
Impact of Viral Decontamination Method on Cytokine Profile of COVID-19 Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples
2.2. Virus Removal Procedures
2.2.1. Ultrafiltration Method
2.2.2. UVC Irradiation Method
2.3. Evaluation of Viral Load Removal
2.3.1. RT-qPCR
2.3.2. Confirmation of Virus Inactivation by Virus Isolation
2.4. Comparison Immunogenicity on Decontaminated Samples
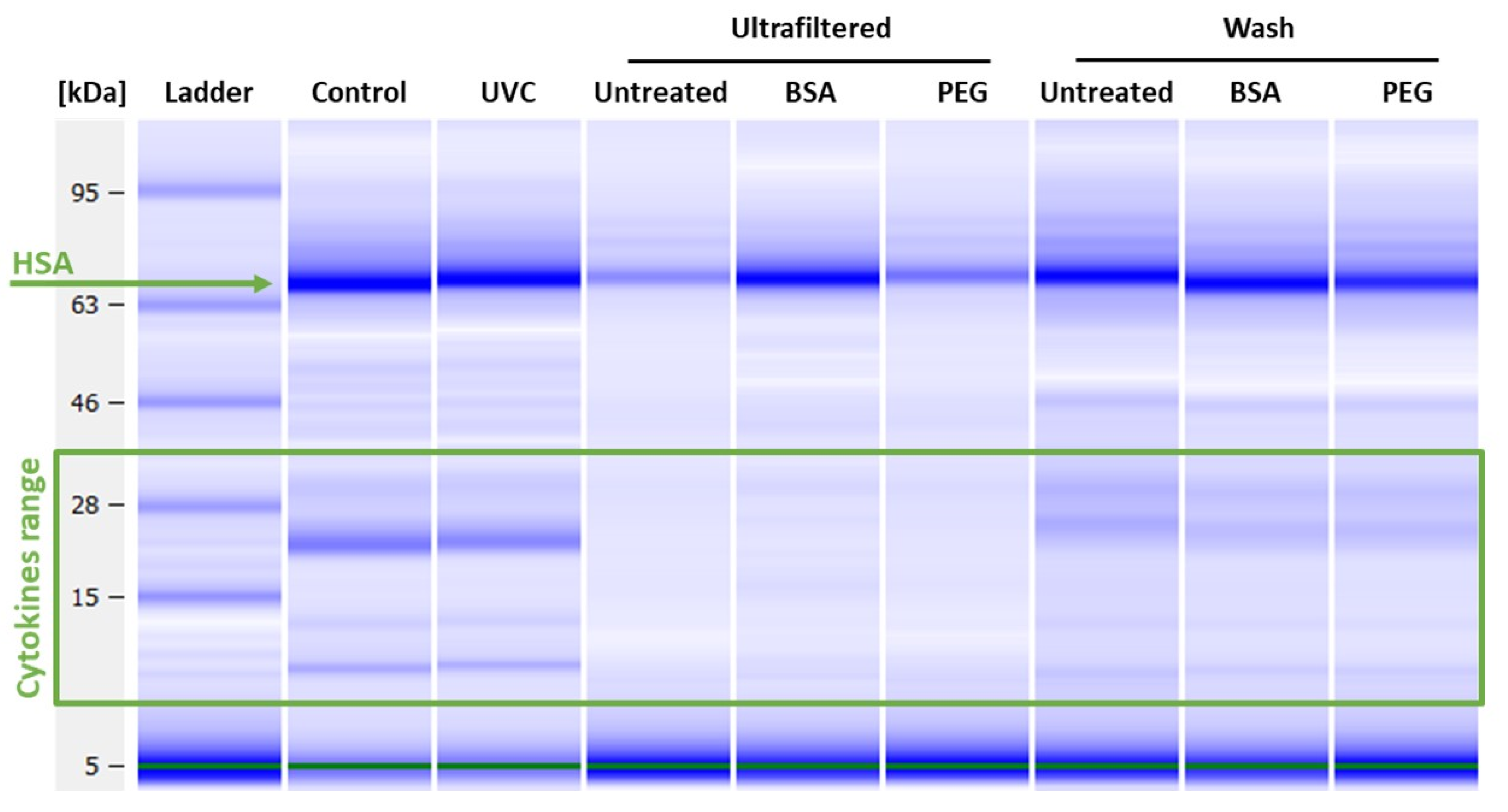
2.5. Bioanalyzer
2.6. Multiplex Immunoassays for Cytokine Detection
3. Results
3.1. Viral Load Removal
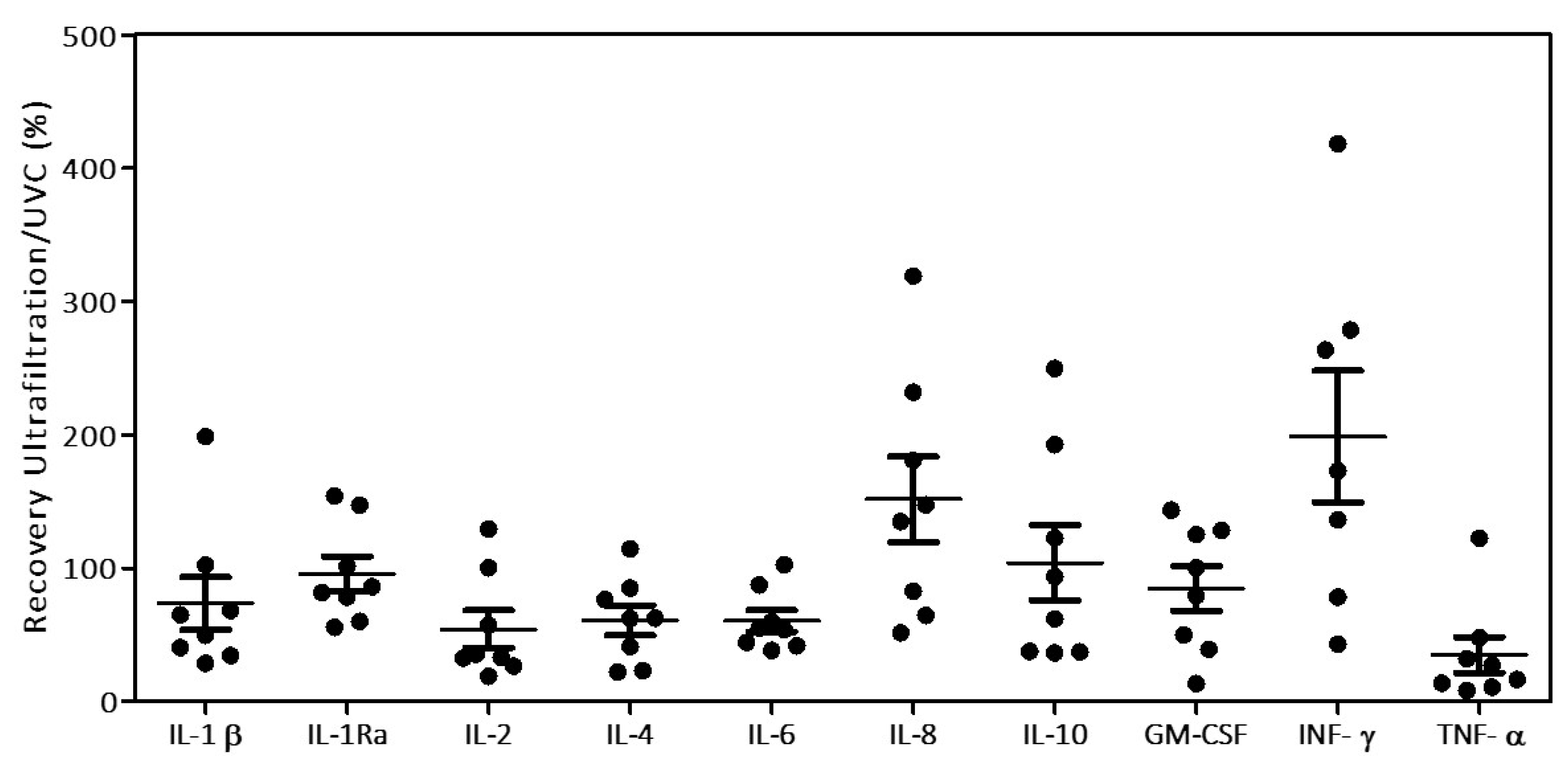
3.2. Cytokine Recovery
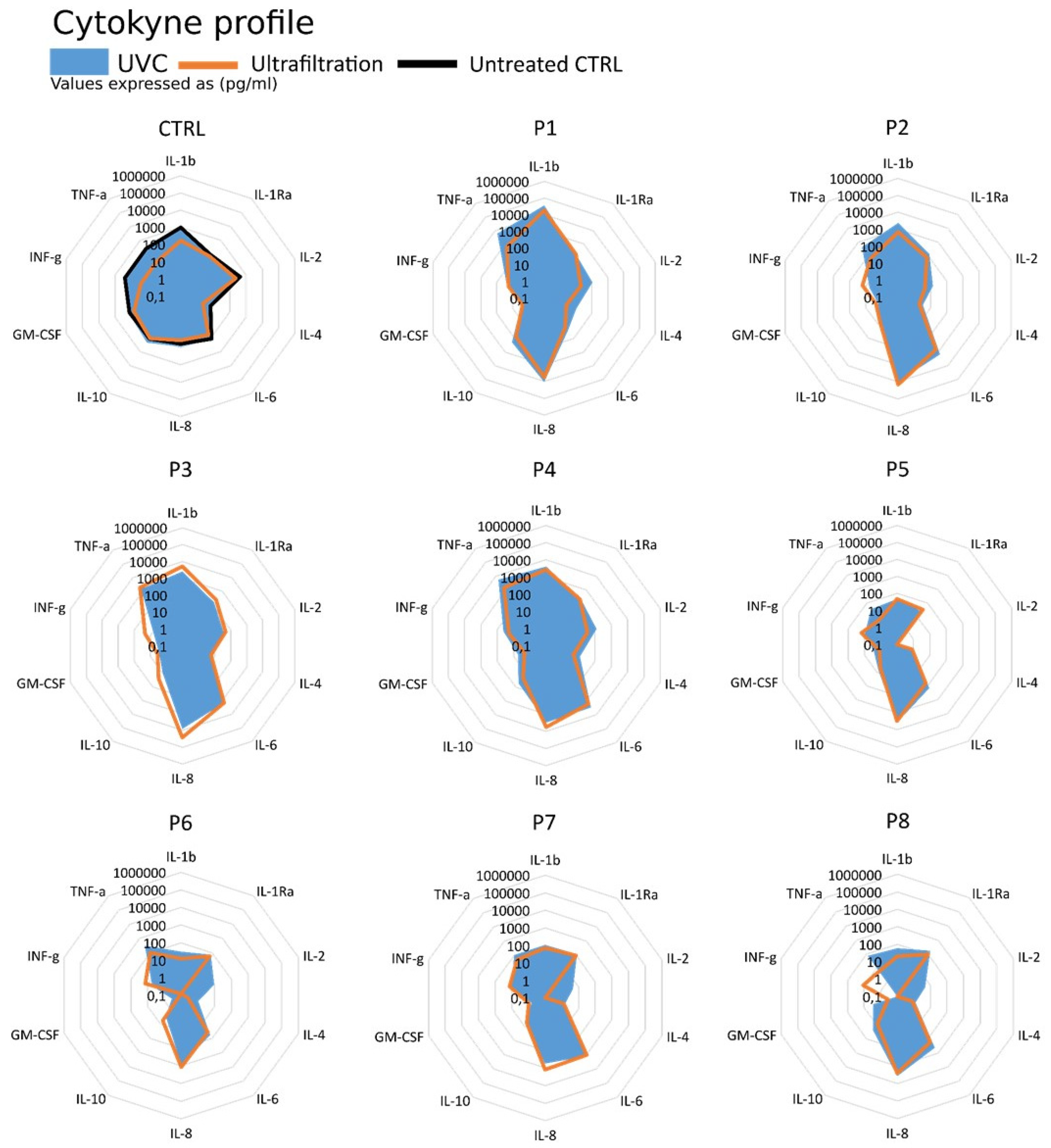
3.3. Cytokine Profiling
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brodin, P. Immune determinants of COVID-19 disease presentation and severity. Nat. Med. 2021, 27, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Fajnzylber, J.; The Massachusetts Consortium for Pathogen Readiness; Regan, J.; Coxen, K.; Corry, H.; Wong, C.; Rosenthal, A.; Worrall, D.; Giguel, F.; Piechocka-Trocha, A.; et al. SARS-CoV-2 viral load is associated with increased disease severity and mortality. Nat. Commun. 2020, 11, 1–9. [Google Scholar] [CrossRef]
- D’Errico, S.; Zanon, M.; Montanaro, M.; Radaelli, D.; Sessa, F.; Di Mizio, G.; Montana, A.; Corrao, S.; Salerno, M.; Pomara, C. More than Pneumonia: Distinctive Features of SARS-Cov-2 Infection. From Autopsy Findings to Clinical Implications: A Systematic Review. Microorganisms 2020, 8, 1642. [Google Scholar] [CrossRef] [PubMed]
- Cipolloni, L.; Sessa, F.; Bertozzi, G.; Baldari, B.; Cantatore, S.; Testi, R.; D’Errico, S.; Di Mizio, G.; Asmundo, A.; Castorina, S.; et al. Preliminary Post-Mortem COVID-19 Evidence of Endothelial Injury and Factor VIII Hyperexpression. Diagnostics 2020, 10, 575. [Google Scholar] [CrossRef] [PubMed]
- Sessa, F.; Salerno, M.; Pomara, C. Autopsy Tool in Unknown Diseases: The Experience with Coronaviruses (SARS-CoV, MERS-CoV, SARS-CoV-2). Medicina 2021, 57, 309. [Google Scholar] [CrossRef]
- Pandolfi, L.; Fossali, T.; Frangipane, V.; Bozzini, S.; Morosini, M.; D’Amato, M.; Lettieri, S.; Urtis, M.; Di Toro, A.; Saracino, L.; et al. Broncho-alveolar inflammation in COVID-19 patients: A correlation with clinical outcome. BMC Pulm. Med. 2020, 20, 301. [Google Scholar] [CrossRef] [PubMed]
- Biosafety in Microbiological and Biomedical Laboratories—6th Edition. Available online: https://www.cdc.gov/labs/pdf/SF__19_308133-A_BMBL6_00-BOOK-WEB-final-3.pdf (accessed on 17 June 2021).
- Goldstein, M.A.; Tauraso, N.M. Effect of Formalin, β-Propiolactone, Merthiolate, and Ultraviolet Light Upon Influenza Virus Infectivity, Chicken Cell Agglutination, Hemagglutination, and Antigenicity. Appl. Microbiol. 1970, 19, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Jonges, M.; Liu, W.M.; van der Vries, E.; Jacobi, R.; Pronk, I.; Boog, C.; Koopmans, M.; Meijer, A.; Soethout, E. Influenza Virus Inactivation for Studies of Antigenicity and Phenotypic Neuraminidase Inhibitor Resistance Profiling. J. Clin. Microbiol. 2010, 48, 928–940. [Google Scholar] [CrossRef] [Green Version]
- Sagripanti, J.-L.; Lytle, C.D. Inactivation of Influenza Virus by Solar Radiation. Photochem. Photobiol. 2007, 83, 1278–1282. [Google Scholar] [CrossRef]
- Sakudo, A. N 8322 gas plasma inactivates influenza virus mediated by oxidative stress. Front. Biosci. 2014, E6, 69–79. [Google Scholar] [CrossRef] [Green Version]
- Bain, W.; Lee, J.S.; Watson, A.M.; Stitt-Fischer, M.S. Practical Guidelines for Collection, Manipulation and Inactivation of SARS-CoV-2 and COVID-19 Clinical Specimens. Curr. Protoc. Cytom. 2020, 93, e77. [Google Scholar] [CrossRef] [PubMed]
- Dowall, S.D.; Graham, V.A.; Fletcher, T.; Hewson, R. Use and reliability of multiplex bead-based assays (Luminex) at Containment Level 4. Methods 2019, 158, 17–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heilingloh, C.S.; Aufderhorst, U.W.; Schipper, L.; Dittmer, U.; Witzke, O.; Yang, D.; Zheng, X.; Sutter, K.; Trilling, M.; Alt, M.; et al. Susceptibility of SARS-CoV-2 to UV irradiation. Am. J. Infect. Control 2020, 48, 1273–1275. [Google Scholar] [CrossRef] [PubMed]
- Storm, N.; McKay, L.G.A.; Downs, S.N.; Johnson, R.I.; Birru, D.; de Samber, M.; Willaert, W.; Cennini, G.; Griffiths, A. Rapid and complete inactivation of SARS-CoV-2 by ultraviolet-C irradiation. Sci. Rep. 2020, 10, 1–5. [Google Scholar] [CrossRef]
- Hennø, L.T.; Storjord, E.; Christiansen, D.; Bergseth, G.; Ludviksen, J.K.; Fure, H.; Barene, S.; Nielsen, E.W.; Mollnes, T.E.; Brekke, O.-L. Effect of the anticoagulant, storage time and temperature of blood samples on the concentrations of 27 multiplex assayed cytokines – Consequences for defining reference values in healthy humans. Cytokine 2017, 97, 86–95. [Google Scholar] [CrossRef] [Green Version]
- Rovida, F.; Cereda, D.; Novati, S.; Licari, A.; Triarico, A.; Marseglia, G.; Bruno, R.; Baldanti, F.; Mondelli, M.; Brunetti, E.; et al. Low risk for SARS-CoV2 symptomatic infection and early complications in paediatric patients during the ongoing CoVID19 epidemics in Lombardy. Clin. Microbiol. Infect. 2020, 26, 1569–1571. [Google Scholar] [CrossRef]
- Piralla, A.; Ricchi, M.; Cusi, M.G.; Prati, P.; Vicari, N.; Scarsi, G.; Gandolfo, C.; Anichini, G.; Terrosi, C.; Percivalle, E.; et al. Residual SARS-CoV-2 RNA in nasal swabs of convalescent COVID-19 patients: Is prolonged quarantine always justified? Int. J. Infect. Dis. 2021, 102, 299–302. [Google Scholar] [CrossRef]
- Sabino, C.P.; Sellera, F.P.; Sales-Medina, D.F.; Machado, R.R.G.; Durigon, E.L.; Freitas-Junior, L.H.; Ribeiro, M.S. UV-C (254 nm) lethal doses for SARS-CoV-2. Photodiagnosis Photodyn. Ther. 2020, 32, 101995. [Google Scholar] [CrossRef]
- Navarro, A.; Gómez, L.; Sanseverino, I.; Niegowska, M.; Roka, E.; Pedraccini, R.; Vargha, M.; Lettieri, T. SARS-CoV-2 detection in wastewater using multiplex quantitative PCR. Sci. Total Environ. 2021, 797, 148890. [Google Scholar] [CrossRef]
- 2019-Novel Coronavirus (2019-NCoV) Real-Time rRT-PCR Panel Primers and Probes. Available online: https://www.cdc.gov/coronavirus/2019-ncov/downloads/rt-pcr-panel-primer-probes.pdf (accessed on 17 June 2021).
- Medema, G.; Heijnen, L.; Elsinga, G.; Italiaander, R.; Brouwer, A. Presence of SARS-Coronavirus-2 RNA in Sewage and Correlation with Reported COVID-19 Prevalence in the Early Stage of the Epidemic in The Netherlands. Environ. Sci. Technol. Lett. 2020, 7, 511–516. [Google Scholar] [CrossRef]
- La Scola, B.; Le Bideau, M.; Andreani, J.; Hoang, V.T.; Grimaldier, C.; Colson, P.; Gautret, P.; Raoult, D. Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1059–1061. [Google Scholar] [CrossRef] [PubMed]
- Sethuraman, N.; Jeremiah, S.S.; Ryo, A. Interpreting Diagnostic Tests for SARS-CoV-2. JAMA 2020, 323, 2249–2251. [Google Scholar] [CrossRef] [PubMed]
- Hamamoto, R.; Ito, H.; Hirohara, M.; Chang, R.; Hongo-Hirasaki, T.; Hayashi, T. Interactions between protein molecules and the virus removal membrane surface: Effects of immunoglobulin G adsorption and conformational changes on filter performance. Biotechnol. Prog. 2018, 34, 379–386. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Flamholz, A.; Phillips, R.; Milo, R. SARS-CoV-2 (COVID-19) by the numbers. eLife 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, W.; Bertsch, P.M.; Bivins, A.; Bibby, K.; Farkas, K.; Gathercole, A.; Haramoto, E.; Gyawali, P.; Korajkic, A.; McMinn, B.R.; et al. Comparison of virus concentration methods for the RT-qPCR-based recovery of murine hepatitis virus, a surrogate for SARS-CoV-2 from untreated wastewater. Sci. Total Environ. 2020, 739, 139960. [Google Scholar] [CrossRef]
- Virus Concentration by Ultrafiltration. Available online: https://www.sigmaaldrich.com/technical-documents/protocols/biology/viral-concentration-amicon-ultrafiltration.html (accessed on 17 May 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| Ct | 17.4 | 22.4 | 24.2 | 21.8 | 18.8 | 21.2 | 20.5 | 19.6 |
| Filtered | UND | UND | UND | UND | UND | UND | UND | UND |
| UVC | 28.17 ± 0.83 | UND | UND | UND | 33.92 ± 2.37 | UND | UND | 32.80 ± 1.08 |
| Advantages | Ultrafiltration | UVC Irradiation |
|---|---|---|
| Cheap | Yes | Yes |
| Rapid | Yes | Yes |
| Applicable for large volume | Up to 70 mL/time | Yes |
| Applicable in BSL3 | Yes (only centrifuge required) | Yes (although might be difficult to set and control radiation) |
| Complete and efficient active virus removal | Yes | Yes |
| Recovery | Poor. Sample interacts with the filter causing sample loss | Good. Disassembly of the dimeric/trimeric forms of IL-8, IL-10 and TNF-α |
| Cytokine profiling | Yes | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magrì, D.; Navarro, A.; Bergami, F.; Percivalle, E.; Ferrari, A.; Lettieri, T.; Calzolai, L.; Piralla, A.; Baldanti, F.; Gioria, S. Impact of Viral Decontamination Method on Cytokine Profile of COVID-19 Patients. Biomedicines 2021, 9, 1287. https://doi.org/10.3390/biomedicines9101287
Magrì D, Navarro A, Bergami F, Percivalle E, Ferrari A, Lettieri T, Calzolai L, Piralla A, Baldanti F, Gioria S. Impact of Viral Decontamination Method on Cytokine Profile of COVID-19 Patients. Biomedicines. 2021; 9(10):1287. https://doi.org/10.3390/biomedicines9101287
Chicago/Turabian StyleMagrì, Davide, Anna Navarro, Federica Bergami, Elena Percivalle, Alessandro Ferrari, Teresa Lettieri, Luigi Calzolai, Antonio Piralla, Fausto Baldanti, and Sabrina Gioria. 2021. "Impact of Viral Decontamination Method on Cytokine Profile of COVID-19 Patients" Biomedicines 9, no. 10: 1287. https://doi.org/10.3390/biomedicines9101287