Survival Analysis of Symptomatic COVID-19 in Phuentsholing Municipality, Bhutan


Abstract
:1. Background
2. Methods
Study Setting
3. Study Design and Study Population
4. Data Source
5. Statistical Analysis
- Mild disease: those with at least one symptom of COVID-19 (fever, fast breathing, cough, and chest x-ray (CXR) change, such as consolidation) but no signs of pneumonia;
- Severe disease: in addition to all or some COVID-19 symptoms, this group of patients had pneumonia (evidenced by CXR changes), needing antibiotics and oxygen therapy;
- Life-threatening: patients who had severe pneumonia and were haemodynamically unstable, needing intensive care unit admission.
6. Results
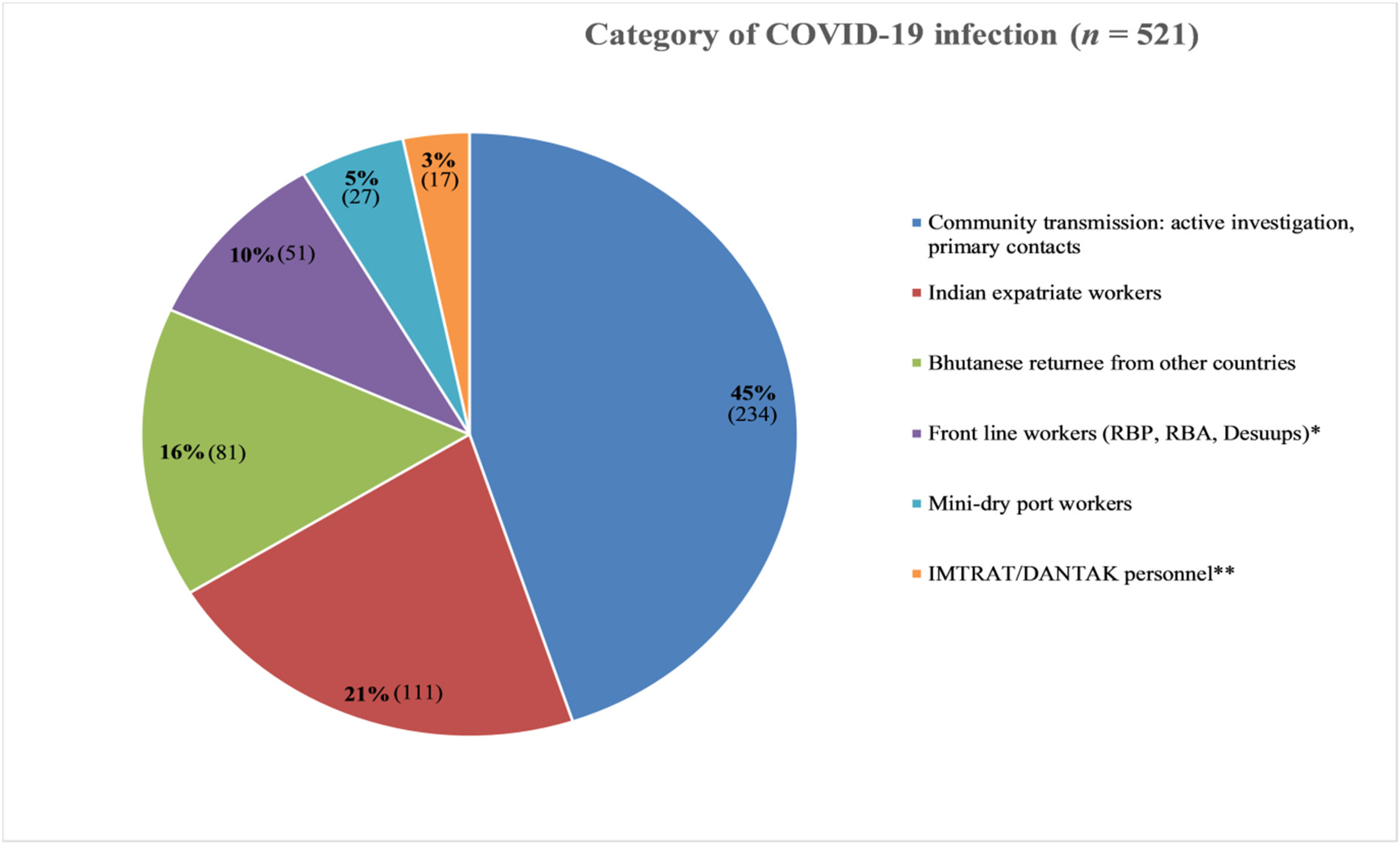
Descriptive Analysis
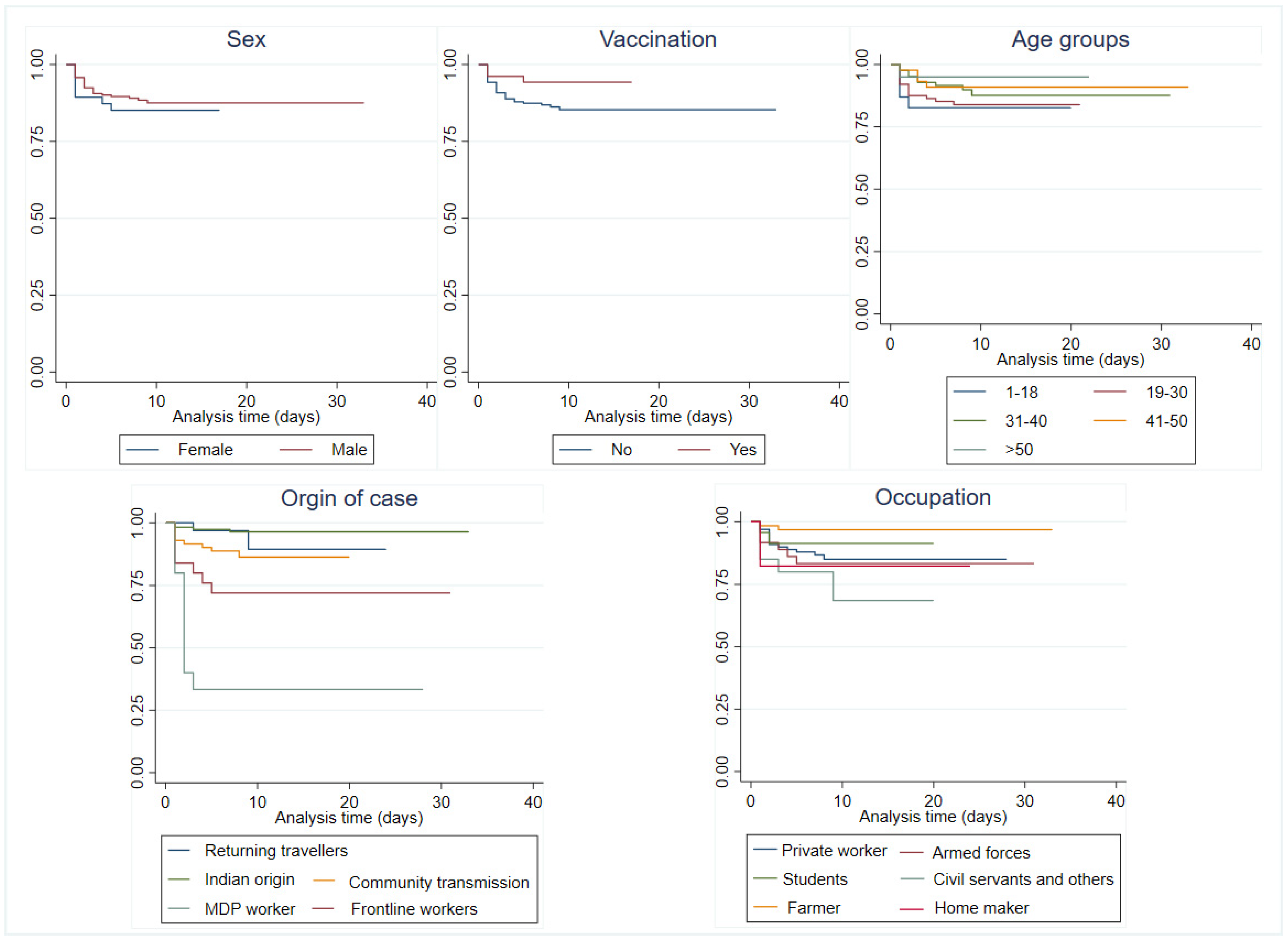
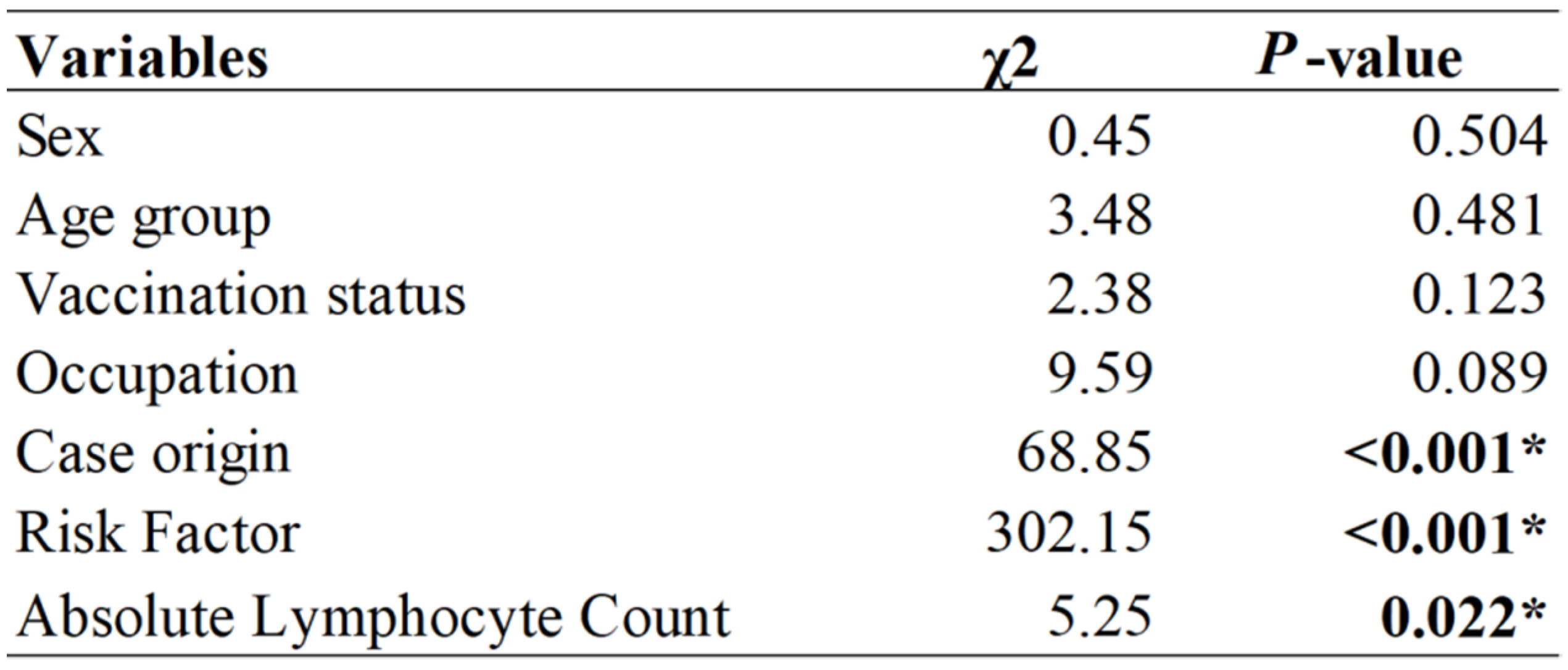
7. Survival Analysis
8. Discussion
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Consent for Publication
References
- Shereen, M.A.; Khan, S.; Kazmi, A.; Bashir, N.; Siddique, R. COVID-19 infection: Origin, transmission, and characteristics of human coronaviruses. J. Adv. Res. 2020, 24, 91–98. [Google Scholar] [CrossRef]
- John Hopkins University. Corona Virus Resource Center. 2021. Available online: https://coronavirus.jhu.edu/map.html (accessed on 19 September 2021).
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Pal, M.; Berhanu, G.; Desalegn, C.; Kandi, V. Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2): An Update. Cureus 2020. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Impact of COVID-19 on People’s Livelihoods, Their Health and Our Food Systems. Available online: https://www.who.int/news/item/13-10-2020-impact-of-covid-19-on-people’s-livelihoods-their-health-and-our-food-systems (accessed on 1 June 2021).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Chen, Z.; Nie, Y.; Ma, Y.; Guo, Q.; Dai, X. Identification of Symptoms Prognostic of COVID-19 Severity: Multivariate Data Analysis of a Case Series in Henan Province. J. Med. Internet Res. 2020, 22, e19636. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Mcfarlane, M.; Goubran, R.; Knoefel, F. Novel Coronavirus Cough Database: NoCoCoDa. IEEE Access 2020, 8, 154087–154094. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, X.; Jia, X.; Li, J.; Hu, K.; Chen, G.; Wei, J.; Gong, Z.; Zhou, C.; Yu, H.; et al. Risk factors for disease severity, unimprovement, and mortality in COVID-19 patients in Wuhan, China. Clin. Microbiol. Infect. 2020, 26, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Lai, A.L.; Millet, J.K.; Daniel, S.; Freed, J.H.; Whittaker, G.R. Towards Controlling the Pandemic. Lancet 2020, 395, 1315. [Google Scholar]
- UNICEF Bhutan. Vaccinating Bhutan against COVID-19. 2021. Available online: https://www.unicef.org/bhutan/ (accessed on 5 July 2021).
- Dorji, T.; Tamang, S.T. Bhutan’s experience with COVID-19 vaccination in 2021. BMJ Glob. Health 2021, 6, e005977. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Bian, L.; Gao, Q.; Gao, F.; Wang, Q.; He, Q.; Wu, X.; Mao, Q.; Xu, M.; Liang, Z. Impact of the Delta variant on vaccine efficacy and response strategies. Expert Rev. Vaccines 2021. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of Covid-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Royal Government of Bhutan. COVID-19 IN BHUTAN. Available online: https://www.gov.bt/covid19/ (accessed on 6 September 2021).
- Kuensel Newspaper. Local transmission in Phuentsholing confirmed. Kuensel Newspaper, 19 April 2021. [Google Scholar]
- South Asia Monitor. 21 new cases in Thimphu, local transmission feared in Bhutan. South Asia Monitor, 9 May 2020. [Google Scholar]
- The Straits Times. Bhutan lifts tobacco ban to temper demand for smuggled cigarettes during Covid-19 pandemic. The Straits Times, 31 August 2021. [Google Scholar]
- National Statistic Bureau. Population and Housing Census of Bhutan, National Report; NSB, Royal Government of Bhutan: Thimphu, Bhutan, 2017.
- Tsheten, T.; Mclure, A.; Clements, A.C.A.; Gray, D.J.; Wangdi, T.; Wangchuk, S.; Wangdi, K. Epidemiological Analysis of the 2019 Dengue Epidemic in Bhutan. Int. J. Environ. Res. Public Health 2021, 18, 354. [Google Scholar] [CrossRef] [PubMed]
- Tapnikar, L.A.; Patil, S.; Nyse, J. Interpreting Kaplan Meier’s survival curve in COVID-19 patients: A systematic review. Int. J. Community Med. Public Health 2020, 8, 424. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Koh, D. Occupational risks for COVID-19 infection. Occup. Med. 2020, 70, 3–5. [Google Scholar] [CrossRef] [Green Version]
- Carlsten, C.; Gulati, M.; Hines, S.; Rose, C.; Scott, K.; Tarlo, S.M.; Torén, K.; Sood, A.; Hoz, R.E. COVID-19 as an occupational disease. Am. J. Ind. Med. 2021, 64, 227–237. [Google Scholar] [CrossRef]
- Bialek, S.; Boundy, E.; Bowen, V.; Chow, N.; Cohn, A.; Dowling, N.; Ellington, S.; Gierke, R.; Hall, A.; MacNeil, J.; et al. Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19)—United States, February 12–March 16 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 343–346. [Google Scholar]
- Lescure, F.-X.; Bouadma, L.; Nguyen, D.; Parisey, M.; Wicky, P.-H.; Behillil, S.; Gaymard, A.; Bouscambert-Duchamp, M.; Donati, F.; Le Hingrat, Q.; et al. Clinical and virological data of the first cases of COVID-19 in Europe: A case series. Lancet Infect. Dis. 2020, 20, 697–706. [Google Scholar] [CrossRef] [Green Version]
- Wise, J. A third of covid-19 patients admitted to UK hospitals die. BMJ 2020, 369, m1794. [Google Scholar] [CrossRef]
- Tian, S.; Hu, N.; Lou, J.; Chen, K.; Kang, X.; Xiang, Z.; Chen, H.; Wang, D.; Liu, N.; Liu, D.; et al. Characteristics of COVID-19 infection in Beijing. J. Infect. 2020, 80, 401–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Huang, D.Q.; Zou, B.; Yang, H.; Hui, W.Z.; Rui, F.; Yee, N.T.S.; Liu, C.; Nerurkar, S.N.; Kai, J.C.Y.; et al. Epidemiology of COVID-19: A systematic review and meta-analysis of clinical characteristics, risk factors, and outcomes. J. Med. Virol. 2021, 93, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Ling, R.; Cheng, Y.; Wen, J.; Dai, Y.; Huang, W.; Zhang, S.; Lu, X.; Luo, Y.; Jiang, Y.Z. Characteristics of the Coronavirus Disease 2019 and related Therapeutic Options. Mol. Ther.-Methods Clin. Dev. 2020, 18, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Struyf, T.; Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Leeflang, M.M.; Spijker, R.; Hooft, L.; Emperador, D.; Dittrich, S.; et al. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19 disease. Cochrane Database Syst. Rev. 2020, 7, CD013665. [Google Scholar] [PubMed]
- Wan, S.; Xiang, Y.; Fang, W.; Zheng, Y.; Li, B.; Hu, Y.; Lang, C.; Huang, D.; Sun, Q.; Xiong, Y.; et al. Clinical features and treatment of COVID-19 patients in northeast Chongqing. J. Med. Virol. 2020, 92, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Benenson, S.; Oster, Y.; Cohen, M.J.; Nir-Paz, R. BNT162b2 mRNA Covid-19 Vaccine Effectiveness among Health Care Workers. N. Engl. J. Med. 2021, 384, 1775–1777. [Google Scholar] [CrossRef]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on covid-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study. BMJ 2021. [Google Scholar] [CrossRef]
- Chodick, G.; Tene, L.; Patalon, T.; Gazit, S.; Ben Tov, A.; Cohen, D.; Muhsen, K. Assessment of Effectiveness of 1 Dose of BNT162b2 Vaccine for SARS-CoV-2 Infection 13 to 24 Days After Immunization. JAMA Netw. Open 2021, 4, e2115985. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Sikavi, D.R.; Lo, C.-H.; Kwon, S.; Song, M.; et al. Risk of COVID-19 among frontline healthcare workers and the general community: A prospective cohort study. medRxiv Prepr. Serv. Health Sci. 2020. [Google Scholar] [CrossRef]
- Lan, F.-Y.; Wei, C.-F.; Hsu, Y.-T.; Christiani, D.C.; Kales, S.N. Work-related COVID-19 transmission in six Asian countries/areas: A follow-up study. PLoS ONE 2020, 15, e0233588. [Google Scholar] [CrossRef]
- Lee, K.; Worsnop, C.Z.; Grépin, K.A.; Kamradt-Scott, A. Global coordination on cross-border travel and trade measures crucial to COVID-19 response. Lancet 2020, 395, 1593–1595. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number | Percent |
|---|---|---|
| Sex | ||
| Male | 368 | 70.6 |
| Female | 153 | 29.4 |
| Age group (years) | ||
| 0–18 | 64 | 12.3 |
| 19–35 | 273 | 52.4 |
| 36–55 | 162 | 31.1 |
| 55–65 | 15 | 2.9 |
| >65 | 7 | 1.3 |
| Occupation | ||
| Civil servant | 16 | 3.1 |
| Private/corporate/business | 200 | 38.4 |
| Student | 78 | 15.0 |
| Farmer | 67 | 12.9 |
| Armed force/uniformed personnel | 65 | 12.5 |
| Homemaker | 54 | 10.4 |
| Monk/nun | 28 | 5.4 |
| Other * | 13 | 2.5 |
| Comorbidities and pregnancies | ||
| Uncomplicated diabetes mellitus | 12 | 2.3 |
| Pregnant women | 4 | 0.7 |
| Other ** | 3 | 0.5 |
| Symptomatic | ||
| No | 224 | 43 |
| Yes | 290 | 56 |
| Onset of symptoms | ||
| Before admission | 214 | 41.1 |
| On admission day | 47 | 9.0 |
| During isolation | 260 | 49.9 |
| Disease category among symptomatic (n = 290) | ||
| Mild disease | 288 | 98.3 |
| Severe pneumonia | 5 | 1.7 |
| Life-threatening anddeath | 0 | 0 |
| Vaccination Status | ||
| Vaccinated | 191 | 36.7 |
| Not vaccinated | 321 | 63.3 |
| Variable | Number | Mean | Std. Dev |
|---|---|---|---|
| Total white cell count | 158 | 6.52 × 103 | 2.149 |
| Absolute lymphocyte count | 158 | 1.88 × 103 | 0.754 |
| Platelets | 131 | 239.72 × 103 | 86.546 |
| Number of days of isolation stay when antibodies were detected | |||
| IgM * | 30 | 17.37 | 6.054 |
| IgG ** | 42 | 18.52 | 7.549 |
| Variables | Adjusted Hazard Ratio (95% Confidence Interval) | p-Value |
|---|---|---|
| Sex | ||
| Male | Reference | |
| Female | 0.95 (0.31, 2.84) | 0.921 |
| Age group (years) | ||
| ≤18 | Reference | |
| 19–30 | 3.56 (0.34, 37.12) | 0.288 |
| 31–40 | 2.03 (0.19, 21.66) | 0.559 |
| 41–50 | 1.41 (0.12, 16.03) | 0.782 |
| >50 | 0.28 (0.02, 3.62) | 0.327 |
| Vaccination status | ||
| Non-vaccinated | Reference | |
| Vaccinated | 0.23 (0.05, 0.98) | 0.047 * |
| Origin of cases | ||
| Returning travellers | Reference | |
| Frontline workers | 14.90 (1.27, 174.09) | 0.031 * |
| Indian origin | 1.95 (0.14, 26.70) | 0.616 |
| Community transmission | 8.33 (0.88, 78.79) | 0.065 |
| MDP worker | 41.29 (4.24, 402.36) | 0.001 * |
| Occupation | ||
| Private worker | Reference | |
| Armed forces | 1.26 (0.32, 4.92) | 0.744 |
| Student | 1.36 (0.12, 15.58) | 0.806 |
| Farmer | 0.73 (0.10, 5.36) | 0.758 |
| Civil servant and others | 7.21 (0.87, 59.96) | 0.067 |
| Homemaker | 2.33 (0.46, 11.77) | 0.308 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gyeltshen, K.; Tsheten, T.; Dorji, S.; Pelzang, T.; Wangdi, K. Survival Analysis of Symptomatic COVID-19 in Phuentsholing Municipality, Bhutan. Int. J. Environ. Res. Public Health 2021, 18, 10929. https://doi.org/10.3390/ijerph182010929
Gyeltshen K, Tsheten T, Dorji S, Pelzang T, Wangdi K. Survival Analysis of Symptomatic COVID-19 in Phuentsholing Municipality, Bhutan. International Journal of Environmental Research and Public Health. 2021; 18(20):10929. https://doi.org/10.3390/ijerph182010929
Chicago/Turabian StyleGyeltshen, Kinley, Tsheten Tsheten, Sither Dorji, Thinley Pelzang, and Kinley Wangdi. 2021. "Survival Analysis of Symptomatic COVID-19 in Phuentsholing Municipality, Bhutan" International Journal of Environmental Research and Public Health 18, no. 20: 10929. https://doi.org/10.3390/ijerph182010929