
Prevalence of Depression and Anxiety in Nurses during the First Eleven Months of the COVID-19 Pandemic: A Systematic Review and Meta-Analysis

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Selection Criteria
2.4. Data Extraction
2.5. Quality Assessment
2.6. Ethical Approval
2.7. Statistics Analysis
3. Results
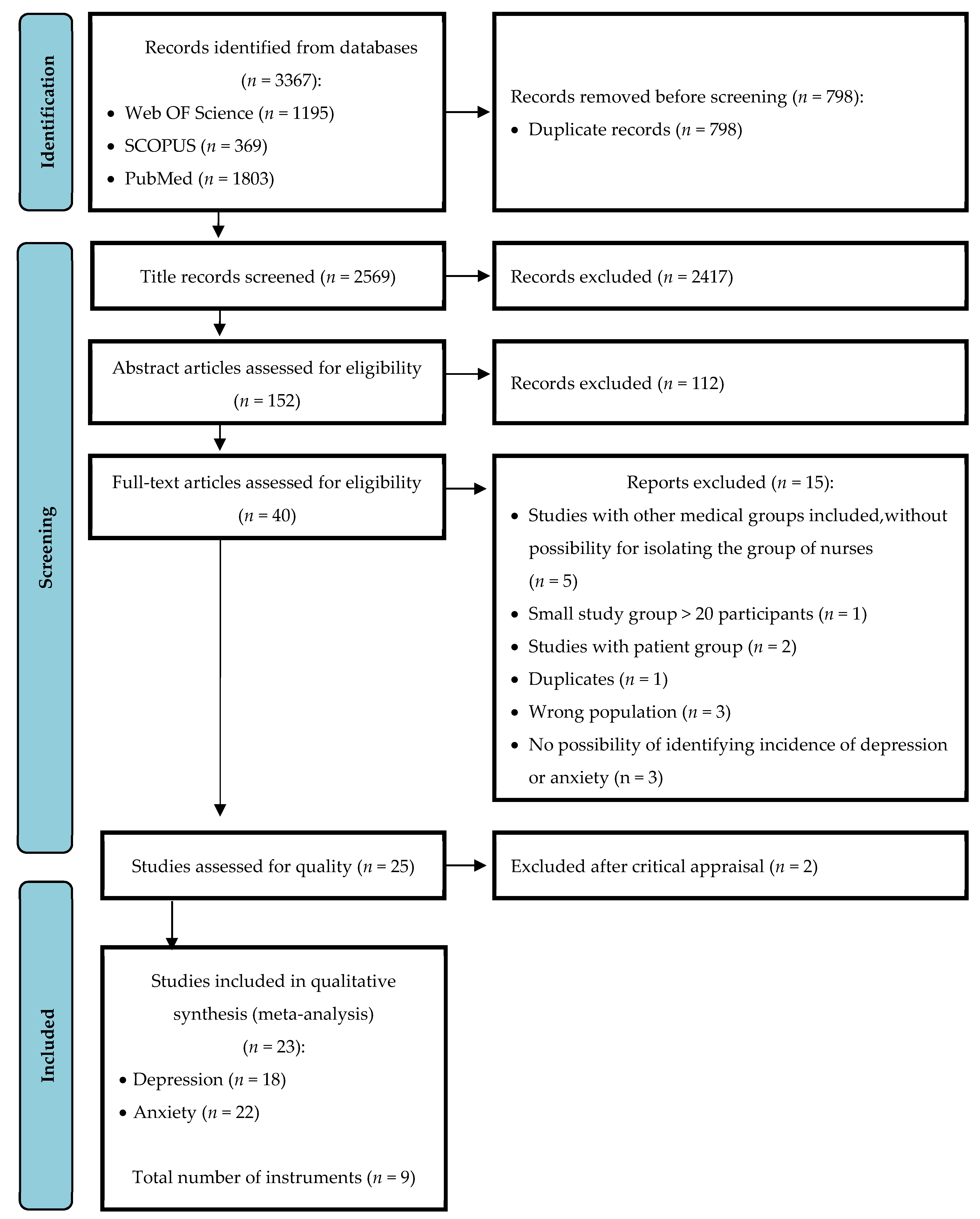
3.1. Study Inclusion
3.2. Description of Included Studies
3.3. Quality Assessment
3.4. Characteristics of Instruments Used to Assess Depression and Anxiety Levels
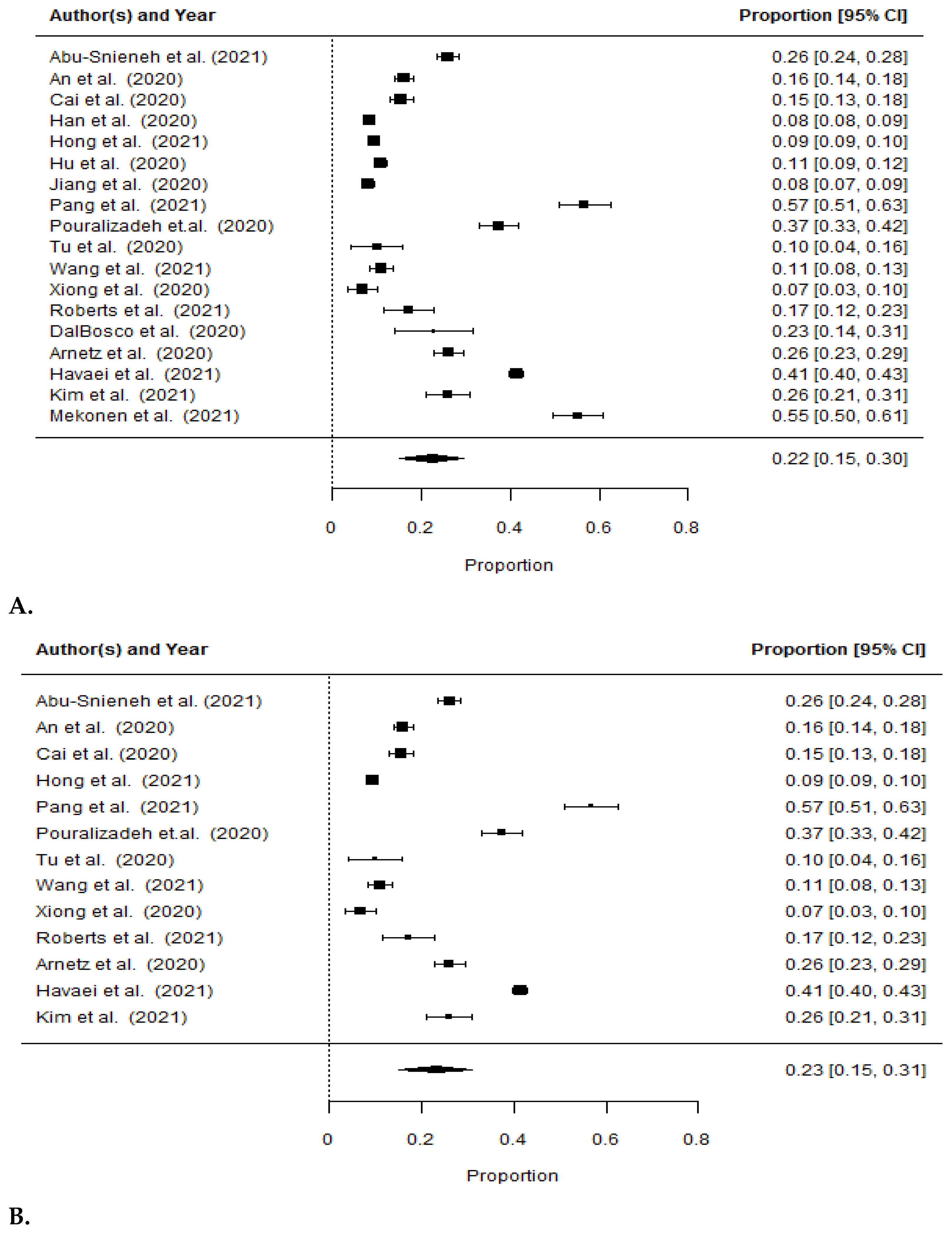
3.5. Incidence of Depression among Nurses during the COVID-19 Pandemic
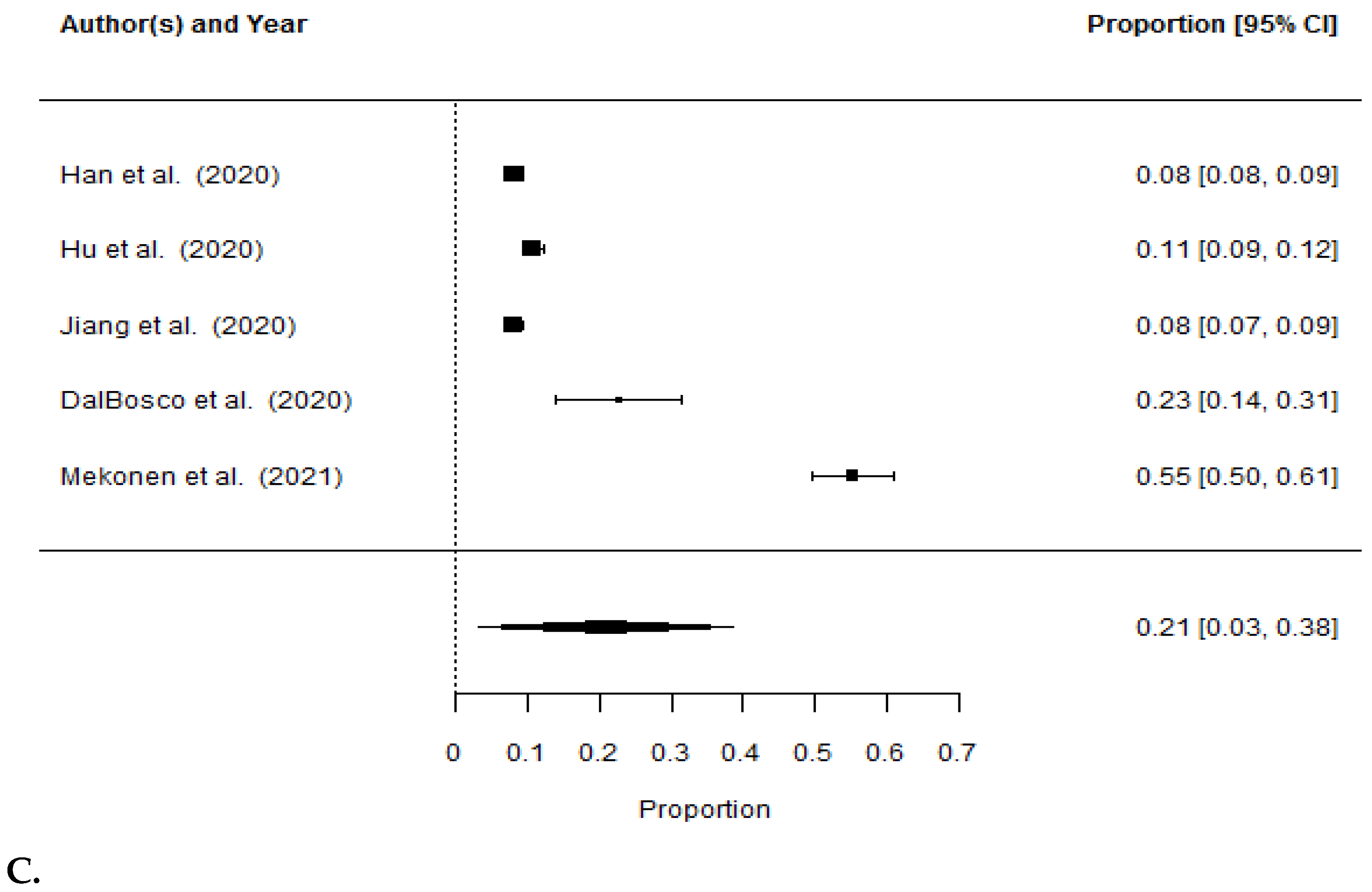
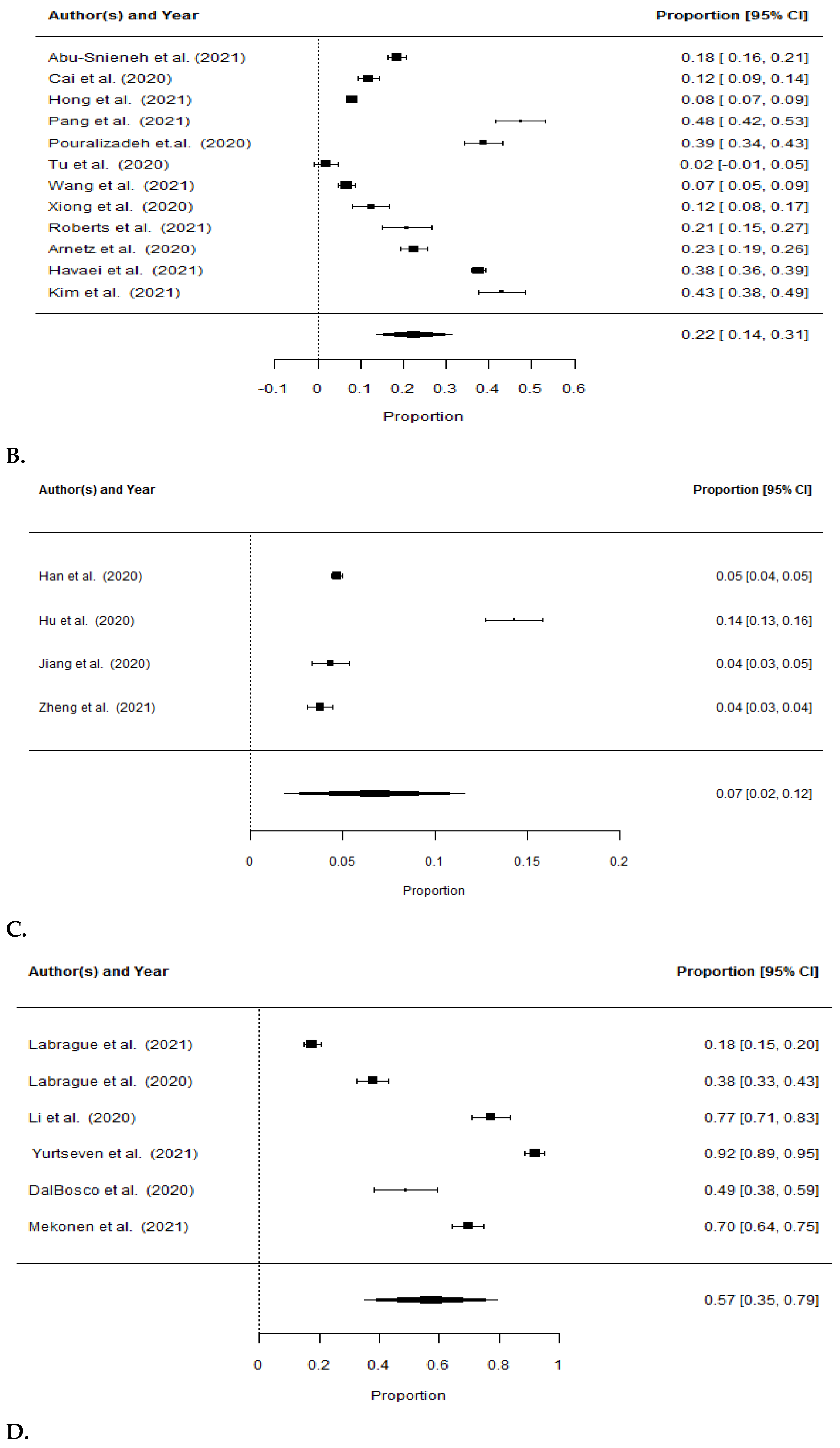
3.6. Incidence of Anxiety among Nurses during the COVID-19 Pandemic
3.7. Factors Relating to the Incidence of Depression and Anxiety
3.8. Publication Bias
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aiken, L.H.; Sloane, D.M.; Bruyneel, L.; Van den Heede, K.; Sermeus, W.; RN4CAST Consortium. Nurses’ reports of working conditions and hospital quality of care in 12 countries in Europe. Int. J. Nurs. Stud. 2013, 50, 143–153. [Google Scholar] [CrossRef]
- World Health Organization. Announces COVID-19 Outbreak a Pandemic Retrieved. Available online: http://www.euro.who.int/en/heps//:coronavirus.jhu.edu/map.alth-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed on 10 March 2021).
- Pfefferbaum, B.; North, C.S. Mental health and the COVID-19 pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Li, X.; Zhou, Y.; Xu, X. Factors associated with the psychological well-being among front-line nurses exposed to COVID-2019 in China: A predictive study. J. Nurs. Manag. 2021, 29, 240–249. [Google Scholar] [CrossRef]
- Halcomb, E.; McInnes, S.; Williams, A.; Ashley, C.; James, S.; Fernandez, R.; Stephen, C.; Calma, K. The experiences of primary healthcare nurses during the COVID-19 pandemic in Australia. J. Nurs. Scholarsh. 2020, 52, 553–563. [Google Scholar] [CrossRef]
- Kim, S.C.; Quiban, C.; Sloan, C.; Montejano, A. Predictors of poor mental health among nurses during COVID-19 pandemic. Nurs. Open. 2021, 8, 900–907. [Google Scholar] [CrossRef]
- Di Tella, M.; Romeo, A.; Benfante, A.; Castelli, L. Mental health of healthcare workers during the COVID-19 pandemic in Italy. J. Eval. Clin. Pract. 2020, 26, 1583–1587. [Google Scholar] [CrossRef]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.E.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef]
- Arnetz, J.E.; Goetz, C.M.; Sudan, S.; Arble, E.; Janisse, J.; Arnetz, B.B. Personal protective equipment and mental health symptoms among nurses during the COVID-19 pandemic. J. Occup. Environ. Med. 2020, 62, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Zaka, A.; Shamloo, S.E.; Fiorente, P.; Tafuri, A. COVID-19 pandemic as a watershed moment: A call for systematic psychological health care for frontline medical staff. J. Health Psychol. 2020, 25, 883–887. [Google Scholar] [CrossRef] [PubMed]
- James, R.K.; Gilliland, B.E. Crisis Intervention Strategies; Cengage Learning: Belmont, MA, USA, 2017. [Google Scholar]
- Li, X.; Li, S.; Xiang, M.; Fang, Y.; Qian, K.; Xu, J.; Li, J.; Zhang, Z.; Wang, B. The prevalence and risk factors of PTSD symptoms among medical assistance workers during the COVID-19 pandemic. J. Psychosom. Res. 2020, 139, 110270. [Google Scholar] [CrossRef] [PubMed]
- Heitzman, J. Impact of COVID-19 pandemic on mental health. Psychiatr. Pol. 2020, 54, 187–198. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatr. 2020, 52, 102066. [Google Scholar] [CrossRef]
- Sahebi, A.; Nejati-Zarnaqi, B.; Moayedi, S.; Yousefi, K.; Torres, M.; Golitaleb, M. The prevalence of anxiety and depression among healthcare workers during the COVID-19 pandemic: An umbrella review of meta-analyses. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 107, 110247. [Google Scholar] [CrossRef]
- Fernandez, R.; Sikhosana, N.; Green, H.; Halcomb, E.J.; Middleton, R.; Alananzeh, I.; Trakis, S.; Moxham, L. Anxiety and depression among healthcare workers during the COVID-19 pandemic: A systematic umbrella review of the global evidence. BMJ Open. 2021, 11, e054528. [Google Scholar] [CrossRef]
- Goldmann, E.; Galea, S. Mental health consequences of disasters. Annu. Rev. Public Health 2014, 35, 169–183. [Google Scholar] [CrossRef]
- Olaya, B.; Pérez-Moreno, M.; Bueno-Notivol, J.; Gracia-García, P.; Lasheras, I.; Santabárbara, J. Prevalence of depression among healthcare workers during the COVID-19 outbreak: A systematic review and meta-analysis. J. Clin. Med. 2021, 10, 3406. [Google Scholar] [CrossRef] [PubMed]
- Al Maqbali, M.; Al Sinani, M.; Al-Lenjawi, B. Prevalence of stress, depression, anxiety and sleep disturbance among nurses during the COVID-19 pandemic: A systematic review and meta-analysis. J. Psychosom. Res. 2021, 141, 110343. [Google Scholar] [CrossRef] [PubMed]
- Varghese, A.; George, G.; Kondaguli, S.V.; Naser, A.Y.; Khakha, D.C.; Chatterji, R. Decline in the mental health of nurses across the globe during COVID-19: A systematic review and meta-analysis. J. Glob. Health 2021, 11, 05009. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Rostom, A.; Dube, C.; Cranney, A.; Saloojee, N.; Sy, R.; Garritty, C.; Sampson, M.; Zhang, L.; Yazdi, F.; Mamaladze, V.; et al. Celiac disease. Evid. Rep. Technol. Assess. (Summ.) 2004, 104, 1–6. [Google Scholar]
- Cai, Z.; Cui, Q.; Liu, Z.; Li, J.; Gong, X.; Liu, J.; Wan, Z.; Yuan, X.; Li, X.; Chen, C.; et al. Nurses endured high risks of psychological problems under the epidemic of COVID-19 in a longitudinal study in Wuhan China. J. Psychiatr. Res. 2020, 131, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Havaei, F.; Ma, A.; Staempfli, S.; MacPhee, M. Nurses’ workplace conditions impacting their mental health during COVID-19: A cross-sectional survey study. Healthcare 2021, 9, 84. [Google Scholar] [CrossRef] [PubMed]
- Abu-Snieneh, H.M. Psychological factors associated with the spread of Coronavirus disease 2019 (COVID-19) among nurses working in health sectors in Saudi Arabia. Perspect. Psychiatr. Care. 2021, 57, 1399–1408. [Google Scholar] [CrossRef] [PubMed]
- An, Y.; Yang, Y.; Wang, A.; Li, Y.; Zhang, Q.; Cheung, T.; Ungvari, G.S.; Qin, M.Z.; An, F.R.; Xiang, Y.T. Prevalence of depression and its impact on quality of life among frontline nurses in emergency departments during the COVID-19 outbreak. J. Affect Disord. 2020, 276, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Han, L.; Wong, F.K.Y.; She, D.L.M.; Li, S.Y.; Yang, Y.F.; Jiang, M.Y.; Ruan, Y.; Su, Q.; Ma, Y.; Chung, L.Y.F. Anxiety and depression of nurses in a North West Province in China during the period of novel coronavirus pneumonia outbreak. J. Nurs. Scholarsh. 2020, 52, 564–573. [Google Scholar] [CrossRef]
- Hu, D.; Kong, Y.; Li, W.; Han, Q.; Zhang, X.; Zhu, L.X.; Wan, S.W.; Liu, Z.; Shen, Q.; Yang, J.; et al. Frontline nurses’ burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: A large-scale cross-sectional study. EClinicalMedicine 2020, 24, 100424. [Google Scholar] [CrossRef]
- Jiang, M.; Li, S.; She, D.; Yan, F.; Chung, Y.F.; Han, L. The psychological effect of 2019 coronavirus disease outbreak on nurses living in Islamic culture dominant region, China. Arch. Psychiatr. Nurs. 2020, 34, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.J.; De Los Santos, J.A.A. COVID-19 anxiety among front-line nurses: Predictive role of organisational support, personal resilience and social support. J. Nurs. Manag. 2020, 28, 1653–1661. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.J.; De Los Santos, J.A.A. Prevalence and predictors of coronaphobia among frontline hospital and public health nurses. Public Health Nurs. 2021, 38, 382–389. [Google Scholar] [CrossRef]
- Pang, Y.; Fang, H.; Li, L.; Chen, M.; Chen, Y.; Chen, M. Predictive factors of anxiety and depression among nurses fighting coronavirus disease 2019 in China. Int. J. Ment. Health Nurs. 2021, 30, 524–532. [Google Scholar] [CrossRef]
- Pouralizadeh, M.; Bostani, Z.; Maroufizadeh, S.; Ghanbari, A.; Khoshbakht, M.; Alavi, S.A.; Ashrafi, S. Anxiety and depression and the related factors in nurses of Guilan University of Medical Sciences hospitals during COVID-19: A web-based cross-sectional study. Int. J. Afr. Nurs. Sci. 2020, 13, 100233. [Google Scholar] [CrossRef] [PubMed]
- Tu, Z.H.; He, J.W.; Zhou, N. Sleep quality and mood symptoms in conscripted frontline nurse in Wuhan, China during COVID-19 outbreak: A cross-sectional study. Medicine 2020, 99, e20769. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.Q.; Fang, Y.Y.; Huang, H.L.; Lv, W.J.; Wang, X.X.; Yang, T.T.; Yuan, J.M.; Gao, Y.; Qian, R.L.; Zhang, Y.H. Anxiety, depression and cognitive emotion regulation strategies in Chinese nurses during the COVID-19 outbreak. J. Nurs. Manag. 2021, 29, 1263–1274. [Google Scholar] [CrossRef] [PubMed]
- Yurtseven, Ş.; Arslan, S. Anxiety levels of university hospital nurses during the COVID-19 pandemic. Perspect. Psychiatr. Care 2021, 57, 1558–1565. [Google Scholar] [CrossRef] [PubMed]
- Roberts, N.J.; McAloney-Kocaman, K.; Lippiett, K.; Ray, E.; Welch, L.; Kelly, C. Levels of resilience, anxiety and depression in nurses working in respiratory clinical areas during the COVID pandemic. Respir. Med. 2021, 176, 106219. [Google Scholar] [CrossRef] [PubMed]
- Mekonen, E.; Shetie, B.; Muluneh, N. The Psychological impact of COVID-19 outbreak on nurses working in the Northwest of Amhara Regional State Referral Hospitals, Northwest Ethiopia. Psychol. Res. Behav. Manag. 2021, 13, 1353–1364. [Google Scholar] [CrossRef]
- Hong, S.; Ai, M.; Xu, X.; Wang, W.; Chen, J.; Zhang, Q.; Wang, L.; Kuang, L. Immediate psychological impact on nurses working at 42 government-designated hospitals during COVID-19 outbreak in China: A cross-sectional study. Nurs. Outlook 2021, 69, 6–12. [Google Scholar] [CrossRef]
- Li, R.; Chen, Y.; Lv, J.; Liu, L.; Zong, S.; Li, H.; Li, H. Anxiety and related factors in frontline clinical nurses fighting COVID-19 in Wuhan. Medicine 2020, 99, e21413. [Google Scholar] [CrossRef]
- Xiong, H.; Yi, S.; Lin, Y. The psychological status and self-efficacy of nurses during COVID-19 outbreak: A cross-sectional survey. Inquiry 2020, 57, 46958020957114. [Google Scholar] [CrossRef]
- Zheng, R.; Zhou, Y.; Fu, Y.; Xiang, Q.; Cheng, F.; Chen, H.; Xu, H.; Fu, L.; Wu, X.; Feng, M.; et al. Prevalence and associated factors of depression and anxiety among nurses during the outbreak of COVID-19 in China: A cross-sectional study. Int. J. Nurs. Stud. 2021, 114, 103809. [Google Scholar] [CrossRef]
- Dal’Bosco, E.B.; Floriano, L.S.M.; Skupien, S.V.; Arcaro, G.; Martins, A.R.; Anselmo, A.C.C. Mental health of nursing in coping with COVID-19 at a regional university hospital. Rev. Bras. Enferm. 2020, 73 (Suppl. 2), e20200434. [Google Scholar] [CrossRef]
- Almazan, J.U.; Albougami, A.S.; Alamri, M.S. Exploring nurses’ work-related stress in an acute care hospital in KSA. J. Taibah Univ. Med. Sci. 2019, 14, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Maharaj, S.; Lees, T.; Lal, S. Prevalence and risk factors of depression, anxiety, and stress in a cohort of Australian nurses. Int. J. Environ. Res. Public Health 2018, 16, 61. [Google Scholar] [CrossRef] [Green Version]
- Tuckett, A.; Winters-Chang, P.; Bogossian, F.; Wood, M. ‘Why nurses are leaving the profession … lack of support from managers’: What nurses from an e-cohort study said. Int. J. Nurs. Pract. 2015, 21, 359–366. [Google Scholar] [CrossRef]
- Saragih, I.D.; Tonapa, S.I.; Saragih, I.S.; Advani, S.; Batubara, S.O.; Suarilah, I.; Lin, C.J. Global prevalence of mental health problems among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2021, 121, 104002. [Google Scholar] [CrossRef]
- Hao, Q.; Wang, D.; Xie, M.; Tang, Y.; Dou, Y.; Zhu, L.; Wu, Y.; Dai, M.; Wu, H.; Wang, Q. Prevalence and risk factors of mental health problems among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Front. Psychiatry 2021, 12, 567381. [Google Scholar] [CrossRef]
- Liu, X.; Zhu, M.; Zhang, R.; Zhang, J.; Zhang, C.; Liu, P.; Feng, Z.; Chen, Z. Public mental health problems during COVID-19 pandemic: A large-scale meta-analysis of the evidence. Transl. Psychiatry 2021, 11, 384. [Google Scholar] [CrossRef] [PubMed]
- Fereidouni, Z.; Dehghan, A.; Najafi Kalyani, M. The prevalence of depression among nurses in Iran: A systematic review and meta-analysis. Int. J. Med. Rev. 2018, 5, 163–167. [Google Scholar] [CrossRef]
- Lasalvia, A.; Bodini, L.; Amaddeo, F.; Porru, S.; Carta, A.; Poli, R.; Bonetto, C. The sustained psychological impact of the COVID-19 pandemic on health care workers one year after the outbreak—A repeated cross-sectional survey in a Tertiary Hospital of North-East Italy. Int. J. Environ. Res. Public Health 2021, 18, 13374. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | First Author (Year)/Country | Study Design | Study Size | Participants | Age, Years (Mean ± SD or n (%)) | Female n (%) | Married n (%) | Position | Start Date | End Date | Depression Assessment Tool | n (%) with Depression | Anxiety Assessment Tool | n (%) with Anxiety | Survey Method | Quality Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Abu-Snieneh (2021)/Saudi Arabia [25] | cross-sectional study | 1265 | nurses from all regions of Saudi Arabia | 28.83 ± 5.29 | 1101 (87) | 783 (61.9) | Mixed | April 2020 | June 2020 | PHQ-9 | 329 (25.9) | GAD-7 | 234 (18.5) | Online survey | 5 |
| 2. | An et al. (2020)/China [26] | cross-sectional study | 1103 | Emergency Department nurses from all regions of China | 32.20 ± 7.61 | 1001 (90.8) | 710 (64.4) | Frontline | 15 March 2020 | 20 March 2020 | PHQ-9 | 176 (16) | N/A | N/A | Online survey | 4 |
| 3. | Cai et al. (2020)/China [23] | longitudinal study | 709 | nurses from Renmin Hospital of Wuhan University (outbreak period of the pandemic) | ≥ 30 287 (40.4) | 684 (96.5) | 376 (53) | Mixed | 29 January 2020 | 2 February 2020 | PHQ-9 | 109 (15.4) | GAD-7 | 84 (11.8) | Online survey | 7 |
| 4. | Han et al. (2020)/China [27] | cross-sectional survey | 21,119 | nurses from 14 prefecture and city hospitals in Gansu Province, located in northwest China | 31.89 ± 7.08 | 20909 (98.6) | 15499 (73.1) | Mixed | 7 February 2020 | 10 February 2020 | SDS | 1738 (8.2) | SAS | 996 (4.7) | Online survey | 5 |
| 5. | Hong et al. (2021)/China [39] | cross-sectional study | 4692 | nurses from the Chongqing region | ≥ 31 2043 (43.6) | 4548 (96.9) | 3013 (64.2) | Frontline | 8 February 2020 | 14 February 2020 | PHQ-9 | 442 (9.4) | GAD-7 | 379 (8.1) | Online survey | 4 |
| 6. | Hu et al. (2020)/China [28] | cross-sectional study | 2014 | nurses from two hospitals in Wuhan | 30.99 ± 6.17 | 1754 (87.1) | 1230 (61.1) | Frontline | 13 February 2020 | 24 February 2020 | SDS | 217 (10.7) | SAS | 288 (14.3) | Online survey | 5 |
| 7. | Jiang et al. (2020)/China [29] | cross-sectional study | 1569 | nurses from the Linxia Hui Autonomous Prefecture | 30.93 ± 6.48 | 1550 (98.8) | 1170 (74.6) | Mixed | 6 February, 2020 | 10 February 2020 | SDS | 127 (8.1) | SAS | 68 (4.3) | Online survey | 3 |
| 8. | Labrague et al. (2021)/Philippines [31] | cross-sectional study | 736 | nurses from frontline hospital and public health nurses in Western Samar | 31.9 ± 7.35 | 574 (78.1) | 312 (42.45) | Frontline | 1 September 2020 | 1 October 2020 | N/A | N/A | CAS | 130 (37.4) | Online survey | 3 |
| 9. | Labrague et al. (2020)/Philippines [30] | cross-sectional study | 325 | nurses from frontline hospital in Region 8, Philippines | 30.94 ± 6.67 | 243 (74.8) | 108 (33.2) | Frontline | 25 April 2020 | 25 May 2020 | N/A | N/A | CAS | 123 (37.8) | PAPI | 4 |
| 10. | Li et al. (2020)/China [12] | cross-sectional study | 176 | nurses from tertiary hospitals in Wuhan city, Hubei province that were designated to receive new patients with COVID-19 | ≥30 72 (40.8) | 136 (77.3) | 88 (50) | Frontline | Unknown | Unknown | N/A | N/A | HAMA | 136 (77.3) | Online survey | 3 |
| 11. | Pang et al. (2021)/China [32] | cross-sectional study | 282 | nurses from three hospitals that received patients with COVID-19 in both Guangdong and Hubei Provinces | 31.61 ± 7.60 | 250 (88.65) | 169 (59.93) | Frontline | 10 March 2020 | 20 March 2020 | PHQ-9 | 160 (56.74) | GAD-7 | 134 (47.52) | Online survey | 4 |
| 12. | Pouralizadeh et al. (2020)/Iran [33] | cross-sectional study | 441 | Nurses working in the province of Guilan at the University of Medical Sciences hospital | 36.34 ± 8.74 | 420 (95.2) | 335 (76) | Mixed | 7 April 2020 | 12 April 2020 | PHQ-9 | 165 (37.5) | GAD-7 | 171 (38.7) | Online survey | 3 |
| 13. | Tu et al. (2020)/China [34] | cross-sectional study | 100 | nurses from Wuhan in “Huoshenshan” hospital | 34.44 ± 5.85 | 100 (100) | 70 (70) | Frontline | 7 February 2020 | 24 February 2020 | PHQ-9 | 10 (10) | GAD-7 | 2 (2) | Online survey | 4 |
| 14. | Wang et al. (2021)/China [35] | cross-sectional study | 586 | nurses working in Nanjing in the province of Jiangsu | 31.07 ± 7.54 | 563 (96.08) | 353 (60.24) | Unknown | 14 February 2020 | 3 March 2020 | PHQ-9 | 64 (11.09) | GAD-7 | 40 (6.83) | Online survey | 6 |
| 15. | Xiong et al. (2020)/China [41] | cross-sectional study | 223 | nurses from one of the public tertiary hospitals in Xiamen, Fujian Province | ≥36 77 (34.5) | 217 (97.3) | Unknown | Frontline | 16 February 2020 | 25 February 2020 | PHQ-9 | 15 (6.7) | GAD-7 | 27 (12.1) | Online survey | 5 |
| 16. | Yurtseven et al. (2021)/Turkey [36] | cross-sectional study | 270 | Nurses working in a university hospital operating as a pandemic hospital | 36.83 ± 9.23 | 237 (87.77) | 193 (71.48) | Frontline | Unknown | Unknown | N/A | N/A | SAI | 249 (92.4) | Online survey | 3 |
| 17. | Zheng et al. (2021)/China [42] | cross-sectional study | 3 228 | nurses from Sichuan Province and Wuhan City | ≥30 1706 (52.9) | 3121 (96.7) | Unknown | Mixed | 27 January 2020 | 3 February 2020 | SDS other cutoff points | N/A | SAS | 122 (3.8) | Online survey | 4 |
| 18. | Roberts et al. (2021)/United Kingdom [37] | cross-sectional study | 255 | nurses working in respiratory clinical areas | 45.1 ± 9.77 | 226 (88.6) | Unknown | Mixed | 1 May 2020 | 1 June 2020 | PHQ-9 | 31 (17.2) | GAD-7 | 40 (20.9) | Online survey | 3 |
| 19. | Dal’Bosco et al. (2020)/Brazil [43] | cross-sectional study | 88 | nurses working at a regional university hospital of reference for coping with COVID-19 in Paraná | ≥ 31 51 (58) | 79 (89.8) | 32 (36.4) | Frontline | March 2020 | April 2020 | HAD-D | 22 (25) | HAD-A | 43 (48.9) | Online survey | 5 |
| 20. | Arnetz et al. (2020)/USA [9] | cross-sectional study | 695 | nurses working in the state of Michigan | ≥45 376 (54.7) | 644 (93.6) | Unknown | Mixed | 7 May 2020 | 29 May 2020 | PHQ-9 | 167 (26.1) | GAD-7 | 144 (22.6) | Online survey | 3 |
| 21. | Havaei et al. (2021)/Canada [24] | cross-sectional study | 3 676 | members of the provincial nurses’ union | Unknown | Unknown | Unknown | Mixed | January 2020 | July 2020 | PHQ-9 | 1391 (41.4) | GAD-7 | 1273 (37.6) | Online survey | 3 |
| 22. | Kim et al. (2021)/USA [6] | cross-sectional study | 320 | nurses who graduated from the nursing school at a private, 4-year liberal arts university in Southern California | 33 (min-max: 21–67) BRAK SD | 302 (94.4) | Unknown | Mixed | 20 April 2020 | 10 May 2020 | PHQ-9 | 83 (26) | GAD-7 | 138 (43) | Online survey | 5 |
| 23. | Mekonen et al. (2021)/China [38] | cross-sectional study | 293 | nurses working in the northwest of Amhara Regional | 29.6 ± 5.1 | 133 (45.4) | 156 (53.2) | Mixed | 25 September 2020 | 20 October 2020 | DASS-21 Depression | 162 (55.3) | DASS-21 Anxiety | 204 (69.6) | PAPI | 6 |
| Instrument | Name Abbreviation | Characteristic Being Assessed | Administration Method | Number of Items, (Sub)Scale(s) (Number of Items) | Response Options, Range of Score | The Cut-Off Point Adopted in the Meta-Analysis |
|---|---|---|---|---|---|---|
| Patient Health Questionnaire | PHQ-9 | Depression | Self-reported | 9 items | Dichotomous scoring system and 4-points Likert scale 0–27
| ≥10 points |
| Self-Rating Depression Scale | SDS | Depression | Self-reported | 20 items | Dichotomous scoring system and 4-points Likert scale 25–100
| ≥63 points |
| Depression Anxiety Stress Scales | DASS-21 | Depression/Anxiety | Self-reported | 21 items, on 7 items for each subscale:
| Dichotomous scoring system and 4-points Likert scale 0–21 for each subscale | Depression ≥ 10 points Anxiety ≥ 8 points |
| Hospital Anxiety and Depression Scale | HAD | Depression/Anxiety | Self-reported | 14 items, on 7 items for each subscale:
| Dichotomous scoring system 0–21 for each subscale | ≥8 points for each subscale: |
| Generalized Anxiety Disorder | GAD-7 | Anxiety | Self-reported | 7 items | Dichotomous scoring system and 4-points Likert scale 0–21
| ≥10 points |
| Self-Rating Anxiety Scale | SAS | Anxiety | Self-reported | 20 items | Dichotomous scoring system and 4-points Likert scale 25–100
| ≥60 points |
| Coronavirus Anxiety Scale | CAS | Anxiety | Self-reported | 5 items | Dichotomous scoring system and 5-points Likert scale 5–25 | ≥9 points |
| The Hamilton rating scale for anxiety | HAMA | Anxiety | Self-reported | 14 items | Dichotomous scoring system 0–56 | ≥7 points |
| State Anxiety Inventory | SAI | Anxiety | Self-reported | 20 items | Dichotomous scoring system and 4-points Likert scale 20–80
| ≥37 points |
| Variable | Depression | Anxiety | ||||
|---|---|---|---|---|---|---|
| Proportion | 95% CI | p | Proportion | 95%CI | p | |
| Place of research: | ||||||
| All instruments | ||||||
| Asia | 0.18 | (0.09–0.26) | 0.063 | 0.25 | (0.11–0.38) | 0.196 |
| Other continents | 0.31 | (0.20–0.43) | 0.40 | (0.20–0.61) | ||
| Only PHQ-9 | Only GAD-7 | |||||
| Asia | 0.21 | (0.10–0.31) | 0.44 | 0.18 | (0.07–0.29) | 0.15 |
| Other continents | 0.28 | (0.13–0.42) | 0.31 | (0.17–0.45) | ||
| Position: | ||||||
| All instruments | ||||||
| Frontline | 0.19 | (0.07–0.31) | 0.45 | 0.31 | (0.15–0.46) | 0.43 |
| Mixed | 0.25 | (0.15–0.35) | 0.23 | (0.11–0.35) | ||
| Only PHQ-9 | Only GAD-7 | |||||
| Frontline | 0.20 | (0.06–0.33) | 0.54 | 0.17 | (0.02–0.32) | 0.40 |
| Mixed | 0.25 | (0.18–0.33) | 0.26 | (0.16–0.35) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ślusarska, B.; Nowicki, G.J.; Niedorys-Karczmarczyk, B.; Chrzan-Rodak, A. Prevalence of Depression and Anxiety in Nurses during the First Eleven Months of the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 1154. https://doi.org/10.3390/ijerph19031154
Ślusarska B, Nowicki GJ, Niedorys-Karczmarczyk B, Chrzan-Rodak A. Prevalence of Depression and Anxiety in Nurses during the First Eleven Months of the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(3):1154. https://doi.org/10.3390/ijerph19031154
Chicago/Turabian StyleŚlusarska, Barbara, Grzegorz Józef Nowicki, Barbara Niedorys-Karczmarczyk, and Agnieszka Chrzan-Rodak. 2022. "Prevalence of Depression and Anxiety in Nurses during the First Eleven Months of the COVID-19 Pandemic: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 3: 1154. https://doi.org/10.3390/ijerph19031154