
Acute Mesenteric Ischemia in COVID-19 Patients

 , , , ,
, , , ,
Abstract
:1. Introduction
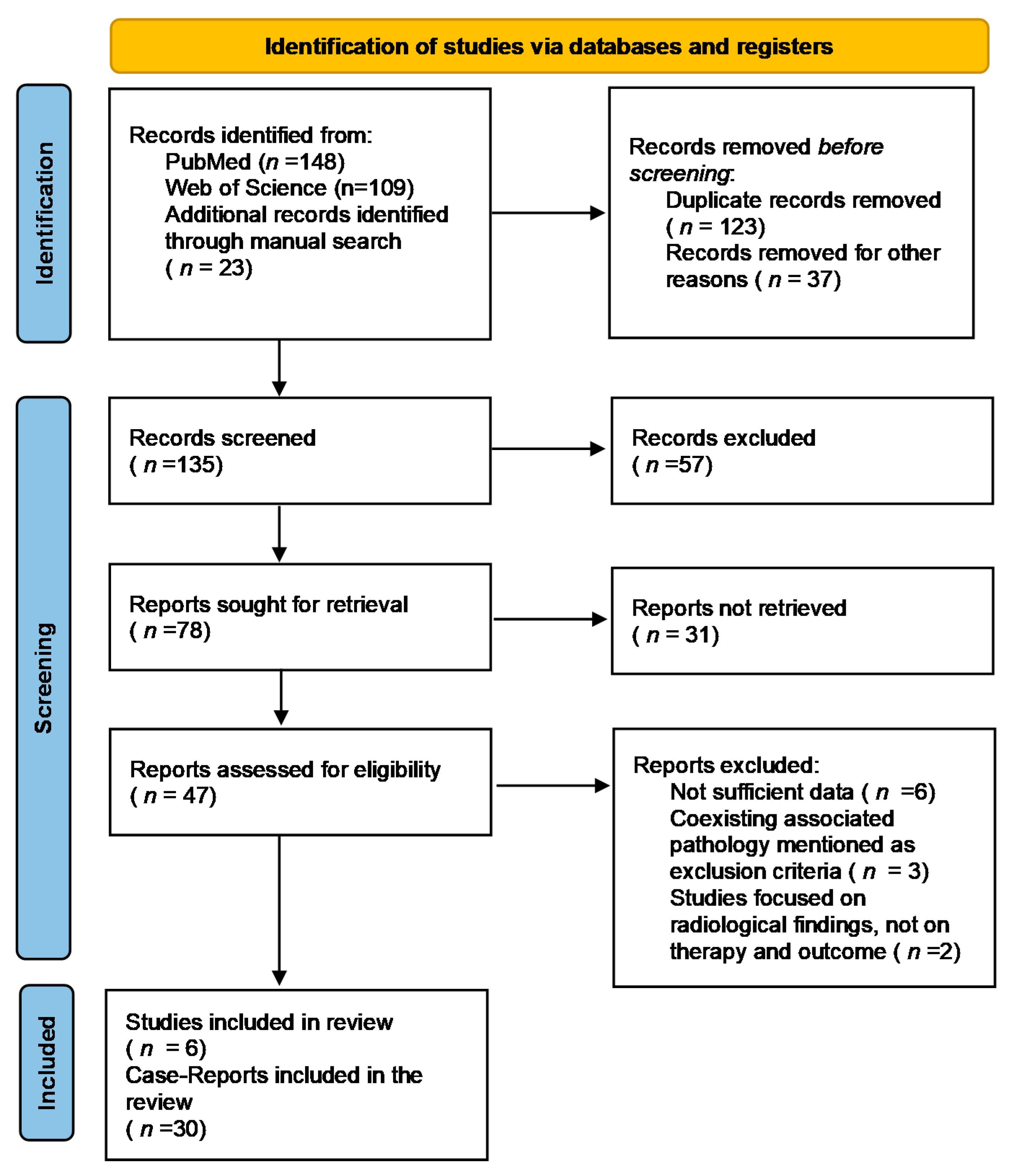
2. Materials and Methods
2.1. Data Extraction and Analysis
2.2. Risk of Bias
3. Results
3.1. Risk Factors of Intestinal Ischemia in COVID-19 Patients
3.2. Clinical Features in COVID-19 Patients with Acute Mesenteric Ischemia
3.3. Imagistic and Lab Test Findings
3.4. Management and Outcomes
4. Discussions
4.1. Pathogenic Pathways of Mesenteric Ischemia in COVID-19 Patients
4.2. Question Still to Be Answered
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bala, M.; Kashuk, J.; Moore, E.E.; Kluger, Y.; Biffl, W.; Gomes, C.A.; Ben-Ishay, O.; Rubinstein, C.; Balogh, Z.J.; Civil, I.; et al. Acute mesenteric ischemia: Guidelines of the World Society of Emergency Surgery. World J. Emerg. Surg. 2017, 12, 38. [Google Scholar] [CrossRef] [Green Version]
- Dumic, I.; Martin, S.; Salfiti, N.; Watson, R.; Alempijevic, T. Deep Venous Thrombosis and Bilateral Pulmonary Embolism Revealing Silent Celiac Disease: Case Report and Review of the Literature. Case Rep. Gastrointest. Med. 2017, 2017, 5236918. [Google Scholar] [CrossRef] [PubMed]
- Akhrass, F.A.; Abdallah, L.; Berger, S.; Sartawi, R. Gastrointestinal variant of Lemierre’s syndrome complicating ruptured appendicitis. IDCases 2015, 2, 72–76. [Google Scholar] [CrossRef] [Green Version]
- Radovanovic, N.; Dumic, I.; Veselinovic, M.; Burger, S.; Milovanovic, T.; Nordstrom, C.W.; Niendorf, E.; Ramanan, P. Fusobacterium necrophorum subsp. necrophorum Liver Abscess with Pylephlebitis: An Abdominal Variant of Lemierre’s Syndrome. Case Rep. Infect. Dis. 2020, 2020, 9237267. [Google Scholar] [CrossRef] [Green Version]
- Sogaard, K.K.; Astrup, L.B.; Vilstrup, H.; Gronbaek, H. Portal vein thrombosis; risk factors, clinical presentation and treatment. BMC Gastroenterol. 2007, 7, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moradi, H.; Mouzannar, S.; Miratashi Yazdi, S.A. Post COVID-19 splenic infarction with limb ischemia: A case report. Ann. Med. Surg. 2021, 71, 102935. [Google Scholar] [CrossRef] [PubMed]
- Elmunzer, B.J.; Spitzer, R.L.; Foster, L.D.; Merchant, A.A.; Howard, E.F.; Patel, V.A.; West, M.K.; Qayed, E.; Nustas, R.; Zakaria, A.; et al. North American Alliance for the Study of Digestive Manifestations of COVID-19. Digestive Manifestations in Patients Hospitalized With Coronavirus Disease 2019. Clin. Gastroenterol. Hepatol. 2021, 19, 1355–1365.e4. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Estevez-Cerda, S.C.; Saldaña-Rodríguez, J.A.; Alam-Gidi, A.G.; Riojas-Garza, A.; Rodarte-Shade, M.; Velazco-de la Garza, J.; Leyva-Alvizo, A.; Gonzalez-Ruvalcaba, R.; Martinez-Resendez, M.F.; Ortiz de Elguea-Lizarraga, J.I. Severe bowel complications in SARS-CoV-2 patients receiving protocolized care. Rev. Gastroenterol. Mex. Engl. Ed. 2021, 86, 378–386. [Google Scholar] [CrossRef]
- Redd, W.D.; Zhou, J.C.; Hathorn, K.E. Prevalence and characteristics of gastrointestinal symptoms in patients with SARS-CoV-2 infection in the United States: A multicenter cohort study. Gastroenterology 2020, 159, 765–767.e2. [Google Scholar] [CrossRef]
- Hajifathalian, K.; Krisko, T.; Mehta, A. Gastrointestinal and hepatic manifestations of 2019 novel coronavirus disease in a large cohort of infected patients from New York: Clinical implications. Gastroenterology 2020, 159, 1137–1140.e2. [Google Scholar] [CrossRef]
- Kotfis, K.; Skonieczna-Żydecka, K. COVID-19: Gastrointestinal symptoms and potential sources of SARS-CoV-2 transmission. Anaesthesiol. Intensive Ther. 2020, 52, 171–172. [Google Scholar] [CrossRef]
- Xiao, F.; Tang, M.; Zheng, X. Evidence for gastrointestinal infection of SARS-CoV-2. Gastroenterology 2020, 158, 1831–1833. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Li, X.; Zhu, B.; Liang, H.; Fang, C.; Gong, Y.; Guo, Q.; Sun, X.; Zhao, D.; Shen, J.; et al. Characteristics of pediatric SARS-CoV-2 infection and potential evidence for persistent fecal viral shedding. Nat. Med. 2020, 26, 502–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludewig, S.; Jarbouh, R.; Ardelt, M.; Mothes, H.; Rauchfuß, F.; Fahrner, R.; Zanow, J.; Settmacher, U. Bowel Ischemia in ICU Patients: Diagnostic Value of I-FABP Depends on the Interval to the Triggering Event. Gastroenterol. Res. Pract. 2017, 2795176. [Google Scholar] [CrossRef] [Green Version]
- Kaafarani, H.; El Moheb, M.; Hwabejire, J.O.; Naar, L.; Christensen, M.A.; Breen, K.; Gaitanidis, A.; Alser, O.; Mashbari, H.; Bankhead-Kendall, B.; et al. Gastrointestinal Complications in Critically Ill Patients With COVID-19. Ann. Surg. 2020, 272, e61–e62. [Google Scholar] [CrossRef]
- Kraft, M.; Pellino, G.; Jofra, M.; Sorribas, M.; Solís-Peña, A.; Biondo, S.; Espín-Basany, E. Incidence, features, outcome and impact on health system of de-novo abdominal surgical diseases in patients admitted with COVID-19. Surg. J. R. Coll. Surg. Edinb. Irel. 2021, 19, e53–e58. [Google Scholar] [CrossRef]
- Yang, C.; Hakenberg, P.; Weiß, C.; Herrle, F.; Rahbari, N.; Reißfelder, C.; Hardt, J. Colon ischemia in patients with severe COVID-19: A single-center retrospective cohort study of 20 patients. Int. J. Colorectal Dis. 2021, 36, 2769–2773. [Google Scholar] [CrossRef]
- Hwabejire, J.O.; Kaafarani, H.M.; Mashbari, H.; Misdraji, J.; Fagenholz, P.J.; Gartland, R.M.; Abraczinskas, D.R.; Mehta, R.S.; Paranjape, C.N.; Eng, G.; et al. Bowel Ischemia in COVID-19 Infection: One-Year Surgical Experience. Am. Surg. 2021, 87, 1893–1900. [Google Scholar] [CrossRef] [PubMed]
- O’shea, A.; Parakh, A.; Hedgire, S.; Lee, S.I. Multisystem assessment of the imaging manifestations of coagulopathy in hospitalized patients with coronavirus. Am. J. Roentgenol. 2021, 216, 1088–1098. [Google Scholar] [CrossRef] [PubMed]
- Qayed, E.; Deshpande, A.R.; Elmunzer, B.J.; North American Alliance for the Study of Digestive Manifestations of COVID-19. Low Incidence of Severe Gastrointestinal Complications in COVID-19 Patients Admitted to the Intensive Care Unit: A Large, Multicenter Study. Gastroenterology 2021, 160, 1403–1405. [Google Scholar] [CrossRef] [PubMed]
- Azouz, E.; Yang, S.; Monnier-Cholley, L.; Arrivé, L. Systemic arterial thrombosis and acute mesenteric ischemia in a patient with COVID-19. Intensive Care Med. 2020, 46, 1464–1465. [Google Scholar] [CrossRef] [PubMed]
- Al Mahruqi, G.; Stephen, E.; Abdelhedy, I.; Al Wahaibi, K. Our early experience with mesenteric ischemia in COVID-19 positive patients. Ann. Vasc. Surg. 2021, 73, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Ucpinar, B.A.; Sahin, C. Superior Mesenteric Artery Thrombosis in a Patient with COVID-19: A Unique Presentation. J. Coll Physicians Surg. Pak. 2020, 30, 112–114. [Google Scholar] [CrossRef]
- Karna, S.T.; Panda, R.; Maurya, A.P.; Kumari, S. Superior Mesenteric Artery Thrombosis in COVID-19 Pneumonia: An Underestimated Diagnosis—First Case Report in Asia. Indian J. Surg. 2020, 82, 1235–1237. [Google Scholar] [CrossRef]
- Abeysekera, K.W.; Karteszi, H.; Clark, A.; Gordon, F.H. Spontaneous portomesenteric thrombosis in a non-cirrhotic patient with SARS-CoV-2 infection. BMJ Case Rep. 2020, 13, e238906. [Google Scholar] [CrossRef]
- Rodriguez-Nakamura, R.M.; Gonzalez-Calatayud, M.; Martinez Martinez, A.R. Acute mesenteric thrombosis in two patients with COVID-19. Two cases report and literature review. Int. J. Surg. Case Rep. 2020, 76, 409–414. [Google Scholar] [CrossRef]
- Dinoto, E.; Ferlito, F.; La Marca, M.A.; Mirabella, D.; Bajardi, G.; Pecoraro, F. Staged acute mesenteric and peripheral ischemia treatment in COVID-19 patient: Case report. Int. J. Surg. Case Rep. 2021, 84, 106105. [Google Scholar] [CrossRef]
- Kiwango, F.; Mremi, A.; Masenga, A.; Akrabi, H. Intestinal ischemia in a COVID-19 patient: Case report from Northern Tanzania. J. Surg. Case Rep. 2021, 2021, rjaa537. [Google Scholar] [CrossRef]
- Sevella, P.; Rallabhandi, S.; Jahagirdar, V.; Kankanala, S.R.; Ginnaram, A.R.; Rama, K. Acute Mesenteric Ischemia as an Early Complication of COVID-19. Cureus 2021, 13, e18082. [Google Scholar] [CrossRef]
- Nasseh, S.; Trabelsi, M.M.; Oueslati, A.; Haloui, N.; Jerraya, H.; Nouira, R. COVID-19 and gastrointestinal symptoms: A case report of a Mesenteric Large vessel obstruction. Clin. Case Rep. 2021, 9, e04235. [Google Scholar] [CrossRef] [PubMed]
- Alemán, W.; Cevallos, L.C. Subacute mesenteric venous thrombosis secondary to COVID-19: A late thrombotic complication in a nonsevere patient. Radiol. Case Rep. 2021, 16, 899–902. [Google Scholar] [CrossRef] [PubMed]
- Jeilani, M.; Hill, R.; Riad, M.; Abdulaal, Y. Superior mesenteric vein and portal vein thrombosis in a patient with COVID-19: A rare case. BMJ Case Rep. 2021, 14, e244049. [Google Scholar] [CrossRef]
- Randhawa, J.; Kaur, J.; Randhawa, H.S.; Kaur, S.; Singh, H. Thrombosis of the Portal Vein and Superior Mesenteric Vein in a Patient With Subclinical COVID-19 Infection. Cureus 2021, 13, e14366. [Google Scholar] [CrossRef] [PubMed]
- Cheung, S.; Quiwa, J.C.; Pillai, A.; Onwu, C.; Tharayil, Z.J.; Gupta, R. Superior Mesenteric Artery Thrombosis and Acute Intestinal Ischemia as a Consequence of COVID-19 Infection. Am. J. Case Rep. 2020, 21, e925753. [Google Scholar] [CrossRef]
- Beccara, L.A.; Pacioni, C.; Ponton, S.; Francavilla, S.; Cuzzoli, A. Arterial Mesenteric Thrombosis as a Complication of SARS-CoV-2 Infection. Eur. J. Case Rep. Intern. Med. 2020, 7, 001690. [Google Scholar] [CrossRef] [PubMed]
- Vulliamy, P.; Jacob, S.; Davenport, R.A. Acute aorto-iliac and mesenteric arterial thromboses as presenting features of COVID-19. Br. J. Haematol. 2020, 189, 1053–1054. [Google Scholar] [CrossRef]
- De Barry, O.; Mekki, A.; Diffre, C.; Seror, M.; El Hajjam, M.; Carlier, R.Y. Arterial and venous abdominal thrombosis in a 79-year-old woman with COVID-19 pneumonia. Radiol. Case Rep. 2020, 15, 1054–1057. [Google Scholar] [CrossRef]
- Romero, M.D.C.V.; Cárdenas, A.M.; Fuentes, A.B.; Barragán, A.A.S.; Gómez, D.B.S.; Jiménez, M.T. Acute mesenteric arterial thrombosis in severe SARS-Co-2 patient: A case report and literature review. Int. J. Surg. Case Rep. 2021, 86, 106307. [Google Scholar] [CrossRef]
- Posada-Arango, A.M.; García-Madrigal, J.; Echeverri-Isaza, S.; Alberto-Castrillón, G.; Martínez, D.; Gómez, A.C.; Pinto, J.A.; Pinillos, L. Thrombosis in abdominal vessels associated with COVID-19 Infection: A report of three cases. Radiol. Case Rep. 2021, 16, 3044–3050. [Google Scholar] [CrossRef]
- Pang, J.H.Q.; Tang, J.H.; Eugene-Fan, B. A peculiar case of small bowel stricture in a coronavirus disease 2019 patient with congenital adhesion band and superior mesenteric vein thrombosis. Ann. Vasc. Surg. 2021, 70, 286–289. [Google Scholar] [CrossRef]
- Lari, E.; Lari, A.; AlQinai, S. Severe ischemic complications in COVID-19-a case series. Int. J. Surg. Case Rep. 2020, 75, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Carmo Filho, A.; Cunha, B.D.S. Inferior mesenteric vein thrombosis and COVID-19. Rev. Soc. Bras. Med. Trop. 2020, 53, e20200412. [Google Scholar] [CrossRef]
- Hanif, M.; Ahmad, Z.; Khan, A.W.; Naz, S.; Sundas, F. COVID-19-Induced Mesenteric Thrombosis. Cureus 2021, 13, e12953. [Google Scholar] [CrossRef]
- Amaravathi, U.; Balamurugan, N.; Muthu Pillai, V.; Ayyan, S.M. Superior Mesenteric Arterial and Venous Thrombosis in COVID-19. J. Emerg. Med. 2021, 60, e103–e107. [Google Scholar] [CrossRef] [PubMed]
- Goodfellow, M.; Courtney, M.; Upadhyay, Y.; Marsh, R.; Mahawar, K. Mesenteric Venous Thrombosis Due to Coronavirus in a Post Roux-en-Y Gastric Bypass Patient: A Case Report. Obes. Surg. 2021, 31, 2308–2310. [Google Scholar] [CrossRef] [PubMed]
- Plotz, B.; Castillo, R.; Melamed, J.; Magro, C.; Rosenthal, P.; Belmont, H.M. Focal small bowel thrombotic microvascular injury in COVID-19 mediated by the lectin complement pathway masquerading as lupus enteritis. Rheumatology 2021, 60, e61–e63. [Google Scholar] [CrossRef]
- Chiu, C.Y.; Sarwal, A.; Mon, A.M.; Tan, Y.E.; Shah, V. Gastrointestinal: COVID-19 related ischemic bowel disease. J. Gastroenterol. Hepatol. 2021, 36, 850. [Google Scholar] [CrossRef] [PubMed]
- Farina, D.; Rondi, P.; Botturi, E.; Renzulli, M.; Borghesi, A.; Guelfi, D.; Ravanelli, M. Gastrointestinal: Bowel ischemia in a suspected coronavirus disease (COVID-19) patient. J. Gastroenterol. Hepatol. 2021, 36, 41. [Google Scholar] [CrossRef]
- Singh, B.; Mechineni, A.; Kaur, P.; Ajdir, N.; Maroules, M.; Shamoon, F.; Bikkina, M. Acute Intestinal Ischemia in a Patient with COVID-19 Infection. Korean J. Gastroenterol. 2020, 76, 164–166. [Google Scholar] [CrossRef]
- Nakatsutsumi, K.; Endo, A.; Okuzawa, H.; Onishi, I.; Koyanagi, A.; Nagaoka, E.; Morishita, K.; Aiboshi, J.; Otomo, Y. Colon perforation as a complication of COVID-19: A case report. Surg. Case Rep. 2021, 7, 175. [Google Scholar] [CrossRef]
- Carubbi, F.; Salvati, L.; Alunno, A.; Maggi, F.; Borghi, E.; Mariani, R.; Mai, F.; Paoloni, M.; Ferri, C.; Desideri, G.; et al. Ferritin is associated with the severity of lung involvement but not with worse prognosis in patients with COVID-19: Data from two Italian COVID-19 units. Sci. Rep. 2021, 11, 4863. [Google Scholar] [CrossRef]
- Isfordink, C.J.; Dekker, D.; Monkelbaan, J.F. Clinical value of serum lactate measurement in diagnosing acute mesenteric ischaemia. Neth. J. Med. 2018, 76, 60–64. [Google Scholar] [PubMed]
- Montagnana, M.; Danese, E.; Lippi, G. Biochemical markers of acute intestinal ischemia: Possibilities and limitations. Ann. Transl. Med. 2018, 6, 341. [Google Scholar] [CrossRef]
- Matsumoto, S.; Sekine, K.; Funaoka, H.; Yamazaki MShimizu, M.; Hayashida, K.; Kitano, M. Diagnostic performance of plasma biomarkers in patients with acute intestinal ischaemia. Br. J. Surg. 2014, 101, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Soni, N.; Bhutra, S.; Vidyarthi, S.H.; Sharma, V. Role of serum lactic dehydrogenase, glutamic oxaloacetic transaminase, creatine phosphokinase, alkaline phospatase, serum phosphorus in the cases of bowel Ischaemia in acute abdomen. Int. Surg. J. 2017, 4, 1997–2001. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.; Zhang, H.; Mu, S.; Wei, W.; Jin, C.; Tong, C.; Song, Z.; Zha, Y.; Xue, Y.; Gu, G. Lactate dehydrogenase, an independent risk factor of severe COVID-19 patients: A retrospective and observational study. Aging 2020, 12, 11245–11258. [Google Scholar] [CrossRef]
- Carpenè, G.; Onorato, D.; Nocini, R.; Fortunato, G.; Rizk, J.G.; Henry, B.M.; Lippi, G. Blood lactate concentration in COVID-19: A systematic literature review. Clin. Chem. Lab. Med. 2021. advance online publication. [Google Scholar] [CrossRef]
- Singh, B.; Kaur, P.; Maroules, M. Splanchnic vein thrombosis in COVID-19: A review of literature. Dig. Liver Dis. 2020, 52, 1407–1409. [Google Scholar] [CrossRef]
- Jagielski, M.; Piątkowski, J.; Jackowski, M. Challenges encountered during the treatment of acute mesenteric ischemia. Gastroenterol. Res. Pract. 2020, 5316849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasslan, R.; Dos Santos, J.P.; Menegozzo, C.; Pezzano, A.; Lunardeli, H.S.; Dos Santos Miranda, J.; Utiyama, E.M.; Damous, S. Outcomes after emergency abdominal surgery in COVID-19 patients at a referral center in Brazil. Updates Surg. 2021, 73, 763–768. [Google Scholar] [CrossRef]
- Lei, S.; Jiang, F.; Su, W.; Chen, C.; Chen, J.; Mei, W.; Zhan, L.Y.; Jia, Y.; Zhang, L.; Liu, D.; et al. Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. EClinicalMedicine 2020, 21, 100331. [Google Scholar] [CrossRef]
- Serban, D.; Socea, B.; Badiu, C.D.; Tudor, C.; Balasescu, S.A.; Dumitrescu, D.; Trotea, A.M.; Spataru, R.I.; Vancea, G.; Dascalu, A.M.; et al. Acute surgical abdomen during the COVID 19 pandemic: Clinical and therapeutic challenges. Exp. Ther. Med. 2021, 21, 519. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Parikh, C.; Verma, D.; Sundararajan, R.; Agrawal, U.; Bheemisetty, N.; Akku, R.; Sánchez-Velazco, D.; Waleed, M.S. Bowel ischaemia in COVID-19: A systematic review. Int. J. Clin. Pract. 2021, 75, e14930. [Google Scholar] [CrossRef] [PubMed]
- Yantiss, R.K.; Qin, L.; He, B.; Crawford, C.V.; Seshan, S.; Patel, S.; Wahid, N.; Jessurun, J. Intestinal Abnormalities in Patients With SARS-CoV-2 Infection: Histopathologic Changes Reflect Mechanisms of Disease. Am. J. Surg. Pathol. 2021, 46, 89–96. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D.; Bridgewood, C.; Ramanan, A.V.; Meaney, J.F.M.; Watad, A. COVID-19 vasculitis and novel vasculitis mimics. Lancet Rheumatol. 2021, 3, e224–e233. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan. China Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Avila, J.; Long, B.; Holladay, D.; Gottlieb, M. Thrombotic complications of COVID-19. Am. J. Emerg. Med. 2021, 39, 213–218. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Maier, C.L.; Truong, A.D.; Auld, S.C.; Polly, D.M.; Tanksley, C.L.; Duncan, A. COVID-19-associated hyperviscosity: A link between inflammation and thrombophilia? Lancet 2020, 395, 1758–1759. [Google Scholar] [CrossRef]
- Miyara, S.J.; Becker, L.B.; Guevara, S.; Kirsch, C.; Metz, C.N.; Shoaib, M.; Grodstein, E.; Nair, V.V.; Jandovitz, N.; McCann-Molmenti, A.; et al. Pneumatosis Intestinalis in the Setting of COVID-19: A Single Center Case Series From New York. Front. Med. 2021, 8, 638075. [Google Scholar] [CrossRef] [PubMed]
- Panigada, M.; Bottino, N.; Tagliabue, P.; Grasselli, G.; Novembrino, C.; Chantarangkul, V.; Pesenti, A.; Peyvandi, F.; Tripodi, A. Hypercoagulability of COVID-19 patients in intensive care unit: A report of thromboelastography findings and other parameters of hemostasis. J. Thromb. Haemost. 2020, 18, 1738–1742. [Google Scholar] [CrossRef]
- Hottz, E.D.; Azevedo-Quintanilha, I.G.; Palhinha, L.; Teixeira, L.; Barreto, E.A.; Pão, C.R.; Righy, C.; Franco, S.; Souza, T.M.; Kurtz, P.; et al. Platelet activation and platelet-monocyte aggregate formation trigger tissue factor expression in patients with severe COVID-19. Blood J. Am. Soc. Hematol. 2020, 136, 1330–1341. [Google Scholar] [CrossRef]
- Stefely, J.A.; Christensen, B.B.; Gogakos, T.; Cone Sullivan, J.K.; Montgomery, G.G.; Barranco, J.P.; Van Cott, E.M. Marked factor V activity elevation in severe COVID-19 is associated with venous thromboembolism. Am. J. Hematol. 2020, 95, 1522–1530. [Google Scholar] [CrossRef]
- Giuffrè, M.; Di Bella, S.; Sambataro, G.; Zerbato, V.; Cavallaro, M.; Occhipinti, A.A.; Palermo, A.; Crescenti, A.; Monica, F.; Luzzati, R.; et al. COVID-19-Induced Thrombosis in Patients without Gastrointestinal Symptoms and Elevated Fecal Calprotectin: Hypothesis Regarding Mechanism of Intestinal Damage Associated with COVID-19. Trop. Med. Infect. Dis. 2020, 5, 147. [Google Scholar] [CrossRef] [PubMed]
- Giuffrè, M.; Vetrugno, L.; Di Bella, S.; Moretti, R.; Berretti, D.; Crocè, L.S. Calprotectin and SARS-CoV-2: A Brief-Report of the Current Literature. Healthcare 2021, 9, 956. [Google Scholar] [CrossRef] [PubMed]
- Buso, G.; Becchetti, C.; Berzigotti, A. Acute splanchnic vein thrombosis in patients with COVID-19: A systematic review. Dig. Liver Dis. 2021, 53, 937–949. [Google Scholar] [CrossRef]
- Thachil, J. The versatile heparin in COVID-19. J. Thromb. Haemost. 2020, 18, 1020–1022. [Google Scholar] [CrossRef] [Green Version]
- Poterucha, T.J.; Libby, P.; Goldhaber, S.Z. More than an anticoagulant: Do heparins have direct anti-inflammatory effects? Thromb. Haemost. 2017, 117, 437–444. [Google Scholar] [CrossRef]
- Wang, M.K.; Yue, H.Y.; Cai, J.; Zhai, Y.J.; Peng, J.H.; Hui, J.F.; Hou, D.Y.; Li, W.P.; Yang, J.S. COVID-19 and the digestive system: A comprehensive review. World J. Clin. Cases 2021, 9, 3796–3813. [Google Scholar] [CrossRef]
- Manolis, A.S.; Manolis, T.A.; Manolis, A.A.; Papatheou, D.; Melita, H. COVID-19 Infection: Viral Macro- and Micro-Vascular Coagulopathy and Thromboembolism/Prophylactic and Therapeutic Management. J. Cardiovasc. Pharmacol. Ther. 2021, 26, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Conti, P.; Caraffa, A.; Gallenga, C.E.; Ross, R.; Kritas, S.K.; Frydas, I.; Younes, A.; Di Emidio, P.; Ronconi, G.; Toniato, E. IL-1 induces throboxane-A2 (TxA2) in COVID-19 causing inflammation and micro-thrombi: Inhibitory effect of the IL-1 receptor antagonist (IL-1Ra). J. Biol. Regul. Homeost. Agents 2020, 34, 1623–1627. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | No of Patients with Gastrointestinal Ischemia (Total No of COVID-19 Patients in ICU) | Sex (M; F) | Age (Mean) | BMI | Time from Admission to Onset (Days) | Abdominal CT Signs | Intraoperative/Endoscopic Findings | Treatment | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Kaafarani HMA [16] | 5 (141); 3.8% | 1;3 | 62.5 | 32.1 | 51.5 (18–104) days | NA | Cecum-1—patchy necrosis Cecum_ileon-1 Small bowel-3; yellow discoloration on the antimesenteric side of the small bowel; 1 case + liver necrosis | Surgical resection | NA |
| Kraft M [17] | 4 (190); 2.1% | NA | NA | NA | NA | NA | Bowel ischemia + perforation (2) Bowel ischemia + perforation (1) MAT+massive bowel ischemia (1) | Right hemicolectomy (2) Transverse colectomy (1) Conservative, not fit for surgery | Recovery (3) Death (1) |
| Yang C [18] | 20 (190 in ICU; 582 in total); 10.5% | 15:5 | 69 | 31.2 | 26.5 (17–42) | Distension Wall thickness Pneumatosis intestinalis Perforation SMA or celiac thrombosis | no info | Right hemicolectomy 7(35%) Sub/total colectomy12 (60%) Ileocecal resection 1(5%) | Recovery (11) Death (9) |
| Hwabejire J [19] | 20 | 13:7 | 58.7 | 32.5 | 13 (1–31) | Pneumatosis intestinalis 42% Portal venous gas (33%) Mesenteric vessel patency 92% | large bowel ischemia (8) small bowel ischemia (4) both (8) yellow discoloration of the ischemic bowel | resection of the ischemic segment abdomen left open + second look (14) | Recovery (10) Death (10) |
| O’Shea A [20] | 4 (142); 2.8% | NA | NA | NA | NA | bowel ischemia, portal vein gas, colic pneumatosis | NA | NA | NA |
| Qayed E [21] | 2 (878); 0.22% | NA | NA | NA | NA | NA | diffuse colonic ischemia (1) Small + large bowel ischemia and pneumatosis (1) | Total colectomy (1) Extensive resection (1) | Recovery (1) Death (1) |
| Article | Sex | Age | Comorbidities | Time from COVID-19 Diagnosis; Time from Admission (Days) | ICU; Type of Ventilation | Clinical Signs at Presentation | Leukocytes (/mm3) | CRP (mg/L) | Lactat mmol/L | Ferritin (ng/mL) | LDH (U/L) | Thrombocytes (/mm3) | D-Dimers (ng/mL) | Abdominal CT Signs | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Azouz E [22] | M | 56 | none | 1; 2 (hospitalized for acute ischemic stroke) | No info | abdominal pain and vomiting | No info | - | - | - | - | - | - | Multiple arterial thromboembolic complications: AMS, right middle cerebral artery, a free-floating clot in the aortic arch | Anticoagulation (no details), endovascular thrombectomy Laparotomy + resection of necrotic small bowel loops | No info |
| Al Mahruqi G [23] | M | 51 | none | 26; 24 | yes, intubated | Fever, metabolic acidosis, required inotropes | 30,000 | - | 7 | 687 | - | - | 2.5 | Non-occlusive AMI Hypoperfused small bowel, permeable aorta, SMA, IMA + deep lower limb thrombosis | enoxaparin 40 mg/day from admission; surgery refused by family | death |
| Ucpinar BA [24] | F | 82 | Atrial fibrillation, hypertension, chronic kidney disease | 3; 3 | no | - | 14,800 | 196 | 5.1 | - | - | - | 1600 | SMA thrombosis; distended small bowel, with diffuse submucosal pneumatosis portomesenteric gas | fluid resuscitation; continued ceftriaxone, enoxaparin 0.4cc twice daily; not operable due to fulminant evolution | Death |
| Karna ST [25] | F | 61 | DM, hypertension | 4; 4 | Yes, HFNO | diffuse abdominal pain with distention | 21,400 | 421.6 | 1.4 | - | - | 464,000 | No | thrombosis of the distal SMA with dilated jejunoileal loops and normal enhancing bowel wall. | Iv heparin 5000 ui, followed by 1000 ui, Ecospin and clopidogrel Laparotomy after 10 days with segmental enterectomy of the necrotic bowel | Death by septic shock and acute renal failure |
| Singh B [26] | F | 82 | Hypertension, T2DM | 32; 18 | Yes, Ventilator support | severe diffuse abdominal distension and tenderness | 22,800 | 308 | 2.5 | 136 | 333 | 146,000 | 1.3 | SMA—colic arteries thrombosis pneumatosis intestinalis affecting the ascending colon and cecum | laparotomy, ischemic colon resection, ileostomy; heparin in therapeutic doses pre- and post-surgery | slow recovery |
| Nakatsutmi K [27] | F | 67 | DM, diabetic nephropathy requiring dialysis, angina, post-resection gastric cancer | 16; 12 | ICU, intubation | hemodynamic deterioration, abdominal distension | 15,100 | 32.14 | - | - | - | - | 26.51 | edematous transverse colon; abdominal vessels with sclerotic changes | laparotomy, which revealed vascular micro thrombosis of transverse colon—right segment resection of the ischemic colonic segment, ABTHERA management, second look, and closure of the abdomen after 24 h | death |
| Dinoto E [28] | F | 84 | DM, hypertension, renal failure | 2; 2 | no | Acute abdominal pain and distension; | 18,000 | 32.47 | - | - | 431 | - | 6937 | SMA origin stenosis and occlusion at 2 cm from the origin, absence of bowel enhancement | Endovascular thrombectomy of SMA; surgical transfemoral thrombectomy and distal superficial femoral artery stenting | Death due to respiratory failure |
| Kiwango F [29] | F | 60 | DM, hypertension | 12; 3 | no | Sudden onset abdominal pain | 7700 | - | - | - | - | - | 23.8 | Not performed | Not performed due to rapid oxygen desaturation Massive bowel acute ischemia | death |
| Article | Sex | Age | Comorbidities | Time from COVID-19 Diagnosis (Days) | Clinical Signs at Presentation | Leukocyte Count (/mm3) | CRP (mg/L) | Lactate mmol/L | Ferritin (ng/mL) | LDH (U/L) | Thrombocytes (/mm3) | D-Dimers (ng/mL) | Abdominal CT Signs | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sevella, P [30] | M | 44 | none | 10 | Acute abdominal pain constipation, vomiting | 23,400 | - | - | - | 1097 | 360,000 | 1590 | Viable jejunum, ischemic bowel, peritoneal thickening with fat stranding; free fluid in the peritoneal cavity | LMWH 60 mg daily Piperacillin 4g/day Tazobactam 500 mg/day Extensive small bowel + right colon resection | death |
| Nasseh S [31] | M | 68 | no info | First diagnosis | epigastric pain and diarrhea for 4 days | 17,660 | 125 | - | - | - | - | 6876 | terminal segment of the ileocolic artery thrombosis; thickening of the right colon wall and the last 30 cm of the small bowl | unfractionated heparin laparoscopy -no bowel resection needed | recovery |
| Aleman W [32] | M | 44 | none | 20 | severe abdominopelvic pain | 36,870 | - | - | 456.23 | - | 574,000 | 263.87 | absence of flow at SMV, splenic, portal vein; Small bowel loop dilatation and mesenteric fat edema | enoxaparin and pain control medication 6 days, then switched to warfarin 6 months | recovery |
| Jeilani M [33] | M | 68 | Alzheimer disease, COPD | 9 | Sharp abdominal pain +distension | 12,440 | 307 | - | - | - | 318,000 | 897 | a central venous filling defect within the portal vein extending to SMV; no bowel wall changes | LMWH, 3 months | recovery |
| Randhawa J [34] | F | 62 | none | First diagnosis | right upper quadrant pain and loss of appetite for 14 days | Normal limits | - | - | - | 346 | - | - | large thrombus involving the SMV, the main portal vein with extension into its branches | Fondaparinux 2.5. mg 5 days, then warfarin 4 mg (adjusted by INR), 6 months | recovery |
| Cheung S [35] | M | 55 | none | 12 (discharged for 7 days) | Nausea, vomiting and worsening generalized abdominal pain with guarding | 12,446 | - | 0.68 | - | - | - | - | low-density clot, 1.6 cm in length, causing high-grade narrowing of the proximal SMA | continuous heparin infusion continued 8 h postoperative, Laparotomy with SMA thromboembolectomy and enterectomy (small bowel) | recovery |
| Beccara L [36] | M | 52 | none | 22 (5 days after discharge and cessation prophylactic LWMH) | vomiting and abdominal pain, tenderness in epigastrium and mesogastrium | 30,000 | 222 | - | - | - | - | - | arterial thrombosis of vessels efferent of the SMA with bowel distension | Enterectomy (small bowel) LMWH plus aspirin 100 mg/day at discharge | recovery |
| Vulliamy P [37] | M | 75 | none | 14 | abdominal pain and vomiting for 2 days | 18,100 | 3.2 | - | - | - | 497,000 | 320 | intraluminal thrombus was present in the descending thoracic aorta with embolic occlusion of SMA | Catheter-directed thrombolysis, enterectomy (small bowel) | recovery |
| De Barry O [38] | F | 79 | none | First diagnosis | Epigastric pain, diarrhea, fever for 8 days, acute dyspnea | 12600 | 125 | 5.36 | - | - | - | - | SMV, portal vein, SMA, and jejunal artery thrombosis Distended loops, free fluid | anticoagulation Resection of affected colon+ ileum, SMA thrombolysis, thrombectomy | death |
| Romero MCV [39] | M | 73 | smoker, DM, hypertension | 14 | severe abdominal pain, nausea. fecal emesis, peritoneal irritation | 18,000 | - | - | - | - | 120,000 | >5000 | RX: distention of intestinal loops, inter-loop edema, intestinal pneumatosis | enoxaparin (60 mg/0.6 mL), antibiotics (no info) enterectomy, anastomotic fistula, reintervention | death |
| Posada Arango [40] | M F F | 62 22 65 | None Appendectomy 7 days before left nephrectomy, | 5 3 15 | colicative abdominal pain at food intake; unsystematized gastrointestinal symptoms; abdominal pain in the upper hemiabdomen | 20,100 - - | - - - | - - - | 1536 - - | 534 - - | - - - | - - - | Case 1: thrombus in distal SMA and its branches, intestinal loops dilatation, hydroaerical levels, free fluid thrombosis of SMV Case 2: SMV thrombosis and adiacent fat edema Case 3: thrombi in the left jejunal artery branch with infarction of the corresponding jejunal loops | Case 1: Laparotomy: extensive jejunum + ileum ischemia; surgery could not be performed Case 2: Anticoagulation analgesic and antibiotics Case 3: segmental enterectomy | Case 1: death Case 2: recovery Case 3: recovery |
| Pang JHQ [41] | M | 30 | none | First diagnosis | colicky abdominal pain, vomiting | - | - | - | - | - | - | 20 | SMV thrombosis with diffuse mural thickening and fat stranding of multiple jejunal loops | conservative, anticoagulation with LMWH 1mg/kc, twice daily, 3 months; readmitted and operated for congenital adherence causing small bowel obstruction | recovery |
| Lari E [42] | M | 38 | none | First diagnosis | abdominal pain, nausea, intractable vomiting, and shortness of breath | Mild leukocytosis | - | 2.2 | - | - | - | 2100 | extensive thrombosis of the portal, splenic, superior, and inferior mesenteric veins + mild bowel ischemia | Anticoagulation, resection of the affected bowel loop | No info |
| Carmo Filho A [43] | M | 33 | Obesity (BMI: 33), other not reported | 7 | severe low back pain radiating to the hypogastric region | - | 58.2 | - | 1570 | - | - | 879 | enlarged inferior mesenteric vein not filled by contrast associated with infiltration of the adjacent adipose planes | enoxaparin 5 days, followed by long term oral warfarin | recovery |
| Hanif M [44] | F | 20 | none | 8 | abdominal pain and abdominal distension | 15,900 | 62 | - | 1435.3 | 825 | 633,000 | 2340 | not performed | evidence of SMA thrombosis; enterectomy with exteriorization of both ends | recovery |
| Amaravathi U [45] | M | 45 | none | 5 | Acute epigastric and periumbilical pain | - | Normal value | 1.3 | 324.3 | - | - | 5.3 | SMA and SMV thrombus | i.v. heparin; Laparotomy with SMA thrombectomy; 48 h Second look: resection of the gangrenous bowel segment | No info |
| Al Mahruqi G [23] | M | 51 | none | 4 | generalized abdominal pain, nausea, vomiting | 16,000 | - | - | 619 | - | - | 10 | SMA thrombosis and non-enhancing proximal ileal loops consistent with small bowel ischemia | unfractionated heparin, thrombectomy + repeated resections of the ischemic bowel at relook (jejunum+ileon+cecum) | Case 2: recovery |
| Goodfellow M [46] | F | 36 | RYGB, depression, asthma | 6 | epigastric pain, irradiating back, nausea | 9650 | 1.2 | 0.7 | - | - | - | - | abrupt cut-off of the SMV in the proximal portion; diffuse infiltration of the mesentery, wall thickening of small bowel | IV heparin infusion, followed by 18,000 UI delteparin after 72 h | recovery |
| Abeysekera KW [26] | M | 42 | Hepatitis B | 14 | right hypochondrial pain, progressively increasing for 9 days | - | - | - | - | - | - | - | enhancement of the entire length of the portal vein and a smaller thrombus in the mid-superior mesenteric vein, mural edema of the distal duodenum, distal small bowel, and descending colon | factor Xa inhibitor apixaban 5 mg ×2/day, 6 months | -recovery |
| Rodriguez-Nakamura RM [27] | M F | 45 42 | -vitiligo -obesity | 14 | severe mesogastric pain, nausea, diaphoresis | 16,400 18,800 | 367 239 | - - | 970 - | - - | 685,000 - | 1450 14,407 | Case 1: SMI of thrombotic etiology with partial rechanneling through the middle colic artery, and hypoxic-ischemic changes in the distal ileum and the cecum Case 2: thrombosis of the portal and mesenteric veins and an abdominopelvic collection in the mesentery with gas | Case 1: resection with entero-enteral anastomosis; rivaroxaban 10 mg/day, 6 months Case 2: Loop resection, entero-enteral manual anastomosis, partial omentectomy, and cavity wash (fecal peritonitis) | Case 1: Recovery Case 2: death |
| Plotz B [47] | F | 27 | SLE with ITP | First diagnosis | acute onset nausea, vomiting, and non-bloody diarrhea | - | - | - | - | - | - | 5446 | diffuse small bowel edema | enoxaparin, long term apixaban at discharge | recovery |
| Chiu CY [48] | F | 49 | Hypertension, DM, chronic kidney disease | 28 | diffuse abdominal pain melena and hematemesis | - | - | - | - | - | - | 12,444 | distended proximal jejunum with mural thickening | laparotomy, proximal jejunum resection | no info |
| Farina D [49] | M | 70 | no info | 3 | abdominal pain, nausea | 15,300 | 149 | - | - | - | - | - | acute small bowel hypoperfusion, SMA thromboembolism | not operable due to general condition | Death |
| Nr. of Patients | 89 |
|---|---|
| M | 48 (61.5% *) |
| F | 30 (38.5% *) |
| NA | 11 |
| The first sign of COVID-19 | 6 (6.7%) |
| Home treated | 17 (19.1%) |
Hospitalized
| 63 (70.7%) 58 (92% of hospitalized patients) |
| Discharged | 3 (3.3%) |
Time from diagnosis of COVID-19 infection
| 8.7 ± 7.4 (1–28 days) 9.6 ± 8.3 (1–26 days) |
| Time from admission in hospitalized patients | 1–104 days |
Age (mean)
| 59.3 ± 12.7 years 62 ± 9.6 years. (p < 0.0001) 52.8 ± 16.4 years. |
| BMI | 31.2–32.5 |
Comorbidities
| 8 7 2 1 2 1 1 1 1 1 1 1 |
| Parameter | Hospitalized (63) | Non-Hospitalized (26) | p * Value |
|---|---|---|---|
Type of mesenteric ischemia:
| 5 (14.7% *) 1 (2.9%) 0 30 (88.2%) 2 (5.8%) 29 | 10 (38.4%) 11 (42.3%) 2 (7.6%) 3 (11.5%) 1 (3.8%) 0 | p < 0.0001 |
Management:
| 0 2 (1 + surgery) (3%) 60 (95.4%) 2 (3%) | 10 (38.4%) 2 (+surgery) 15 (57.6%) 1 (3.8%) | p < 0.0001 |
Location of the resected segment:
| 35 (56%) 10 (16%) 15 (24%) 6 | 0 12 (80%) 3 (20%) 0 | p < 0.0001 |
Outcomes:
| 26 (46.4%) 30 (54.4%) 7 | 17 (79.3%) 5 (21.7%) 3 | p = 0.013 |
| Parameters | Outcome: Death | p-Value |
|---|---|---|
Age
| 27.2% 60% | 0.0384 * 0.043 ** |
Surgery
| 0% 60% | 0.019 ** |
Type of mesenteric ischemia
| 47% 20% 66% | 0.23 ** |
| D dimers | Wide variation | 0.085 * 0.394 ** |
| Leucocytes | Wide variation (9650–37,000/mmc) | 0.803 0.385 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serban, D.; Tribus, L.C.; Vancea, G.; Stoian, A.P.; Dascalu, A.M.; Suceveanu, A.I.; Tanasescu, C.; Costea, A.C.; Tudosie, M.S.; Tudor, C.; et al. Acute Mesenteric Ischemia in COVID-19 Patients. J. Clin. Med. 2022, 11, 200. https://doi.org/10.3390/jcm11010200
Serban D, Tribus LC, Vancea G, Stoian AP, Dascalu AM, Suceveanu AI, Tanasescu C, Costea AC, Tudosie MS, Tudor C, et al. Acute Mesenteric Ischemia in COVID-19 Patients. Journal of Clinical Medicine. 2022; 11(1):200. https://doi.org/10.3390/jcm11010200
Chicago/Turabian StyleSerban, Dragos, Laura Carina Tribus, Geta Vancea, Anca Pantea Stoian, Ana Maria Dascalu, Andra Iulia Suceveanu, Ciprian Tanasescu, Andreea Cristina Costea, Mihail Silviu Tudosie, Corneliu Tudor, and et al. 2022. "Acute Mesenteric Ischemia in COVID-19 Patients" Journal of Clinical Medicine 11, no. 1: 200. https://doi.org/10.3390/jcm11010200