

Influence of the COVID-19 Pandemic on Italian LGBT+ Young Adults’ Mental Health: The Role of Neuroticism and Family Climate
 , , , and
, , , and
Abstract
:1. Theoretical Background
1.1. Prior Knowledge: Societal Stressors for LGBT+ People Living in Italy
1.2. COVID-19 and Psychological Adjustment for LGBT+ People
1.3. Factors Associated with Psychological Adjustment during Pandemic Time
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Psychosocial Effects of the COVID-19 Pandemic (Ad Hoc Questionnaire)
- ▪
- “To what extent has the COVID-19 pandemic affected your life?”
- ▪
- “To what extent do you currently feel limited in carrying out your usual activities due to the COVID-19 pandemic?”
- ▪
- “To what extent has the COVID-19 pandemic affected you emotionally (has made you feel angry, scared, upset or depressed)?”
- ▪
- “To what extent has the COVID-19 pandemic made you feel isolated from your heterosexual or cisgender friends?”
- ▪
- “To what extent has the COVID-19 pandemic made you feel isolated from your LGBT+ friends?”
- ▪
- “To what extent do you feel uncomfortable in your family in this specific moment of the COVID-19 pandemic?”
- ▪
- “To what extent did you feel “suffocated” because you could not express your LGBT+ identity with your family when restrictions were in place?”
- ▪
- “If the people you currently live with are aware of your LGBT+ identity. how do they respond to this?”
2.3.2. NEO Five-Factor Inventory-3 (NEO-FFI-3)
2.3.3. Enacted Stigma Scale of the Minority Stress Scale (MSS)
2.3.4. Depression, Anxiety and Stress Scale (DASS-21; for Mental Health Measures)
2.4. Data Analysis
2.4.1. Preliminary Analysis
2.4.2. Multiple Regressions: Predictors of Adverse Mental Health Conditions
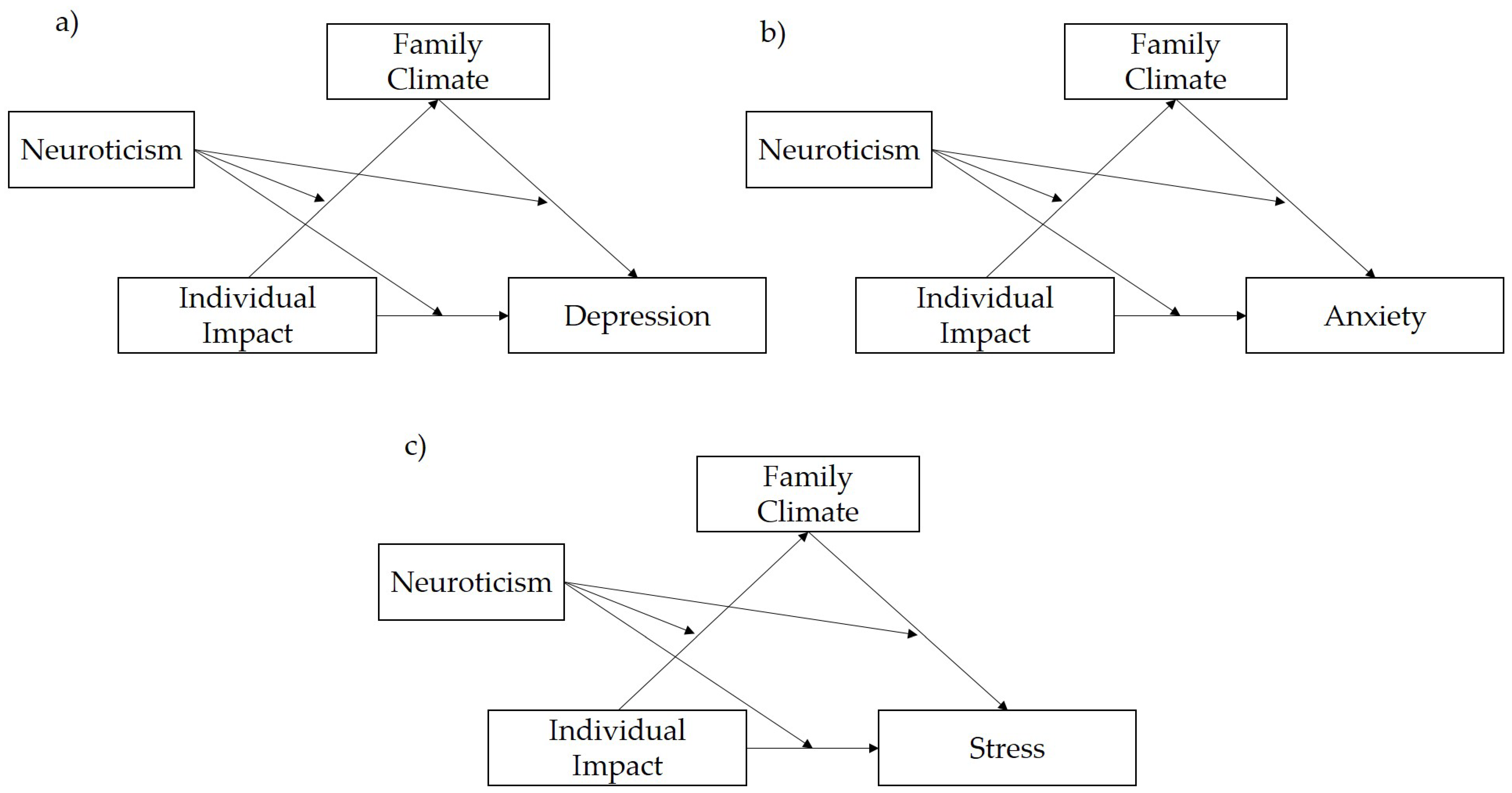
2.4.3. Conditional (Moderated) Mediation Analysis: Mechanisms Underlying Psychological Distress during the COVID-19 Pandemic
3. Results
3.1. Descriptive and Preliminary Analysis
3.2. Multiple Regressions: Predictors of Adverse Mental Health Conditions
3.3. Condition (Mediated) Moderation in jAMM: Mechanisms Underlying Psychological Distress during the COVID-19 Pandemic
4. Discussion
Limitations and Further Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cénat, J.M.; Farahi, S.M.M.M.; Dalexis, R.D.; Darius, W.P.; Bekarkhanechi, F.M.; Poisson, H.; Labelle, P.R. The global evolution of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis of longitudinal studies. J. Affect. Diso Rd. 2022, 315, 70–95. [Google Scholar] [CrossRef] [PubMed]
- Dpcm 8 March 2020 n. 59, Official Journal of the Italian Republic. Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/08/20A01522/sg (accessed on 3 November 2022).
- Dpcm 3 December 2020 n. 301 Official Journal of the Italian Republic. Available online: https://www.gazzettaufficiale.it/eli/id/2020/12/03/20A06767/sg (accessed on 3 November 2022).
- Dpcm 22 April 2021 n. 52 Official Journal of the Italian Republic. Available online: https://www.gazzettaufficiale.it/eli/id/2021/04/22/21G00064/sg (accessed on 3 November 2022).
- Leung, C.M.C.; Ho, M.K.; Bharwani, A.A.; Cogo-Moreira, H.; Wang, Y.; Chow, M.S.C.; Fan, X.; Galea, S.; Leung, G.M.; Ni, M.Y. Mental Disorders Following COVID-19 and Other Epidemics: A Systematic Review and Meta-Analysis. Transl. Psychiatry 2022, 12, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Boden, M.; Zimmerman, L.; Azevedo, K.J.; Ruzek, J.I.; Gala, S.; Abdel, M.H.S.; Cohen, N.; Walser, R.; Mahtani, N.D.; Hoggatt, K.J.; et al. Addressing the mental health impact of COVID-19 through population health. Clin. Psychol. Rev. 2021, 85, 102006. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. SSRN 2020, 395, 10227. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Beam, C.R.; Kim, A.J. Psychological sequelae of social isolation and loneliness might be a larger problem in young adults than older adults. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S58. [Google Scholar] [CrossRef] [PubMed]
- Fana, M.; Torrejón Pérez, S.; Fernández-Macías, E. Employment impact of Covid-19 crisis: From short term effects to long terms prospects. J. Ind. Bus. Econ. 2020, 47, 391–410. [Google Scholar] [CrossRef]
- Puers, A.S. COVID-19, Youth Employment, and Mental Health in Italy. European Student Think Tank. Available online: https://esthinktank.com/2021/06/24/covid-19-youth-employment-and-mental-health-in-italy/ (accessed on 26 August 2021).
- Khawar, M.B.; Abbasi, M.H.; Hussain, S.; Riaz, M.; Rafiq, M.; Mehmood, R.; Farooq, A. Psychological impacts of COVID-19 and satisfaction from online classes: Disturbance in daily routine and prevalence of depression, stress, and anxiety among students of Pakistan. Heliyon 2021, 7, e07030. [Google Scholar] [CrossRef] [PubMed]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef]
- ILGA-Europe. Annual Review of the Human Rights Situation of Lesbian, Gay, Bisexual, Trans and Intersex People in Europe and Central Asia. 2022. Available online: https://www.ilga-europe.org/annualreview/2022 (accessed on 3 November 2022).
- Flores, A.R.; The Williams Institute. Social Acceptance of LGBTI People in 175 Countries and Locations 1981 to 2020. Available online: https://williamsinstitute.law.ucla.edu/publications/global-acceptance-index-lgbt/ (accessed on 3 November 2022).
- Chamber of Deputees. DDL 4 November 2020, Measures against Discrimination and Violence on the Basis of Sex, Gender, Sexual Orientation, Gender Identity, and Disability, n. 2005. Available online: http://www.senato.it/leg/18/BGT/Schede/Ddliter/53457.htm# (accessed on 3 November 2022).
- Organisation for Economic Co-operation and Development (OECD). Society at a Glance 2019: OECD Social Indicators. OECD Publishing. Available online: https://doi.org/10.1787/soc_glance-2019-en (accessed on 3 November 2022).
- European Commission. Special Eurobarometer 493. Discrimination in the European Union. Directorate-General for Communication. 2019. Available online: https://doi.org/10.2838/5155 (accessed on 3 November 2022).
- Italian Constitutional Court. Sentence n. 180/2017. Available online: https://www.cortecostituzionale.it/actionSchedaPronuncia.do?anno=2017&numero=180 (accessed on 26 November 2022).
- Istituto Superiore di Sanità (ISS); Ufficio Nazionale Antidiscriminazioni Razziali—Presidenza del Consiglio dei Ministri (UNAR). Infotrans—Gender Identity Rights and Protection. 2020. Available online: https://www.infotrans.it/ (accessed on 3 November 2022).
- SIGIS. Il Percorso in Pillole. Available online: https://www.sigis.info/mappametro/ (accessed on 4 November 2022).
- Carpenter, M. The human rights of intersex people: Addressing harmful practices and rhetoric of change. Reprod. Health Matters 2016, 24, 74–84. [Google Scholar] [CrossRef] [Green Version]
- Creighton, S.; Minto, C. Managing intersex. BMJ 2001, 323, 1264–1265. [Google Scholar] [CrossRef] [PubMed]
- Minto, C.L.; Liao, L.M.; Woodhouse, C.R.; Ransley, P.G.; Creighton, S.M. The effect of clitoral surgery on sexual outcome in individuals who have intersex conditions with ambiguous genitalia: A cross-sectional study. Lancet 2003, 361, 1252–1257. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Truffer, D.; Crocetti, D. Intersex human rights. Int. J. Hum. Rights 2019, 24, 724–749. [Google Scholar] [CrossRef]
- Lebow, J.L. Family in the Age of COVID-19. Fam. Process 2020, 59, 309–312. [Google Scholar] [CrossRef]
- Smith, S.K. Transgender and Gender Nonbinary Persons’ Health and Well-Being: Reducing Minority Stress to Improve Well-Being. Creat. Nurs. 2020, 26, 88–95. [Google Scholar] [CrossRef]
- Soiné, H.; Kriegel, L.; Dollmann, J. The impact of the COVID-19 pandemic on risk perceptions: Differences between ethnic groups in Germany. Eur. Soc. 2020, 23, S289–S306. [Google Scholar] [CrossRef]
- Rothman, S.; Gunturu, S.; Korenis, P. The mental health impact of the COVID-19 epidemic on immigrants and racial and ethnic minorities. QJM Int. J. Med. 2020, 113, 779–782. [Google Scholar] [CrossRef] [PubMed]
- Gouvernet, B.; Bonierbale, M. Bio-psychosocial study on the impact of the COVID-19 lockdown on depression and anxiety in a sample of 1753 French-speaking subjects. Encephale 2022, 48, 118–124. [Google Scholar] [CrossRef]
- Peterson, Z.D.; Vaughan, E.L.; Carver, D.N. Sexual identity and psychological reactions to COVID-19. Traumatology 2021, 27, 6–13. [Google Scholar] [CrossRef]
- Phillips Ii, G.; Felt, D.; Ruprecht, M.M.; Wang, X.; Xu, J.; Pérez-Bill, E.; Bagnarol, R.M.; Roth, J.; Curry, C.W.; Beach, L.B. Addressing the Disproportionate Impacts of the COVID-19 Pandemic on Sexual and Gender Minority Populations in the United States: Actions Toward Equity. LGBT Health 2020, 7, 279–282. [Google Scholar] [CrossRef]
- Meyer, I.H. Minority Stress and Mental Health in Gay Men. J. Health Soc. Behav. 1995, 36, 38. [Google Scholar] [CrossRef] [PubMed]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, T.H.; Zlotorzynska, M.; Rai, M.; Baral, S.D. Characterizing the impact of COVID-19 on men who have sex with men across the United States in April 2020. AIDS Behav. 2020, 24, 2024–2032. [Google Scholar] [CrossRef] [PubMed]
- Silliman, C.R.I.; Bosk, E.A. Vulnerable Youth and the COVID-19 Pandemic. Pediatrics 2020, 146, e20201306. [Google Scholar] [CrossRef]
- The Lancet HIV. Lockdown fears for key populations. Lancet HIV 2020, 7, e373. [Google Scholar] [CrossRef]
- Salerno, J.P.; Devadas, J.; Pease, M.; Nketia, B.; Fish, J.N. Sexual and Gender Minority Stress Amid the COVID-19 Pandemic: Implications for LGBTQ Young Persons’ Mental Health and Well-Being. Public Health Rep. 2020, 135, 721–727. [Google Scholar] [CrossRef]
- Gato, J.; Barrientos, J.; Tasker, F.; Miscioscia, M.; Cerqueira-Santos, E.; Malmquist, A.; Seabra, D.; Leal, D.; Houghton, M.; Poli, M.; et al. Psychosocial effects of the COVID-19 pandemic and mental health among LGBTQ+ young adults: A cross-cultural comparison across six nations. J. Homosex. 2021, 68, 612–630. [Google Scholar] [CrossRef]
- Malmquist, A.; Bredenberg, C.; Melin, J.; Wurm, M.; Tasker, F.; Gato, J. Queers in quarantine: Young LGBTQ+ people’s experiences during the COVID-19 pandemic in Sweden. Scand. J. Psychol. 2022. [Google Scholar] [CrossRef]
- Gonzales, G.; de Mola, E.L.; Gavulic, K.A.; McKay, T.; Purcell, C. Mental health needs among lesbian, gay, bisexual, and transgender college students during the COVID-19 pandemic. J. Adolesc. Health 2020, 67, 645–648. [Google Scholar] [CrossRef]
- Konnoth, C. Supporting LGBT communities in the COVID-19 pandemic. In COVID-19 Policy Playbook: Legal Recommendations for a Safer, More Equitable Future; Burris, S., de Guia, S., Gable, L., Levin, D.E., Parmet, W.E., Terry, N.P., Eds.; Public Health Law Watch: Boston, MA, USA, 15 February 2021; Available online: https://ssrn.com/abstract=3809468 (accessed on 15 February 2021).
- Mattei, G.; Russo, T.; Addabbo, T.; Galeazzi, G.M. The COVID-19 recession might increase discriminating attitudes toward LGBT people and mental health problems due to minority stress. Int. J. Soc. Psychiatry 2021, 67, 400–401. [Google Scholar] [CrossRef] [PubMed]
- Mirabella, M.; Senofonte, G.; Giovanardi, G.; Lingiardi, V.; Fortunato, A.; Lombardo, F.; Speranza, A.M. Psychological Well-Being of Trans* People in Italy During the COVID-19 Pandemic: Critical Issues and Personal Experiences. Sex Res. Social Policy 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Diener, E. Subjective well-being: The science of happiness and a proposal for a national index. Am. Psychol. 2000, 55, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Erikson, E.H. Youth: Fidelity and Diversity in Youth: Change & Challenge; Basic Books, Inc.: New York, NY, USA, 1963; pp. 1–23. [Google Scholar]
- Vleioras, G.; Bosma, H.A. Are identity styles important for psychological well-being? J. Adolesc. 2005, 28, 397–409. [Google Scholar] [CrossRef]
- McCrae, R.R. Controlling neuroticism in the measurement of stress. Stress Med. 1990, 6, 237–241. [Google Scholar] [CrossRef]
- Schmutte, P.S.; Ryff, C.D. Personality and well-being: Reexamining methods and meanings. J. Pers. Soc. Psychol. 1997, 73, 549–559. [Google Scholar] [CrossRef]
- Lavasani, M.G.; Borhanzadeh, S.; Afzali, L.; Hejazi, E. The Relationship between Perceived Parenting Styles, Social Support with Psychological Well- Being. Procedia Soc. Behav. Sci. 2011, 15, 1852–1856. [Google Scholar] [CrossRef] [Green Version]
- Shaw, D.S.; Criss, M.M.; Schonberg, M.A.; Beck, J.E. The Development of Family Hierarchies and Their Relation to Children’s Conduct Problems. Dev. Psychopathol. 2004, 16, 483–500. [Google Scholar] [CrossRef] [Green Version]
- Wickrama KA, S.; Lorenz, F.O.; Conger, R.D. Parental Support and Adolescent Physical Health Status: A Latent Growth- Curve Analysis. J. Health Soc. Behav. 1997, 38, 149–163. [Google Scholar] [CrossRef]
- Carr, D. The Fulfillment of Career Dreams at Midlife: Does It Matter for Women’s Mental Health? J. Health Soc. Behav. 1997, 38, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Lindfors, P.; Berntsson, L.; Lundberg, U. Total Workload as Related to Psychological Well-Being and Symptoms in Full-Time Employed Female and Male White-Collar Workers. Int. J. Behav. Med. 2006, 13, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, L.R. The structure of phenotypic personality traits. Am. Psychol. 1993, 48, 26–34. [Google Scholar] [CrossRef]
- McCrae, R.R.; Costa, P.T. Validation of the five-factor model of personality across instruments and observers. J. Personal. Soc. Psychol. 1987, 52, 81. [Google Scholar] [CrossRef] [PubMed]
- Campbell-Sills, L.; Cohan, S.L.; Stein, M.B. Relationship of resilience to personality, coping, and psychiatric symptoms in young adults. Behav. Res. Ther. 2006, 44, 585–599. [Google Scholar] [CrossRef] [PubMed]
- Komulainen, E.; Meskanen, K.; Lipsanen, J.; Lahti, J.M.; Jylhä, P.; Melartin, T.; Ekelund, J. The effect of personality on daily life emotional processes. PLoS ONE 2014, 9, e110907. [Google Scholar] [CrossRef]
- Schneider, T.R. The role of neuroticism on psychological and physiological stress responses. J. Exp. Soc. Psychol. 2004, 40, 795–804. [Google Scholar] [CrossRef]
- DeNeve, K.M.; Cooper, H. The happy personality: A meta-analysis of 137 personality traits and subjective well-being. Psychol. Bull. 1998, 124, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hao, R.; Dong, H.; Zhang, R.; Li, P.; Zhang, P.; Hu, J.; Zhang, M. The relationship between neuroticism fit and general well-being: The mediating effect of psychological resilience. Front. Psychol. 2019, 10, 2219. [Google Scholar] [CrossRef]
- Roelofs, J.; Huibers, M.; Peeters, F.; Arntz, A.; van Os, J. Rumination and Worrying as Possible Mediators in the Relation between Neuroticism and Symptoms of Depression and Anxiety in Clinically Depressed Individuals. Behav. Res. 2008, 46, 1283–1289. [Google Scholar] [CrossRef]
- Sobol-Kwapinska, M. Calm down—It’s only neuroticism. Time perspectives as moderators and mediators of the relationship between neuroticism and well-being. Personal. Individ. Differ. 2016, 94, 64–71. [Google Scholar] [CrossRef]
- Liu, C.; Chen, L.; Chen, S. Influence of Neuroticism on Depressive Symptoms Among Chinese Adolescents: The Mediation Effects of Cognitive Emotion Regulation Strategies. Front. Psychiatry 2020, 11, 420. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Shi, Z.; Li, H. Neuroticism, Extraversion, Emotion Regulation, Negative Affect and Positive Affect: The Mediating Roles of Reappraisal and Suppression. Soc. Behav. Personal. Int. J. 2009, 37, 193–194. [Google Scholar] [CrossRef]
- Trnka, R.; Čábelková, I. Neuroticism across cultures: Macro-level insights into the worldwide distribution of neuroticism. In Neuroticism: Characteristics, Impact on Job Performance and Health Outcomes; Di Fabio, A., Ed.; Nova Science Publishers: New York, NY, USA, 2016; pp. 161–185. [Google Scholar]
- Widiger, T.A.; Mullins-Sweatt, S.N. Five-factor model of personality disorder: A proposal for DSM-V. Annu. Rev. Clin. Psychol. 2009, 5, 197–220. [Google Scholar] [CrossRef] [PubMed]
- Dalton III, W.T.; Frick-Horbury, D.; Kitzmann, K.M. Young adults’ retrospective reports of parenting by mothers and fathers: Associations with current relationship quality. J. Gen. Psychol. 2006, 133, 5–18. [Google Scholar] [CrossRef]
- Levine, S. Psychological and social aspects of resilience: A synthesis of risks and resources. Dialogues Clin. Neurosci. 2003, 5, 273–280. [Google Scholar] [CrossRef]
- Noble, T.; McGrath, H. Wellbeing and resilience in young people and the role of positive relationships. In Positive Relationships; Springer: Dordrecht, The Netherlands, 2012; pp. 17–33. [Google Scholar]
- Masten, A.S. Ordinary magic: Resilience processes in development. Am. Psychol. 2001, 56, 227. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Wortman, C.B.; Nesse, R.M. Prospective patterns of resilience and maladjustment during widowhood. Psychol. Aging 2004, 19, 260. [Google Scholar] [CrossRef] [Green Version]
- Masten, A.S. Ordinary magic: Lessons from research on resilience in human development. Educ. Can. 2009, 49, 28–32. [Google Scholar]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Neighmond, P. Home However, Not Safe, Some LGBTQ Young People Face Rejection From Families in Lockdown. NPR. Available online: https://www.npr.org/sections/health-shots/2020/05/17/856090474/home-but-not-safe-some-lgbtq-young-people-face-rejection-from-families-in-lockdo?t=1630005639617 (accessed on 26 August 2021).
- Gattamorta, K.; Salerno, J.P.; Roman Laporte, R. Family Rejection during COVID-19: Effects on Sexual and Gender Minority Stress and Mental Health among LGBTQ University Students. LGBTQ+ Fam. Interdiscip. J. 2022, 18, 1–14. [Google Scholar] [CrossRef]
- Dishion, T.; Forgatch, M.; Chamberlain, P.; Pelham, W.E. The Oregon model of behavior family therapy: From intervention design to promoting large-scale system change. Behav. Ther. 2016, 47, 812–837. [Google Scholar] [CrossRef] [PubMed]
- Fish, J.N.; McInroy, L.B.; Paceley, M.S.; Williams, N.D.; Henderson, S.; Levine, D.S.; Edsall, R.N. “I’m kinda stuck at home with unsupportive parents right now”: LGBTQ youths’ experiences with COVID-19 and the importance of online support. J. Adolesc. Health 2020, 67, 450–452. [Google Scholar] [CrossRef] [PubMed]
- Suen, Y.T.; Chan, R.; Wong, E.M.Y. Effects of general and sexual minority-specific covid-19-related stressors on the mental health of lesbian, gay, and bisexual people in Hong Kong. Psychiatry Res. 2020, 292, 113365. [Google Scholar] [CrossRef] [PubMed]
- McEwing, E. Delivering Culturally Competent Care to the Lesbian, Gay, Bisexual, And Transgender (LGBT) Population: Education for Nursing Students. Nurse Educ. Today 2020, 94, 104573. [Google Scholar] [CrossRef]
- Lim, F.A.; Brown, D.V.; Justin Kim, S.M. Addressing Health Care Disparities in the Lesbian, Gay, Bisexual, and Transgender Population: A Review of Best Practices. AJN Am. J. Nurs. 2014, 114, 24–34. [Google Scholar] [CrossRef]
- Barrientos, J.; Guzmán-González, M.; Urzúa, A.; Ulloa, F. Psychosocial impact of COVID-19 pandemic on LGBT people in Chile. Sexologies 2021, 30, e35–e41. [Google Scholar] [CrossRef]
- Gato, J.; Leal, D.; Seabra, D. When home is not a safe haven: Effects of the COVID-19 pandemic on LGBTQ adolescents and young adults in Portugal. Psicologia 2020, 34, 89–100. [Google Scholar] [CrossRef]
- Bojanowska, A.; Zalewska, A.M. Subjective well-being among teenagers of different ages: The role of emotional reactivity and social support from various sources. Stud. Psychol. 2011, 49, 5–21. [Google Scholar] [CrossRef]
- Lynskey, M.T.; Fergusson, D.M. Factors protecting against the development of adjustment difficulties in young adults exposed to childhood sexual abuse. Child Abus. Negl. 1997, 21, 1177–1190. [Google Scholar] [CrossRef]
- McCrae, R.R.; Costa, P.T., Jr.; Martin, T.A. The NEO-PI-3: A more readable Revised. NEO Personality Inventory. J. Personal. Assess. 2005, 84, 261–270. [Google Scholar] [CrossRef]
- Fossati, L.; Ciancaleoni, M. NEO-PI-3-NEO Personality Inventory-3 (Italian Validation); Hogrefe Editore: Firenze, Italy, 2014. [Google Scholar]
- Costa, P.T.; McCrae, R.R. Four ways five factors are basic. Pers. Individ. Dif. 1992, 13, 653–665. [Google Scholar] [CrossRef]
- Pala, A.N.; Dell’Amore, F.; Steca, P.; Clinton, L.; Sandfort, T.; Rael, C. Validation of the Minority Stress Scale among Italian gay and bisexual men. Psychol. Sex. Orientat. Gend. 2017, 4, 451–459. [Google Scholar]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety & Stress Scales, 2nd ed.; Sydney, Psychology Foundation: Sydney, Australia, 1995. [Google Scholar]
- Bottesi, G.; Ghisi, M.; Altoè, G.; Conforti, E.; Melli, G.; Sica, C. The Italian version of the Depression Anxiety Stress Scales-21: Factor structure and psychometric properties on community and clinical samples. Compr. Psychiatry. 2015, 60, 170–181. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing (3.6.3) [Computer software], R Foundation for Statistical Com-puting: Vienna, Austria. Available online: https://www.r-project.org/(accessed on 3 November 2022).
- RStudio Team. RStudio: Integrated Development for R (1.2.5033-1) [Computer Software], RStudio, Inc.: Boston, MA, USA. Available online: http://www.rstudio.com/(accessed on 3 November 2022).
- The Jamovi Project. Jamovi (1.8.2) [Computer Software]. Available online: https://www.jamovi.org(accessed on 3 November 2022).
- Snapp, S.D.; Watson, R.J.; Russell, S.T.; Diaz, R.M.; Ryan, C. Social support networks for LGBT young adults: Low cost strategies for positive adjustment. Fam. Relat. 2015, 64, 420–430. [Google Scholar] [CrossRef]
- Testa, R.J.; Habarth, J.; Peta, J.; Balsam, K.; Bockting, W. Development of the gender minority stress and resilience measure. Psychol. Sex. Orientat. Gend. Divers. 2015, 2, 65–77. [Google Scholar] [CrossRef]
- Scandurra, C.; Pennasilico, A.; Esposito, C.; Mezza, F.; Vitelli, R.; Bochicchio, V.; Maldonato, N.M.; Amodeo, A.L. Minority Stress and Mental Health in Italian Bisexual People. Soc. Sci. 2020, 9, 46. [Google Scholar] [CrossRef] [Green Version]
- Kelleher, C. Minority stress and health: Implications for lesbian, gay, bisexual, transgender, and questioning (LGBTQ) young people. Couns. Psychol. Q. 2009, 22, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Mink, M.D.; Lindley, L.L.; Weinstein, A.A. Stress, Stigma, and Sexual Minority Status: The Intersectional Ecology Model of LGBTQ Health. J. Gay Lesbian Soc. Serv. 2014, 26, 502–521. [Google Scholar] [CrossRef]
- Newcomb, M.E.; Mustanski, B. Internalized homophobia and internalizing mental health problems: A meta-analytic review. Clin. Psychol. Rev. 2010, 30, 1019–1029. [Google Scholar] [CrossRef]
- Clarke, D. Neuroticism: Moderator or mediator in the relation between locus of control and depression? Pers. Individ. Dif. 2004, 37, 245–258. [Google Scholar] [CrossRef]
- Calvo, V.; Cusinato, M.; Meneghet, N.; Miscioscia, M. Perceived Social Support Mediates the Negative Impact of Insecure Attachment Orientations on Internalized Homophobia in Gay Men. J. Homosex. 2021, 13, 2266–2284. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | n | % | Variable | n | % |
|---|---|---|---|---|---|
| Sex assigned at birth | Area of residence | ||||
| Female | 228 | 56.02 | Rural | 110 | 27.03 |
| Male | 171 | 42.01 | Urban | 297 | 72.97 |
| Intersex | 3 | 0.74 | Relationship status | ||
| Prefer not to say | 5 | 1.23 | Not in a relationship | 190 | 46.68 |
| Gender identity | In a relationship | 217 | 53.32 | ||
| Cisgender women | 170 | 41.77 | Living with family | ||
| Cisgender men | 150 | 36.86 | Yes | 277 | 68.06 |
| Transgender persons | 16 | 3.93 | No | 130 | 31.94 |
| Non-binary persons | 51 | 12.53 | Educational level | ||
| Other | 21 | 5.16 | Lower secondary | 25 | 6.14 |
| Sexual orientation | Upper secondary | 211 | 51.84 | ||
| Gay/lesbian | 230 | 56.51 | Bachelor’s | 89 | 21.87 |
| Bisexual | 104 | 25.55 | Postgraduate | 82 | 20.15 |
| Pansexual | 40 | 9.83 | Work status | ||
| Asexual | 9 | 2.21 | Student | 172 | 42.26 |
| Heterosexual | 5 | 1.23 | Student-worker | 47 | 11.55 |
| Other | 19 | 4.67 | Full-time worker | 92 | 22.60 |
| Nationality | Part-time worker | 32 | 7.86 | ||
| Italian | 397 | 97.54 | Unemployed | 49 | 12.04 |
| Other | 10 | 2.46 | Payroll subsidies | 1 | 0.25 |
| Region of residence | Other | 14 | 3.44 | ||
| North | 261 | 64.13 | Work changes due to COVID-19 | ||
| Centre | 69 | 16.95 | Yes | 161 | 39.56 |
| South | 52 | 12.78 | No | 246 | 60.44 |
| Islands | 25 | 6.14 |
| Factor Loading | |||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | Communality | Uniqueness | |
| Item 1 | 0.71 | 0.20 | 0.55 | 0.45 | |
| Item 2 | 0.73 | 0.17 | 0.58 | 0.42 | |
| Item 3 | 0.76 | 0.16 | 0.18 | 0.64 | 0.36 |
| Item 6 | 0.35 | 0.20 | 0.53 | 0.44 | 0.56 |
| Item 9 | 0.31 | 0.68 | 0.11 | 0.57 | 0.43 |
| Item 10 | 0.18 | 0.97 | 0.12 | 0.99 | 0.01 |
| Item 7 | 0.17 | 0.11 | 0.79 | 0.67 | 0.33 |
| Item 8 | 0.72 | 0.51 | 0.49 | ||
| % Explained variance | 0.24 | 0.20 | 0.19 | ||
| Eigenvalue | 1.90 | 1.56 | 1.49 | ||
| Coefficient alpha | 0.81 | 0.73 | 0.84 | ||
| Variable | Mean | SD | Median | MAD | Min | Max | Skew | Kurtosis | SE |
|---|---|---|---|---|---|---|---|---|---|
| Individual Impact | 7.24 | 2.06 | 7.67 | 1.98 | 0 | 10 | −0.88 | 0.32 | 0.10 |
| Social Isolation | 5.93 | 3.07 | 6.50 | 3.71 | 0 | 10 | −0.54 | −0.74 | 0.15 |
| Family Climate | 6.55 | 2.67 | 7.00 | 2.97 | 0 | 10 | −0.57 | −0.61 | 0.13 |
| DASS_Depression | 10.81 | 6.39 | 11 | 8.90 | 0 | 21 | 0.06 | −1.21 | 0.32 |
| DASS_Anxiety | 7.51 | 6.11 | 6 | 5.93 | 0 | 21 | 0.60 | −0.85 | 0.30 |
| DASS_Stress | 12.91 | 5.35 | 13 | 5.93 | 0 | 21 | −0.23 | −0.94 | 0.27 |
| NEO-FFI3_Neuroticism | 72.88 | 14.89 | 74.32 | 15.44 | 25.34 | 102.59 | −0.26 | −0.52 | 0.74 |
| MSS_Enacted stigma | 2.11 | 0.76 | 2 | 0.74 | 1 | 5 | 0.60 | 0.05 | 0.04 |
| M1 Depression | M2 Anxiety | M3 Stress | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 95% C.I. | 95% C.I. | 95% C.I. | |||||||||||||||||||
| Predictor (model 1) | Estimate | SE | t | p | Stand. Estimate | Lower | Upper | Estimate | SE | t | p | Stand. Estimate | Lower | Upper | Estimate | SE | t | p | Stand. Estimate | Lower | Upper |
| Intercept a | 6.534 | 2.183 | 2.993 | 0.003 | 5.064 | 2.093 | 2.420 | 0.016 | 9.746 | 1.921 | 5.073 | <0 .001 | |||||||||
| Age | −0.131 | 0.078 | −1.670 | 0.096 | −0.096 | −0.209 | 0.017 | −0.235 | 0.075 | −3.126 | 0.002 | −0.180 | −0.293 | −0.067 | −0.154 | 0.069 | −2.228 | 0.026 | −0.134 | −0.253 | −0.016 |
| Gender Identity | |||||||||||||||||||||
| other–cis | 0.509 | 1.306 | 0.390 | 0.697 | 0.080 | −0.322 | 0.481 | −0.937 | 1.252 | −0.749 | 0.455 | −0.153 | −0.556 | 0.249 | 1.680 | 1.149 | 1.462 | 0.145 | 0.314 | −0.108 | 0.736 |
| nb–cis | 0.496 | 0.908 | 0.546 | 0.585 | 0.078 | −0.202 | 0.357 | −0.524 | 0.870 | −0.603 | 0.547 | −0.086 | −0.366 | 0.194 | 0.416 | 0.799 | 0.521 | 0.602 | 0.078 | −0.216 | 0.371 |
| tg–cis | −1.346 | 1.543 | −0.872 | 0.384 | −0.211 | −0.685 | 0.264 | −1.249 | 1.479 | −0.844 | 0.399 | −0.204 | −0.680 | 0.272 | −1.325 | 1.358 | −0.976 | 0.330 | −0.248 | −0.747 | 0.251 |
| Sexual Orientation: | |||||||||||||||||||||
| other–homo | 0.374 | 1.132 | 0.330 | 0.742 | 0.058 | −0.290 | 0.407 | 0.202 | 1.085 | 0.186 | 0.852 | 0.033 | −0.316 | 0.382 | −0.106 | 0.996 | −0.106 | 0.915 | −0.020 | −0.386 | 0.346 |
| bisex–homo | 1.677 | 0.710 | 2.364 | 0.019 | 0.263 | 0.044 | 0.481 | 0.487 | 0.680 | 0.716 | 0.474 | 0.080 | −0.139 | 0.299 | 1.172 | 0.625 | 1.876 | 0.061 | 0.219 | −0.011 | 0.448 |
| pan–homo | 1.893 | 1.038 | 1.823 | 0.069 | 0.296 | −0.023 | 0.616 | 1.685 | 0.995 | 1.692 | 0.091 | 0.276 | −0.045 | 0.596 | 1.407 | 0.914 | 1.540 | 0.124 | 0.263 | −0.073 | 0.599 |
| Living in Family | 0.753 | 0.661 | 1.140 | 0.255 | 0.055 | −0.040 | 0.150 | 0.315 | 0.634 | 0.497 | 0.619 | 0.024 | −0.071 | 0.119 | −0.153 | 0.582 | −0.264 | 0.792 | −0.013 | −0.113 | 0.086 |
| Education | 0.035 | 0.637 | 0.055 | 0.957 | 0.003 | −0.094 | 0.100 | −0.065 | 0.611 | −0.106 | 0.915 | −0.005 | −0.102 | 0.092 | 0.335 | 0.561 | 0.598 | 0.551 | 0.031 | −0.071 | 0.133 |
| Employment Situation | −1.810 | 0.655 | −2.763 | 0.006 | −0.141 | −0.242 | −0.041 | 0.147 | 0.628 | 0.234 | 0.815 | 0.012 | −0.089 | 0.113 | −0.018 | 0.577 | −0.031 | 0.976 | −0.002 | −0.107 | 0.104 |
| In a Romantic Relationship | −0.348 | 0.595 | −0.584 | 0.559 | −0.027 | −0.119 | 0.064 | −0.119 | 0.571 | −0.208 | 0.835 | −0.010 | −0.101 | 0.082 | 0.544 | 0.524 | 1.039 | 0.299 | 0.051 | −0.045 | 0.147 |
| other problems: | |||||||||||||||||||||
| pnr–no | 3.281 | 0.930 | 3.528 | <0 .001 | 0.513 | 0.227 | 0.800 | 3.153 | 0.891 | 3.537 | <0 .001 | 0.516 | 0.229 | 0.803 | 2.677 | 0.818 | 3.271 | 0.001 | 0.500 | 0.200 | 0.801 |
| yes–no | 3.901 | 0.656 | 5.943 | <0 .001 | 0.610 | 0.409 | 0.813 | 4.079 | 0.629 | 6.482 | <0 .001 | 0.668 | 0.465 | 0.870 | 2.564 | 0.578 | 4.438 | <0 .001 | 0.479 | 0.267 | 0.691 |
| Enacted Stigma | 1.528 | 0.389 | 3.924 | <0 .001 | 0.183 | 0.091 | 0.274 | 1.693 | 0.373 | 4.536 | <0 .001 | 0.212 | 0.120 | 0.304 | 1.108 | 0.343 | 3.233 | 0.001 | 0.158 | 0.062 | 0.255 |
| Time | 1.399 | 0.631 | 2.216 | 0.027 | 0.102 | 0.012 | 0.192 | 1.574 | 0.605 | 2.601 | 0.010 | 0.120 | 0.029 | 0.210 | 1.341 | 0.556 | 2.414 | 0.016 | 0.116 | 0.022 | 0.211 |
| 95% C.I. | 95% C.I. | 95% C.I. | |||||||||||||||||||
| Predictor (model 2) | Estimate | SE | t | p | Stand. Estimate | Lower | Upper | Estimate | SE | t | p | Stand. Estimate | Lower | Upper | Estimate | SE | t | p | Stand. Estimate | Lower | Upper |
| Intercept a | −7.898 | 2.324 | −3.399 | <0 .001 | −3.255 | 2.442 | −1.333 | 0.183 | −0.444 | 2.192 | −0.202 | 0.840 | |||||||||
| Age | −0.020 | 0.063 | −0.315 | 0.753 | −0.014 | −0.105 | 0.076 | −0.183 | 0.066 | −2.765 | 0.006 | −0.140 | −0.239 | −0.040 | −0.099 | 0.059 | −1.663 | 0.097 | −0.086 | −0.188 | 0.016 |
| Gender Identity | |||||||||||||||||||||
| other–cis | 0.123 | 1.033 | 0.119 | 0.905 | 0.019 | −0.299 | 0.337 | −1.507 | 1.085 | −1.389 | 0.166 | −0.247 | −0.596 | 0.103 | 1.208 | 0.974 | 1.240 | 0.216 | 0.226 | −0.132 | 0.584 |
| nb–cis | −0.369 | 0.719 | −0.513 | 0.608 | −0.058 | −0.279 | 0.164 | −1.263 | 0.755 | −1.672 | 0.095 | −0.207 | −0.450 | 0.036 | −0.201 | 0.678 | −0.297 | 0.767 | −0.038 | −0.287 | 0.212 |
| tg–cis | −1.740 | 1.219 | −1.427 | 0.154 | −0.272 | −0.647 | 0.103 | −1.446 | 1.281 | −1.129 | 0.260 | −0.237 | −0.649 | 0.176 | −1.406 | 1.150 | −1.222 | 0.222 | −0.263 | −0.685 | 0.160 |
| Sexual Orientation: | |||||||||||||||||||||
| other–homo | 0.715 | 0.899 | 0.795 | 0.427 | 0.112 | −0.165 | 0.389 | 0.681 | 0.945 | 0.720 | 0.472 | 0.111 | −0.193 | 0.415 | 0.473 | 0.848 | 0.558 | 0.578 | 0.088 | −0.223 | 0.400 |
| bisex–homo | 0.541 | 0.564 | 0.959 | 0.338 | 0.085 | −0.089 | 0.258 | −0.329 | 0.593 | −0.556 | 0.579 | −0.054 | −0.245 | 0.137 | 0.355 | 0.532 | 0.667 | 0.505 | 0.066 | −0.129 | 0.262 |
| pan–homo | 0.786 | 0.822 | 0.956 | 0.340 | 0.123 | −0.130 | 0.376 | 0.870 | 0.864 | 1.007 | 0.315 | 0.142 | −0.136 | 0.420 | 0.682 | 0.776 | 0.879 | 0.380 | 0.127 | −0.158 | 0.412 |
| Living in Family | 0.977 | 0.537 | 1.820 | 0.070 | 0.071 | −0.006 | 0.149 | 0.563 | 0.564 | 0.997 | 0.319 | 0.043 | −0.042 | 0.128 | −0.162 | 0.507 | −0.320 | 0.749 | −0.014 | −0.101 | 0.073 |
| Education | −0.170 | 0.502 | −0.338 | 0.736 | −0.013 | −0.090 | 0.063 | −0.245 | 0.528 | −0.463 | 0.643 | −0.020 | −0.104 | 0.064 | 0.166 | 0.474 | 0.349 | 0.727 | 0.015 | −0.071 | 0.101 |
| Employment Situation | −0.886 | 0.522 | −1.695 | 0.091 | −0.069 | −0.149 | 0.011 | 0.895 | 0.549 | 1.630 | 0.104 | 0.073 | −0.015 | 0.161 | 0.717 | 0.493 | 1.455 | 0.146 | 0.067 | −0.024 | 0.157 |
| In a Romantic Relationship | −0.144 | 0.479 | −0.301 | 0.763 | −0.011 | −0.085 | 0.062 | 0.265 | 0.503 | 0.526 | 0.599 | 0.022 | −0.059 | 0.102 | 0.719 | 0.451 | 1.593 | 0.112 | 0.067 | −0.016 | 0.150 |
| other problems: | |||||||||||||||||||||
| pnr–no | 1.008 | 0.748 | 1.346 | 0.179 | 0.158 | −0.073 | 0.388 | 1.504 | 0.786 | 1.912 | 0.057 | 0.246 | −0.007 | 0.499 | 1.092 | 0.706 | 1.547 | 0.123 | 0.204 | −0.055 | 0.463 |
| yes–no | 1.562 | 0.545 | 2.868 | 0.004 | 0.244 | 0.077 | 0.412 | 2.389 | 0.572 | 4.175 | <0 .001 | 0.391 | 0.207 | 0.575 | 0.834 | 0.514 | 1.624 | 0.105 | 0.156 | −0.033 | 0.345 |
| Enacted Stigma | 0.013 | 0.329 | 0.038 | 0.969 | 0.002 | −0.076 | 0.079 | 0.302 | 0.346 | 0.873 | 0.383 | 0.038 | −0.047 | 0.123 | −0.154 | 0.311 | −0.497 | 0.620 | −0.022 | −0.109 | 0.065 |
| Time | 0.186 | 0.532 | 0.350 | 0.727 | 0.014 | −0.063 | 0.090 | 0.340 | 0.559 | 0.607 | 0.544 | 0.026 | −0.058 | 0.110 | −0.012 | 0.502 | −0.023 | 0.982 | −9.95 × 10−4 | −0.087 | 0.085 |
| Individual Impact | 0.460 | 0.140 | 3.288 | 0.001 | 0.148 | 0.060 | 0.237 | 0.451 | 0.147 | 3.065 | 0.002 | 0.152 | 0.054 | 0.249 | 0.619 | 0.132 | 4.691 | <0 .001 | 0.238 | 0.138 | 0.338 |
| Family Climate | −0.286 | 0.102 | −2.815 | 0.005 | −0.120 | −0.203 | −0.036 | −0.360 | 0.107 | −3.365 | <0 .001 | −0.157 | −0.249 | −0.065 | −0.167 | 0.096 | −1.742 | 0.082 | −0.083 | −0.178 | 0.011 |
| Social Isolation | −0.094 | 0.085 | −1.101 | 0.272 | −0.045 | −0.126 | 0.035 | 0.133 | 0.090 | 1.486 | 0.138 | 0.067 | −0.022 | 0.155 | 0.066 | 0.080 | 0.818 | 0.414 | 0.038 | −0.053 | 0.128 |
| Neuroticism | 0.228 | 0.019 | 11.993 | <0 .001 | 0.530 | 0.443 | 0.617 | 0.141 | 0.020 | 7.069 | <0 .001 | 0.344 | 0.248 | 0.439 | 0.145 | 0.018 | 8.077 | <0 .001 | 0.402 | 0.304 | 0.500 |
| Overall Model Test | ||||||||
|---|---|---|---|---|---|---|---|---|
| Model | R | R² | adj. R² | F | df1 | df2 | p | |
| Depression | ||||||||
| Model fit measures | ||||||||
| 1 | 0.495 | 0.245 | 0.216 | 8.45 | 15 | 391 | < 0.001 | |
| 2 | 0.732 | 0.537 | 0.514 | 23.58 | 19 | 387 | < 0.001 | |
| Comparison | ||||||||
| Model | ΔR2 | F | df1 | df2 | p | |||
| 1 | 2 | 0.292 | 60.9 | 4 | 387 | < 0.001 | ||
| Anxiety | ||||||||
| Model fit measures | ||||||||
| 1 | 0.491 | 0.241 | 0.212 | 8.29 | 15 | 391 | < 0.001 | |
| 2 | 0.664 | 0.441 | 0.413 | 16.04 | 19 | 387 | < 0.001 | |
| Comparison | ||||||||
| 1 | 2 | 0.199 | 34.5 | 4 | 387 | < 0.001 | ||
| Stress | ||||||||
| Model fit measures | ||||||||
| 1 | 0.408 | 0.166 | 0.134 | 5.2 | 15 | 391 | < 0.001 | |
| 2 | 0.642 | 0.412 | 0.383 | 14.27 | 19 | 387 | < 0.001 | |
| Comparison | ||||||||
| 1 | 2 | 0.246 | 40.5 | 4 | 387 | < 0.001 | ||
| Moderator | Interaction | Estimate | SE | Lower | Upper | β | z | p | |
| neuroticism | neuroticism:individual_impact ⇒ family_climate | −0.003 | 0.004 | −0.010 | 0.004 | −0.036 | −0.781 | 0.435 | |
| neuroticism:individual_impact ⇒ depression | 0.018 | 0.007 | 0.004 | 0.031 | 0.093 | 2.538 | 0.011 | ||
| neuroticism:family_climate ⇒ depression | 0.007 | 0.006 | −0.005 | 0.018 | 0.110 | 1.174 | 0.240 | ||
| Moderator levels | 95% C.I. (a) | ||||||||
| neuroticism | Type | Effect | Estimate | SE | Lower | Upper | β | z | p |
| Mean-1·SD | Indirect | individual_impact ⇒ family_climate ⇒ depression | 0.075 | 0.033 | 0.010 | 0.140 | 0.024 | 2.250 | 0.025 |
| Mean-1·SD | Component | individual_impact ⇒ family_climate | −0.201 | 0.075 | −0.347 | −0.055 | −0.155 | −2.700 | 0.007 |
| Mean-1·SD | family_climate ⇒ depression | −0.372 | 0.092 | −0.552 | −0.193 | −0.155 | −4.070 | <0.001 | |
| Mean-1·SD | Direct | individual_impact ⇒ depression | 0.253 | 0.139 | −0.020 | 0.525 | 0.081 | 1.820 | 0.069 |
| Mean-1·SD | Total | individual_impact ⇒ depression | 0.341 | 0.139 | 0.068 | 0.614 | 0.110 | 2.450 | 0.014 |
| Mean | Indirect | individual_impact ⇒ family_climate ⇒ depression | 0.066 | 0.028 | 0.010 | 0.121 | 0.021 | 2.310 | 0.021 |
| Mean | Component | individual_impact ⇒ family_climate | −0.244 | 0.065 | −0.371 | −0.116 | −0.188 | −3.740 | <0.001 |
| Mean | family_climate ⇒ depression | −0.270 | 0.092 | −0.449 | −0.090 | −0.113 | −2.950 | 0.003 | |
| Mean | Direct | individual_impact ⇒ depression | 0.516 | 0.123 | 0.276 | 0.756 | 0.166 | 4.210 | <0.001 |
| Mean | Total | individual_impact ⇒ depression | 0.587 | 0.122 | 0.348 | 0.826 | 0.189 | 4.820 | <0.001 |
| Mean+1·SD | Indirect | individual_impact ⇒ family_climate ⇒ depression | 0.048 | 0.031 | −0.012 | 0.108 | 0.015 | 1.560 | 0.118 |
| Mean+1·SD | Component | individual_impact ⇒ family_climate | −0.286 | 0.094 | −0.471 | −0.101 | −0.220 | −3.030 | 0.002 |
| Mean+1·SD | family_climate ⇒ depression | −0.167 | 0.092 | −0.347 | 0.012 | −0.070 | −1.830 | 0.068 | |
| Mean+1·SD | Direct | individual_impact ⇒ depression | 0.780 | 0.176 | 0.434 | 1.125 | 0.251 | 4.420 | <0.001 |
| Mean+1·SD | Total | individual_impact ⇒ depression | 0.833 | 0.176 | 0.488 | 1.179 | 0.268 | 4.720 | <0.001 |
| Moderator | Interaction | Estimate | SE | Lower | Upper | β | z | p | |
| neuroticism | neuroticism:individual_impact ⇒ family_climate | −0.003 | 0.004 | −0.010 | 0.004 | −0.036 | −0.781 | 0.435 | |
| neuroticism:individual_impact ⇒ anxiety | 0.025 | 0.007 | 0.011 | 0.039 | 0.138 | 3.389 | <0.001 | ||
| neuroticism:family_climate ⇒ anxiety | −0.007 | 0.006 | −0.020 | 0.005 | −0.124 | −1.195 | 0.232 | ||
| Moderator levels | 95% C.I. (a) | ||||||||
| neuroticism | Type | Effect | Estimate | SE | Lower | Upper | β | z | p |
| Mean-1·SD | Indirect | individual_impact ⇒ family_climate ⇒ anxiety | 0.044 | 0.026 | −0.006 | 0.094 | 0.015 | 1.740 | 0.082 |
| Mean-1·SD | Component | individual_impact ⇒ family_climate | −0.201 | 0.075 | −0.347 | −0.055 | −0.155 | −2.700 | 0.007 |
| Mean-1·SD | family_climate ⇒ anxiety | −0.221 | 0.097 | −0.411 | −0.031 | −0.097 | −2.280 | 0.023 | |
| Mean-1·SD | Direct | individual_impact ⇒ anxiety | 0.307 | 0.147 | 0.019 | 0.596 | 0.104 | 2.090 | 0.037 |
| Mean-1·SD | Total | individual_impact ⇒ anxiety | 0.338 | 0.149 | 0.046 | 0.629 | 0.114 | 2.270 | 0.023 |
| Mean | Indirect | individual_impact ⇒ family_climate ⇒ anxiety | 0.081 | 0.032 | 0.018 | 0.144 | 0.027 | 2.520 | 0.012 |
| Mean | Component | individual_impact ⇒ family_climate | −0.244 | 0.065 | −0.371 | −0.116 | −0.188 | −3.740 | <0.001 |
| Mean | family_climate ⇒ anxiety | −0.332 | 0.097 | −0.522 | −0.142 | −0.145 | −3.420 | <0.001 | |
| Mean | Direct | individual_impact ⇒ anxiety | 0.680 | 0.130 | 0.425 | 0.934 | 0.229 | 5.240 | <0.001 |
| Mean | Total | individual_impact ⇒ anxiety | 0.755 | 0.130 | 0.500 | 1.010 | 0.254 | 5.810 | <0.001 |
| Mean+1·SD | Indirect | individual_impact ⇒ family_climate ⇒ anxiety | 0.127 | 0.050 | 0.028 | 0.225 | 0.042 | 2.530 | 0.012 |
| Mean+1·SD | Component | individual_impact ⇒ family_climate | −0.286 | 0.094 | −0.471 | −0.101 | −0.220 | −3.030 | 0.002 |
| Mean+1·SD | family_climate ⇒ anxiety | −0.442 | 0.097 | −0.632 | −0.252 | −0.192 | −4.560 | <0001 | |
| Mean+1·SD | Direct | individual_impact ⇒ anxiety | 1.052 | 0.187 | 0.686 | 1.418 | 0.352 | 5.630 | <0.001 |
| Mean+1·SD | Total | individual_impact ⇒ anxiety | 1.172 | 0.188 | 0.803 | 1.541 | 0.394 | 6.230 | <0.001 |
| Moderator | Interaction | Estimate | SE | Lower | Upper | β | z | p | |
| neuroticism | neuroticism:individual_impact ⇒ family_climate | −0.003 | 0.004 | −0.010 | 0.004 | −0.036 | −0.781 | 0.435 | |
| neuroticism:individual_impact ⇒ stress | 0.009 | 0.007 | −0.004 | 0.022 | 0.056 | 1.369 | 0.171 | ||
| neuroticism:family_climate ⇒ stress | −0.008 | 0.006 | −0.019 | 0.003 | −0.149 | −1.422 | 0.155 | ||
| Moderator levels | 95% C.I. (a) | ||||||||
| neuroticism | Type | Effect | Estimate | SE | Lower | Upper | Β | z | p |
| Mean-1·SD | Indirect | individual_impact ⇒ family_climate ⇒ stress | 0.004 | 0.017 | −0.030 | 0.038 | 0.001 | 0.207 | 0.836 |
| Mean-1·SD | Component | individual_impact ⇒ family_climate | −0.201 | 0.075 | −0.347 | −0.055 | −0.155 | −2.698 | 0.007 |
| Mean-1·SD | family_climate ⇒ stress | −0.018 | 0.086 | −0.186 | 0.150 | −0.009 | −0.208 | 0.835 | |
| Mean-1·SD | Direct | individual_impact ⇒ stress | 0.577 | 0.130 | 0.322 | 0.832 | 0.222 | 4.430 | <0.001 |
| Mean-1·SD | Total | individual_impact ⇒ stress | 0.566 | 0.130 | 0.311 | 0.820 | 0.217 | 4.354 | <0.001 |
| Mean | Indirect | individual_impact ⇒ family_climate ⇒ stress | 0.033 | 0.023 | −0.012 | 0.077 | 0.013 | 1.443 | 0.149 |
| Mean | Component | individual_impact ⇒ family_climate | −0.244 | 0.065 | −0.371 | −0.116 | −0.188 | −3.736 | <0.001 |
| Mean | family_climate ⇒ stress | −0.134 | 0.086 | −0.302 | 0.034 | −0.067 | −1.565 | 0.118 | |
| Mean | Direct | individual_impact ⇒ stress | 0.710 | 0.115 | 0.485 | 0.935 | 0.273 | 6.185 | <0.001 |
| Mean | Total | individual_impact ⇒ stress | 0.737 | 0.114 | 0.514 | 0.960 | 0.283 | 6.481 | <0.001 |
| Mean+1·SD | Indirect | individual_impact ⇒ family_climate ⇒ stress | 0.072 | 0.034 | 0.005 | 0.139 | 0.027 | 2.104 | 0.035 |
| Mean+1·SD | Component | individual_impact ⇒ family_climate | −0.286 | 0.094 | −0.471 | −0.101 | −0.220 | −3.032 | 0.002 |
| Mean+1·SD | family_climate ⇒ stress | −0.251 | 0.086 | −0.419 | −0.083 | −0.124 | −2.922 | 0.003 | |
| Mean+1·SD | Direct | individual_impact ⇒ stress | 0.843 | 0.165 | 0.520 | 1.167 | 0.323 | 5.105 | <0.001 |
| Mean+1·SD | Total | individual_impact ⇒ stress | 0.908 | 0.165 | 0.586 | 1.231 | 0.349 | 5.518 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miscioscia, M.; Poli, M.; Gubello, A.; Simonelli, A.; Gatta, M.; Gato, J.; Rigo, P. Influence of the COVID-19 Pandemic on Italian LGBT+ Young Adults’ Mental Health: The Role of Neuroticism and Family Climate. Int. J. Environ. Res. Public Health 2022, 19, 15795. https://doi.org/10.3390/ijerph192315795
Miscioscia M, Poli M, Gubello A, Simonelli A, Gatta M, Gato J, Rigo P. Influence of the COVID-19 Pandemic on Italian LGBT+ Young Adults’ Mental Health: The Role of Neuroticism and Family Climate. International Journal of Environmental Research and Public Health. 2022; 19(23):15795. https://doi.org/10.3390/ijerph192315795
Chicago/Turabian StyleMiscioscia, Marina, Mikael Poli, Alessio Gubello, Alessandra Simonelli, Michela Gatta, Jorge Gato, and Paola Rigo. 2022. "Influence of the COVID-19 Pandemic on Italian LGBT+ Young Adults’ Mental Health: The Role of Neuroticism and Family Climate" International Journal of Environmental Research and Public Health 19, no. 23: 15795. https://doi.org/10.3390/ijerph192315795