
Clinical Characteristics of Coronavirus Disease (COVID-19) in Mexican Children and Adolescents

 , , , , , ,
, , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Sources
2.2.1. National Data: Mexico
2.2.2. Regional Data: HIMFG
2.3. Statistical Analysis and Graphs
3. Results
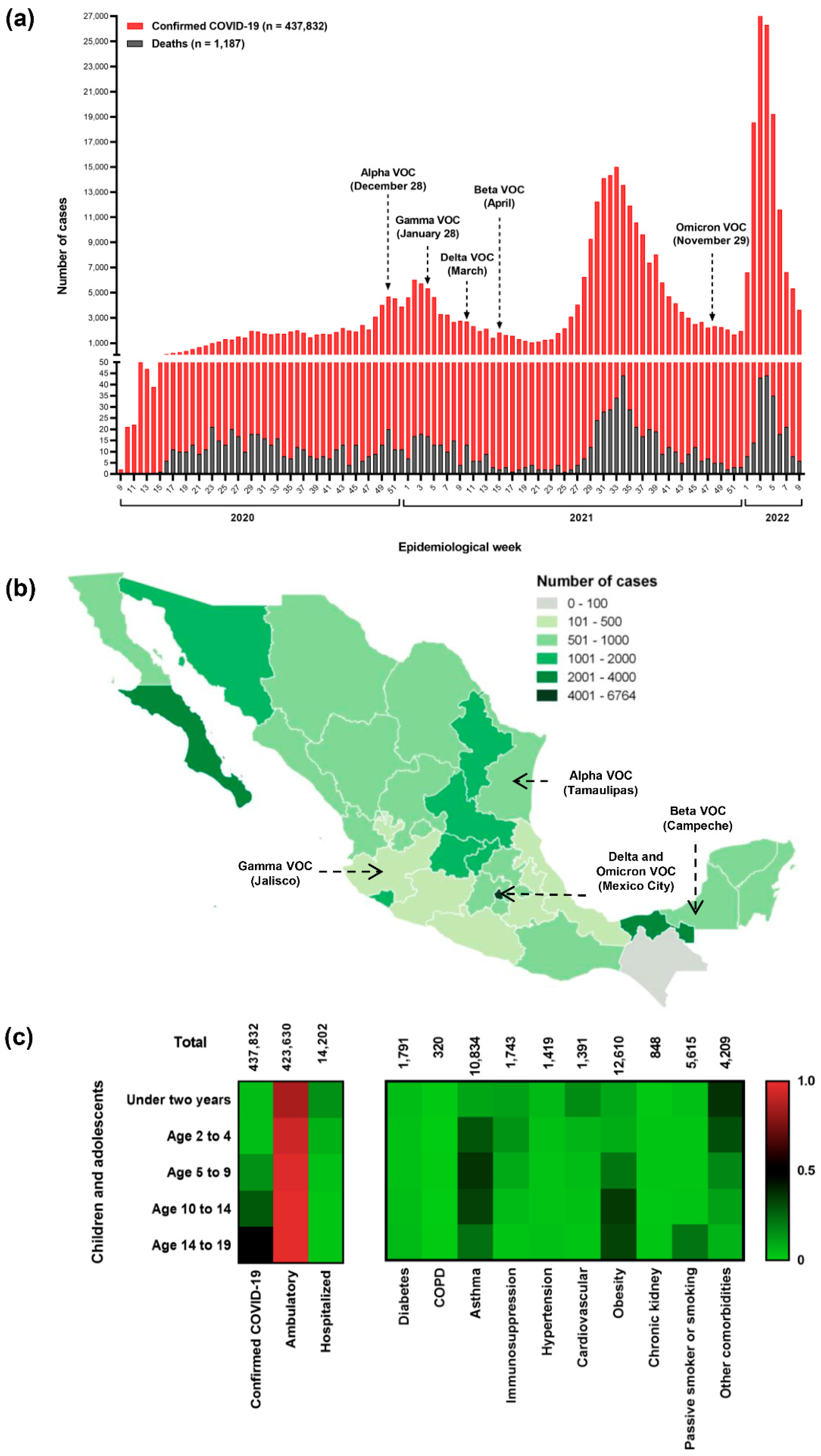
3.1. National Outlook of the Pediatric and Adolescent Population
3.2. Perspectives of a Tertiary-Care Pediatric Hospital (HIMFG)
3.2.1. Features of Ambulatory and Hospitalized Patients Who Attended HIMFG
3.2.2. Analysis of Viral Load and Serology from Patients Diagnosed through RT-PCR
3.2.3. Evaluation of Deceased Patients Who Attended HIMFG
4. Discussion
5. Strengths and Weakness
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guan, W.-J.; Liang, W.-H.; Zhao, Y.; Liang, H.-R.; Chen, Z.-S.; Li, Y.-M.; Liu, X.-Q.; Chen, R.-C.; Tang, C.-L.; Wang, T.; et al. Comorbidity and Its Impact on 1590 Patients with COVID-19 in China: A Nationwide Analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Bartrand, T.A.; Weir, M.H.; Omura, T.; Haas, C.N. Development of a Dose-Response Model for SARS Coronavirus. Risk Anal. 2010, 30, 1129–1138. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiology of COVID-19 Among Children in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [PubMed]
- Viner, R.M.; Mytton, O.T.; Bonell, C.; Melendez-Torres, G.J.; Ward, J.; Hudson, L.; Waddington, C.; Thomas, J.; Russell, S.; van der Klis, F.; et al. Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared With Adults. JAMA Pediatr. 2021, 175, 143–156. [Google Scholar] [CrossRef]
- Yasuhara, J.; Watanabe, K.; Takagi, H.; Sumitomo, N.; Kuno, T. COVID-19 and Multisystem Inflammatory Syndrome in Children: A Systematic Review and Meta-Analysis. Pediatr. Pulmonol. 2021, 56, 837–848. [Google Scholar] [CrossRef]
- Du, H.; Dong, X.; Zhang, J.; Cao, Y.; Akdis, M.; Huang, P.; Chen, H.; Li, Y.; Liu, G.; Akdis, C.A.; et al. Clinical Characteristics of 182 Pediatric COVID-19 Patients with Different Severities and Allergic Status. Allergy 2020, 76, 510–532. [Google Scholar] [CrossRef]
- Palomo-Collí, M.Á.; Fuentes-Lugo, A.D.; Cobo-Ovando, S.R.; Juárez-Villegas, L. COVID-19 in Children and Adolescents With Cancer From a Single Center in Mexico City. J. Pediatr. Hematol. Oncol. 2021, 43, e1047–e1048. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Zhang, W.; Wang, Y.; Bao, S.; Li, Y.; et al. SARS-CoV-2 Infection in Children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef]
- Parri, N.; Lenge, M.; Buonsenso, D. Coronavirus Infection in Pediatric Emergency Departments (CONFIDENCE) Research Group Children with Covid-19 in Pediatric Emergency Departments in Italy. N. Engl. J. Med. 2020, 383, 187–190. [Google Scholar] [CrossRef]
- Cortés-Sarabia, K.; Cruz-Rangel, A.; Flores-Alanis, A.; Salazar-García, M.; Jiménez-García, S.; Rodríguez-Martínez, G.; Reyes-Grajeda, J.P.; Rodríguez-Téllez, R.I.; Patiño-López, G.; Parra-Ortega, I.; et al. Clinical Features and Severe Acute Respiratory Syndrome-Coronavirus-2 Structural Protein-Based Serology of Mexican Children and Adolescents with Coronavirus Disease 2019. PLoS ONE 2022, 17, e0273097. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Magaziotou, I.; Dedoukou, X.; Eleftheriou, E.; Raftopoulos, V.; Michos, A.; Lourida, A.; Panopoulou, M.; Stamoulis, K.; Papaevangelou, V.; et al. Children and Adolescents With SARS-CoV-2 Infection: Epidemiology, Clinical Course and Viral Loads. Pediatr. Infect. Dis. J. 2020, 39, e388–e392. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Rangel, A.; Gómez-Romero, L.; Cisneros-Villanueva, M.; de Anda Jáuregui, G.; Luna-Pineda, V.; Cedro-Tanda, A.; Campos-Romero, A.; Mendoza-Vargas, A.; Reyes-Grajeda, J.P.; Hidalgo-Miranda, A.; et al. End-Point RT-PCR Based on a Conservation Landscape for SARS-COV-2 Detection. Sci. Rep. 2022, 12, 4759. [Google Scholar] [CrossRef] [PubMed]
- Cramér, H. Mathematical Methods of Statistics (PMS-9); Princeton University Press: Princeton, NJ, USA, 1999; ISBN 978-0-691-00547-8. [Google Scholar]
- Sanchez-Piedra, C.; Gamiño-Arroyo, A.-E.; Cruz-Cruz, C.; Prado-Galbarro, F.-J. Impact of Environmental and Individual Factors on COVID-19 Mortality in Children and Adolescents in Mexico: An Observational Study. Lancet Reg. Health Am. 2022, 8, 100184. [Google Scholar] [CrossRef]
- Singh, P.; Attri, K.; Mahto, D.; Kumar, V.; Kapoor, D.; Seth, A.; Singh, V.; Pemde, H.; Kumar, P.; Sodani, R.; et al. Clinical Profile of COVID-19 Illness in Children-Experience from a Tertiary Care Hospital. Indian J. Pediatr. 2022, 89, 45–51. [Google Scholar] [CrossRef]
- Satdhabudha, A.; Chaiyakulsil, C.; Sritipsukho, P.; Sinlapamongkolkul, P.; Chaumrattanakul, U.; Tangsathapornpong, A.; Bunjoungmanee, P.; Thaweekul, P.; Kwankua, A.; Pharadornuwat, O.; et al. Epidemiological and Clinical Characteristics of Pediatric COVID-19 in the Tertiary Care System in Thailand: Comparative Delta and Pre-Delta Era. Mediterr. J. Hematol. Infect. Dis. 2022, 14, e2022044. [Google Scholar] [CrossRef]
- Zhang, Z.-Z.; Chen, D.-P.; Liu, Q.-B.; Gan, C.; Jiang, L.; Zhu, K.; Zhang, X.-Y.; Xu, H.-M.; Huang, A.-L.; Long, Q.-X.; et al. Clinical Features of Chinese Children with COVID-19 and Other Viral Respiratory Infections. Pediatr. Pulmonol. 2022, 57, 49–56. [Google Scholar] [CrossRef]
- Martin, B.; DeWitt, P.E.; Russell, S.; Anand, A.; Bradwell, K.R.; Bremer, C.; Gabriel, D.; Girvin, A.T.; Hajagos, J.G.; McMurry, J.A.; et al. Characteristics, Outcomes, and Severity Risk Factors Associated With SARS-CoV-2 Infection Among Children in the US National COVID Cohort Collaborative. JAMA Netw. Open 2022, 5, e2143151. [Google Scholar] [CrossRef]
- Nikolopoulou, G.B.; Maltezou, H.C. COVID-19 in Children: Where Do We Stand? Arch. Med. Res. 2022, 53, 1–8. [Google Scholar] [CrossRef]
- Chaiyakulsil, C.; Sritipsukho, P.; Satdhabudha, A.; Bunjoungmanee, P.; Tangsathapornpong, A.; Sinlapamongkolkul, P.; Sritipsukho, N. An Epidemiological Study of Pediatric COVID-19 in the Era of the Variant of Concern. PLoS ONE 2022, 17, e0267035. [Google Scholar] [CrossRef]
- Funk, A.L.; Florin, T.A.; Kuppermann, N.; Tancredi, D.J.; Xie, J.; Kim, K.; Neuman, M.I.; Ambroggio, L.; Plint, A.C.; Mintegi, S.; et al. Outcomes of SARS-CoV-2–Positive Youths Tested in Emergency Departments: The Global PERN–COVID-19 Study. JAMA Netw. Open 2022, 5, e2142322. [Google Scholar] [CrossRef] [PubMed]
- Murugan, T.; Ghosh, U.; Rajan, R.J.; Punnen, A.; Chandran, J.; Das Adhikari, D.; Mathew, L.G.; Rose, W. Spectrum of COVID-19 Disease in Children: A Retrospective Analysis Comparing Wave 1 and Wave 2 from a Tertiary Hospital in South India. Indian J. Pediatr. 2022, 25, 1–7. [Google Scholar] [CrossRef]
- Kepenekli, E.; Yakut, N.; Ergenc, Z.; Aydıner, Ö.; Sarınoğlu, R.C.; Karahasan, A.; Karakoc-Aydıner, E.; Memişoğlu, A.; Gökdemir, Y.; Eralp, E.E.; et al. COVID-19 Disease Characteristics in Different Pediatric Age Groups. J. Infect. Dev. Ctries. 2022, 16, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.-H.; Yao, K.-H. Clinical Characteristics and Epidemiological Significance of Coronavirus Disease 2019 in Children and Adolescents. Zhongguo Dang Dai Er Ke Za Zhi Chin. J. Contemp. Pediatr. 2022, 24, 846–852. [Google Scholar] [CrossRef]
- Flores-Alanis, A.; Delgado, G.; Espinosa-Camacho, L.F.; Rodríguez-Gómez, F.; Cruz-Rangel, A.; Sandner-Miranda, L.; Cravioto, A.; Morales-Espinosa, R. Two Years of Evolutionary Dynamics of SARS-CoV-2 in Mexico, With Emphasis on the Variants of Concern. Front. Microbiol. 2022, 13, 886585. [Google Scholar] [CrossRef] [PubMed]
- Lugo-Zamudio, G.E.; Aguilar-Rojas, A.; Vázquez-Medina, M.U.; Gutiérrez-Ramírez, A.; Upton-Alvarado, M.C.; Espinoza-Rivas, P.; Lagunas-Torres, G.; Rojo-Gutiérrez, M.I.; Ibáñez-Cervantes, G.; Vargas-De-León, C. Epidemiological and Clinical Characteristics of Hospitalized Pediatric Patients with SARS-CoV-2 Infection in Mexico City, Mexico. Can. J. Infect. Dis. Med. Microbiol. J. Can. Mal. Infect. Microbiol. Med. 2022, 2022, 6780575. [Google Scholar] [CrossRef]
- Simões, E.; Silva, A.C.; Vasconcelos, M.A.; Colosimo, E.A.; Mendonça, A.C.Q.; Martelli-Júnior, H.; Silva, L.R.; Oliveira, M.C.L.; Pinhati, C.C.; Mak, R.H.; et al. Outcomes and Risk Factors of Death among Hospitalized Children and Adolescents with Obesity and COVID-19 in Brazil: An Analysis of a Nationwide Database. Pediatr. Obes. 2022, 17, e12920. [Google Scholar] [CrossRef]
- Setiadi, W.; Rozi, I.E.; Safari, D.; Daningrat, W.O.D.; Johar, E.; Yohan, B.; Yudhaputri, F.A.; Lestari, K.D.; Oktavianthi, S.; Myint, K.S.A.; et al. Prevalence and Epidemiological Characteristics of COVID-19 after One Year of Pandemic in Jakarta and Neighbouring Areas, Indonesia: A Single Center Study. PLoS ONE 2022, 17, e0268241. [Google Scholar] [CrossRef]
- Casas-Deza, D.; Bernal-Monterde, V.; Aranda-Alonso, A.N.; Montil-Miguel, E.; Julián-Gomara, A.B.; Letona-Giménez, L.; Arbones-Mainar, J.M. Age-Related Mortality in 61,993 Confirmed COVID-19 Cases over Three Epidemic Waves in Aragon, Spain. Implications for Vaccination Programmes. PLoS ONE 2021, 16, e0261061. [Google Scholar] [CrossRef]
- Guzman, B.V.; Elbel, B.; Jay, M.; Messito, M.J.; Curado, S. Age-Dependent Association of Obesity with COVID-19 Severity in Paediatric Patients. Pediatr. Obes. 2022, 17, e12856. [Google Scholar] [CrossRef]
- Marroquín-Yáñez, M.L.; Medeiros, M.; Chávez-López, A.; Carrillo-López, H.A.; Soto-Bautista, N.P.; Jarillo-Quijada, A.E.; Gómez-Murillo, S.Y.; Láscari-Jiménez, E.C.; Ruiz-Quiñones, G.; Barrera-Alonzo, C.J.; et al. Clinical Characteristics of Pediatric Patients with Acute Respiratory Distress Syndrome Due to COVID-19. Bol. Med. Hosp. Infant. Mex. 2022, 79, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.-Y.; Ellwood, P.; Ellwood, E.; García-Marcos, L.; Masekela, R.; Asher, I.; Badellino, H.; Sanz, A.B.; Douros, K.; El Sony, A.; et al. Infection with SARS-CoV-2 among Children with Asthma: Evidence from Global Asthma Network. Pediatr. Allergy Immunol. Off. Publ. Eur. Soc. Pediatr. Allergy Immunol. 2022, 33, e13709. [Google Scholar] [CrossRef] [PubMed]
- Feldman, A.G.; Danziger-Isakov, L.A. The Impact of COVID-19 on the Pediatric Solid Organ Transplant Population. Semin. Pediatr. Surg. 2022, 31, 151178. [Google Scholar] [CrossRef] [PubMed]
- Demeterco-Berggren, C.; Ebekozien, O.; Rompicherla, S.; Jacobsen, L.; Accacha, S.; Gallagher, M.P.; Todd Alonso, G.; Seyoum, B.; Vendrame, F.; Haw, J.S.; et al. Age and Hospitalization Risk in People With Type 1 Diabetes and COVID-19: Data From the T1D Exchange Surveillance Study. J. Clin. Endocrinol. Metab. 2022, 107, 410–418. [Google Scholar] [CrossRef]
- Djuric, O.; Ottone, M.; Vicentini, M.; Venturelli, F.; Pezzarossi, A.; Manicardi, V.; Greci, M.; Giorgi Rossi, P. Reggio Emilia Covid-19 Working Group Diabetes and COVID-19 Testing, Positivity, and Mortality: A Population-Wide Study in Northern Italy. Diabetes Res. Clin. Pract. 2022, 191, 110051. [Google Scholar] [CrossRef]
- Choi, J.H.; Choi, S.-H.; Yun, K.W. Risk Factors for Severe COVID-19 in Children: A Systematic Review and Meta-Analysis. J. Korean Med. Sci. 2022, 37, e35. [Google Scholar] [CrossRef]
- Harwood, R.; Yan, H.; Talawila Da Camara, N.; Smith, C.; Ward, J.; Tudur-Smith, C.; Linney, M.; Clark, M.; Whittaker, E.; Saatci, D.; et al. Which Children and Young People Are at Higher Risk of Severe Disease and Death after Hospitalisation with SARS-CoV-2 Infection in Children and Young People: A Systematic Review and Individual Patient Meta-Analysis. EClinicalMedicine 2022, 44, 101287. [Google Scholar] [CrossRef]
- Reiersen, J.; Romero-Hernández, M.; Adán-González, R. Government Reactions, Citizens’ Responses, and COVID-19 around the World. Int. J. Environ. Res. Public Health 2022, 19, 5667. [Google Scholar] [CrossRef]
- Brümmer, L.E.; Katzenschlager, S.; McGrath, S.; Schmitz, S.; Gaeddert, M.; Erdmann, C.; Bota, M.; Grilli, M.; Larmann, J.; Weigand, M.A.; et al. Accuracy of Rapid Point-of-Care Antigen-Based Diagnostics for SARS-CoV-2: An Updated Systematic Review and Meta-Analysis with Meta-Regression Analyzing Influencing Factors. PLoS Med. 2022, 19, e1004011. [Google Scholar] [CrossRef]
- Götzinger, F.; Strenger, V. The Role of Children and Young People in the Transmission of SARS-CoV-2. Pediatr. Infect. Dis. J. 2022, 41, e172–e174. [Google Scholar] [CrossRef]
- Alteri, C.; Scutari, R.; Costabile, V.; Colagrossi, L.; Yu La Rosa, K.; Agolini, E.; Lanari, V.; Chiurchiù, S.; Romani, L.; Markowich, A.H.; et al. Epidemiological Characterization of SARS-CoV-2 Variants in Children over the Four COVID-19 Waves and Correlation with Clinical Presentation. Sci. Rep. 2022, 12, 10194. [Google Scholar] [CrossRef] [PubMed]
- Kolodziej, L.M.; van Lelyveld, S.F.L.; Haverkort, M.E.; Mariman, R.; Sluiter-Post, J.G.C.; Badoux, P.; de Koff, E.M.; Koole, J.C.D.; Miellet, W.R.; Swart, A.N.; et al. High Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Household Transmission Rates Detected by Dense Saliva Sampling. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2022, 75, e10–e19. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total n (%, 95% CI) | Ambulatory n (%, 95% CI) | Hospitalized n (%, 95% CI) | p Value |
|---|---|---|---|---|
| Patient care | 1349 (100) | 846 (62.7,60.1–65.2) | 503 (37.3, 34.7–39.9) | <0.001 |
| Sex | ||||
| Female | 612 (45.4, 42.7–48.0) | 383 (62.6, 58.7–66.3) | 229 (37.4, 33.7–41.3) | <0.001 |
| Male | 737 (54.6, 52.0–57.3) | 463 (62.8, 59.3–66.2) | 274 (37.2, 33.8–40.7) | <0.001 |
| Age (years) | ||||
| <2 | 265 (19.6, 17.6–21.8) | 157 (59.2, 53.2–49.9) | 108 (40.8, 35.0–46.8) | <0.01 |
| 2–4 | 219 (16.2, 14.4–18.3) | 156 (71.2, 64.9–76.8) | 63 (28.8, 23.2–35.1) | <0.001 |
| 5–9 | 299 (22.2, 20.0–24.4) | 189 (63.2, 57.6–68.5) | 110 (36.8, 31.5–42.4) | <0.001 |
| 10–14 | 315 (23.3, 21.2–25.7) | 203 (64.4, 59.0–69.5) | 112 (35.6, 30.5–41.0) | <0.001 |
| 15–19 | 251 (18.6, 16.6–20.8) | 141 (56.2, 50.0–62.2) | 110 (43.8, 37.8–50.0) | ns |
| Diagnostic | ||||
| RT-qPCR | 528 (39.1, 36.6–41.8) | 241 (45.6, 41.4–50.0) | 287 (54.3, 50.1–58.5) | <0.05 |
| Rapid antigen test | 821 (60.9, 58.2–63.4) | 371 (45.2, 41.8–48.6) | 450 (54.8, 51.4–58.2) | <0.05 |
| Viral load | ||||
| Low | 257 (19, 17.0–21.2) | 152 (59.1, 53.0–65.0) | 105 (40.9, 35.0–46.9) | <0.05 |
| Moderate | 68 (5, 4.0–6.3) | 38 (55.9, 44.1–67.0) | 30 (44.1, 32.9–55.9) | ns |
| High | 203 (15, 13.2–17.0) | 123 (60.6, 53.7–67.0) | 80 (39.4, 32.9–46.3) | <0.05 |
| Non-determinate | 821 (61, 58.2–63.4) | 533 (64.9, 61.6–68.1) | 288 (35.1, 31.9–38.4) | <0.001 |
| SARS-CoV-2 infection | ||||
| Asymptomatic | 430 (31.9, 29.4–34.4) | 289 (67.2, 62.6–71.5) | 141 (32.8, 28.5–37.4) | <0.001 |
| Mild | 557 (41.3, 38.7–43.9) | 557 (100) | 0 | ND |
| Moderate | 323 (23.9, 21.7–26.3) | 0 | 323 (100) | ND |
| Severe | 39 (2.9, 2.1–3.9) | 0 | 39 (100) | ND |
| Comorbidities | ||||
| Immunosuppression | 126 (9.3, 7.9–11.0) | 50 (39.7, 31.6–48.4) | 76 (60.3, 51.6–68.4) | <0.05 |
| Cardiovascular disease (no hypertension) | 48 (3.6, 2.7–4.7) | 21 (43.7, 30.7–57.7) | 27 (56.3, 42.3–69.3) | ns |
| Obesity | 42 (3.1, 2.3–4.2) | 21 (50.0, 35.5–64.5) | 21 (50.0, 35.5–64.5) | ns |
| Asthma | 36 (2.7, 1.9–3.7) | 24 (66.7, 50.3–79.8) | 12 (33.3, 20.2–49.7) | <0.05 |
| Chronic kidney disease | 36 (2.7, 1.9–3.7) | 19 (52.8, 37.0–68.0) | 17 (47.2, 32.0–63.0) | ns |
| Chronic hypertension | 16 (1.2, 0.7–1.9) | 8 (50.0, 28.0–63.0) | 8 (50.0, 28.0–63.0) | ns |
| Diabetes mellitus | 9 (0.7, 0.3–1.2) | 4 (44.4, 18.9–73.3) | 5 (55.6, 26.7–81.1) | ns |
| Passive smoker or smoking | 9 (0.7, 0.3–1.2) | 4 (44.4, 18.9–73.3) | 5 (55.6, 26.7–81.1) | ns |
| HIV | 3 (0.2, 0.07–0.65) | 2 (67.0, 20.8–93.8) | 1 (33.0, 6.15–72.2) | ND |
| COPD | 2 (0.1, 0.04–0.54) | 1 (50.0, 9.45–90.5) | 1 (50.0, 9.45–90.5) | ND |
| Other diseases | 63 (4.7, 3.7–5.9) | 24 (38.1, 27.1–50.4) | 39 (61.9, 49.5–72.9) | ns |
| Signs/Symptoms | ||||
| Fever | 593 (43.9, 41.3–46.6) | 367 (61.9, 57.9–65.7) | 226 (38.1, 34.3–42.1) | <0.001 |
| Cough | 420 (31.1, 28.7–33.6) | 270 (64.3, 59.6–68.7) | 150 (35.7, 31.3–40.4) | <0.001 |
| Headache | 244 (18.1, 16.1–20.2) | 154 (63.1, 56.9–68.9) | 90 (36.9, 31.1–43.1) | <0.001 |
| Irritability | 230 (17, 15.1–19.1) | 136 (59.1, 52.7–65.3) | 94 (40.9, 34.7–47.3) | <0.001 |
| Rhinorrhea | 203 (15, 13.2–17.0) | 136 (67.0, 60.3–73.1) | 67 (33.0, 26.9–39.7) | <0.001 |
| Abdominal pain | 179 (13.3, 11.6–15.2) | 93 (52.0, 44.7–59.1) | 86 (48.0, 40.8–55.3) | ns |
| Vomiting | 173 (12.8, 11.1–14.7) | 94 (54.3, 46.9–61.6) | 79 (45.7, 38.4–53.1) | ns |
| Diarrhea | 167 (12.4, 10.7–14.2) | 85 (50.9, 43.4–58.4) | 82 (49.1, 41.6–56.6) | ns |
| Dyspnea | 166 (12.3, 10.6–14.2) | 94 (56.6, 49.0–63.9) | 72 (43.4, 36.1–51.0) | ns |
| Chills | 165 (12.2, 10.6–14.1) | 97 (58.8, 51.2–66.0) | 68 (41.2, 34.0–48.8) | <0.05 |
| Odynophagia | 145 (10.7, 9.2–12.5) | 98 (67.6, 59.6–74.7) | 47 (32.4, 25.3–40.4) | <0.001 |
| Myalgia | 140 (10.4, 8.9–12.1) | 84 (60.0, 51.7–67.7) | 56 (40.0, 32.2–48.3) | <0.05 |
| Thoracic pain | 110 (8.1, 6.8–9.7) | 66 (60.0, 50.6–68.7) | 44 (40.0, 31.3–49.3) | <0.05 |
| Polypnea | 119 (8.8, 7.4–10.4) | 63 (52.9, 44.0–61.7) | 56 (47.1, 38.3–56.0) | ns |
| Arthralgia | 102 (7.6, 6.3–9.1) | 63 (61.8, 52.1–70.6) | 39 (38.2, 29.4–47.9) | <0.05 |
| Conjunctivitis | 63 (4.7, 3.7–5.9) | 39 (61.9, 49.5–72.9) | 24 (38.1, 27.1–50.4) | ns |
| Anosmia | 48 (3.6, 2.7–4.7) | 29 (60.4, 46.3–73.0) | 19 (39.6, 27.0–53.7) | ns |
| Cyanosis | 43 (3.2, 2.4–4.3) | 27 (62.8, 47.8–75.6) | 16 (37.2, 24.4–52.1) | ns |
| Dysgeusia | 39 (2.9, 2.1–3.9) | 28 (71.8, 56.2–83.4) | 11 (28.2, 16.5–43.8) | <0.001 |
| Viral Load | ||||||||
|---|---|---|---|---|---|---|---|---|
| Variable n (%) | Total, n = 528 (%, 95% CI) | p Value | Low a, n = 257 (%, 95% CI) | p Value | Moderate b, n = 68 (%, 95% CI) | p Value | High c, n = 203 (%, 95% CI) | p Value |
| Gender | ||||||||
| Female | 241 (45.6, 41.4–50.0) | <0.05 | 119 (46.3, 40.3–52.4) | ns | 35 (51.5, 39.8–62.9) | ns | 87 (42.9, 36.2–49.7) | <0.05 |
| Male | 287 (54.4, 50.1–58.5) | 138 (53.7, 47.6–59.7) | 33 (48.5, 37.0–60.2) | 116 (57.1, 50.3–63.7) | ||||
| Age (years) | ||||||||
| <2 | 77 (14.6, 11.8–17.8) | Ref | 32 (12.4, 8.9–17.0) | Ref | 11 (16.2, 9.3–26.7) | Ref | 34 (16.7, 12.2–22.5) | Ref |
| 2–4 | 92 (17.4, 14.4–20.9) | ns | 47 (18.3, 14.0–23.5) | ns | 9 (13.2, 7.1–23.3) | ns | 36 (17.7, 13.1–23.6) | ns |
| 5–9 | 135 (25.6, 22.0–29.4) | <0.001 | 76 (29.6, 24.3–35.4) | <0.001 | 11 (16.2, 9.3–26.7) | ns | 48 (23.6, 18.3–29.9) | ns |
| 10–14 | 127 (24.0, 20.6–27.9) | <0.001 | 60 (23.3, 18.6–28.9) | <0.05 | 21 (30.9, 21.2–42.6) | ns | 46 (22.7, 17.4–28.9) | ns |
| 15–19 | 97 (18.4, 15.3–21.9) | ns | 42 (16.3, 12.3–21.3) | ns | 16 (23.5, 15.0–34.8) | ns | 39 (19.2, 14.4–25.2) | ns |
| Patient care | ||||||||
| Ambulatory | 313 (59.3, 55.0–63.4) | <0.001 | 152 (59.1, 53–65) | <0.05 | 38 (55.9, 44.1–67.0) | ns | 123 (60.6, 53.7–67.0) | <0.05 |
| Hospitalized | 215 (40.7, 36.6–45.0) | 105 (40.9, 35–47) | 30 (44.1, 32.9–55.9) | 80 (39.4, 32.9–46.3) | ||||
| SARS-CoV-2 infection | ||||||||
| Asymptomatic | 169 (32, 28.2–36.1) | ref | 84 (32.7, 27.2–38.6) | ref | 24 (35.3, 25.0–47.1) | ref | 61 (30.0, 24.2–36.7) | ref |
| Mild | 203 (38.4, 34.4–42.7) | ns | 98 (38.1, 32.4–44.2) | ns | 23 (33.8, 23.7–45.7) | ns | 82 (40.4, 33.9–47.3) | ns |
| Moderate | 134 (25.4, 21.8–29.2) | <0.05 | 60 (23.3, 18.6–28.9) | <0.05 | 19 (27.9, 18.7–39.6) | ns | 55 (27.1, 21.4–33.6) | ns |
| Severe | 22 (4.2, 2.8–6.2) | <0.001 | 15 (5.8, 3.6–9.4) | <0.001 | 2 (2.9, 0.8–10.1) | <0.001 | 5 (2.5, 1.0–5.6) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flores-Alanis, A.; Saldaña-Ahuactzi, Z.; Parra-Ortega, I.; López-Ramírez, P.; Salazar-García, M.; Alemán-García, Y.P.; Cruz-Rangel, A.; Moreno-Paredes, A.; Diaz-Rojas, A.; Maldonado-Bernal, C.; et al. Clinical Characteristics of Coronavirus Disease (COVID-19) in Mexican Children and Adolescents. Viruses 2022, 14, 2162. https://doi.org/10.3390/v14102162
Flores-Alanis A, Saldaña-Ahuactzi Z, Parra-Ortega I, López-Ramírez P, Salazar-García M, Alemán-García YP, Cruz-Rangel A, Moreno-Paredes A, Diaz-Rojas A, Maldonado-Bernal C, et al. Clinical Characteristics of Coronavirus Disease (COVID-19) in Mexican Children and Adolescents. Viruses. 2022; 14(10):2162. https://doi.org/10.3390/v14102162
Chicago/Turabian StyleFlores-Alanis, Alejandro, Zeus Saldaña-Ahuactzi, Israel Parra-Ortega, Pablo López-Ramírez, Marcela Salazar-García, Yolanda P. Alemán-García, Armando Cruz-Rangel, Alba Moreno-Paredes, Adrián Diaz-Rojas, Carmen Maldonado-Bernal, and et al. 2022. "Clinical Characteristics of Coronavirus Disease (COVID-19) in Mexican Children and Adolescents" Viruses 14, no. 10: 2162. https://doi.org/10.3390/v14102162