
Measuring Time-Varying Effective Reproduction Numbers for COVID-19 and Their Relationship with Movement Control Order in Malaysia

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
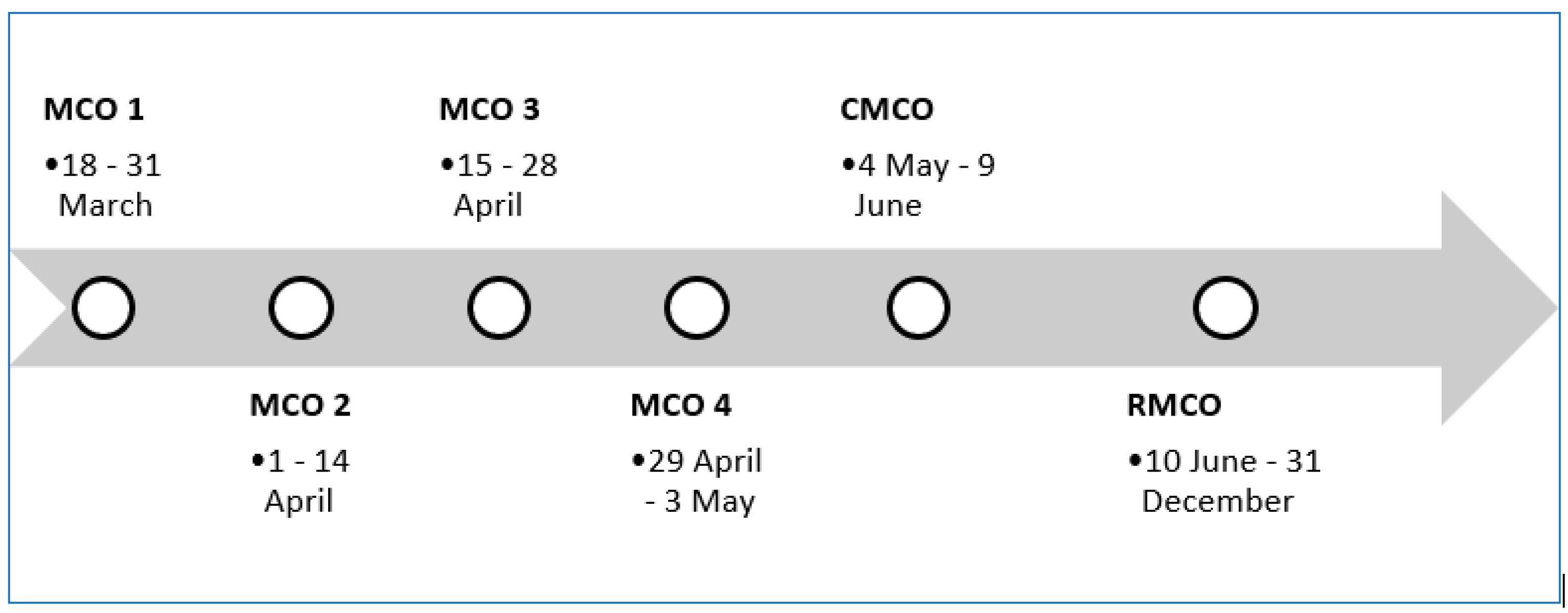
1.1. Movement Control Orders (MCOs) in Malaysia
1.2. Reproduction Number (Rt) and COVID-19
2. Materials and Methods
2.1. Source of COVID-19 Data and Variables
2.2. MCOs
2.3. Estimating Rt
3. Results
4. Discussion
Main Results
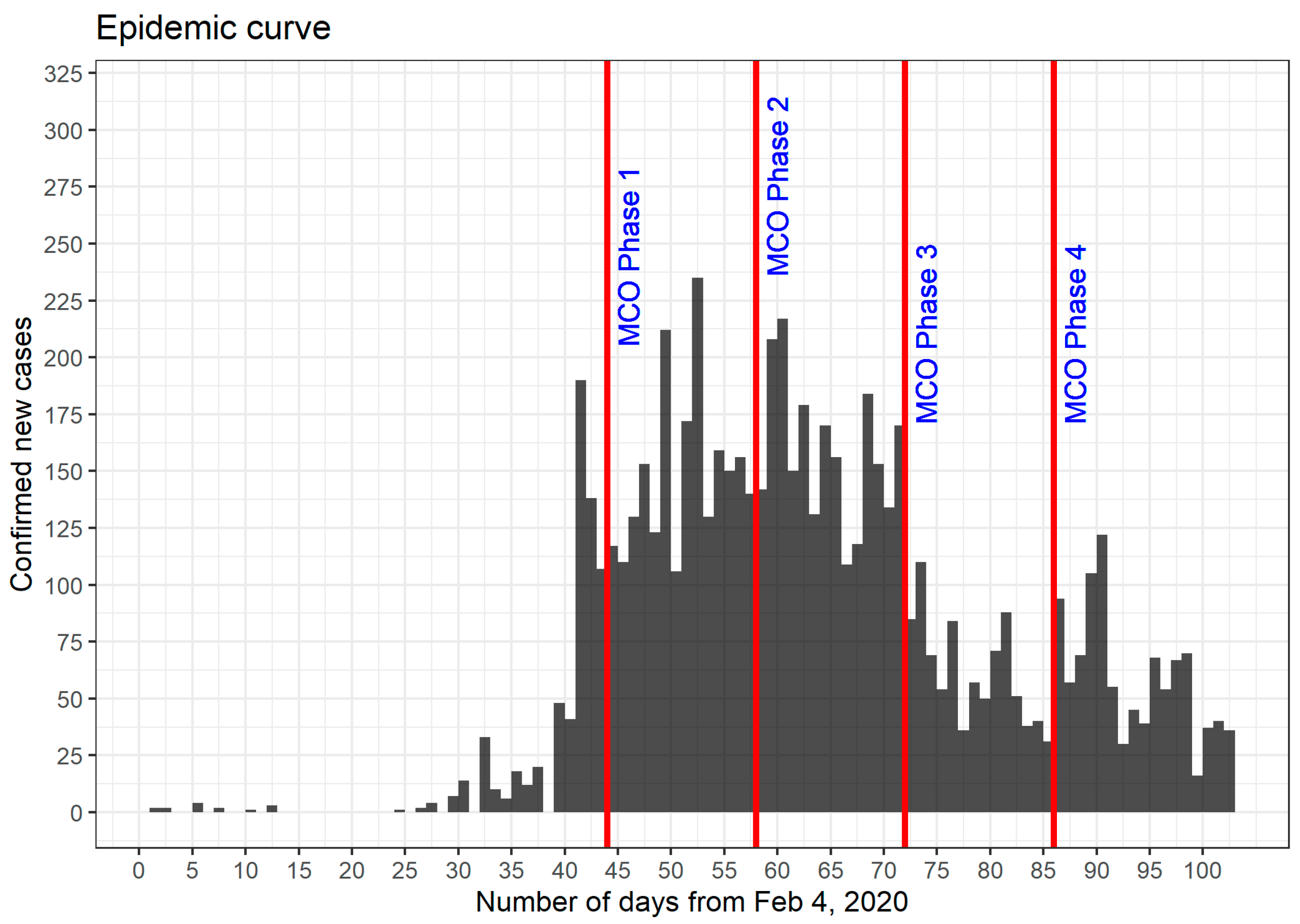
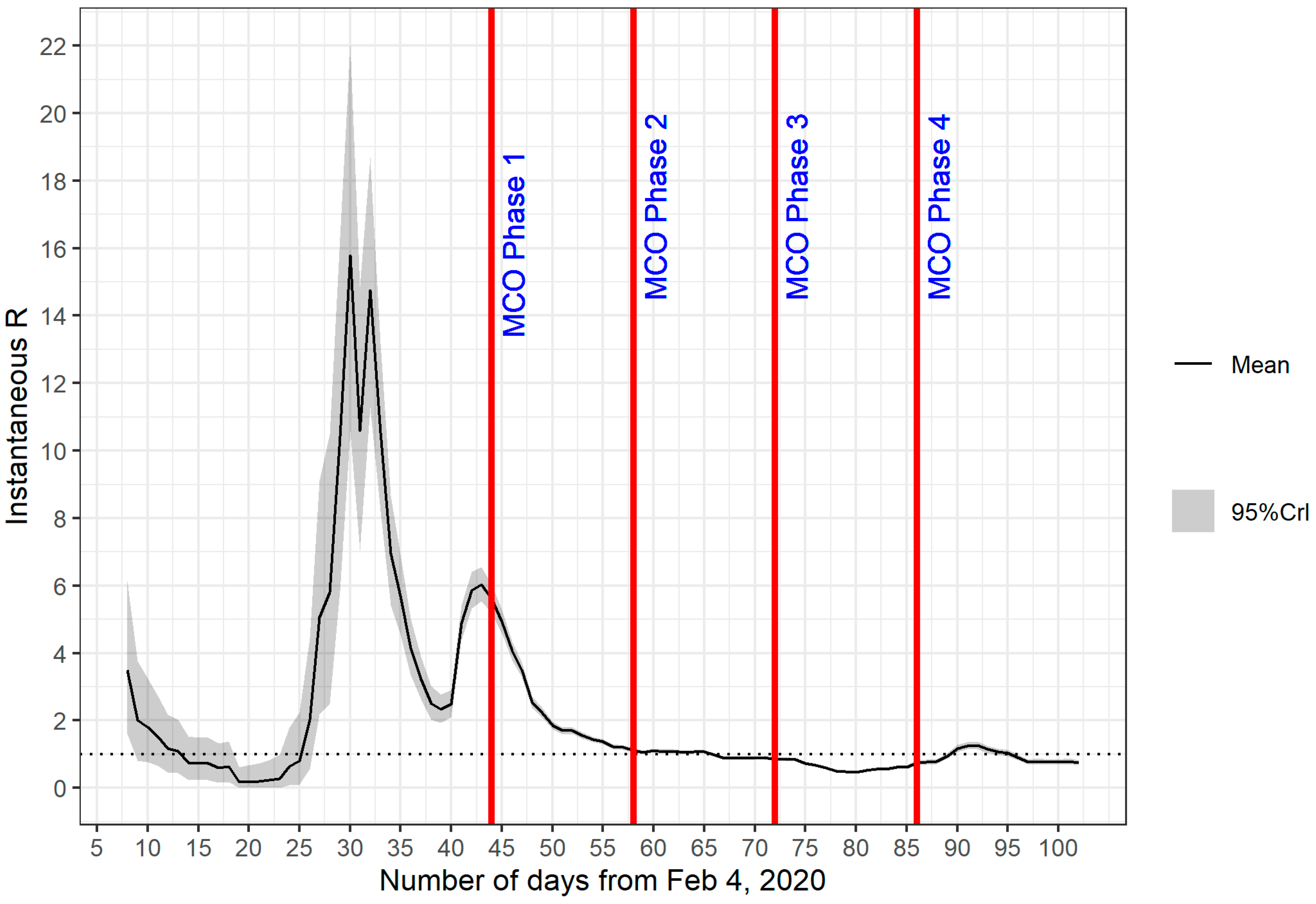
- The overall trend of Rt values do correspond with the timeline of the pandemic and the level of strict measures imposed during each phase of the MCO. The Rt values peaked around day 43, which was shortly before the start of MCO 1. A marked decline in Rt values was observed during MCO 1, and the reduction in transmissibility is reflected in a reduction in the rate of increase in daily cases. Thus, we can say that measures taken during MCO 1 were successful in taming the exponential growth of the number of infections. The Rt values started to fall below the threshold value of 1 during MCO 2, at which time the number of daily cases began to show a downward trend. Rt values remained below 1 throughout MCO 3. The relaxation of certain restrictions during MCO 3 and MCO 4 might have allowed a few spikes of confirmed cases and this is indicated by a slight increase in Rt values, but the Rt values remained stable and hovered around 1 and slightly below that.
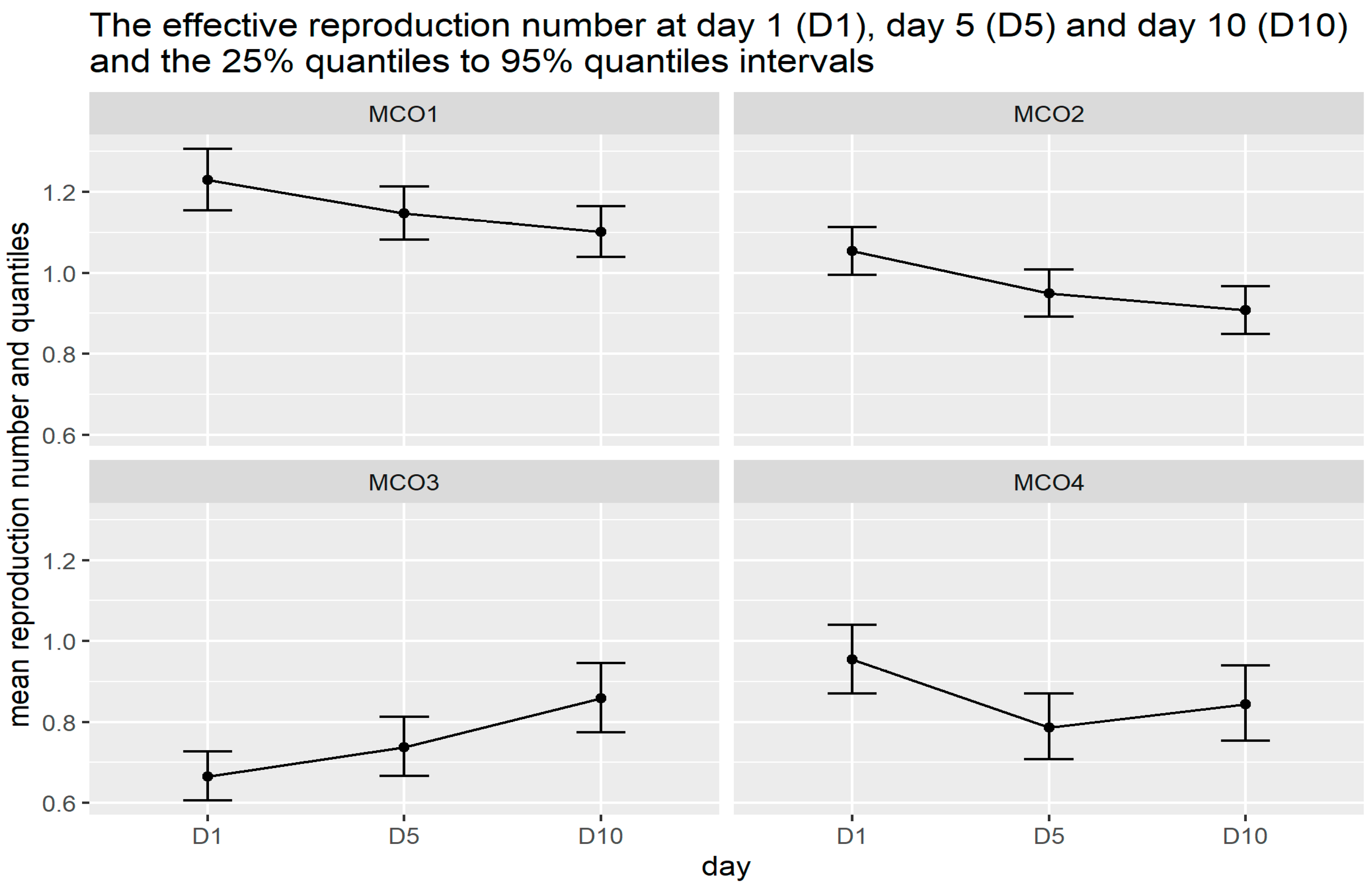
- The instantaneous mean Rt values computed for day 1, day 5 and day 10 of each phase of the MCO provide further insight into the suitability of Rt values as a quantifiable indicator to the impact of each MCO phase. From day 1 to day 10 of MCO 1, the instantaneous mean Rt reduces progressively and monotonically and this behaviour persists until day 10 of MCO 2. The continuous decrease in the mean Rt is a reflection of the strict measures imposed during MCO 1 and MCO 2. The impact of strict MCOs managed to bring down the mean Rt value from 1.23 to below 1 in about three weeks where at this level of Rt, the spread of infection is expected to be under control. The relaxation of the level of restrictions during MCO 3 and MCO 4 is also reflected in the instantaneous mean Rt, where a steady rise of the values is picked during MCO 3.
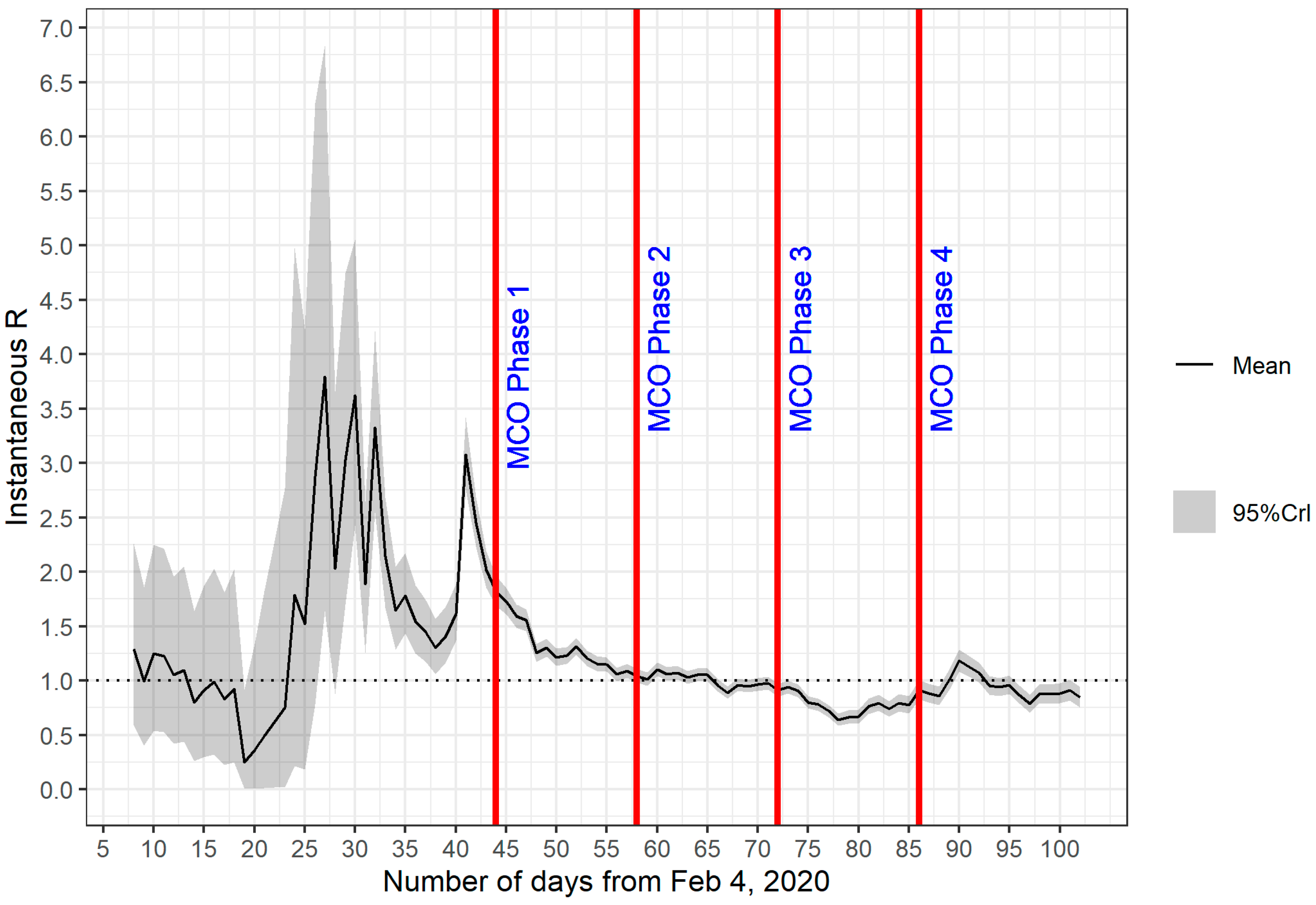
- Sensitivity of Rt values with respect to the choice of parameter values. Our results reveal the sensitivity of Rt values with respect to the choice of parameter values, namely, the mean and SD. This is particularly a concern, especially at the start of the pandemic where two significant peaks of Rt values were observed. A change in mean and SD values modified the profile of these peaks rather abruptly. Our hypothesis is that the sensitivity is due to the small sample size problem where data are insufficient to capture the essential features of the dynamical system. This hypothesis is supported further by the wider 95% percentiles for values observed on day 1 until day 45. Although reasons exist to believe that these peaks represent the relevant historical events of the pandemic (peak 1 can be associated with the start of the second wave of the pandemic in Malaysia that started around 27 February 2020 (day 23), whereas peak 2 can be tied up with the wave of infection originated from a mass gathering at Sri Petaling, Kuala Lumpur, which took place between 27 February 2020 and 1 March 2020), the accuracy of computed Rt values and the time they occurred should be investigated further.
- Sensitivity to outliers. In the presence of outliers, the instantaneous mean Rt values can be affected. This is observed in our analyses of the mean values during MCO 3 and MCO 4 and the associated timeline of the pandemic in Malaysia. The outlier is a cluster of cases involving students returning from Temboro, Magetan, Indonesia which is not a contributing factor to the community transmission during MCO 3. During the first 10 days of MCO 3, a steady increase in the instantaneous mean Rt values was detected, peaked around the first day of MCO 4, and then decreased to steady values between 0.8 and 0.9. It is possible that the rise of cases may also be due to the relaxation of certain measures during MCO 3, however, the rising trend does not persist in MCO 4. This gives the indication that the effects of outliers on Rt are possibly short-lived and do not contribute significantly to the baseline value associated with community transmission that is directly impacted by MCO measures. This supposition is further strengthened by the fact that the 95% percentile of the instantaneous mean Rt remain mostly below the threshold value of 1 throughout MCO 3 and MCO 4.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koya, Z. Movement Control: Offenders Face RM 1k Fine, Six Months’ Jail or Both. Star 2020. Available online: https://www.thestar.com.my/news/nation/2020/03/18/movement-control-offenders-face-rm1k-fine-six-months039-jail-or-both (accessed on 10 September 2020).
- Salim, N.; Chan, W.H.; Mansor, S.; Bazin, N.E.N.; Amaran, S.; Mohd Faudzi, A.A.; Zainal, A.; Huspi, H.S.; Hooi, E.K.J.; Shithil, S.M. COVID-19 epidemic in Malaysia: Impact of lock-down on infection dynamics. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Landau, E. No time limit for firms allowed to operate during MCO. New Straits Times 2020. Available online: https://www.thestar.com.my/news/nation/2020/04/28/companies-allowed-to-operate-during-mco-can-go-full-capacity-says-azmin (accessed on 28 April 2020).
- Landau, E. Public can travel beyond 10km radius for necessities, medical services. New Straits Times 2020. Available online: https://www.nst.com.my/news/nation/2020/04/588499/public-can-travel-beyond-10km-radius-necessities-medical-services (accessed on 28 April 2020).
- Tang, K.H.D. Movement control as an effective measure against Covid-19 spread in Malaysia: An overview. J. Public Health 2020, 1. [Google Scholar] [CrossRef]
- Gill, B.S.; Jayaraj, V.J.; Singh, S.; Ghazali, S.M.; Cheong, Y.L.; Iderus, N.H.M.; Sundram, B.M.; Bin Aris, T.; Ibrahim, H.M.; Hong, B.H.; et al. Modelling the effectiveness of epidemic control measures in preventing the transmission of COVID-19 in Malaysia. Int. J. Environ. Res. Public Health 2020, 17, 5509. [Google Scholar] [CrossRef]
- Delamater, P.L.; Street, E.J.; Leslie, T.F.; Yang, Y.T.; Jacobsen, K.H. Complexity of the basic reproduction number (R(0)). Emerg. Infect. Dis. 2019, 25, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Al Wahaibi, A.; Al Manji, A.; Al Maani, A.; Al Rawahi, B.; Al Harthy, K.; Alyaquobi, F.; Al-Jardani, A.; Petersen, E.; Al Abri, S. COVID-19 epidemic monitoring after non-pharmaceutical interventions: The use of time-varying reproduction number in a country with a large migrant population. Int. J. Infect. Dis. 2020, 99, 466–472. [Google Scholar] [CrossRef]
- Li, Q.; Guan, X.; Wu, P.; Qun, L.; Xuhua, G.; Peng, W.; Xiaoye, W.; Lei, Z.; Yeqing, T.; Ruiqi, R.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 2020, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Xu, X.; Wu, Y.; Wang, L.; Cowling, B.J.; Meyers, L.A. Serial interval of COVID-19 among publicly reported confirmed cases. Emerg. Infect. Dis. 2020, 1341–1343. [Google Scholar] [CrossRef]
- Cori, A.; Ferguson, N.M.; Fraser, C.; Cauchemez, S. A new framework and software to estimate time-varying reproduction numbers during epidemics. Am. J. Epidemiol. 2013, 178, 1505–1512. [Google Scholar] [CrossRef] [Green Version]
- Cori, A.; Ferguson, N.M.; Fraser, C.; Dahlqwist, E.; Demarsh, P.A.; Jombart, T.; Kamvar, Z.N.; Lessler, J.; Li, S.; Polonsky, J.A.; et al. Package ‘EpiEstim’; CRAN: Vienna, Austria, 2020; Available online: https://cran.r-project.org/web/packages/EpiEstim/EpiEstim.pdf (accessed on 12 December 2020).
- Price, D.J.; Shearer, F.M.; Meehan, M.T.; McBryde, E.; Moss, R.; Golding, N.; Conway, E.J.; Dawson, P.; Cromer, D.; Wood, J.; et al. Serial interval of SARS-CoV-2 was shortened over time by nonpharmaceutical interventions. Science 2020, eabc9004. [Google Scholar] [CrossRef]
- Price, D.J.; Shearer, F.M.; Meehan, M.T.; McBryde, E.; Moss, R.; Golding, N.; Conway, E.J.; Dawson, P.; Cromer, D.; Wood, J.; et al. Early analysis of the Australian covid-19 epidemic. Elife 2020, 9, 1–14. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: http://www.r-project.org/ (accessed on 12 December 2020).
- Mohd, M.H.; Sulayman, F. Unravelling the myths of R0 in controlling the dynamics of COVID-19 outbreak: A modelling perspective. Chaos Solitons Fractals 2020, 138, 109943. [Google Scholar] [CrossRef]
- Mat, N.F.C.; Edinur, H.A.; Razab, M.K.A.A.; Safuan, S. A single mass gathering resulted in massive transmission of COVID-19 infections in Malaysia with further international spread. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef]
- Chong, Y.M.; Sam, I.-C.; Chong, J.; Bador, M.K.; Ponnampalavanar, S.; Omar, S.F.S.; Kamarulzaman, A.; Munusamy, V.; Wong, C.K.; Jamaluddin, F.H.; et al. SARS-CoV-2 lineage B. 6 was the major contributor to early pandemic transmission in Malaysia. PLoS Negl. Trop. Dis. 2020, 14, e0008744. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Guidelines for the Implementation of Non-Pharmaceutical Interventions against COVID-19; European Centre for Disease Prevention and Control: Solna, Sweden, 2020; Available online: https://www.ecdc.europa.eu/en/publications-data/covid-19-guidelines-non-pharmaceutical-interventions (accessed on 1 November 2020).
- Tang, B.; Wang, X.; Li, Q.; Bragazzi, N.L.; Tang, S.; Xiao, Y.; Wu, J. Estimation of the transmission risk of 2019-nCov and its implication for public health interventions. SSRN Electron. J. 2020. [Google Scholar] [CrossRef] [Green Version]
- Boo, S.L. How MySejahtera Protects Your Data and Does More Than Contact Tracing. CodeBlue 2020. Available online: https://codeblue.galencentre.org/2020/08/12/how-mysejahtera-protects-your-data-and-does-more-than-contact-tracing/ (accessed on 7 March 2021).
- Boo, S.L. MOH: Home Quarantine Close Contacts, Test Only Those with Symptoms. CodeBlue 2021. Available online: https://codeblue.galencentre.org/2021/01/14/moh-home-quarantine-close-contacts-test-only-those-with-symptoms/ (accessed on 7 March 2021).
- Kretzschmar, M.E.; Rozhnova, G.; Bootsma, M.C.; van Boven, M.; van de Wijgert, J.H.; Bonten, M.J. Impact of delays on effectiveness of contact tracing strategies for COVID-19: A modelling study. Lancet Public Health 2020, 5, e452–e459. [Google Scholar] [CrossRef]
- Fifa, R. The Malaysian Response to COVID-19: Building Preparedness for ‘Surge Capacity’, Testing Efficiency, and Containment. Eur. Pharm. Rev. 2020. Available online: https://www.europeanpharmaceuticalreview.com/article/125084/the-malaysian-response-to-covid-19-building-preparedness-for-surge-capacity-testing-efficiency-and-containment/ (accessed on 7 March 2021).
- Max, R.; Esteban, O.-O. Coronavirus (COVID-19) Testing; Global Change Data Lab: Oxford, UK, 2021; Available online: https://ourworldindata.org/coronavirus-testing (accessed on 7 March 2021).
- Nicola, D. K number: What is the coronavirus metric that could be crucial as lockdown eases? Guardian 2020. Available online: https://www.theguardian.com/world/2020/jun/01/k-number-what-is-coronavirus-metric-crucial-lockdown-eases (accessed on 7 March 2021).
- Adam, K. Is the K number the new R number? What you need to know. World Econ. Forum 2020. Available online: https://www.weforum.org/agenda/2020/06/covid19-superspreaders-model-infection/ (accessed on 7 March 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phase | NPIs |
|---|---|
| MCO | Movement control of the public (i–viii) and border control (ix–xii)
|
| CMCO |
|
| RMCO |
|
| Day | MCO | Mean Rt | Difference | Difference (%) | Day Started | Day Ended | 2.5 Percentile | 97.5 Percentile |
|---|---|---|---|---|---|---|---|---|
| D1 | 1 | 1.23 | REF | REF | 45 | 51 | 1.155 | 1.307 |
| D5 | 1.147 | −0.082 | −6.69 | 49 | 55 | 1.082 | 1.214 | |
| D10 | 1.101 | −0.046 | −4.023 | 54 | 60 | 1.039 | 1.165 | |
| D1 | 2 | 1.054 | REF | REF | 59 | 65 | 0.995 | 1.114 |
| D5 | 0.949 | −0.104 | −9.913 | 63 | 69 | 0.892 | 1.008 | |
| D10 | 0.907 | −0.042 | −4.4 | 68 | 74 | 0.849 | 0.967 | |
| D1 | 3 | 0.665 | REF | REF | 73 | 79 | 0.606 | 0.728 |
| D5 | 0.738 | 0.072 | 10.869 | 77 | 83 | 0.667 | 0.813 | |
| D10 | 0.858 | 0.12 | 16.283 | 82 | 88 | 0.774 | 0.946 | |
| D1 | 4 | 0.954 | REF | REF | 87 | 93 | 0.871 | 1.041 |
| D5 | 0.787 | −0.167 | −17.526 | 91 | 97 | 0.707 | 0.87 | |
| D10 | 0.844 | 0.058 | 7.317 | 96 | 102 | 0.754 | 0.939 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Musa, K.I.; Arifin, W.N.; Mohd, M.H.; Jamiluddin, M.S.; Ahmad, N.A.; Chen, X.W.; Hanis, T.M.; Bulgiba, A. Measuring Time-Varying Effective Reproduction Numbers for COVID-19 and Their Relationship with Movement Control Order in Malaysia. Int. J. Environ. Res. Public Health 2021, 18, 3273. https://doi.org/10.3390/ijerph18063273
Musa KI, Arifin WN, Mohd MH, Jamiluddin MS, Ahmad NA, Chen XW, Hanis TM, Bulgiba A. Measuring Time-Varying Effective Reproduction Numbers for COVID-19 and Their Relationship with Movement Control Order in Malaysia. International Journal of Environmental Research and Public Health. 2021; 18(6):3273. https://doi.org/10.3390/ijerph18063273
Chicago/Turabian StyleMusa, Kamarul Imran, Wan Nor Arifin, Mohd Hafiz Mohd, Mohammad Subhi Jamiluddin, Noor Atinah Ahmad, Xin Wee Chen, Tengku Muhammad Hanis, and Awang Bulgiba. 2021. "Measuring Time-Varying Effective Reproduction Numbers for COVID-19 and Their Relationship with Movement Control Order in Malaysia" International Journal of Environmental Research and Public Health 18, no. 6: 3273. https://doi.org/10.3390/ijerph18063273