1. Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) emerged in late December 2019, with the epicenter in Wuhan, China, and has since infected more than 135 million people, causing over 2.9 million deaths worldwide [
1]. The COVID-19 pandemic has proven to be a serious challenge for the Romanian healthcare system, with more than 1 million infections and approximately 25,000 deaths being reported in the country at the time of writing. Comorbidities are observed in 20–30% of COVID-19 patients, while the proportion increases to 50–80% in patients with severe COVID-19 [
2]. Since the beginning of the pandemic, the effect of comorbidities has been widely discussed; however, the impact of coronavirus infection on the liver has not been well studied. Furthermore, several medications used for the treatment of COVID-19 may cause hepatotoxicity [
3].
In 2018, there was a reported incidence of 37,527 cases of chronic hepatitis C in the EU/EEA Member States [
4], with a total prevalence of 19 million cases [
5] and 71 million cases worldwide [
6]. As the global prevalence of hepatitis C virus (HCV) and SARS-CoV-2 infections are geographically variable, epidemiological data across Europe may help improve our understanding of the reciprocal impact of SARS-CoV-2 and HCV. Simultaneously, we have investigated the prevalence of COVID-19 among HCV patients who achieved cure using a sofosbuvir/velpatasvir (SOF/VEL) combination antiviral treatment in all cases. The interplay between a pre-existing liver disease and SARS-CoV-2 infection may be important for patients’ outcomes, since chronic hepatitis C is still a health burden in many European countries. Even though the exact impact of SARS-CoV-2 infection on the liver is unknown, abnormalities in liver biochemistry are typical in COVID-19 cases, arising in 15–65% of patients infected with SARS-CoV-2 [
7,
8].
In the present study, we focused on the assessment of hematological changes and liver function abnormalities, as evidenced by routine laboratory testing in patients co-infected with HCV and SARS-CoV-2, and the relationship between COVID-19 severity and progression of liver disease. We describe the possible relationship between the clinical course, laboratory findings, and outcome of 126 patients admitted in our department with documented HCV infection and COVID-19 disease.
2. Materials and Methods
We conducted a retrospective cohort study to evaluate the risk for liver impairment and all-cause mortality in COVID-19 patients with active HCV infection. We collected clinical and laboratory data using the archived records of consecutive patients with COVID-19 at the Infectious Diseases and Pulmonology Hospital, “Victor Babes” Timisoara from 1 April 2020 to 1 September 2020. Among the patients confirmed with SARS-CoV-2 infection within this time frame, we identified those cases with a documented history of HCV infection. The group of patients with HCV and SARS-CoV-2 co-infection was further divided into active and non-active HCV infection groups according to their history of hepatitis C diagnosis and treatment. Patients with liver cirrhosis were excluded from the study. An active HCV infection was defined by an HCV RNA viral load greater than 0.015 (U/L × 103). Subsequently, various clinical parameters and outcomes, such as length of hospital stay, number of intensive care unit (ICU) admissions, length of ICU stay(s), as well as routine blood parameters, including white blood cell count (WBC), red blood cell count (RBC), hemoglobin levels (Hb), platelet count (PLT), liver function tests such as alanine transaminase (ALT), aspartate transaminase (AST), alkaline phosphatase (ALP), albumin and total plasma proteins, total bilirubin, gamma-glutamyltransferase (GGT), L-lactate dehydrogenase (LDH), and prothrombin time (PT); HCV viral load, procalcitonin, C-reactive protein (CRP), and all-cause mortality were assessed and compared between those with and without active HCV infection. Serial monitoring of the laboratory profile was performed according to the clinical progress of each individual patient. Liver impairment was defined as the alteration above normal ranges for the liver function tests: ALT, AST, ALP, GGT, LDH, PT, albumin, total plasma proteins, total bilirubin.
The patients enrolled were at least 18 years old, the intensive care unit (ICU) admissions were required for a rapid progression of severe pneumonia with pulmonary infiltrates covering over 50% of the lung fields, severe dyspnea, oxygen saturation ≤ 93% despite face mask oxygen supplementation, or paCO2 > 55 mmHg in patients without chronic obstructive pulmonary disease (COPD). SARS-CoV-2 infection was confirmed by the detection of viral RNA in nasopharyngeal secretion using specific reverse-transcription polymerase chain reaction (RT-PCR) test. COVID-19 infection was further classified into three clinical forms: mild, moderate, and severe. The mild form of COVID-19 infection was defined as a low-grade fever without pneumonia. The moderate form was defined by the presence of fever and signs of non-severe pneumonia, without need for oxygen treatment. The criteria used to define the severe cases included respiratory failure requiring mechanical ventilation, a respiratory rate greater than 30/min, oxygen saturation of hemoglobin measured by pulse-oximetry (SpO
2) < 90%, coagulation disorders, failure of other organs requiring admission to the ICU, and ground-glass opacities involving more than 50% of the lungs on the chest X-ray or CT scan. The treatment scheme for all patients admitted to our clinic with COVID-19 infection included a standard association of remdesivir, dexamethasone, azithromycin antibiotic prophylaxis, and anticoagulation using enoxaparin, since studies confirmed the correlation between COVI-19 and thrombosis [
9], with adjustments being made based on patient profile.
The Local Committee of Ethics for Scientific Research of “Dr. Victor Babes” Infectious Diseases and Pulmonology Clinical Hospital Timisoara operates under art provisions 167 of Law no. 95/2006, art. 28, chapter VIII of order 904/2006 and with EU GCP Directives 2005/28/EC, International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH), and with the Declaration of Helsinki—Recommendations Guiding Medical Doctors in Biomedical Research Involving Human Subjects. The current study protocol received the ethical approval on the 10th of September 2020, with the approval number 1292.
We compared clinical and laboratory data of COVID-19 patients with and without active HCV infection using the IBM SPSS v.26 statistical software. The χ2 test and Fisher’s exact test were used for categorical variables and Student’s t-test or Mann–Whitney U-test for continuous variables. The independent risk factors associated with the COVID-19-related clinical outcomes of liver impairment and mortality were identified using a logistic regression model. Risk factors are reported as odds ratios (ORs) with 95% confidence intervals (CIs). The significance threshold was set for α = 0.05.
3. Results
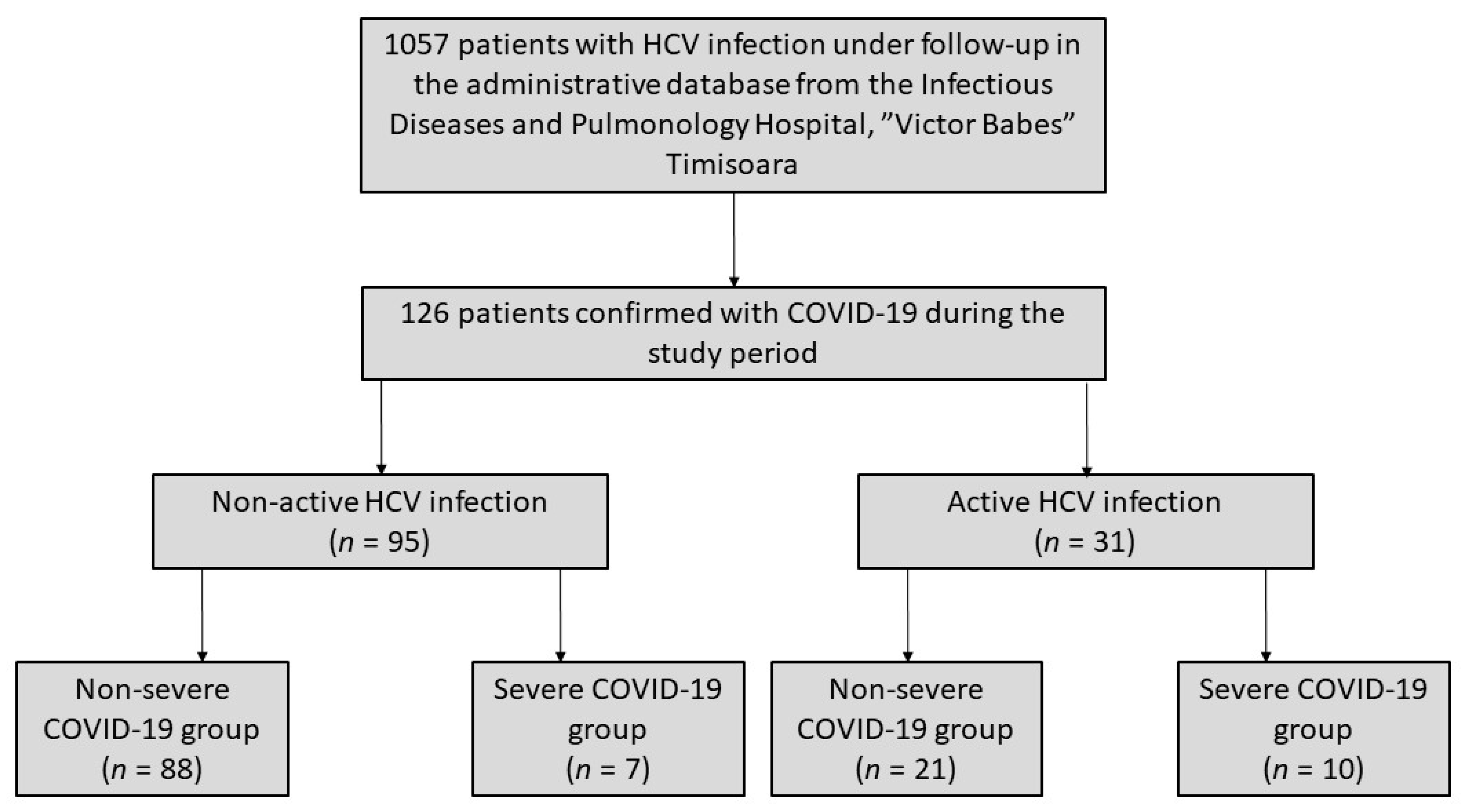
Among 1057 patients infected with HCV that were under follow-up in our clinic, 126 (11.9%) were confirmed with COVID-19 between 1 April 2020 and 1 September 2020. Of these, 95 patients (75.4%) were under treatment with the SOF/VEL scheme or achieved sustained virologic response (SVR), while in the other 31 (24.6%), we found active HCV replication. In the group of patients with a non-active HCV infection, 88 (92.6%) had a mild or moderate form of COVID-19 infection, while seven patients (7.4%) presented a severe form of disease. In the group of patients with active HCV infection, 21 (67.7%) had a mild or moderate form of COVID-19, while 10 (32.3%) presented with severe COVID-19 infection (
Figure 1).
When comparing the proportion of severe COVID-19 cases in the active and non-active HCV infection groups, we found a statistically significant higher prevalence in the active HCV group (32.2 vs. 7.3%, χ2 = 12.40, p-value = 0.0004).
The baseline demographics of the study population are shown in
Table 1. The majority of patients in the active HCV group were male (58.1 vs. 35.7%,
p-value < 0.0001) and belonged to the 41–60 years age group (51.6 vs. 30.6%,
p-value < 0.0001). There was no difference between groups in the prevalence of reported comorbidities. The patients in the active HCV group experienced more signs and symptoms, fatigue being significantly more prevalent in the active HCV group (83.8 vs. 64.2%,
p-value < 0.0001), followed by myalgia (54.8 vs. 34.7%,
p-value < 0.0001), and fever (87.0 vs. 72.6%,
p-value < 0.0001). Oxygen saturation levels on admission were most commonly above 95% in the non-active HCV infection group (83.1 vs. 45.1%
p-value < 0.0001), while in the active HCV group, we found significantly higher proportions of patients with oxygen saturation levels between 90–95% and below 90% (19.3 vs. 7.3%,
p-value < 0.0001 and 35.4 vs. 9.4%,
p-value < 0.0001, respectively). A lung involvement consisting in > 40% of the lung parenchyma affected by the SARS-CoV-2 infection on chest computed tomography (CT) was significantly more prevalent in patients with active HCV infection (32.2 vs. 7.3%,
p-value < 0.0001).
Table 2 compares the clinical outcomes between non-active and active HCV infection groups. The rate of hospitalization and length of stay were significantly higher in the active HCV group (61.2 vs. 40.0%,
p-value < 0.0001 and 28 vs. 21 days,
p-value = 0.0142, respectively). Among the patients hospitalized for COVID-19, 10 patients (52.6%) in the active HCV group and seven patients (18.4%) in the non-active HCV group were admitted to the ICU (
p-value < 0.0001). The proportion of patients requiring mechanical ventilation (26.3 vs. 13.1%,
p-value = 0.0007) and all-cause mortality were higher in the active HCV group (48.3 vs. 11.5%,
p-value < 0.0001).
A multivariate analysis (
Table 3) was conducted to assess the risk factors for liver impairment and all-cause mortality in COVID-19 patients with chronic hepatitis C. Age over 60 years (OR = 2.51, 95%CI 1.43–3.02), male gender (OR = 2.36, 95%CI 1.41–3.15), ALT (OR = 3.17, 95%CI 1.61–3.98), procalcitonin (OR = 2.88, 95%CI 1.45–2.95) levels, and HCV viral load were all independent risk factors for liver impairment. Furthermore, an age over 60 years (OR = 8.27, 95%CI 5.14–13.5), male gender (OR = 1.66, 95%CI 1.27–2.20), ALT level (OR = 1.45, 95%CI 1.18–2.19), and HCV viral load (OR = 2.46, 95%CI 1.17–3.56) were also independent risk factors for all-cause mortality.
Significant changes in blood parameters (
Table 4.) were observed in both study groups, with mean WBC (
p < 0.0001), ALT (
p < 0.0001), AST (
p < 0.0001), ALP (
p = 0.012), LDH (
p < 0.0001), PT (
p < 0.0001), procalcitonin (
p < 0.0001), CRP (
p < 0.0001), and HCV viral load (
p < 0.0001) being significantly higher and platelet count significantly lower (
p < 0.0001) in COVID-19 patients with active HCV infection.
4. Discussion
Previous studies [
10] investigated the changes in liver function in patients with COVID-19, assessing the routine blood parameters in liver function tests. Partially their observations were consistent with our findings, showing significant increases in ALT, AST, LDH, CRP, and coagulation tests in severe COVID-19 cases and a decrease in albumin, when compared to mild cases of infection. However, these findings did not differ when compared to hospitalized patients with community-acquired pneumonia. Moreover, no liver parameter demonstrated any significant relationship as a risk factor with severe COVID-19 cases and mortality, since only old age and the neutrophil–lymphocyte ratio (NLR) were identified as independent risk factors. On the other hand, our study focused only on patients with chronic HCV infection, thus, the higher likelihood of worsened liver function compared to the general population. Other larger studies [
11] demonstrated that impaired liver function is a prognostic factor for poor outcomes in patients with COVID-19, consequently increasing the length of hospital stay, similar to our observations. The disease severity in patients with chronic liver dysfunction was closely associated with older age, male gender, and high body mass index (BMI). The authors assumed that the liver injury may have been actually induced by hepatotoxic effect of drugs used to treat the SARS-CoV-2 infection.
Another study analyzed the possible pathologic mechanisms standing behind impaired liver function in patients with COVID-19 [
12]. However, there were no conclusive arguments and data to clarify whether these changes may have been a result of the direct action of SARS-CoV-2 on the liver. It was reported that patients with chronic liver disease are more likely to die by acute-on-chronic liver failure and respiratory failure, while suffering from COVID-19. In the same direction, Grove J. et al. [
13] studied the molecular mechanisms involved in the coronaviruses hepatotropism, which was earlier hypothesized as hepatic injury and inflammation being able to potentiate SARS-CoV-2 hepatotropism by modulating viral receptor expression, since the angiotensin-converting enzyme 2 (ACE2) receptor was earlier identified as an interferon-inducible gene in human respiratory epithelia [
14]. Additionally, the SARS-CoV receptor-binding domain (RBD) binds to the ACE2 receptors allowing the virus to enter targeted cells [
15], while also inhibiting the ACE2 enzyme, which typically protects the lungs from damage [
16]. Since ACE2 receptors are found in biliary and hepatic epithelial cells, the liver appears to be vulnerable to SARS-CoV-2 infection [
17]. The study described how the high-density lipoprotein scavenger receptor B type 1 (SR-B1) helps facilitate ACE2-dependent coronavirus attachment in vitro, reminiscent of HCV infection.
The possibility of drug-induced hepatotoxicity was also taken into consideration in our research. Other studies explored this hypothesis [
18], showing that patients with HCV infection were more likely to experience drug-induced liver damage, particularly when receiving highly active antiretroviral therapy [
19]. Thus, all hospitalized patients in our cohort received a treatment scheme consisting of lopinavir/ritonavir and darunavir, based on the existing national guidelines. Inconsistently, 103 (81.7%) patients also received antibiotic therapy comprising of azithromycin, moxifloxacin, vancomycin, meropenem, ceftriaxone, or levofloxacin, according to the alleged bacterial pathogens involved, therapies that may have potential hepatotoxic consequences [
20].
Our study is limited by the retrospective cohort study design, since there were multiple healthcare workers engaged in patient care; therefore, measuring risk factors and effects through the database is likely to be less reliable and accurate when compared to a prospective cohort design where these factors can be carefully controlled.
Finally, the current study brings novel findings and conclusions regarding patients with active and non-active chronic HCV infection without liver cirrhosis, who are subsequently infected with the SARS-CoV-2 virus, since this topic has not been fully studied to this date. Various studies [
21,
22] observed higher mortality rates in COVID-19 patients with liver cirrhosis caused by chronic hepatitis B and C, although a recent meta-analysis [
23] concluded that chronic liver disease, including chronic HCV infection, appears to have a small impact on the COVID-19 progression to a severe form of disease, findings that are inconsistent with our observations.
5. Conclusions
In conclusion, active HCV infection was associated with more severe disease and higher mortality in patients co-infected with SARS-CoV-2, HCV viral load being an independent risk factor for all-cause mortality and liver impairment. The severity of liver impairment was associated with poor clinical outcomes in COVID-19 patients. Further research is required to confirm our findings in prospective studies and larger samples. Our results suggest that close monitoring and careful treatment for active-HCV patients with COVID-19 are needed to avoid health deterioration and fatal outcome.
Author Contributions
Conceptualization, B.C., M.T., and I.M.; methodology, I.M., I.V., and S.P.; software, F.B.; validation, I.M., B.C., and M.T.; formal analysis, F.B., E.B., and S.P.; investigation, S.P., E.B., and I.M.; resources, I.M.; data curation, F.B. and I.V.; writing—original draft preparation, I.V., B.C., and S.F.; writing—review and editing, F.B., E.B., and S.F.; visualization, F.B. and S.P.; supervision, B.C., I.M., and M.T.; project administration, I.M. and S.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of Victor Babes Clinical Hospital for Infectious Diseases and Pulmonology in Timisoara, approved on 10 September 2020.
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
Data available on request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization (WHO). Situation Reports December 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus2019/situation-reports (accessed on 4 December 2020).
- Goyal, P.; Choi, J.J.; Pinheiro, L.C.; Schenck, E.J.; Chen, R.; Jabri, A.; Satlin, M.J.; Campion, T.R., Jr.; Nahid, M.; Ringel, J.B.; et al. Clinical characteristics of Covid-19 in New York city. N. Engl. J. Med. 2020, 382, 2372–2374. [Google Scholar] [CrossRef]
- Vitiello, A.; La Porta, R.; D’Aiuto, V.; Ferrara, F. The risks of liver injury in COVID-19 patients and pharmacological management to reduce or prevent the damage induced. Egypt. Liver J. 2021, 11, 1–6. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Hepatitis C. In Annual Epidemiological Report for 2018; ECDC: Stockholm, Sweden, 2020. [Google Scholar]
- Negro, F. Epidemiology of hepatitis C in Europe. Dig. Liver Dis. 2014, 46, S158–S164. [Google Scholar] [CrossRef]
- Matičič, M.; Lombardi, A.; Mondelli, M.U.; Colombo, M. Elimination of hepatitis C in Europe: Can WHO targets be achieved? Clin. Microbiol. Infect. 2020, 26, 818–823. [Google Scholar] [CrossRef]
- Fu, Y.; Zhu, R.; Bai, T.; Han, P.; He, Q.; Jing, M.; Xiong, X.; Zhao, X.; Quan, R.; Chen, C.; et al. Clinical features of COVID-19-infected patients with elevated liver biochemistries: A multicenter, retrospective study. Hepatology 2020. [Google Scholar] [CrossRef] [PubMed]
- Hundt, M.A.; Deng, Y.; Ciarleglio, M.M.; Nathanson, M.H.; Lim, J.K. Abnormal Liver Tests in COVID-19: A Retrospective Observa-tional Cohort Study of 1,827 Patients in a Major US Hospital Network. Hepatology 2020, 72, 1169–1176. [Google Scholar] [CrossRef]
- Słomka, A.; Kowalewski, M.; Żekanowska, E. Coronavirus Disease 2019 (COVID–19): A Short Review on Hematological Manifestations. Pathogens 2020, 9, 493. [Google Scholar] [CrossRef]
- Zhang, Y.; Zheng, L.; Liu, L.; Zhao, M.; Xiao, J.; Zhao, Q. Liver impairment in COVID-19 patients: A retrospective analysis of 115 cases from a single centre in Wuhan city, China. Liver Int. 2020, 40, 2095–2103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cichoż-Lach, H.; Michalak, A. Liver injury in the era of COVID-19. World J. Gastroenterol. 2021, 27, 377–390. [Google Scholar] [CrossRef]
- Marjot, T.; Webb, G.J.; Barritt, A.S.; Moon, A.M.; Stamataki, Z.; Wong, V.W.; Barnes, E. COVID-19 and liver disease: Mechanistic and clinical perspectives. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 348–364. [Google Scholar] [CrossRef] [PubMed]
- Grove, J.; Huby, T.; Stamataki, Z.; Vanwolleghem, T.; Meuleman, P.; Farquhar, M.; Schwarz, A.; Moreau, M.; Owen, J.S.; Leroux-Roels, G.; et al. Scavenger Receptor BI and BII Expression Levels Modulate Hepatitis C Virus Infectivity. J. Virol. 2007, 81, 3162–3169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziegler, C.G.; Allon, S.J.; Nyquist, S.K.; Mbano, I.M.; Miao, V.N.; Tzouanas, C.N.; Cao, Y.; Yousif, A.S.; Bals, J.; Hauser, B.M.; et al. SARS-CoV-2 receptor ACE2 is an interferon-stimulated gene in human airway epithelial cells and is detected in specific cell subsets across tissues. Cell 2020, 181, 1016–1035. [Google Scholar] [CrossRef]
- Rabi, F.A.; Al Zoubi, M.S.; Kasasbeh, G.A.; Salameh, D.M.; Al-Nasser, A.D. SARS-CoV-2 and Coronavirus Disease 2019: What We Know So Far. Pathogens 2020, 9, 231. [Google Scholar] [CrossRef] [PubMed]
- Neerukonda, S.N.; Katneni, U. A Review on SARS-CoV-2 Virology, Pathophysiology, Animal Models, and Anti-Viral Interventions. Pathogens 2020, 9, 426. [Google Scholar] [CrossRef] [PubMed]
- Chai, X.; Hu, L.; Zhang, Y.; Han, W. Specific ACE2 expression in cholangiocytes may cause liver damage after 2019-nCoV infec-tion. bioRxiv. 2020. [Google Scholar] [CrossRef] [Green Version]
- Boeckmans, J.; Rodrigues, R.M.; Demuyser, T.; Piérard, D.; Vanhaecke, T.; Rogiers, V. COVID-19 and drug-induced liver injury: A problem of plenty or a petty point? Arch. Toxicol. 2020, 94, 1367–1369. [Google Scholar] [CrossRef] [Green Version]
- Naidoo, K.; Hassan-Moosa, R.; Mlotshwa, P.; Yende-Zuma, N.; Govender, D.; Padayatchi, N.; Abdool-Karim, S.S.S. High Rates of Drug-induced Liver Injury in People Living with HIV Coinfected With Tuberculosis (TB) Irrespective of Antiretroviral Therapy Timing During Antituberculosis Treatment: Results From the Starting Antiretroviral Therapy at Three Points in TB Trial. Clin. Infect. Dis. 2020, 70, 2675–2682. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Liu, J.; Lu, M.; Yang, D.; Zheng, X. Liver injury during highly pathogenic human coronavirus infections. Liver Int. 2020, 40, 998–1004. [Google Scholar] [CrossRef] [Green Version]
- Moon, A.M.; Webb, G.J.; Aloman, C.; Armstrong, M.J.; Cargill, T.; Dhanasekaran, R.; Genescà, J.; Gill, U.S.; James, T.W.; Jones, P.D.; et al. High mortality rates for SARS-CoV-2 infection in patients with pre-existing chronic liver disease and cirrhosis: Preliminary results from an international registry. J. Hepatol. 2020, 73, 705–708. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Garcia-Tsao, G.; Biggins, S.W.; Kamath, P.S.; Wong, F.; McGeorge, S.; Shaw, J.; Pearson, M.; Chew, M.; Fagan, A.; et al. Comparison of mortality risk in patients with cirrhosis and COVID-19 compared with patients with cirrhosis alone and COVID-19 alone: Multicentre matched cohort. Gut 2021, 70, 531–536. [Google Scholar] [CrossRef]
- Lippi, G.; de Oliveira, M.H.S.; Henry, B.M. Chronic liver disease is not associated with severity or mortality in Coronavirus dis-ease 2019 (COVID-19): A pooled analysis. Eur. J. Gastroenterol. Hepatol. 2021, 33, 114–115. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 ,
, 


{kind=link}