
Cross-Country Differences in Stay-at-Home Behaviors during Peaks in the COVID-19 Pandemic in China and the United States: The Roles of Health Beliefs and Behavioral Intention



Abstract
:1. Introduction
1.1. Stay-at-Home Behaviors in China and the United States
1.2. The Mediating Role of Health Beliefs
1.3. The Mediating Role of Behavioral Intention
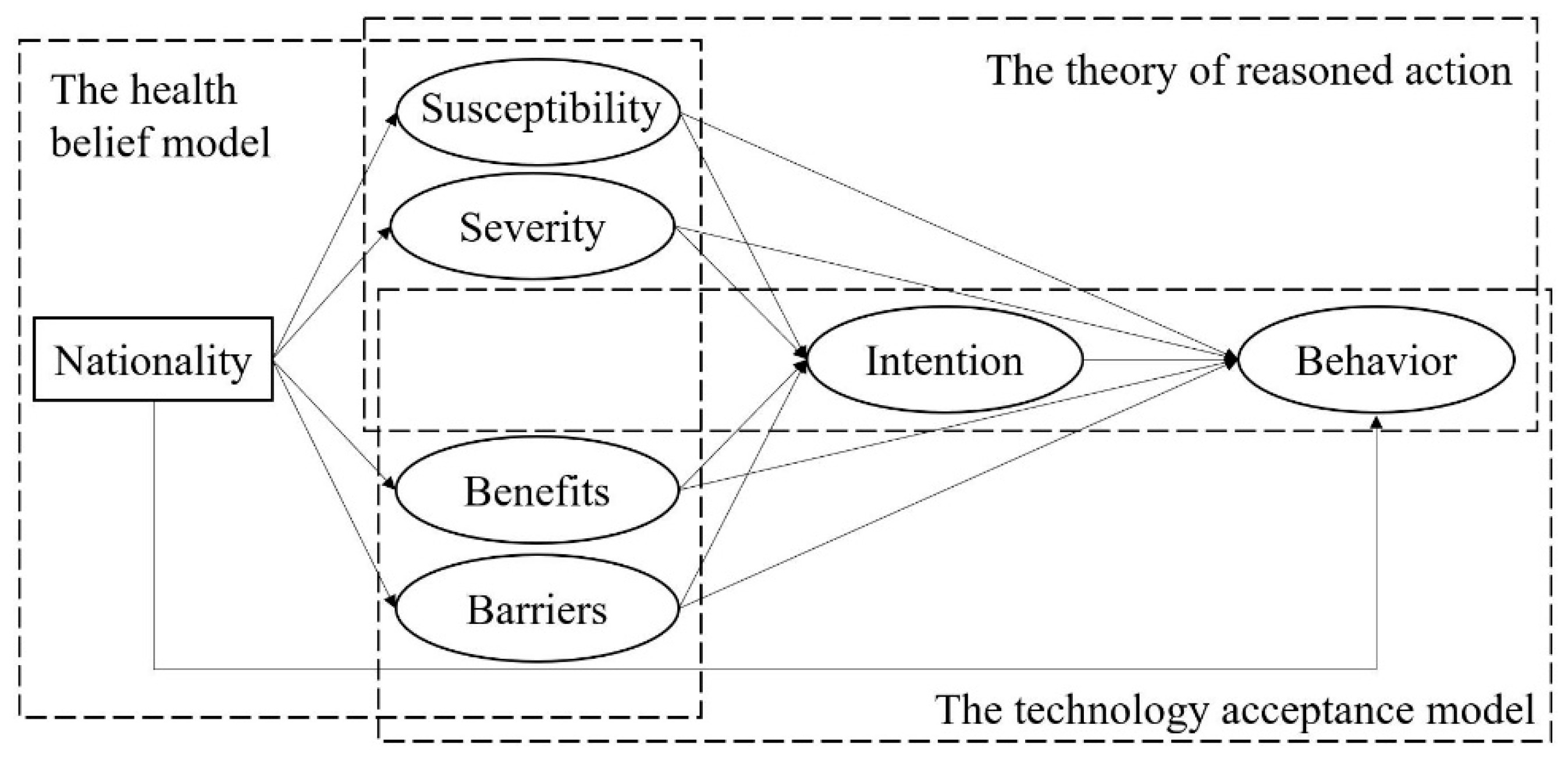
1.4. The Mediation Model
2. Methods
2.1. Participants and Procedures
2.2. Measures
2.2.1. Perceived Susceptibility
2.2.2. Perceived Severity
2.2.3. Perceived Benefits
2.2.4. Perceived Barriers
2.2.5. Behavioral Intention
2.2.6. Actual Behaviors
2.3. Data Analyses
3. Results
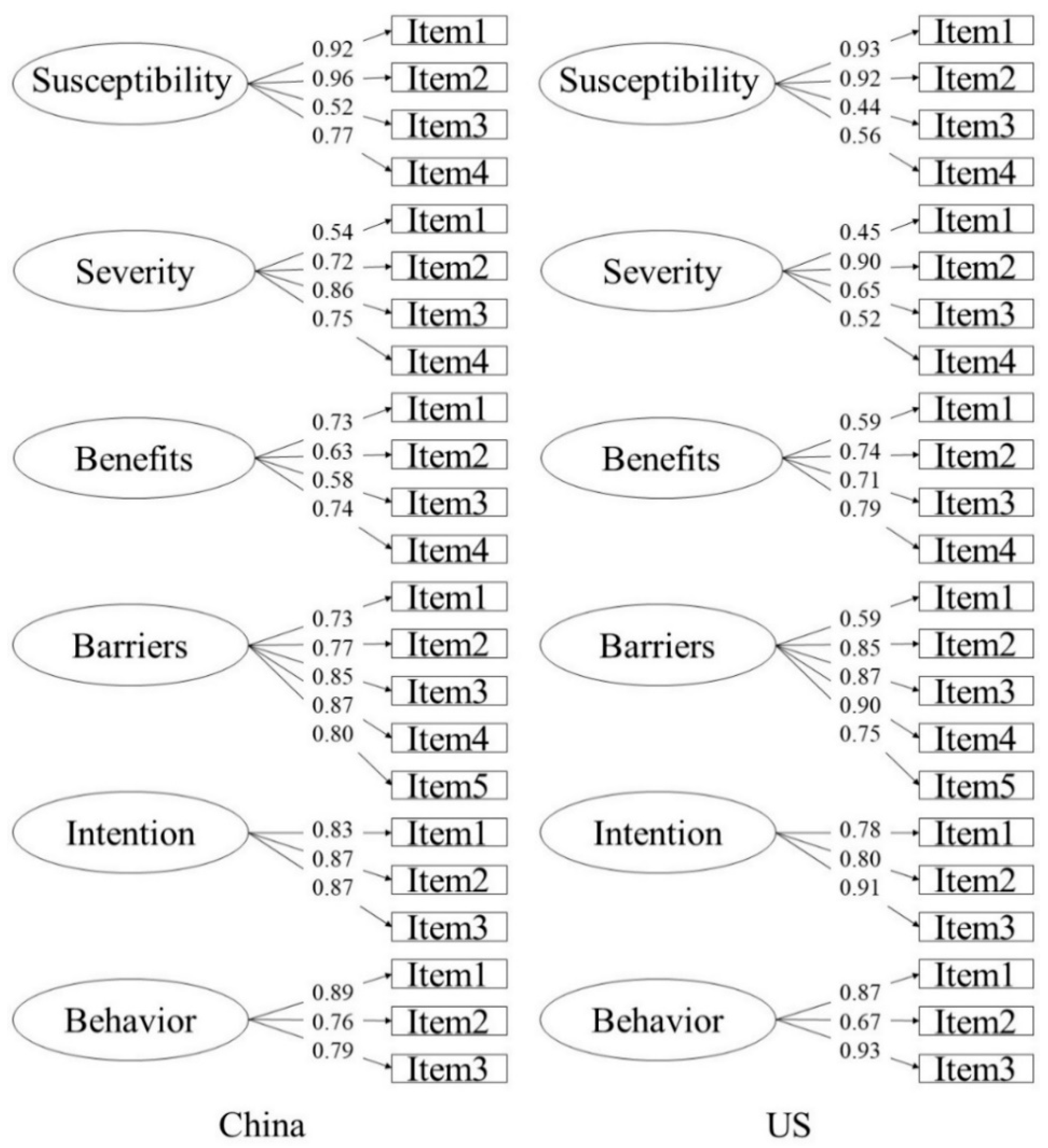
3.1. The Measurement Model
3.2. Descriptive Statistics and Correlations
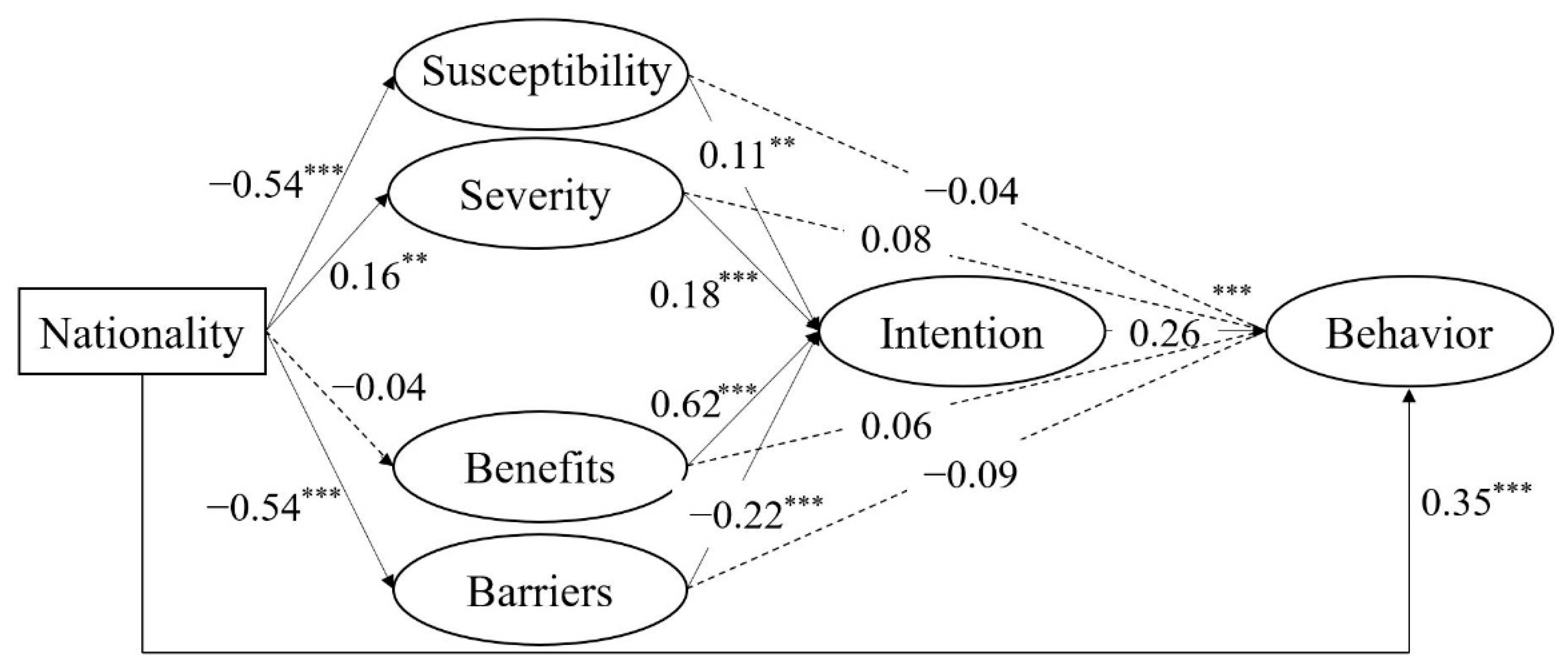
3.3. The Structural Model
4. Discussion
4.1. The Mediating Roles of Perceived Susceptibility and Behavioral Intention
4.2. The Mediating Roles of Perceived Severity and Behavioral Intention
4.3. The Mediating Roles of Perceived Benefits and Behavioral Intention
4.4. The Mediating Roles of Perceived Barriers and Behavioral Intention
4.5. Limitations and Future Directions
4.6. Theoretical and Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Transmission of SARS-COV-2: Implications for Infection Prevention Precautions. Available online: https://www.who.int/news-room/commentaries/detail/transmission-of-sars-cov-2-implications-for-infection-prevention-precautions (accessed on 9 July 2020).
- van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support covid-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schunemann, H.J.; Covid-19 Systematic Urgent Review Group Effort Study Authors. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-COV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Nussbaumer-Streit, B.; Mayr, V.; Dobrescu, A.I.; Chapman, A.; Persad, E.; Klerings, I.; Wagner, G.; Siebert, U.; Christof, C.; Zachariah, C.; et al. Quarantine alone or in combination with other public health measures to control COVID-19: A rapid review. Cochrane Database Syst. Rev. 2020, 4, CD013574. [Google Scholar]
- Lunn, P.D.; Timmons, S.; Julienne, H.; Belton, C.A.; Barjaková, M.; Lavin, C.; McGowan, F.P. Using decision aids to support self-isolation during the COVID-19 pandemic. Psychol. Health 2020, 36, 195–213. [Google Scholar] [CrossRef]
- Xinhua. Fighting COVID-19: China in Action. Available online: http://www.xinhuanet.com/english/2020-06/07/c_139120424.htm (accessed on 7 June 2020).
- Lee, A. These States Have Implemented Stay-at-Home Orders. Here’s What That Means for You. Available online: https://edition.cnn.com/2020/03/23/us/coronavirus-which-states-stay-at-home-order-trnd/index.html (accessed on 7 April 2020).
- Champion, V.L.; Skinner, C.S. The health belief model. In Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Karen, G., Barbara, K.R., Viswanath, K., Eds.; Jossey-Bass: Hoboken, NJ, USA, 2008; pp. 45–64. [Google Scholar]
- Janz, N.K.; Becker, M.H. The health belief model: A decade later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Fishbein, M.; Ajzen, I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research; Addison-Wesley: Reading, MA, USA, 1975. [Google Scholar]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User acceptance of computer technology: A comparison of two theoretical models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.; Ng, A.-K. Psychosocial factors predicting sars-preventive behaviors in four major sars-affected regions. J. Appl. Soc. Psychol. 2006, 36, 222–247. [Google Scholar] [CrossRef]
- Hofstede, G.; Hofstede, G.J.; Minkov, M. Cultures and Organizations: Software of the Mind, 3rd ed.; McGraw-Hill: New York, NY, USA, 2010. [Google Scholar]
- Fincher, C.L.; Thornhill, R.; Murray, D.R.; Schaller, M. Pathogen prevalence predicts human cross-cultural variability in individualism/collectivism. Proc. Biol. Sci. 2008, 275, 1279–1285. [Google Scholar] [CrossRef] [Green Version]
- Huang, F.; Ding, H.; Liu, Z.; Wu, P.; Zhu, M.; Li, A.; Zhu, T. How fear and collectivism influence public’s preventive intention towards covid-19 infection: A study based on big data from the social media. BMC Public Health 2020, 20, 1707. [Google Scholar] [CrossRef]
- Murray, D.R.; Trudeau, R.; Schaller, M. On the origins of cultural differences in conformity: Four tests of the pathogen prevalence hypothesis. Personal. Soc. Psychol. Bull. 2011, 37, 318–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofstede, G.; McCrae, R.R. Personality and culture revisited: Linking traits and dimensions of culture. Cross-Cult. Res. 2004, 38, 52–88. [Google Scholar] [CrossRef]
- Alessandri, G.; Filosa, L.; Tisak, M.S.; Crocetti, E.; Crea, G.; Avanzi, L. Moral disengagement and generalized social trust as mediators and moderators of rule-respecting behaviors during the covid-19 outbreak. Front. Psychol. 2020, 11, 2102. [Google Scholar] [CrossRef]
- Sheeran, P.; Abraham, C. The health belief model. In Predicting Health Behavior; Conner, M., Norman, P., Eds.; Open University Press: Buckingham, UK, 1996; pp. 23–62. [Google Scholar]
- Livi, S.; Zeri, F.; Baroni, R. Health beliefs affect the correct replacement of daily disposable contact lenses: Predicting compliance with the health belief model and the theory of planned behaviour. Contact Lens Anterior Eye 2017, 40, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Germani, A.; Buratta, L.; Delvecchio, E.; Mazzeschi, C. Emerging adults and covid-19: The role of individualism-collectivism on perceived risks and psychological maladjustment. Int. J. Environ. Res. Public Health 2020, 17, 3497. [Google Scholar] [CrossRef]
- Yoshitake, N.; Omori, M.; Sugawara, M.; Akishinonomiya, K.; Shimada, S.; Iannello, P. Do health beliefs, personality traits, and interpersonal concerns predict TB prevention behavior among Japanese adults? PLoS ONE 2019, 14, e0211728. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Sherman, D.K.; Updegraff, J.A. Fear of ebola: The influence of collectivism on xenophobic threat responses. Psychol. Sci. 2016, 27, 935–944. [Google Scholar] [CrossRef]
- Nowak, B.; Brzoska, P.; Piotrowski, J.; Sedikides, C.; Zemojtel-Piotrowska, M.; Jonason, P.K. Adaptive and maladaptive behavior during the covid-19 pandemic: The roles of dark triad traits, collective narcissism, and health beliefs. Personal. Individ. Differ. 2020, 167, 110232. [Google Scholar] [CrossRef] [PubMed]
- Jose, R.; Narendran, M.; Bindu, A.; Beevi, N.; Manju, L.; Benny, P.V. Public perception and preparedness for the pandemic covid 19: A health belief model approach. Clin. Epidemiol. Glob. Health 2020, 9, 41–46. [Google Scholar] [CrossRef]
- Alsulaiman, S.; Rentner, T. The health belief model and preventive measures: A study of the ministry of health campaign on coronavirus in Saudi Arabia. J. Int. Crisis Risk Commun. Res. 2018, 1, 27–56. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Lu, Y.; Zhou, T.; Wang, B. Exploring Chinese users’ acceptance of instant messaging using the theory of planned behavior, the technology acceptance model, and the flow theory. Comput Hum. Behav 2009, 25, 29–39. [Google Scholar] [CrossRef]
- Sun, X.; Guo, Y.; Wang, S.; Sun, J. Predicting iron-fortified soy sauce consumption intention: Application of the theory of planned behavior and health belief model. J. Nutr. Educ. Behav. 2006, 38, 276–285. [Google Scholar] [CrossRef]
- Chen, X.; Chen, H. Differences in preventive behaviors of covid-19 between urban and rural residents: Lessons learned from a cross-sectional study in China. Int. J. Environ. Res. Public Health 2020, 17, 4437. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behavior. In Handbook of Theories of Social Psychology; Lange, P.A.M.V., Kruglanski, A.W., Higgins, E.T., Eds.; SAGE Publications: London, UK, 2012; Volume 1, pp. 438–460. [Google Scholar]
- Sheeran, P. Intention-behavior relations: A conceptual and empirical review. In European Review of Social Psychology; Stroebe, W., Hewstone, M., Eds.; Wiley: Chichester, UK, 2002; Volume 12, pp. 1–36. [Google Scholar]
- Webb, T.L.; Sheeran, P. Does changing behavioral intentions engender behavior change? A meta-analysis of the experimental evidence. Psychol. Bull. 2006, 132, 249–268. [Google Scholar] [CrossRef] [Green Version]
- Champion, V.L. Instrument development for health belief model constructs. Adv. Nurs. Sci. 1984, 6, 73–85. [Google Scholar] [CrossRef]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. Mis Q. 1989, 13, 319–340. [Google Scholar] [CrossRef] [Green Version]
- Moon, J.-W.; Kim, Y.-G. Extending the tam for a world-wide-web context. Inf. Manag. 2001, 38, 217–230. [Google Scholar] [CrossRef]
- Cheung, M.W.L. Comparison of approaches to constructing confidence intervals for mediating effects using structural equation models. Struct. Equ. Modeling A Multidiscip. J. 2007, 14, 227–246. [Google Scholar] [CrossRef]
- Wen, Z.L.; Hau, K.T.; Marsh, H.W. Structural equation model testing: Cutoff criteria for goodness of fit indices and chi-square test. Acta Psychol. Sin. 2004, 36, 186–194. (In Chinese) [Google Scholar]
- Liu, H. Advanced Statistics for Psychology; China Renmin University Press: Beijing, China, 2019. (In Chinese) [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Hui, C.H.; Triandis, H.C. Individualism-collectivism: A study of cross-cultural researchers. J. Cross-Cult. Psychol. 1986, 17, 225–248. [Google Scholar] [CrossRef]
- Li, J.B.; Yang, A.; Dou, K.; Wang, L.X.; Zhang, M.C.; Lin, X.Q. Chinese public’s knowledge, perceived severity, and perceived controllability of covid-19 and their associations with emotional and behavioural reactions, social participation, and precautionary behaviour: A national survey. BMC Public Health 2020, 20, 1589. [Google Scholar] [CrossRef] [PubMed]
- Mander, J. Coronavirus: How Consumers Are Actually Reacting. Available online: https://blog.globalwebindex.com/trends/coronavirus-and-consumers/ (accessed on 12 March 2020).
- Quest Mobile. A Special Report on “Overcoming COVID-19” of Chinese Mobile Internet in 2020. Available online: https://www.questmobile.com.cn/research/report-new/81 (accessed on 12 February 2020).
- Min, C.; Shen, F.; Yu, W.; Chu, Y. The relationship between government trust and preventive behaviors during the covid-19 pandemic in china: Exploring the roles of knowledge and negative emotion. Prev. Med. 2020, 141, 106288. [Google Scholar] [CrossRef] [PubMed]
- He, J.; van de Vijver, F. Bias and equivalence in cross-cultural research. Online Read. Psychol. Cult. 2012, 2. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| During Peaks in the COVID-19 Pandemic, | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Factor 6 |
|---|---|---|---|---|---|---|
| 1. My chances of getting COVID-19 are great. | 0.94 | |||||
| 2. There is a good possibility that I will get COVID-19. | 0.93 | |||||
| 3. I worry a lot about getting COVID-19. | 0.53 | |||||
| 4. I am more likely than the average person to get COVID-19. | 0.73 | |||||
| 5. COVID-19 is a hopeless disease. | 0.50 | |||||
| 6. Problems I would experience from COVID-19 would last a long time. | 0.72 | |||||
| 7. Getting COVID-19 would result in serious consequences. | 0.84 | |||||
| 8. If I got COVID-19, my life would change. | 0.76 | |||||
| 9. Staying at home prevents me from getting COVID-19. | 0.69 | |||||
| 10. If I do not stay at home, it is more likely that I will get COVID-19. | 0.60 | |||||
| 11. If I stay at home, I would become less anxious about getting COVID-19. | 0.64 | |||||
| 12. Staying at home can help me to stay in a healthy condition. | 0.71 | |||||
| 13. Staying at home causes me inconvenience. | 0.75 | |||||
| 14. Staying at home interferes with my activities. | 0.86 | |||||
| 15. If I stay at home, I will have to break my usual life habits. | 0.84 | |||||
| 16. If I stay at home, my daily schedule will be disrupted. | 0.83 | |||||
| 17. In order to stay at home, I have to give up quite a bit. | 0.82 | |||||
| 18. I will always stay at home except for essential activities. | 0.82 | |||||
| 19. I will recommend others to stay at home. | 0.78 | |||||
| 20. I will continue staying at home. | 0.88 | |||||
| 21. How many times did you go outside each week? | 0.90 | |||||
| 22. How many hours did you go outside each week? | 0.74 | |||||
| 23. How frequently did you go outside? | 0.85 | |||||
| Percentage of variance accounted for (%) | 8.96 | 8.11 | 16.19 | 21.44 | 2.85 | 5.74 |
| Cronbach α for subscale | 0.86 | 0.79 | 0.77 | 0.91 | 0.87 | 0.87 |
| Composite reliability (CR) | 0.87 | 0.80 | 0.77 | 0.91 | 0.88 | 0.87 |
| Average variance extracted (AVE) | 0.64 | 0.51 | 0.46 | 0.68 | 0.70 | 0.70 |
| Models | Interpretations | χ2 | df | CFI | TLI | RMSEA | SRMR | Δχ2 | Δdf |
|---|---|---|---|---|---|---|---|---|---|
| Model 1a | China | 683.50 | 215 | 0.93 | 0.91 | 0.07 | 0.06 | – | – |
| Model 1b | USA | 485.75 | 213 | 0.92 | 0.90 | 0.07 | 0.07 | – | – |
| Model 2: configural invariance | same indicators | 1066.79 | 428 | 0.93 | 0.92 | 0.06 | 0.07 | – | – |
| Model 3: metric invariance | same loadings | 1174.78 | 445 | 0.92 | 0.91 | 0.06 | 0.08 | 107.99 | 17 |
| Model 4: scalar invariance | same intercepts | 1363.08 | 458 | 0.91 | 0.90 | 0.07 | 0.08 | 188.30 | 13 |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1 gender | – | ||||||||
| 2 age | 0.30 *** | – | |||||||
| 3 nationality | −0.29 *** | −0.59 *** | – | ||||||
| 4 susceptibility | 0.18 *** | 0.33 *** | −0.51 *** | 0.80 | |||||
| 5 severity | −0.05 | −0.09 * | 0.17 *** | 0.13 *** | 0.72 | ||||
| 6 benefits | 0.07 * | 0.11 ** | −0.09 ** | −0.03 | 0.15 *** | 0.68 | |||
| 7 barriers | 0.07 * | 0.25 *** | −0.45 *** | 0.29 *** | 0.04 | −0.02 | 0.82 | ||
| 8 intention | 0.09 * | 0.05 | 0.04 | 0.04 | 0.22 *** | 0.52 *** | −0.17 *** | 0.84 | |
| 9 behavior | −0.11 ** | −0.25 *** | 0.40 *** | −0.20 *** | 0.19 *** | 0.18 *** | −0.28 *** | 0.32 *** | 0.83 |
| M | – | 20.83 | – | 2.31 | 3.25 | 3.97 | 3.24 | 4.00 | 5.45 |
| SD | – | 2.89 | – | 0.91 | 0.83 | 0.71 | 1.03 | 0.80 | 1.15 |
| Paths | Standardized (β) | 95% CI | Significance | |
|---|---|---|---|---|
| Low | High | |||
| Nationality → Behavior | 0.347 | 0.237 | 0.456 | √ |
| Nationality → Susceptibility → Behavior | 0.020 | −0.029 | 0.068 | × |
| Nationality → Severity → Behavior | 0.012 | −0.004 | 0.028 | × |
| Nationality → Benefits → Behavior | −0.002 | −0.013 | 0.008 | × |
| Nationality → Barriers → Behavior | 0.047 | −0.005 | 0.099 | × |
| Nationality → Susceptibility → Intention → Behavior | −0.015 | −0.030 | −0.001 | √ |
| Nationality → Severity → Intention → Behavior | 0.007 | 0.001 | 0.014 | √ |
| Nationality → Benefits → Intention → Behavior | −0.006 | −0.023 | 0.011 | × |
| Nationality → Barriers → Intention → Behavior | 0.032 | 0.012 | 0.052 | √ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, W.; Liu, R.-D.; Ding, Y.; Hwang, J.; Wang, J.; Yang, Y. Cross-Country Differences in Stay-at-Home Behaviors during Peaks in the COVID-19 Pandemic in China and the United States: The Roles of Health Beliefs and Behavioral Intention. Int. J. Environ. Res. Public Health 2021, 18, 2104. https://doi.org/10.3390/ijerph18042104
Hong W, Liu R-D, Ding Y, Hwang J, Wang J, Yang Y. Cross-Country Differences in Stay-at-Home Behaviors during Peaks in the COVID-19 Pandemic in China and the United States: The Roles of Health Beliefs and Behavioral Intention. International Journal of Environmental Research and Public Health. 2021; 18(4):2104. https://doi.org/10.3390/ijerph18042104
Chicago/Turabian StyleHong, Wei, Ru-De Liu, Yi Ding, Jacqueline Hwang, Jia Wang, and Yi Yang. 2021. "Cross-Country Differences in Stay-at-Home Behaviors during Peaks in the COVID-19 Pandemic in China and the United States: The Roles of Health Beliefs and Behavioral Intention" International Journal of Environmental Research and Public Health 18, no. 4: 2104. https://doi.org/10.3390/ijerph18042104