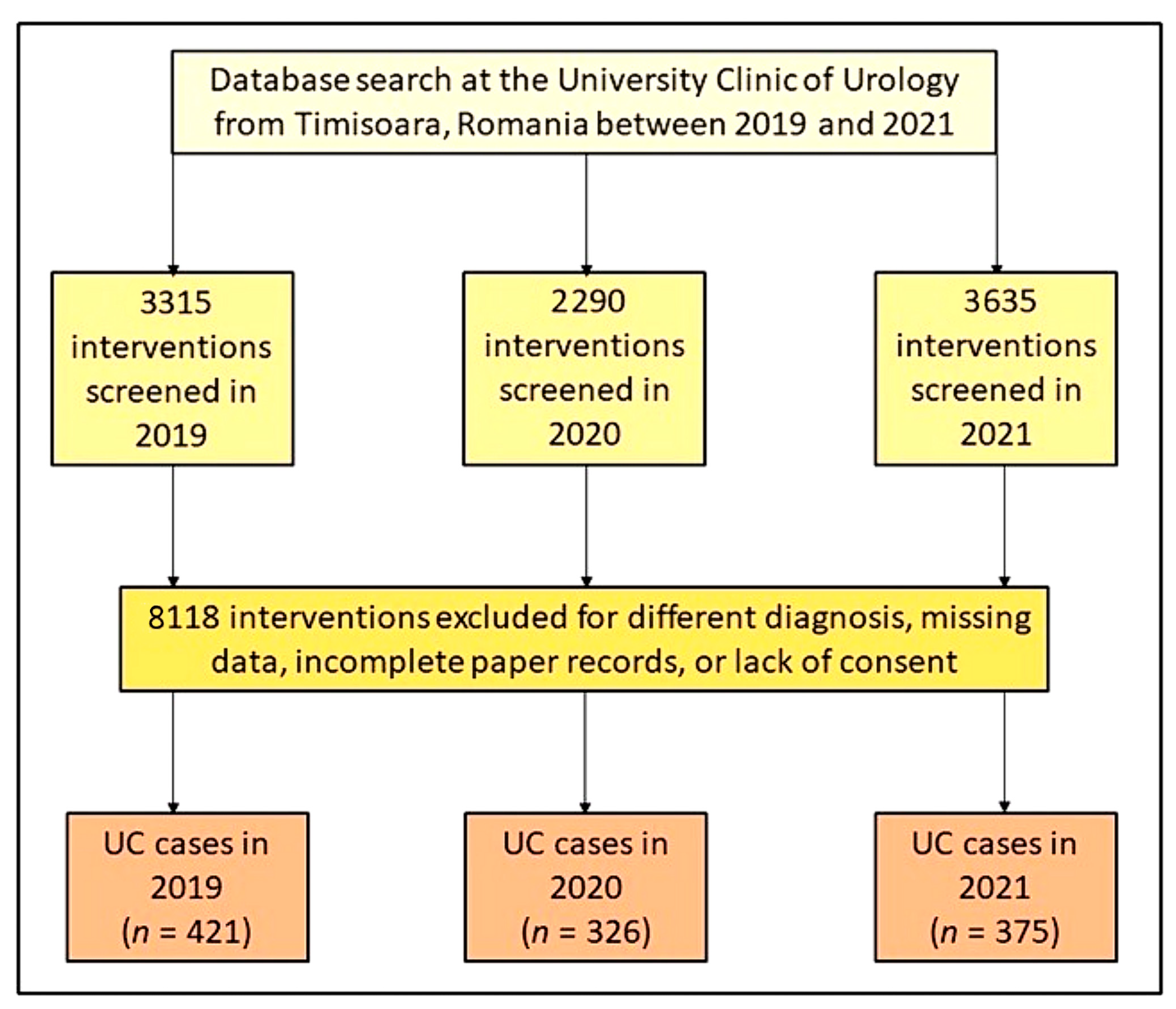
2.2. Inclusion Criteria
2.3. Variables
2.4. Statistical Analysis
3. Results
3.1. Patients’ Baseline Characteristics
3.2. Oncological Features
3.3. Comparison of Outcomes and Interventions
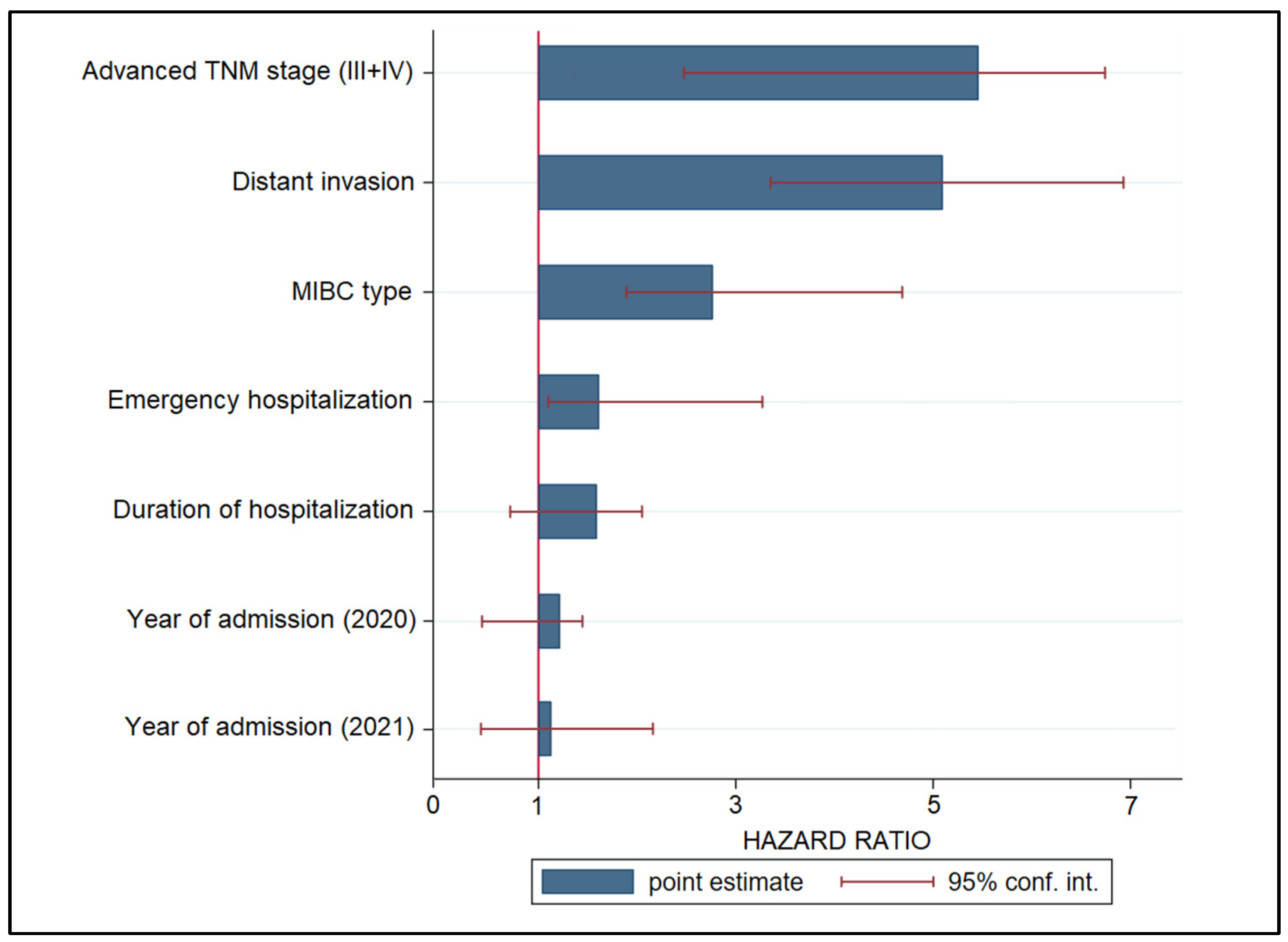
3.4. Risk Factor Analysis
4. Discussion
4.1. Important Findings and Literature Review
4.2. Study Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, S.; McNab, C.; Olson, R.M.; Bristol, N.; Nolan, C.; Bergstrøm, E.; Bartos, M.; Mabuchi, S.; Panjabi, R.; Karan, A.; et al. How an outbreak became a pandemic: A chronological analysis of crucial junctures and international obligations in the early months of the COVID-19 pandemic. Lancet 2021, 398, 2109–2124. [Google Scholar] [CrossRef] [PubMed]
- Citu, I.M.; Citu, C.; Gorun, F.; Neamtu, R.; Motoc, A.; Burlea, B.; Rosca, O.; Bratosin, F.; Hosin, S.; Manolescu, D.; et al. Using the NYHA Classification as Forecasting Tool for Hospital Readmission and Mortality in Heart Failure Patients with COVID-19. J. Clin. Med. 2022, 11, 1382. [Google Scholar] [CrossRef] [PubMed]
- Bogdan, I.; Citu, C.; Bratosin, F.; Malita, D.; Romosan, I.; Gurban, C.V.; Bota, A.V.; Turaiche, M.; Bratu, M.L.; Pilut, C.N.; et al. The Impact of Multiplex PCR in Diagnosing and Managing Bacterial Infections in COVID-19 Patients Self-Medicated with Antibiotics. Antibiotics 2022, 11, 437. [Google Scholar] [CrossRef] [PubMed]
- Aabed, H.; Bloanca, V.; Crainiceanu, Z.; Bratosin, F.; Citu, C.; Diaconu, M.M.; Ciorica, O.; Bratu, T. The Impact of SARS-CoV-2 Pandemic on Patients with Malignant Melanoma at a Romanian Academic Center: A Four-Year Retrospective Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8499. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.P.; Devana, S.K.; Chaudhary, K.; Singh, S.K. Changing urological practice during COVID-19. Indian J. Urol. 2020, 36, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; Wang, M. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [Green Version]
- Van Poel, E.; Vanden Bussche, P.; Klemenc-Ketis, Z.; Willems, S. How did general practices organize care during the COVID-19 pandemic: The protocol of the cross-sectional PRICOV-19 study in 38 countries. BMC Prim. Care 2022, 23, 11. [Google Scholar] [CrossRef]
- Popescu, A.; Craina, M.; Pantea, S.; Pirvu, C.; Chiriac, V.D.; Marincu, I.; Bratosin, F.; Bogdan, I.; Hosin, S.; Citu, C.; et al. COVID-19 Pandemic Effects on Cervical Cancer Diagnosis and Management: A Population-Based Study in Romania. Diagnostics 2022, 12, 907. [Google Scholar] [CrossRef]
- Davidson, N.E.; Knudsen, K.E.; Nasso, S.F.; Oyer, R.; Pergam, S.; Strawbridge, L.; Shulman, L. Cancer Care at the Beginning of the COVID-19 Pandemic: Effects on Patients and Early Interventions to Mitigate Stresses on Care. Cancer J. 2022, 28, 107–110. [Google Scholar] [CrossRef]
- Cerbu, B.; Grigoras, M.L.; Bratosin, F.; Bogdan, I.; Citu, C.; Bota, A.V.; Timircan, M.; Bratu, M.L.; Levai, M.C.; Marincu, I. Laboratory Profile of COVID-19 Patients with Hepatitis C-Related Liver Cirrhosis. J. Clin. Med. 2022, 11, 652. [Google Scholar] [CrossRef]
- Citu, C.; Gorun, F.; Motoc, A.; Ratiu, A.; Gorun, O.M.; Burlea, B.; Neagoe, O.; Citu, I.M.; Rosca, O.; Bratosin, F.; et al. Evaluation and Comparison of the Predictive Value of 4C Mortality Score, NEWS, and CURB-65 in Poor Outcomes in COVID-19 Patients: A Retrospective Study from a Single Center in Romania. Diagnostics 2022, 12, 703. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Khillan, R.; Mishra, Y.; Khurana, S. The safety profile of COVID-19 vaccinations in the United States. Am. J. Infect. Control 2022, 50, 15–19. [Google Scholar] [CrossRef]
- Citu, I.M.; Citu, C.; Gorun, F.; Sas, I.; Bratosin, F.; Motoc, A.; Burlea, B.; Rosca, O.; Malita, D.; Gorun, O.M. The Risk of Spontaneous Abortion Does Not Increase Following First Trimester mRNA COVID-19 Vaccination. J. Clin. Med. 2022, 11, 1698. [Google Scholar] [CrossRef] [PubMed]
- Madan, A.; Siglin, J.; Khan, A. Comprehensive review of implications of COVID-19 on clinical outcomes of cancer patients and management of solid tumors during the pandemic. Cancer Med. 2020, 9, 9205–9218. [Google Scholar] [CrossRef]
- Ribas, A.; Sengupta, R.; Locke, T.; Zaidi, S.K.; Campbell, K.M.; Carethers, J.M.; Jaffee, E.M.; Wherry, E.J.; Soria, J.-C.; D’Souza, G. Priority COVID-19 Vaccination for Patients with Cancer while Vaccine Supply Is Limited. Cancer Discov. 2021, 11, 233–236. [Google Scholar] [CrossRef]
- Tulchiner, G.; Staudacher, N.; Fritz, J.; Radmayr, C.; Culig, Z.; Horninger, W.; Pichler, R. The “COVID-19 Pandemic Gap” and Its Influence on Oncologic Outcomes of Bladder Cancer. Cancers 2021, 13, 1754. [Google Scholar] [CrossRef]
- Van Hoogstraten, L.M.C.; Kiemeney, L.A.; Meijer, R.P.; Van Leenders, G.J.L.H.; Vanneste, B.G.L.; Incrocci, L.; Smilde, T.J.; Siesling, S.; Witjes, J.A.; Aben, K.K.H. The Impact of the COVID-19 Pandemic on Bladder Cancer Care in the Netherlands. Bladder. Cancer 2022, 8, 139–154. [Google Scholar] [CrossRef]
- Sanchez-Ortiz, R.F.; Huang, W.C.; Mick, R.; Van Arsdalen, K.N.; Wein, A.J.; Malkowicz, S.B. An interval longer than 12 weeks between the diagnosis of muscle invasion and cystectomy is associated with worse outcome in bladder carcinoma. J. Urol. 2003, 169, 110–115. [Google Scholar] [CrossRef]
- Boeri, L.; Soligo, M.; Frank, I.; Boorjian, S.A.; Thompson, R.H.; Tollefson, M.; Quevedo, F.J.; Cheville, J.C.; Karnes, R.J. Delaying Radical Cystectomy After Neoadjuvant Chemotherapy for Muscle-invasive Bladder Cancer is Associated with Adverse Survival Outcomes. Eur. Urol. Oncol. 2019, 2, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Galsky, M.D.; Chen, G.J.; Oh, W.K.; Bellmunt, J.; Roth, B.J.; Petrioli, R.; Dogliotti, L.; Dreicer, R.; Sonpavde, G. Comparative effectiveness of cisplatin-based and carboplatin-based chemotherapy for treatment of advanced urothelial carcinoma. Ann. Oncol. 2012, 23, 406–410. [Google Scholar] [CrossRef]
- Dash, A.; Pettus, I.V.J.A.; Herr, H.W.; Bochner, B.H.; Dalbagni, G.; Donat, S.M.; Bajorin, D.F. A role for neoadjuvant gemcitabine plus cisplatin in muscle-invasive urothelial carcinoma of the bladder: A retrospective experience. Cancer 2008, 113, 2471–2477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katims, A.B.; Razdan, S.; Eilender, B.M.; Wiklund, P.; Tewari, A.K.; Kyprianou, N.; Badani, K.K.; Mehrazin, R. Urologic oncology practice during COVID-19 pandemic: A systematic review on what can be deferrable vs. nondeferrable. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Lin-Brande, M.; Pearce, S.M.; Ashrafi, A.N.; Nazemi, A.; Burg, M.L.; Ghodoussipour, S.; Miranda, G.; Djaladat, H.; Schuckman, A.; Daneshmand, S. Assessing the Impact of Time to Cystectomy for Variant Histology of Urothelial Bladder Cancer. Urology 2019, 133, 157–163. [Google Scholar] [CrossRef]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004; Available online: https://apps.who.int/iris/handle/10665/42980 (accessed on 21 September 2022).
- Desouky, E. Impact of COVID-19 on Urologists: Learning on the Go. Eur. Urol. Focus 2020, 6, 1132–1134. [Google Scholar] [CrossRef]
- Jäger, W.; Thomas, C.; Haag, S.; Hampel, C.; Salzer, A.; Thüroff, J.W.; Wiesner, C. Early vs delayed radical cystectomy for ‘high-risk’ carcinoma not invading bladder muscle: Delay of cystectomy reduces cancer-specific survival. Br. J. Urol. 2011, 108, E284–E288. [Google Scholar] [CrossRef] [PubMed]
- Teoh, J.Y.C.; Roupret, M.; Shariat, S.F.; Herrmann, T. Intravesical therapy for bladder cancer in the pandemic of COVID-19. World J. Urol. 2021, 39, 1313–1314. [Google Scholar] [CrossRef] [PubMed]
- Tachibana, I.; Ferguson, E.L.; Mahenthiran, A.; Natarajan, J.P.; Masterson, T.A.; Bahler, C.D.; Sundaram, C.P. Delaying Cancer Cases in Urology during COVID-19: Review of the Literature. J. Urol. 2020, 204, 926–933. [Google Scholar] [CrossRef]
- Wallis, C.J.D.; Novara, G.; Marandino, L.; Bex, A.; Kamat, A.M.; Karnes, R.J.; Morgan, T.M.; Mottet, N.; Gillessen, S.; Bossi, A.; et al. Risks from Deferring Treatment for Genitourinary Cancers: A Collaborative Review to Aid Triage and Management During the COVID-19 Pandemic. Eur. Urol. 2020, 78, 29–42. [Google Scholar] [CrossRef]
- Ok, F.; Durmus, E. Disease management in a patient diagnosed with COVID-19 disease during induction intravesical BCG therapy: A case report and review of the literature. Urol. J. 2021. [Google Scholar] [CrossRef]
- Wallace, D.M.A.; Bryan, R.T.; Dunn, J.A.; Begum, G.; Bathers, S.; West Midlands Urological Research Group. Delay and survival in bladder cancer. BJU Int. 2002, 89, 868–878. [Google Scholar] [CrossRef]
- Elkaddoum, R.; Haddad, F.G.; Eid, R.; Kourie, H.R. Telemedicine for cancer patients during COVID-19 pandemic: Between threats and opportunities. Futur. Oncol. 2020, 16, 1225–1227. [Google Scholar] [CrossRef] [PubMed]
- Burbury, K.; Wong, Z.; Yip, D.; Thomas, H.; Brooks, P.; Gilham, L.; Piper, A.; Solo, I.; Underhill, C. Telehealth in cancer care: During and beyond the COVID -19 pandemic. Intern. Med. J. 2021, 51, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Sekaran, S.; Royapuram Parathasarathy, P.; Palati, S.; Ganapathy, D.; Muzammil, K.; Nasir, N. Commentary: Telemedicine for cancer patients in the COVIDian era-A long overdue promise? Front. Public Health 2022, 10, 931380. [Google Scholar] [CrossRef]
- Cumberbatch, M.G.K.; Noon, A.P. Epidemiology, aetiology and screening of bladder cancer. Transl. Androl. Urol. 2019, 8, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Waldert, M.; Karakiewicz, P.I.; Raman, J.D.; Remzi, M.; Isbarn, H.; Lotan, Y.; Capitanio, U.; Bensalah, K.; Marberger, M.J.; Shariat, S.F. A delay in radical nephroureterectomy can lead to upstaging. BJU Int. 2010, 105, 812–817. [Google Scholar] [CrossRef]
- Lee, J.N.; Kwon, S.Y.; Choi, G.-S.; Kim, H.T.; Kim, T.-H.; Kwon, T.G.; Kim, B.W. Impact of surgical wait time on oncologic outcomes in upper urinary tract urothelial carcinoma. J. Surg. Oncol. 2014, 110, 468–475. [Google Scholar] [CrossRef]
- Nison, L.; Rouprêt, M.; Bozzini, G.; Ouzzane, A.; Audenet, F.; Pignot, G.; Ruffion, A.; Cornu, J.-N.; Hurel, S. The oncologic impact of a delay between diagnosis and radical nephroureterectomy due to diagnostic ureteroscopy in upper urinary tract urothelial carcinomas: Results from a large collaborative database. World J. Urol. 2013, 31, 69–76. [Google Scholar] [CrossRef]
- O’Meara, S.; Bhatt, N.R.; Flynn, R.J.; Manecksha, R.P.; Thomas, A.Z. Bladder cancer in Ireland: A 21-year review. Ir. J. Med. Sci. 2021, 190, 531–538. [Google Scholar] [CrossRef]
- Leow, J.J.; Tan, W.S.; Tan, T.W.; Chan, V.W.-S.; Tikkinen, K.A.O.; Kamat, A.; Sengupta, S.; Meng, M.V.; Shariat, S.; Roupret, M.; et al. A systematic review and meta-analysis on delaying surgery for urothelial carcinoma of bladder and upper tract urothelial carcinoma: Implications for the COVID19 pandemic and beyond. Front. Surg. 2022, 9, 879774. [Google Scholar] [CrossRef]
- Sánchez-González, J.V.; Colet, O.; Gómez-Palomo, F.; Pérez-Ardavin, J.; Bernal, A.; Boronat, F. The invisible impact of COVID-19: Indirect mortality in urology. Minerva Urol. Nephrol. 2021, 73, 132–133. [Google Scholar] [CrossRef]
- Ficarra, V.; Novara, G.; Abrate, A.; Bartoletti, R.; Crestani, A.; De Nunzio, C.; Giannarini, G.; Gregori, A.; Liguori, G.; Mirone, V.; et al. Urology practice during the COVID-19 pandemic. Minerva Urol. Nefrol. 2020, 72, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Kool, R.; Yanev, I.; Hijal, T.; Vanhuyse, M.; Cury, F.L.; Souhami, L.; Kassouf, W.; Dragomir, A. Trimodal therapy vs. radical cystectomy for muscle-invasive bladder cancer: A Canadian cost-effectiveness analysis. Can. Urol. Assoc. J. 2022, 16, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Byun, S.J.; Ahn, H.; Kim, C.-S.; Hong, B.-S.; Yoo, S.; Lee, J.-L.; Kim, Y.S. Comparison of outcomes between trimodal therapy and radical cystectomy in muscle-invasive bladder cancer: A propensity score matching analysis. Oncotarget 2017, 8, 68996–69004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wettstein, M.S.; Rooprai, J.K.; Pazhepurackel, C.; Wallis, C.J.D.; Klaassen, Z.; Uleryk, E.M.; Hermanns, T.; Fleshner, N.E.; Zlotta, A.R.; Kulkarni, G.S. Systematic review and meta-analysis on trimodal therapy versus radical cystectomy for muscle-invasive bladder cancer: Does the current quality of evidence justify definitive conclusions? PLoS ONE 2019, 14, e0216255. [Google Scholar] [CrossRef]
- Oderda, M.; Soria, F.; Rosi, F.; Calleris, G.; Mazzoli, S.; Giordano, A.; Pizzuto, G.; Marquis, A.; De Bellis, M.; Vitiello, F.; et al. COVID-19 pandemic impact on uro-oncological disease outcomes at an Italian tertiary referral center. World J. Urol. 2021, 40, 263–269. [Google Scholar] [CrossRef]
- Anderson, S.; Rigney, K.; Hayes, L.; Ryan, P.C.; Chaitanya, V.; Jacob, P.T.; Abdelrahman, M.; Giri, S.K. A retrospective cohort study of bladder cancer following the COVID-19 pandemic: Are patients presenting with more aggressive disease? . Ann. Med. Surg. 2022, 81, 104430. [Google Scholar] [CrossRef]
- Tayeh, G.A.; Khalil, N.; Alkassis, M.; Aoun, F.; Waked, C.; Nemr, E. Urothelial carcinoma in COVID-19: Lessons from a pandemic and their impact on clinical practice. Future Oncol. 2021, 17, 4233–4235. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| 2019 (n = 421) | 2020 (n = 326) | 2021 (n = 375) | p-Value * | |
|---|---|---|---|---|
| Background | ||||
| Age, years (mean ± SD) ** | 63.2 ± 9.6 | 64.0 ± 10.1 | 64.4 ± 10.3 | 0.224 |
| Age range | 0.356 | |||
| <50 | 88 (20.9%) | 81 (24.8%) | 76 (20.3%) | |
| 50–70 | 175 (41.6%) | 143 (43.9%) | 164 (43.7%) | |
| ≥71 | 158 (37.5%) | 102 (31.3%) | 135 (36.0%) | |
| Gender | 0.911 | |||
| Female | 186 (44.2%) | 142 (43.6%) | 160 (42.7%) | |
| Male | 235 (55.8%) | 184 (56.4%) | 215 (57.3%) | |
| BMI, kg/m2 (mean ± SD) | 26.6 ± 3.7 | 27.2 ± 3.9 | 27.0 ± 4.1 | 0.097 |
| Substance use behavior | ||||
| Chronic smoking | 149 (35.4%) | 132 (40.5%) | 141 (37.6%) | 0.361 |
| Chronic alcohol use | 32 (7.6%) | 28 (8.6%) | 25 (6.7%) | 0.630 |
| Place of origin | 0.436 | |||
| Rural | 182 (43.2%) | 155 (47.5%) | 163 (43.5%) | |
| Urban | 239 (56.8%) | 171 (52.5%) | 212 (56.5%) | |
| Referred from | 0.090 | |||
| Primary care | 194 (46.1%) | 127 (39.0%) | 173 (46.1%) | |
| Secondary care | 227 (53.9%) | 199 (61.0%) | 202 (53.9%) | |
| SARS-CoV-2 infection | - | 17 (5.2%) | 13 (3.5%) | 0.254 |
| COVID-19 vaccination status | <0.001 | |||
| Yes | - | 37 (11.3%) | 94 (25.1%) | |
| No | - | 289 (88.7%) | 281 (74.9%) |
| 2019 (n = 421) | 2020 (n = 326) | 2021 (n = 375) | p-Value | |
|---|---|---|---|---|
| Number of comorbidities | 0.150 | |||
| 0-1 | 116 (27.6%) | 103 (31.6%) | 98 (26.1%) | |
| 2 | 162 (38.5%) | 119 (36.5%) | 127 (33.9%) | |
| ≥3 | 143 (34.0%) | 104 (31.9%) | 150 (40.0%) | |
| Anatomical distribution | 0.939 | |||
| Renal pelvis and ureter | 83 (19.7%) | 61 (18.7%) | 73 (19.5%) | |
| Bladder | 338 (80.3%) | 265 (81.3%) | 302 (80.5%) | |
| Tumoral infiltration | (n = 338) | (n = 265) | (n = 302) | 0.046 |
| NMIBC | 235 (69.5%) | 166 (62.6%) | 183 (60.6%) | |
| MIBC | 103 (30.5%) | 99 (37.4%) | 119 (39.4%) | |
| Grading | 0.081 | |||
| Low grade | 149 (35.4%) | 127 (39.0%) | 131 (34.9%) | |
| High grade | 144 (34.2%) | 116 (35.6%) | 112 (29.9%) | |
| Unknown | 128 (30.4%) | 83 (25.5%) | 132 (35.2%) | |
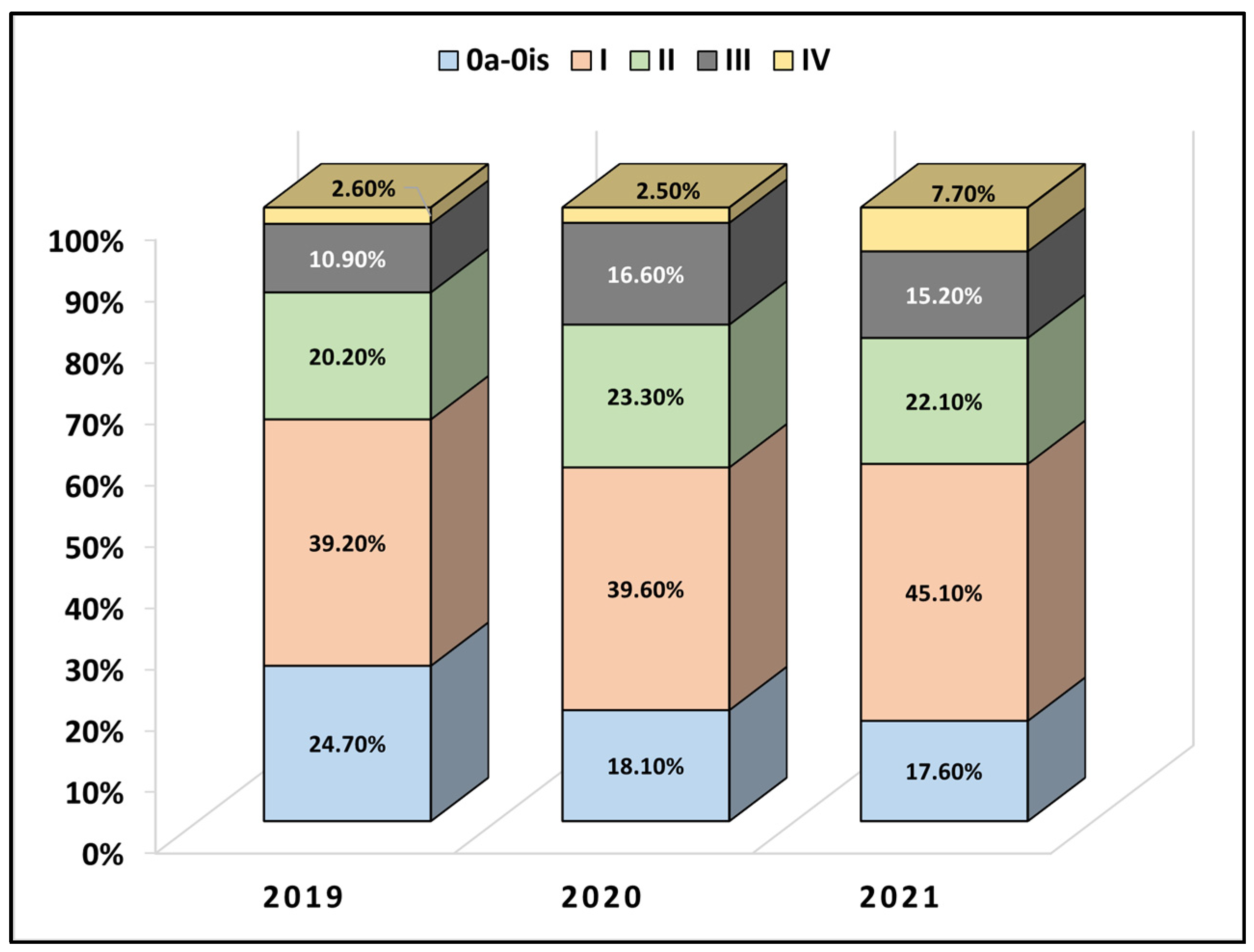
| TNM staging | <0.001 | |||
| Stage 0a-0is | 104 (24.7%) | 59 (18.1%) | 66 (17.6%) | |
| Stage I | 175 (39.2%) | 129 (39.6%) | 169 (45.1%) | |
| Stage II | 85 (20.2%) | 76 (23.3%) | 54 (14.4%) | |
| Stage III | 46 (10.9%) | 54 (16.6%) | 57 (15.2%) | |
| Stage IV | 11 (2.6%) | 8 (2.5%) | 29 (7.7%) | |
| Invasion | <0.001 | |||
| Local invasion | 131 (31.1%) | 130 (39.9%) | 140 (37.3%) | |
| Distant invasion | 11 (2.6%) | 8 (2.5%) | 29 (7.7%) |
| 2019 (n = 421) | 2020 (n = 326) | 2021 (n = 375) | p-Value * | |
|---|---|---|---|---|
| Intervention | ||||
| Cystectomy | 22 (5.2%) | 14 (4.3%) | 38 (10.1%) | 0.003 |
| TURBT | 368 (87.4%) | 289 (88.7%) | 292 (77.9%) | <0.001 |
| Nephrectomy | 31 (7.4%) | 23 (7.1%) | 45 (12.0%) | 0.028 |
| Neoadjuvant chemotherapy | 86 (20.4%) | 71 (21.8%) | 89 (23.7%) | 0.529 |
| Radiotherapy | 48 (11.4%) | 36 (11.0%) | 54 (14.4%) | 0.312 |
| Emergency presentation | (n = 59) | (n = 67) | (n = 73) | 0.038 |
| Urinary obstruction | 48 (11.4%) | 52 (16.0%) | 55 (14.7%) | |
| Hemorrhagic cystitis | 11 (2.6%) | 15 (4.6%) | 18 (4.8%) | |
| Outcomes | ||||
| Days of hospitalization | 9.8 ± 3.9 | 8.3 ± 4.1 | 8.5 ± 4.0 | <0.001 |
| In-hospital mortality | 13 (3.1%) | 16 (4.9%) | 14 (3.7%) | 0.434 |
| Disease progression at six months | 37 (8.8%) | 35 (10.7%) | 44 (11.7%) | 0.380 |
| Risk Factors | HR | CI | p-Value |
|---|---|---|---|
| Advanced TNM stage (III + IV) | 5.61 | 2.29–6.90 | <0.001 |
| Distant invasion | 5.13 | 3.06–7.08 | <0.001 |
| MIBC type | 2.49 | 1.52–4.26 | 0.001 |
| Emergency hospitalization | 1.32 | 1.04–3.17 | 0.009 |
| Duration of hospitalization | 1.27 | 0.95–2.03 | 0.166 |
| Year of admission (2020) | 1.13 | 0.90–1.76 | 0.183 |
| Year of admission (2021) | 1.04 | 0.87–1.92 | 0.242 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbos, V.; Feciche, B.; Bratosin, F.; Bogdan, I.; Negrean, R.A.; Latcu, S.; Croitor, A.; Dema, V.; Bardan, R.; Cumpanas, A.A. A Retrospective Analysis of the Challenges of Urothelial Cancer Management during the COVID-19 Pandemic at a Single Academic Center in Romania. Healthcare 2023, 11, 812. https://doi.org/10.3390/healthcare11060812
Barbos V, Feciche B, Bratosin F, Bogdan I, Negrean RA, Latcu S, Croitor A, Dema V, Bardan R, Cumpanas AA. A Retrospective Analysis of the Challenges of Urothelial Cancer Management during the COVID-19 Pandemic at a Single Academic Center in Romania. Healthcare. 2023; 11(6):812. https://doi.org/10.3390/healthcare11060812
Chicago/Turabian StyleBarbos, Vlad, Bogdan Feciche, Felix Bratosin, Iulia Bogdan, Rodica Anamaria Negrean, Silviu Latcu, Alexei Croitor, Vlad Dema, Razvan Bardan, and Alin Adrian Cumpanas. 2023. "A Retrospective Analysis of the Challenges of Urothelial Cancer Management during the COVID-19 Pandemic at a Single Academic Center in Romania" Healthcare 11, no. 6: 812. https://doi.org/10.3390/healthcare11060812