
Confinement Situation of the Spanish Population during the Health Crisis of COVID-19: Resilience Mediation Process in the Relationship of Dispositional Optimism and Psychological Well-Being



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Description of the Sample for Economic and Socio-Demographic Data before the State of Alarm
3.2. Sociodemographic and Economic Indicators of Confinement and Their Relationship with Dispositional Optimism, Resilience, and Psychological Well-Being
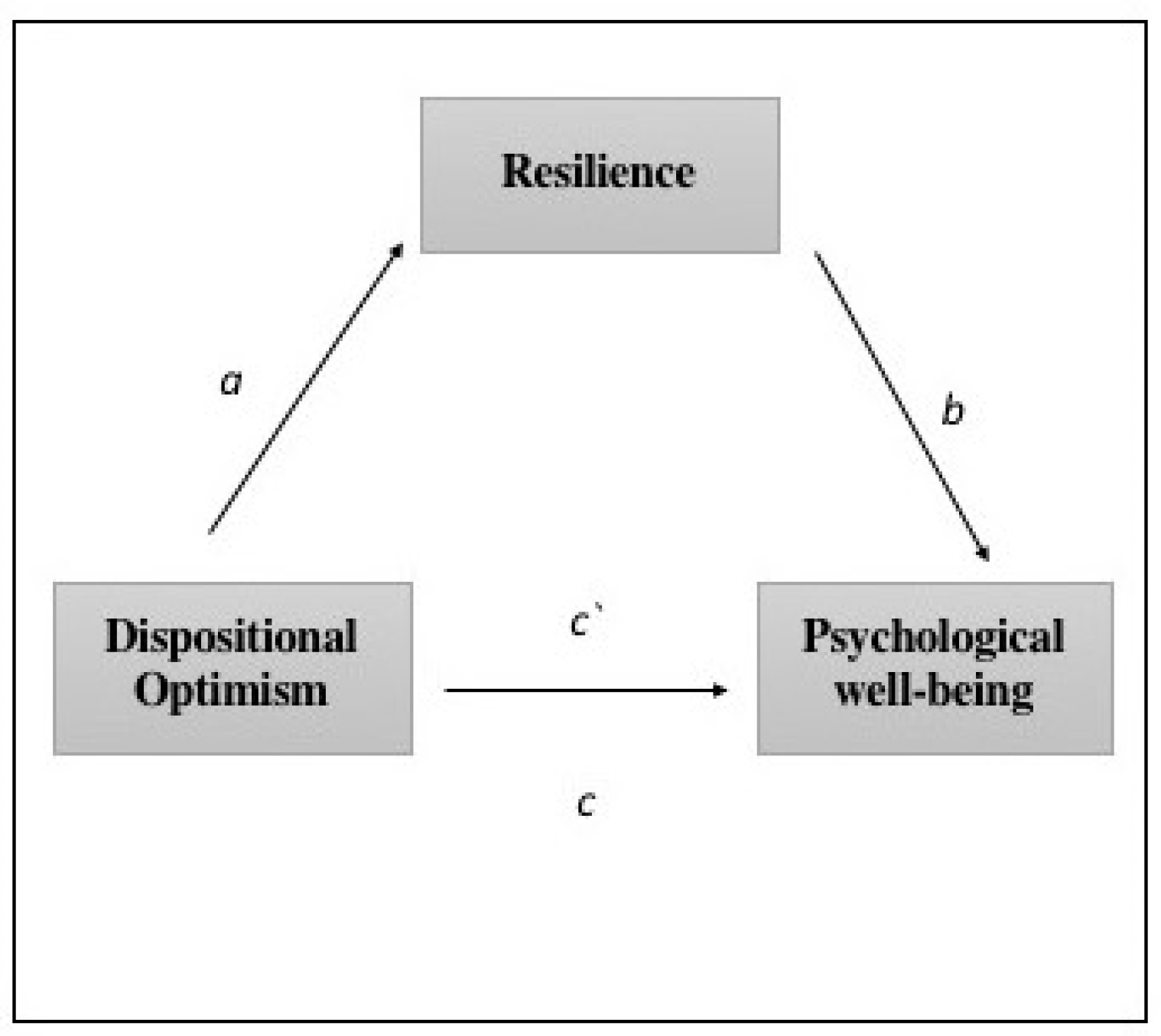
3.3. Analysis of the Resilence Mediation between Optimism and Psychological Well-Being, Controlling for Economic and Sociodemographic Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Coronavirus Disease (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 5 August 2020).
- Centro de Coordinación de Alertas y Emergencias Sanitarias. Enfermedad Por Coronavirus, COVID-19; Ministerio de Sanidad: Madrid, Spain, 2020. [Google Scholar]
- Ministerio de la Presidencia, Relaciones con las Cortes y Memoria Democrática. Real Decreto 463/2020, de 14 de Marzo, Por El Que Se Declara El Estado de Alarma Para La Gestión de La Situación de Crisis Sanitaria Ocasionada Por El COVID-19; Agencia Estatal Boletín Oficial del Estado: Madrid, Spain, 2020. [Google Scholar]
- Sandín, B.; Valiente, R.M.; García-Escalera, J.; Chorot, P. Impacto psicológico de la pandemia de COVID-19: Efectos negativos y positivos en población española asociados al periodo de confinamiento nacional. Rev. Psicopatol. Psicol. Clin. 2020, 25. [Google Scholar] [CrossRef]
- Karasar, B.; Canlı, D. Psychological resilience and depression during the COVID-19 pandemic in Turkey. Psychiatr. Danub. 2020, 32, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.C.; Saletti-Cuesta, L.; Tumas, N. Emociones, preocupaciones y reflexiones frente a la pandemia del COVID-19 en Argentina. Ciência Saúde Coletiva 2020, 25, 2447–2456. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Farre, L.; Fawaz, Y.; Gonzalez, L.; Graves, J. How the COVID-19 Lockdown Affected Gender Inequality in Paid and Unpaid Work in Spain; Social Science Research Network: Rochester, NY, USA, 2020. [Google Scholar]
- Canivet, C.; Bodin, T.; Emmelin, M.; Toivanen, S.; Moghaddassi, M.; Östergren, P.-O. Precarious employment is a risk factor for poor mental health in young individuals in Sweden: A cohort study with multiple follow-ups. BMC Public Health 2016, 16, 687. [Google Scholar] [CrossRef] [Green Version]
- Parrado-González, A.; León-Jariego, J.C. COVID-19: Factores asociados al malestar emocional y morbilidad psíquica en población española. Rev. Esp. Salud Pública 2020, 94, 1–16. [Google Scholar]
- Mohr, G.B. The changing significance of different stressors after the announcement of bankruptcy: A longitudinal investigation with special emphasis on job insecurity. J. Organ. Behav. 2000, 21, 337–359. [Google Scholar] [CrossRef]
- De Witte, H.; Pienaar, J.; De Cuyper, N. Review of 30 Years of Longitudinal Studies on the Association between Job Insecurity and Health and Well-Being. Is There Causal Evidence? Aust. Psychol. 2016, 51, 18–31. [Google Scholar] [CrossRef]
- Cheung, F.; Lucas, R. Income inequality is associated with stronger social comparison effects: The effect of relative income on life satisfaction. J. Pers. Soc. Psychol. 2016, 110, 332–341. [Google Scholar] [CrossRef] [Green Version]
- Gardner, J.; Oswald, A.J. Money and mental wellbeing: A longitudinal study of medium-sized lottery wins. J. Health Econ. 2007, 26, 49–60. [Google Scholar] [CrossRef] [Green Version]
- Diener, E.; Ng, W.; Harter, J.; Arora, R. Wealth and happiness across the world: Material prosperity predicts life evaluation, whereas psychosocial prosperity predicts positive feeling. J. Pers. Soc. Psychol. 2010, 99, 52–61. [Google Scholar] [CrossRef] [Green Version]
- Shaw, M. Housing and Public Health. Annu. Rev. Public Health 2004, 25, 397–418. [Google Scholar] [CrossRef] [Green Version]
- Seligman, M.E.P. Positive psychology, positive prevention, and positive therapy. In Handbook of Positive Psychology; Snyder, C.R., Lopez, S.J., Eds.; Oxford University Press: Oxford, UK, 2002. [Google Scholar]
- Seligman, M.E.P.; Csikszentmihalyi, M. Positive psychology: An introduction. In Flow and the Foundations of Positive Psychology; Springer: Berlin/Heidelberg, Germany, 2014; pp. 279–298. [Google Scholar]
- Scheier, M.F.; Carver, C.S. Optimism, Coping, and Health: Assessment and Implications of Generalized Outcome Expectancies. Health Psychol. 1985, 4, 219. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F. Dispositional optimism. Trends Cogn. Sci. 2014, 18, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, H.N.; Scheier, M.F.; Greenhouse, J.B. Optimism and Physical Health: A Meta-analytic Review. Ann. Behav. Med. 2009, 37, 239–256. [Google Scholar] [CrossRef] [Green Version]
- Sardella, A.; Lenzo, V.; Alibrandi, A.; Catalano, A.; Corica, F.; Quattropani, M.; Basile, G. A Clinical Bridge between Family Caregivers and Older Adults: The Contribution of Patients’ Frailty and Optimism on Caregiver Burden. Int. J. Environ. Res. Public Health 2021, 18, 3406. [Google Scholar] [CrossRef] [PubMed]
- Sardella, A.; Lenzo, V.; Bonanno, G.; Basile, G.; Quattropani, M. Expressive Flexibility and Dispositional Optimism Contribute to the Elderly’s Resilience and Health-Related Quality of Life during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 1698. [Google Scholar] [CrossRef] [PubMed]
- Luthar, S.S. Resilience in development: A synthesis of research across five decades. In Developmental Psychopathology: Risk, Disorder and Adaptation, 2nd ed.; Wiley: New York, NY, USA, 2006; Volume 3, pp. 739–795. [Google Scholar]
- Lemery-Chalfant, K.; Reich, J.W.; Zautra, A.J.; Hall, J.S. Genes and environments: How they work together to promote resilience. In Handbook of Adult Resilience; Guilford Press: New York, NY, USA, 2010; pp. 55–78. [Google Scholar]
- Wagnild, G. A Review of the Resilience Scale. J. Nurs. Meas. 2009, 17, 105–113. [Google Scholar] [CrossRef] [PubMed]
- He, F.; Cao, R.; Feng, Z.; Guan, H.; Peng, J. The Impacts of Dispositional Optimism and Psychological Resilience on the Subjective Well-Being of Burn Patients: A Structural Equation Modelling Analysis. PLoS ONE 2013, 8, e82939. [Google Scholar] [CrossRef]
- Kapikiran, N.A. Positive and Negative Affectivity as Mediator and Moderator of the Relationship between Optimism and Life Satisfaction in Turkish University Students. Soc. Indic. Res. 2012, 106, 333–345. [Google Scholar] [CrossRef]
- Jung, J.Y.; Oh, Y.H.; Oh, K.S.; Suh, D.W.; Shin, Y.C.; Kim, H.J. Positive-Thinking and Life Satisfaction amongst Koreans. Yonsei Med. J. 2007, 48, 371–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, B.W.-C.; Moneta, G.B.; McBride-Chang, C. Think Positively and Feel Positively: Optimism and Life Satisfaction in Late Life. Int. J. Aging Hum. Dev. 2005, 61, 335–365. [Google Scholar] [CrossRef]
- Bosze, J.P.; Köteles, F.; Komlósi, F.; Boros, S.; Szabo, A. Positive life-event expectancies are associated with greater optimism, well-being and emotional intelligence. Cogn. Brain Behav. 2020, 24, 139–152. [Google Scholar] [CrossRef]
- Samani, S.; Jokar, B.; Sahragard, N. Effects of Resilience on Mental Health and Life Satisfaction. Iran. J. Psychiatry Clin. Psychol. 2007, 13, 290–295. [Google Scholar]
- Ghanei-Gheshlagh, R.; Sayehmiri, K.; Ebadi, A.; Dalvandi, A.; Dalvand, S.; Maddah, S.S.B.; Tabrizi, K.N. The Relationship between Mental Health and Resilience: A Systematic Review and Meta-Analysis. Iran. Red Crescent Med. J. 2017, 19. [Google Scholar] [CrossRef] [Green Version]
- Pérez Viejo, J.M.; Dorado Barbé, A.; Pérez, R.-B.; del Mar, M.; López Pérez, J. Resiliencia Para La Promoción de La Salud En La Crisis Covid-19 En España. Rev. Cienc. Soc. 2020, 26, 52–63. [Google Scholar]
- Justo-Alonso, A.; García-Dantas, A.; González-Vázquez, A.I.; Sánchez-Martín, M.; Del Río-Casanova, L. How did Different Generations Cope with the COVID-19 Pandemic? Early Stages of the Pandemic in Spain. Psicothema 2020, 32, 490–500. [Google Scholar] [PubMed]
- Kamel, S.D.-E.; Hentati, Y. Portrait of resilience among Tunisians locked down in times of COVID-19. Traumatology 2021, 27, 70–77. [Google Scholar] [CrossRef]
- Robles-Bello, M.A.; Sánchez-Teruel, D.; Naranjo, N.V. Variables protecting mental health in the Spanish population affected by the COVID-19 pandemic. Curr. Psychol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Goldbach, C.; Knutson, D.; Milton, D.C. LGBTQ+ people and COVID-19: The importance of resilience during a pandemic. Psychol. Sex. Orientat. Gend. Divers. 2020. [Google Scholar] [CrossRef]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the Resilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar]
- Ferrando, P.J.; Chico, E.; Tous, J.M. Propiedades Psicométricas Del Test de Optimismo Life Orientation Test. Psicothema 2002, 14, 673–680. [Google Scholar]
- Ryff, C.D.; Singer, B. The Contours of Positive Human Health. Psychol. Inq. 1998, 9, 1–28. [Google Scholar] [CrossRef]
- Van Dierendonck, D. The construct validity of Ryff’s Scales of Psychological Well-being and its extension with spiritual well-being. Pers. Individ. Differ. 2004, 36, 629–643. [Google Scholar] [CrossRef]
- Díaz, D.; Rodríguez-Carvajal, R.; Blanco, A.; Moreno-Jiménez, B.; Gallardo, I.; Valle, C.; Van Dierendonck, D. Adaptación Española de Las Escalas de Bienestar Psicológico de Ryff. Psicothema 2006, 18, 572–577. [Google Scholar] [PubMed]
- Hayes, A.F. Model Templates for PROCESS for SPSS and SAS; Guilford: New York, NY, USA, 2013. [Google Scholar]
- Instituto Nacional de Estadística Sección Prensa/Encuesta de Población Activa (EPA). Available online: https://www.ine.es/prensa/epa_prensa.htm (accessed on 6 August 2020).
- Ozamiz-Etxebarria, N.; Idoiaga Mondragon, N.; Dosil Santamaría, M.; Picaza Gorrotxategi, M. Psychological Symptoms during the Two Stages of Lockdown in Response to the COVID-19 Outbreak: An Investigation in a Sample of Citizens in Northern Spain. Front. Psychol. 2020, 11, 1491. [Google Scholar] [CrossRef] [PubMed]
- Shigemura, J.; Ursano, R.J.; Morganstein, J.; Kurosawa, M.; Benedek, D.M. Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: Mental health consequences and target populations. Psychiatry Clin. Neurosci. 2020, 74, 281–282. [Google Scholar] [CrossRef]
- Wild, J.; El-Salahi, S.; Degli Esposti, M. The Effectiveness of Interventions Aimed at Improving Well-Being and Resilience to Stress in First Responders. Eur. Psychol. 2020, 25, 252–271. [Google Scholar] [CrossRef]
- Kunzler, A.M.; Helmreich, I.; Chmitorz, A.; König, J.; Binder, H.; Wessa, M.; Lieb, K. Psychological interventions to foster resilience in healthcare professionals. Cochrane Database Syst. Rev. 2020, 7, CD012527. [Google Scholar] [CrossRef] [PubMed]
- Sánchez Hernández, O.; Canales, A. Eficacia y Satisfacción Del Programa Resiliencia y Bienestar: Quédate En Casa. Rev. Psicoter. 2020, 31, 381–398. [Google Scholar] [CrossRef]


{kind=link}
| Socio-Demographic Variables | n | % | Economic Variables | n | % |
|---|---|---|---|---|---|
| Gender | Employment situation | ||||
| Woman | 416 | 73.5 | Unemployment | 154 | 27.4 |
| Man | 150 | 26.5 | Freelance with hired staff | 14 | 2.49 |
| Marital Status | Freelance without hired staff | 25 | 4.45 | ||
| Single | 266 | 47 | Hired in general temporary regime | 94 | 16.73 |
| De facto couple | 35 | 6.18 | Hired in an indefinite general regime | 160 | 28.47 |
| Married | 213 | 37.63 | Official | 85 | 15.12 |
| Widowed | 11 | 1.94 | Seasonal self-employed summer season | 2 | 0.36 |
| Divorced | 41 | 7.2 | Retirement | 28 | 4.98 |
| Level of studies (completed) | Leave | 4 | 0.71 | ||
| No studies | 1 | 0.18 | Monthly Income level | ||
| Primary Studies | 21 | 3.71 | Less than 500 € | 19 | 3.36 |
| Secondary Studies | 188 | 33.2 | Between 500–1000 € | 56 | 9.89 |
| University Studies | 242 | 42.76 | Between 1000–1500 € | 133 | 23.5 |
| Postgraduate studies | 76 | 13.43 | Between 1500–2000 € | 102 | 18.02 |
| Doctorate Program | 38 | 6.71 | Between 2000–2500 € | 96 | 16.96 |
| More than 2500 € | 160 | 28.27 |
| Resilience | Dispositional Optimism | Psychological Well-Being | ||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Category | n | M | SD | M | SD | M | SD |
| Gender | Woman | 416 | 138.14 | 18.16 | 22.02 | 4.37 | 178.52 | 25.02 |
| Man | 150 | 138.99 | 17.93 | 22.32 | 4.22 | 176.39 | 26.39 | |
| Z | −0.698 | −0.553 | −0.528 | |||||
| p | 0.485 | 0.580 | 0.598 | |||||
| Marital Status | Unmarried (single and de facto couple) | 301 | 136.72 | 18.36 | 21.81 | 4.50 | 175.62 | 26.21 |
| Marrried/Widowed/Divorced | 265 | 140.22 | 17.63 | 22.43 | 4.10 | 180.61 | 24.18 | |
| Z | −2.497 | −1.361 | −2.311 | |||||
| p | 0.013 * | 0.173 | 0.021 * | |||||
| Level of studies | No studies/Primary Studies | 22 | 142.18 | 20.13 | 20.32 | 3.39 | 171.55 | 22.23 |
| Secondary Studies | 188 | 137.84 | 18.79 | 21.77 | 4.81 | 177.61 | 26.70 | |
| University Studies | 242 | 137.41 | 18.15 | 22.12 | 4.24 | 176.08 | 25.85 | |
| Postgraduate studies | 76 | 139.12 | 16.80 | 23.08 | 3.72 | 182.26 | 20.99 | |
| Doctorate Program | 38 | 143.26 | 14.84 | 22.66 | 3.57 | 186.74 | 23.30 | |
| H | 4.521 | 10.004 | 11.181 | |||||
| p | 0.340 | 0.040 * | 0.025 * | |||||
| Change in Employment situation | No | 398 | 138.47 | 17.94 | 22.09 | 4.29 | 178.15 | 24.93 |
| Yes | 168 | 138.10 | 18.48 | 22.11 | 4.44 | 177.50 | 26.51 | |
| Z | −0.210 | −0.097 | −0.155 | |||||
| p | 0.833 | 0.923 | 0.877 | |||||
| Change in income. | No | 336 | 139.15 | 18.17 | 22.29 | 4.31 | 179.12 | 24.92 |
| Yes | 230 | 137.21 | 17.94 | 21.82 | 4.35 | 176.26 | 26.01 | |
| Z | −1.071 | −1.279 | −1.083 | |||||
| p | 0.284 | 0.201 | 0.279 | |||||
| People you live with | Only | 55 | 138.02 | 17.58 | 22.53 | 4.07 | 173.58 | 27.70 |
| 1 | 151 | 140.40 | 17.91 | 22.39 | 4.43 | 179.84 | 27.01 | |
| 2 | 145 | 138.77 | 18.95 | 21.98 | 4.21 | 177.94 | 24.46 | |
| 3 | 142 | 136.58 | 16.88 | 22.11 | 4.35 | 179.51 | 21.92 | |
| >3 | 73 | 137.07 | 19.34 | 21.40 | 4.50 | 174.36 | 28.01 | |
| H | 3.979 | 2.510 | 3.907 | |||||
| p | 0.409 | 0.643 | 0.419 | |||||
| Housing meters | <60 | 51 | 133.63 | 20.61 | 21.12 | 4.67 | 171.55 | 28.63 |
| 60–90 | 200 | 138.84 | 16.76 | 22.07 | 4.21 | 177.23 | 23.33 | |
| 90–120 | 178 | 139.59 | 18.27 | 22.79 | 3.96 | 180.24 | 26.01 | |
| 120–150 | 62 | 136.18 | 16.61 | 20.97 | 4.86 | 179.66 | 23.80 | |
| >150 | 75 | 139.20 | 20.12 | 22.15 | 4.54 | 177.43 | 27.77 | |
| H | 6.329 | 9.506 | 6.893 | |||||
| p | 0.176 | 0.050 * | 0.142 | |||||
| Housing having open air | No | 177 | 136.63 | 18.33 | 21.64 | 4.36 | 174.32 | 24.42 |
| Yes | 389 | 139.15 | 17.94 | 22.31 | 4.30 | 179.61 | 25.67 | |
| Z | −1.881 | −1.901 | −2.646 | |||||
| p | 0.060 | 0.057 | 0.008 ** | |||||
| Correlation | |||
|---|---|---|---|
| 1 | 2 | 3 | |
| 1. Age | - | ||
| 2. Resilience | 0.157 ** | - | |
| 3. Dispositional optimism | 0.116 ** | 0.465 ** | |
| 4. Psychological well-being | 0.102 * | 0.683 ** | 0.652 ** |
| IC 95% | |||||
|---|---|---|---|---|---|
| Effects | Path | Coeff | SE | LLCI | ULCI |
| Direct between optimism and resilience | a | 2.101 | 0.1536 | 1.799 | 2.403 |
| Direct between resilience and psychological well-being | b | 0.721 | 0.0419 | 0.639 | 0.803 |
| Direct between optimism and psychological well-being | c' | 2.345 | 0.1757 | 1.999 | 2.689 |
| Total effect between optimism and psychological well-being | c | 3.859 | 0.1880 | 3.490 | 4.229 |
| Indirect effects | Effect | SE | BootLLCI | BootULCI | |
| Total indirect effect | 1.515 | 0.156 | 1.224 | 1.833 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zayas, A.; Merchán-Clavellino, A.; López-Sánchez, J.A.; Guil, R. Confinement Situation of the Spanish Population during the Health Crisis of COVID-19: Resilience Mediation Process in the Relationship of Dispositional Optimism and Psychological Well-Being. Int. J. Environ. Res. Public Health 2021, 18, 6190. https://doi.org/10.3390/ijerph18126190
Zayas A, Merchán-Clavellino A, López-Sánchez JA, Guil R. Confinement Situation of the Spanish Population during the Health Crisis of COVID-19: Resilience Mediation Process in the Relationship of Dispositional Optimism and Psychological Well-Being. International Journal of Environmental Research and Public Health. 2021; 18(12):6190. https://doi.org/10.3390/ijerph18126190
Chicago/Turabian StyleZayas, Antonio, Ana Merchán-Clavellino, José Antonio López-Sánchez, and Rocío Guil. 2021. "Confinement Situation of the Spanish Population during the Health Crisis of COVID-19: Resilience Mediation Process in the Relationship of Dispositional Optimism and Psychological Well-Being" International Journal of Environmental Research and Public Health 18, no. 12: 6190. https://doi.org/10.3390/ijerph18126190