
Heart Rate Variability in Elite Swimmers before, during and after COVID-19 Lockdown: A Brief Report on Time Domain Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Data Collection
2.3. Statistics
3. Results
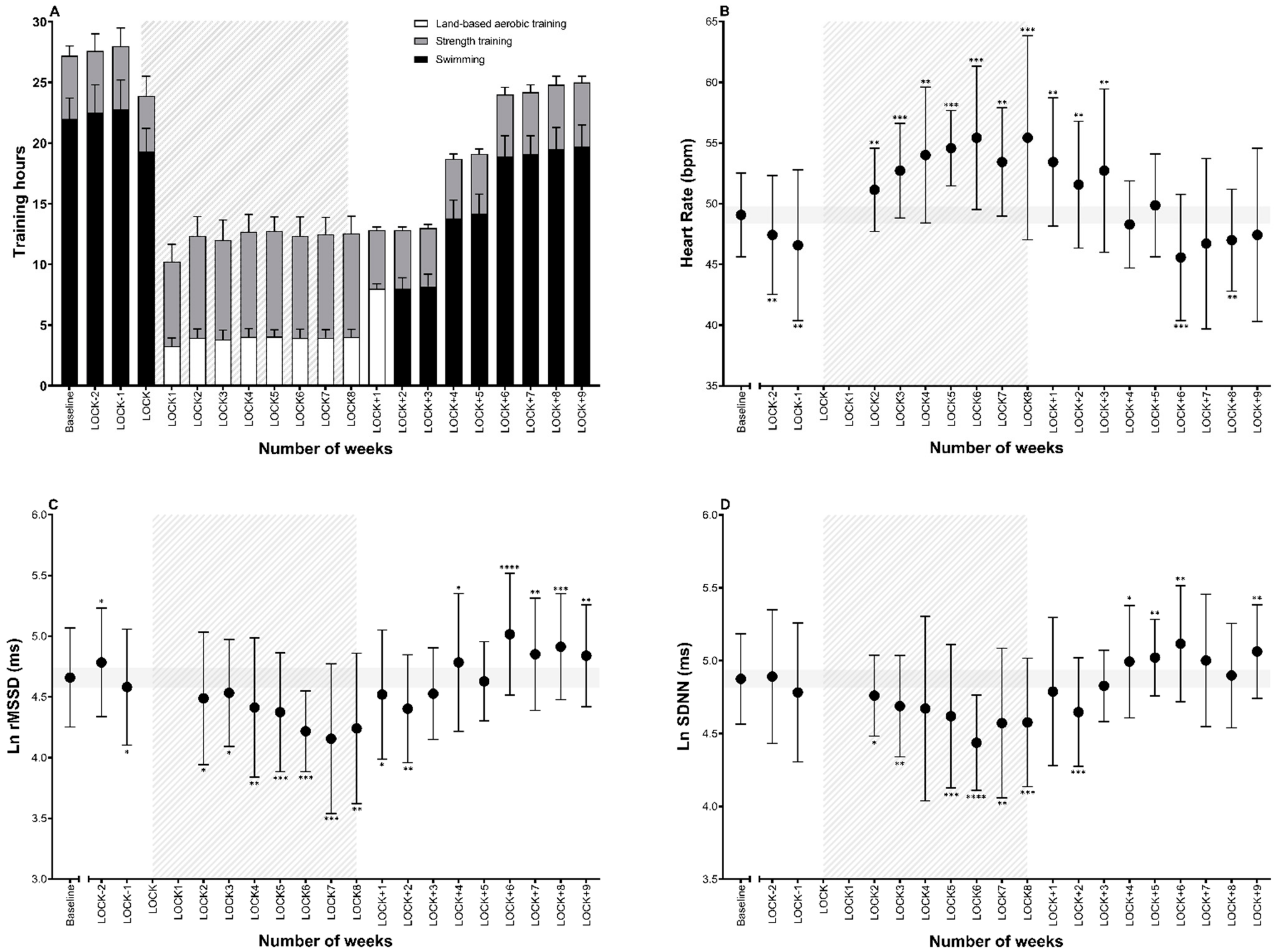
3.1. Training Volume
3.2. HRV Changes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Novel Coronavirus (2019-nCoV). Situation Report—100. April 2020. Available online: https//www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 10 May 2021).
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef]
- Sarto, F.; Impellizzeri, F.M.; Spörri, J.; Porcelli, S.; Olmo, J.; Requena, B.; Suarez-Arrones, L.; Arundale, A.; Bilsborough, J.; Buchheit, M.; et al. Impact of Potential Physiological Changes due to COVID-19 Home Confinement on Athlete Health Protection in Elite Sports: A Call for Awareness in Sports Programming. Sports Med. 2020, 50, 1417–1419. [Google Scholar] [CrossRef] [PubMed]
- Mon-López, D.; de la Rubia Riaza, A.; Hontoria Galán, M.; Refoyo Roman, I. The Impact of Covid-19 and the Effect of Psychological Factors on Training Conditions of Handball Players. Int. J. Environ. Res. Public Health 2020, 17, 6471. [Google Scholar] [CrossRef]
- di Cagno, A.; Buonsenso, A.; Baralla, F.; Grazioli, E.; Di Martino, G.; Lecce, E.; Calcagno, G.; Fiorilli, G. Psychological Impact of the Quarantine-Induced Stress during the Coronavirus (COVID-19) Outbreak among Italian Athletes. Int. J. Environ. Res. Public Health 2020, 17, 8867. [Google Scholar] [CrossRef]
- Ruffault, A.; Bernier, M.; Fournier, J.; Hauw, N. Anxiety and Motivation to Return to Sport During the French COVID-19 Lockdown. Front. Psychol. 2020, 11, 610882. [Google Scholar] [CrossRef]
- Fikenzer, S.; Fikenzer, K.; Laufs, U.; Falz, R.; Pietrek, H.; Hepp, P. Impact of COVID-19 lockdown on endurance capacity of elite handball players. J. Sports Med. Phys. Fit. 2020, 61, 977–982. [Google Scholar] [CrossRef]
- Herrera-Valenzuela, T.; Narrea Vargas, J.J.; Merlo, R.; Valdés-Badilla, P.A.; Pardo-Tamayo, C.; Franchini, E. Effect of the COVID-19 quarantine on body mass among combat sports athletes. Nutr. Hosp. 2020, 37, 1186–1189. [Google Scholar] [CrossRef] [PubMed]
- Pla, R.; Bosquet, L.; Aubry, A.; Toussaint, J.F.; Sedeaud, A. Resting Heart Rate Measurement in Elite Athletes during COVID-19 Lockdown: The Impact of Decreased Physical Activity. Sustainability 2021, 13, 2970. [Google Scholar] [CrossRef]
- Plews, D.J.; Laursen, P.B.; Stanley, J.; Kilding, A.E.; Buchheit, M. Training adaptation and heart rate variability in elite endurance athletes: Opening the door to effective monitoring. Sports Med. 2013, 43, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Task Force Report. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Atlaoui, D.; Pichot, V.; Lacoste, L.; Barale, F.; Lacour, J.R.; Chatard, J.C. Heart rate variability, training variation and performance in elite swimmers. Int. J. Sports Med. 2007, 28, 394–400. [Google Scholar] [CrossRef]
- Blásquez, J.C.C.; Font, G.R.; Ortís, L.C. Heart-rate variability and precompetitive anxiety in swimmers. Psicothema 2009, 21, 531–536. [Google Scholar]
- Fortes, L.S.; da Costa, B.; Paes, P.P.; do Nascimento Júnior, J.; Fiorese, L.; Ferreira, M. Influence of Competitive-Anxiety on Heart Rate Variability in Swimmers. J. Sports Sci. Med. 2017, 16, 498–504. [Google Scholar]
- Pla, R.; Aubry, A.; Resseguier, N.; Merino, M.; Toussaint, J.F.; Hellard, P. Training Organization, Physiological Profile and Heart Rate Variability Changes in an Open-water World Champion. Int. J. Sports Med. 2019, 40, 519–527. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopkins, W.G. Spreadsheets for analysis of controlled trials with adjustment for a subject characteristic. Sportscience 2006, 10, 46–50. [Google Scholar]
- Plews, D.J.; Laursen, P.B.; Buchheit, M. Day-to-Day Heart-Rate Variability Recordings in World-Champion Rowers: Appreciating Unique Athlete Characteristics. Int. J. Sports Physiol. Perform. 2017, 12, 697–703. [Google Scholar] [CrossRef]
- Stanley, J.; D’Auria, S.; Buchheit, M. Cardiac parasympathetic activity and race performance: An elite triathlete case study. Int. J. Sports Physiol. Perform. 2015, 10, 528–534. [Google Scholar] [CrossRef]
- Hansen, A.L.; Johnsen, B.H.; Sollers, J.J., 3rd; Stenvik, K.; Thayer, J.F. Heart rate variability and its relation to prefrontal cognitive function: The effects of training and detraining. Eur. J. Appl. Physiol. 2004, 93, 263–272. [Google Scholar] [CrossRef]
- Pereira, L.A.; Nakamura, F.Y.; Castilho, C.; Kitamura, K.; Kobal, R.; Cal Abad, C.C.; Loturco, I. The impact of detraining on cardiac autonomic function and specific endurance and muscle power performances of high-level endurance runners. J. Sports Med. Phys. Fit. 2016, 56, 1583–1591. [Google Scholar]
- Gamelin, F.X.; Berthoin, S.; Sayah, H.; Libersa, C.; Bosquet, L. Effect of training and detraining on heart rate variability in healthy young men. Int. J. Sports Med. 2007, 28, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Gindre, C. Cardiac parasympathetic regulation: Respective associations with cardiorespiratory fitness and training load. Am. J. Physiol. Heart Circ. Physiol. 2006, 291, H451–H458. [Google Scholar] [CrossRef]
- Flatt, A.A.; Hornikel, B.; Esco, M.R. Heart rate variability and psychometric responses to overload and tapering in collegiate sprint-swimmers. J. Sci. Med. Sport 2017, 20, 606–610. [Google Scholar] [CrossRef] [PubMed]
- Licht, C.M.; de Geus, E.J.; van Dyck, R.; Penninx, B.W. Association between anxiety disorders and heart rate variability in The Netherlands Study of Depression and Anxiety (NESDA). Psychosom. Med. 2009, 71, 508–518. [Google Scholar] [CrossRef] [Green Version]
- García-Pallarés, J.; Carrasco, L.; Díaz, A.; Sánchez-Medina, L. Post-season detraining effects on physiological and performance parameters in top-level kayakers: Comparison of two recovery strategies. J. Sports Sci. Med. 2009, 8, 622–628. [Google Scholar]
- Saw, A.E.; Main, L.C.; Gastin, P.B. Monitoring the athlete training response: Subjective self-reported measures trump commonly used objective measures: A systematic review. Br. J. Sports Med. 2016, 50, 281–291. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Training Period | Date | Monday | Tuesday | Wednesday | Thursday | Friday | Saturday | Sunday |
|---|---|---|---|---|---|---|---|---|
| Baseline | AM | Swimming | Swimming | Swimming | Swimming | Swimming | Swimming | Rest |
| PM | Swimming + ST | Swimming + ST | Swimming + ST | Swimming + ST | Swimming + ST | Rest | Rest | |
| BEF | AM | Swimming | Swimming | Swimming | Swimming | Swimming | Swimming | Rest |
| PM | Swimming + ST | Swimming + ST | Swimming + ST | Swimming + ST | Swimming + ST | Rest | Rest | |
| LOCK | AM | Aerobic | Flexibility | Aerobic | Flexibility | Aerobic | ST or Aerobic | Rest |
| PM | ST | ST | Flexibility | ST | ST | Rest | Rest | |
| AFT1 | AM | Aerobic | Aerobic | Aerobic | Aerobic | Aerobic | Rest | Rest |
| PM | ST | ST | ST | ST | ST | Rest | Rest | |
| AFT2–3 | AM | Swimming | Swimming | Swimming | Swimming | Swimming | Rest | Rest |
| PM | ST | ST | ST | ST | ST | Rest | Rest | |
| AFT4–5 | AM | Swimming | Swimming | Swimming | Swimming | Swimming | Rest | Rest |
| PM | Swimming + ST | ST | Swimming + ST | ST | Swimming + ST | Rest | Rest | |
| AFT6–9 | AM | Swimming | Swimming | Swimming | Swimming | Swimming | Swimming | Rest |
| PM | Swimming + ST | Swimming + ST | Swimming + ST | Swimming + ST | Swimming + ST | Rest | Rest |
| Heart Rate | Ln RMSSD | Ln SDNN | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Weeks | ES | CL | Inference | p-Value | ES | CL | Inference | p-Value | ES | CL | Inference | p-Value |
| 0–1 | −0.34 | 0.32 | 1/21/78 | 0.09 | 0.25 | 0.19 | 70/30/0 | 0.04 | 0.04 | 0.63 | 31/44/25 | 0.92 |
| 0–2 | −0.43 | 0.52 | 3/18/79 | 0.16 | −0.15 | 0.25 | 2/62/37 | 0.28 | −0.20 | 0.57 | 11/39/50 | 0.52 |
| 0–3 | X | X | X | X | X | X | X | X | X | X | X | X |
| 0–4 | X | X | X | X | X | X | X | X | X | X | X | X |
| 0–5 | 0.52 | 0.67 | 81/15/4 | 0.18 | −0.31 | 0.35 | 1/27/72 | 0.14 | −0.34 | 0.39 | 2/24/74 | 0.15 |
| 0–6 | 0.86 | 0.48 | 98/2/0 | 0.01 | −0.26 | 0.38 | 3/36/61 | 0.23 | −0.49 | 0.54 | 2/14/83 | 0.13 |
| 0–7 | 0.92 | 0.81 | 93/5/2 | 0.07 | −0.43 | 0.39 | 1/14/85 | 0.08 | −0.35 | 0.63 | 7/26/68 | 0.31 |
| 0–8 | 1.46 | 0.91 | 98/1/1 | 0.02 | −0.55 | 0.31 | 0/3/97 | 0.01 | −0.54 | 0.34 | 0/5/95 | 0.02 |
| 0–9 | 1.14 | 0.63 | 99/1/0 | 0.01 | −1.03 | 0.68 | 1/2/97 | 0.03 | −1.20 | 0.44 | 0/0/100 | 0.00 |
| 0–10 | 0.95 | 0.82 | 94/5/2 | 0.07 | −0.84 | 0.41 | 0/1/99 | 0.01 | −0.62 | 0.53 | 1/7/91 | 0.06 |
| 0–11 | 0.86 | 0.64 | 96/4/1 | 0.04 | −0.69 | 0.53 | 1/5/94 | 0.04 | −0.68 | 0.39 | 0/2/97 | 0.01 |
| 0–12 | 0.85 | 0.65 | 95/4/1 | 0.04 | −0.26 | 0.39 | 3/36/61 | 0.25 | −0.18 | 0.55 | 11/41/47 | 0.55 |
| 0–13 | 0.49 | 0.60 | 81/16/3 | 0.17 | −0.52 | 0.36 | 0/6/93 | 0.03 | −0.58 | 0.27 | 0/2/98 | 0.01 |
| 0–14 | 0.59 | 0.58 | 88/10/2 | 0.09 | −0.30 | 0.54 | 6/31/63 | 0.33 | −0.15 | 0.71 | 19/37/45 | 0.70 |
| 0–15 | −0.19 | 0.47 | 8/43/49 | 0.46 | 0.22 | 0.32 | 54/43/2 | 0.23 | 0.30 | 0.38 | 68/30/2 | 0.18 |
| 0–16 | 0.18 | 0.57 | 47/41/12 | 0.57 | −0.08 | 0.32 | 7/69/24 | 0.66 | 0.44 | 0.46 | 82/16/2 | 0.11 |
| 0–17 | −0.69 | 0.44 | 0/3/96 | 0.02 | 0.68 | 0.23 | 100/0/0 | 0.00 | 0.59 | 0.41 | 94/5/1 | 0.03 |
| 0–18 | −0.37 | 0.60 | 6/24/70 | 0.28 | 0.38 | 0.28 | 87/12/0 | 0.04 | 0.28 | 0.70 | 59/30/1 | 0.46 |
| 0–19 | −0.47 | 0.47 | 2/14/84 | 0.10 | 0.52 | 0.24 | 98/2/0 | 0.01 | 0.06 | 0.61 | 34/44/22 | 0.86 |
| 0–20 | −0.25 | 0.49 | 6/36/58 | 0.35 | 0.38 | 0.42 | 78/20/2 | 0.13 | 0.52 | 0.51 | 86/12/2 | 0.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pla, R.; Bosquet, L.; McGibbon, K.; Mujika, I.; Aubry, A. Heart Rate Variability in Elite Swimmers before, during and after COVID-19 Lockdown: A Brief Report on Time Domain Analysis. Appl. Sci. 2021, 11, 8106. https://doi.org/10.3390/app11178106
Pla R, Bosquet L, McGibbon K, Mujika I, Aubry A. Heart Rate Variability in Elite Swimmers before, during and after COVID-19 Lockdown: A Brief Report on Time Domain Analysis. Applied Sciences. 2021; 11(17):8106. https://doi.org/10.3390/app11178106
Chicago/Turabian StylePla, Robin, Laurent Bosquet, Katie McGibbon, Iñigo Mujika, and Anaël Aubry. 2021. "Heart Rate Variability in Elite Swimmers before, during and after COVID-19 Lockdown: A Brief Report on Time Domain Analysis" Applied Sciences 11, no. 17: 8106. https://doi.org/10.3390/app11178106