
Fear of COVID-19, Anxiety and Depression in Patients with Pulmonary Arterial Hypertension and Chronic Thromboembolic Pulmonary Hypertension during the Pandemic

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Methods
2.3. Statistical Analysis
3. Results
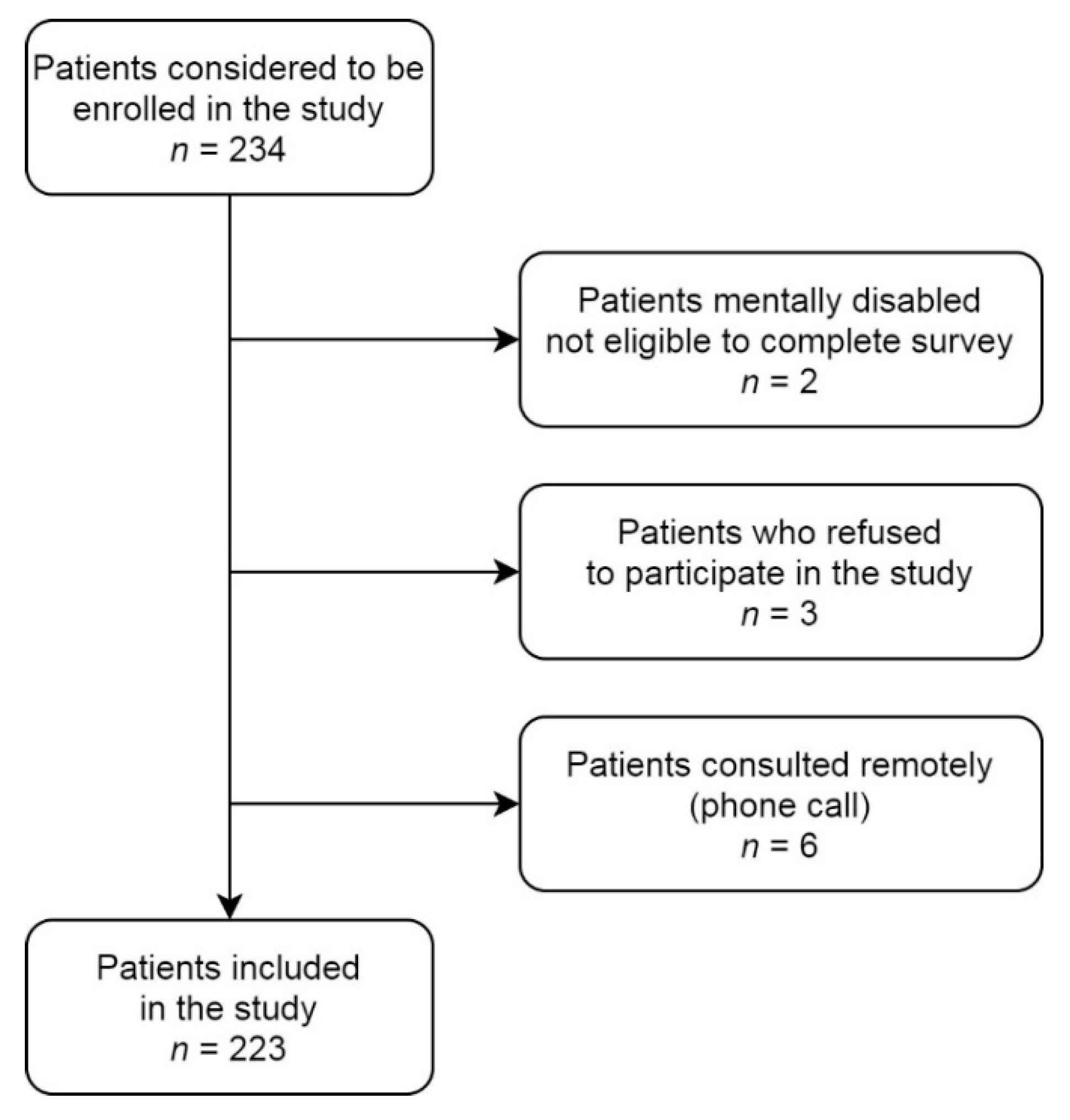
3.1. Study Group
3.2. Fear of COVID-19 and Hospital Anxiety and Depression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chudasama, Y.V.; Gillies, C.L.; Zaccardi, F.; Coles, B.; Davies, M.J.; Seidu, S.; Khunti, K. Impact of COVID-19 on routine care for chronic diseases: A global survey of views from healthcare professionals. Diabetes Metab. Syndr. 2020, 14, 965–967. [Google Scholar] [CrossRef]
- Kopec, G.; Tyrka, A.; Jonas, K.; Magon, W.; Waligora, M.; Stepniewski, J.; Podolec, P. The coronavirus disease 2019 pandemic prevents patients with pulmonary hypertension from seeking medical help. Kardiol. Pol. 2020, 78, 916–918. [Google Scholar] [CrossRef] [PubMed]
- Pawlikowski, J. The ethical dimension of prioritization and allocation decisions within the context of the coronavirus disease 2019 pandemic. Pol. Arch. Intern. Med. 2020, 130, 466–472. [Google Scholar] [CrossRef]
- Kopec, G.; Kurzyna, M.; Mroczek, E.; Chrzanowski, L.; Mularek-Kubzdela, T.; Skoczylas, I.; Kusmierczyk, B.; Pruszczyk, P.; Blaszczak, P.; Lewicka, E.; et al. Characterization of Patients with Pulmonary Arterial Hypertension: Data from the Polish Registry of Pulmonary Hypertension (BNP-PL). J. Clin. Med. 2020, 9, 173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galie, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [CrossRef]
- Kopec, G.; Dzikowska-Diduch, O.; Mroczek, E.; Mularek-Kubzdela, T.; Chrzanowski, L.; Skoczylas, I.; Tomaszewski, M.; Peregud-Pogorzelska, M.; Karasek, D.; Lewicka, E.; et al. Characteristics and outcomes of patients with chronic thromboembolic pulmonary hypertension in the era of modern therapeutic approaches: Data from the Polish multicenter registry (BNP-PL). Ther. Adv. Chronic. Dis. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Wieteska, M.; Biederman, A.; Kurzyna, M.; Dyk, W.; Burakowski, J.; Wawrzynska, L.; Szturmowicz, M.; Fijalkowska, A.; Szatkowski, P.; Torbicki, A. Outcome of Medically Versus Surgically Treated Patients With Chronic Thromboembolic Pulmonary Hypertension. Clin. Appl. Thromb. Hemost. 2016, 22, 92–99. [Google Scholar] [CrossRef] [Green Version]
- Siennicka, A.; Darocha, S.; Banaszkiewicz, M.; Kedzierski, P.; Dobosiewicz, A.; Blaszczak, P.; Peregud-Pogorzelska, M.; Kasprzak, J.D.; Tomaszewski, M.; Mroczek, E.; et al. Treatment of chronic thromboembolic pulmonary hypertension in a multidisciplinary team. Ther. Adv. Respir. Dis. 2019, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.D.; Burger, C.D.; Delossantos, G.B.; Grinnan, D.; Ralph, D.D.; Rayner, S.G.; Ryan, J.J.; Safdar, Z.; Ventetuolo, C.E.; Zamanian, R.T.; et al. A Survey-based Estimate of COVID-19 Incidence and Outcomes among Patients with Pulmonary Arterial Hypertension or Chronic Thromboembolic Pulmonary Hypertension and Impact on the Process of Care. Ann. Am. Thorac. Soc. 2020, 17, 1576–1582. [Google Scholar] [CrossRef]
- Belge, C.; Quarck, R.; Godinas, L.; Montani, D.; Escribano Subias, P.; Vachiery, J.L.; Nashat, H.; Pepke-Zaba, J.; Humbert, M.; Delcroix, M. COVID-19 in pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension: A reference centre survey. ERJ Open Res. 2020, 6. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Park, D.H.; Fuge, J.; Meltendorf, T.; Kahl, K.G.; Richter, M.J.; Gall, H.; Ghofrani, H.A.; Kamp, J.C.; Hoeper, M.M.; Olsson, K.M. Impact of SARS-CoV-2-Pandemic on Mental Disorders and Quality of Life in Patients With Pulmonary Arterial Hypertension. Front. Psychiatry 2021, 12, 668647. [Google Scholar] [CrossRef]
- Godinas, L.; Iyer, K.; Meszaros, G.; Quarck, R.; Escribano-Subias, P.; Vonk Noordegraaf, A.; Jansa, P.; D’Alto, M.; Luknar, M.; Milutinov Ilic, S.; et al. PH CARE COVID survey: An international patient survey on the care for pulmonary hypertension patients during the early phase of the COVID-19 pandemic. Orphanet. J. Rare Dis. 2021, 16, 196. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowska, J.; Meyer-Szary, J.; Mazurek-Kula, A.; Zuk, M.; Migdal, A.; Kusa, J.; Skiba, E.; Zygielo, K.; Przetocka, K.; Kordon, Z.; et al. The Impact of COVID-19 Pandemic on Children with Pulmonary Arterial Hypertension. Parental Anxiety and Attitudes. Follow-Up Data from the Polish Registry of Pulmonary Hypertension (BNP-PL). J. Clin. Med. 2021, 10, 1640. [Google Scholar] [CrossRef] [PubMed]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health. Addict. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Somaini, G.; Hasler, E.D.; Saxer, S.; Huber, L.C.; Lichtblau, M.; Speich, R.; Bloch, K.E.; Ulrich, S. Prevalence of Anxiety and Depression in Pulmonary Hypertension and Changes during Therapy. Respiration 2016, 91, 359–366. [Google Scholar] [CrossRef] [Green Version]
- Shafazand, S.; Goldstein, M.K.; Doyle, R.L.; Hlatky, M.A.; Gould, M.K. Health-related quality of life in patients with pulmonary arterial hypertension. Chest 2004, 126, 1452–1459. [Google Scholar] [CrossRef] [Green Version]
- Ibbotson, T.; Maguire, P.; Selby, P.; Priestman, T.; Wallace, L. Screening for anxiety and depression in cancer patients: The effects of disease and treatment. Eur. J. Cancer 1994, 30A, 37–40. [Google Scholar] [CrossRef]
- Evren, C.; Evren, B.; Dalbudak, E.; Topcu, M.; Kutlu, N. Measuring anxiety related to COVID-19: A Turkish validation study of the Coronavirus Anxiety Scale. Death Stud. 2020, 1–7. [Google Scholar] [CrossRef]
- Voitsidis, P.; Nikopoulou, V.A.; Holeva, V.; Parlapani, E.; Sereslis, K.; Tsipropoulou, V.; Karamouzi, P.; Giazkoulidou, A.; Tsopaneli, N.; Diakogiannis, I. The mediating role of fear of COVID-19 in the relationship between intolerance of uncertainty and depression. Psychol. Psychother. 2020, 94, 884–893. [Google Scholar] [CrossRef] [PubMed]
- Nikopoulou, V.A.; Holeva, V.; Parlapani, E.; Karamouzi, P.; Voitsidis, P.; Porfyri, G.N.; Blekas, A.; Papigkioti, K.; Patsiala, S.; Diakogiannis, I. Mental Health Screening for COVID-19: A Proposed Cutoff Score for the Greek Version of the Fear of COVID-19 Scale (FCV-19S). Int. J. Ment. Health Addict. 2020, 1–14. [Google Scholar] [CrossRef]
- Soraci, P.; Ferrari, A.; Abbiati, F.A.; Del Fante, E.; De Pace, R.; Urso, A.; Griffiths, M.D. Validation and Psychometric Evaluation of the Italian Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 1–10. [Google Scholar] [CrossRef]
- Reznik, A.; Gritsenko, V.; Konstantinov, V.; Khamenka, N.; Isralowitz, R. COVID-19 Fear in Eastern Europe: Validation of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Pilch, I.; Kurasz, Z.; Turska-Kawa, A. Experiencing fear during the pandemic: Validation of the fear of COVID-19 scale in Polish. PeerJ 2021, 9, e11263. [Google Scholar] [CrossRef] [PubMed]
- Pisula, E.; Nowakowska, I. Skala Lęku przed Koronawirusem FCV-19S (Ahorsu i in., 2020)—Polskie Tłumaczenie; Warsaw, Poland. 2020. Available online: https://www.researchgate.net/publication/344690639_Skala_Leku_przed_Koronawirusem_FCV-19S_Ahorsu_i_in_2020_-_polskie_tlumaczenie (accessed on 31 May 2021).
- Wichowicz, H.M.; Wieczorek, D. Screening post-stroke depression using the Hospital Anxiety and Depression Scale. Psychiatr. Pol. 2011, 45, 505–514. [Google Scholar] [PubMed]
- Babicki, M.; Szewczykowska, I.; Mastalerz-Migas, A. Mental Health in the Era of the Second Wave of SARS-CoV-2: A Cross-Sectional Study Based on an Online Survey among Online Respondents in Poland. Int. J. Environ. Res. Public Health 2021, 18, 2522. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, R.T.; Gati, S.; Papadakis, M.; Sharma, S. The Impact of COVID-19 on the Continuity of Cardiovascular Care. Eur. Heart J. 2021, 42, 215–217. [Google Scholar] [CrossRef]
- Sigorski, D.; Sobczuk, P.; Osmola, M.; Kuc, K.; Walerzak, A.; Wilk, M.; Ciszewski, T.; Kopec, S.; Hryn, K.; Rutkowski, P.; et al. Impact of COVID-19 on anxiety levels among patients with cancer actively treated with systemic therapy. ESMO Open 2020, 5, e000970. [Google Scholar] [CrossRef]
- Malik, S.; Ullah, I.; Irfan, M.; Ahorsu, D.K.; Lin, C.Y.; Pakpour, A.H.; Griffiths, M.D.; Rehman, I.U.; Minhas, R. Fear of COVID-19 and workplace phobia among Pakistani doctors: A survey study. BMC Public Health 2021, 21, 833. [Google Scholar] [CrossRef]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Vanhoof, J.M.; Delcroix, M.; Vandevelde, E.; Denhaerynck, K.; Wuyts, W.; Belge, C.; Dobbels, F. Emotional symptoms and quality of life in patients with pulmonary arterial hypertension. J. Heart Lung Transplant. 2014, 33, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Pfeuffer, E.; Krannich, H.; Halank, M.; Wilkens, H.; Kolb, P.; Jany, B.; Held, M. Anxiety, Depression, and Health-Related QOL in Patients Diagnosed with PAH or CTEPH. Lung 2017, 195, 759–768. [Google Scholar] [CrossRef]
- White, J.; Hopkins, R.O.; Glissmeyer, E.W.; Kitterman, N.; Elliott, C.G. Cognitive, emotional, and quality of life outcomes in patients with pulmonary arterial hypertension. Respir. Res. 2006, 7, 55. [Google Scholar] [CrossRef] [Green Version]
- McCollister, D.H.; Beutz, M.; McLaughlin, V.; Rumsfeld, J.; Masoudi, F.A.; Tripputi, M.; Yaeger, T.; Weintraub, P.; Badesch, D.B. Depressive symptoms in pulmonary arterial hypertension: Prevalence and association with functional status. Psychosomatics 2010, 51, 339.e8. [Google Scholar] [CrossRef]
- Lowe, B.; Grafe, K.; Ufer, C.; Kroenke, K.; Grunig, E.; Herzog, W.; Borst, M.M. Anxiety and depression in patients with pulmonary hypertension. Psychosom. Med. 2004, 66, 831–836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harzheim, D.; Klose, H.; Pinado, F.P.; Ehlken, N.; Nagel, C.; Fischer, C.; Ghofrani, A.; Rosenkranz, S.; Seyfarth, H.J.; Halank, M.; et al. Anxiety and depression disorders in patients with pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension. Respir. Res. 2013, 14, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, X.; Shi, H.; Yang, Y.; Zhang, Z.; Zhai, Z.; Wang, C. Anxiety and depression in patients with pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension: Results from a Chinese survey. Exp. Ther. Med. 2020, 19, 3124–3132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Djukanovic, I.; Carlsson, J.; Arestedt, K. Is the Hospital Anxiety and Depression Scale (HADS) a valid measure in a general population 65–80 years old? A psychometric evaluation study. Health Qual. Life Outcomes 2017, 15, 193. [Google Scholar] [CrossRef] [Green Version]
- Poland Coronavirus—Worldometer. Available online: https://covid19.who.int/region/euro/country/pl (accessed on 31 May 2021).
- Pilling, S.; Mayo-Wilson, E.; Mavranezouli, I.; Kew, K.; Taylor, C.; Clark, D.M.; Guideline Development, G. Recognition, assessment and treatment of social anxiety disorder: Summary of NICE guidance. BMJ 2013, 346, f2541. [Google Scholar] [CrossRef] [Green Version]
- Sobanski, P.Z.; Brzezinska Rajszys, G.; Grodzicki, T.; Jakubow, P.; Jankowski, P.; Kurzyna, M.; Nessler, J.; Przybylski, A.; Ratajska, A.; Tomkiewicz Pajak, L.; et al. Palliative care for people living with cardiac disease. Kardiol. Pol. 2020, 78, 364–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humbert, M.; Simonneau, G.; Rubin, L.J. A decade of achievement in pulmonary hypertension. Eur. Respir. Rev. 2011, 20, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Guillevin, L.; Armstrong, I.; Aldrighetti, R.; Howard, L.S.; Ryftenius, H.; Fischer, A.; Lombardi, S.; Studer, S.; Ferrari, P. Understanding the impact of pulmonary arterial hypertension on patients’ and carers’ lives. Eur. Respir. Rev. 2013, 22, 535–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Total Study Group n (%) or Mean (SD) | PAH n (%) or Mean (SD) | CTEPH n (%) or Mean (SD) | p < 0.05 PAH vs. CTEPH | |
|---|---|---|---|---|
| Number of patients | 223 (100%) | 147 (66%) | 76 (34%) | |
| Females/males | 141/82 (63%/37%) | 108/39 (73%/27%) | 33/43 (43%/56%) | 0.00001 * |
| Age, years | 59 (18–90) | 56 (18–88) | 66 (22–90) | 0.002 * |
| Duration of disease, years | 7.4 ± 7.3 | 8.6 ± 8.1 | 5.0 ± 4.5 | 0.001 * |
| PAH patients | ||||
| Idiopathic PAH | 75 (51%) | |||
| Heritable PAH | 5 (3%) | |||
| PAH associated with CHD | 34 (23%) | |||
| PAH associated with CTD | 27 (18%) | |||
| PAH porto-pulmonary | 5 (3%) | |||
| Drug-induced PAH | 1 (0.6%) | |||
| PAH monotherapy | 35 (24%) | |||
| PAH two drugs | 58 (40%) | |||
| PAH three drugs | 54 (36%) | |||
| CTEPH-BPA | 58 (76%) | |||
| CTEPH-PEA | 17 (22%) | |||
| CTEPH monotherapy (riociguat or sildenafil) | 59 (78%) | |||
| WHO functional class | 2.4 ± 0.7 | 2.5 ± 0.6 | 2.1 ± 0.8 | 0.002 * |
| 1 | 17 (8%) | 3 (2%) | 14 (18%) | |
| 2 | 109 (49%) | 73 (50%) | 36 (47%) | |
| 3 | 85 (38%) | 61 (41%) | 24 (32%) | |
| 4 | 12 (5%) | 10 (7%) | 2 (3%) | |
| Vaccinated against COVID-19 | 96 (43%) | 56 (38%) | 40 (53%) | 0.03 * |
| COVID-19 disease | 37 (17%) | 21 (14%) | 16 (21%) | 0.19 |
| History of depression | 29 (13%) | 22 (15%) | 7 (9%) | 0.23 |
| Concomitant disease | 142 (58%) | 85 (58%) | 57 (75%) | 0.01 * |
| Arterial hypertension | 100 (41%) | 60 (41%) | 40 (53%) | 0.10 |
| Diabetes | 37 (15%) | 25 (17%) | 12 (16%) | 0.81 |
| COPD | 20 (8%) | 11 (7%) | 9 (12%) | 0.28 |
| Coronary artery disease | 32 (13%) | 22 (15%) | 10 (13%) | 0.72 |
| Neoplasm | 21 (9%) | 11 (7%) | 10 (13%) | 0.17 |
| Obesity, BMI ≥ 30 kg/m2 | 59 (24%) | 36 (24%) | 23 (30%) | 0.35 |
| All Patients n (%); Median (IQR) or Mean (SD) n = 223 | PAH n (%); Median (IQR) or Mean (SD) n = 147 | CTEPH n (%); Median (IQR) or Mean (SD) n = 76 | p-Value | |
|---|---|---|---|---|
| Fear of COVID-19, points | 19 (13–24) 18.9 ± 7.4 | 20 (14–25) 19.3 ± 7.4 | 17 (12.5–23) 17.9 ± 7.3 | 0.12 |
| HADS-A, points | 6.0 (3–9) 6.0 ± 3.7 | 6 (3–9) 6.1 ± 3.6 | 6 (2.5–9) 5.8 ± 3.8 | 0.54 |
| HADS-D, points | 4 (1–7) 4.5 ± 3.6 | 3.0 (1–7) 4.3 ± 3.5 | 4 (1–7) 4.8 ± 3.8 | 0.49 |
| HADS ratty, points | 2 (1–4) 2.7 ± 1.8 | 2 (1–4) 2.7 ± 1.8 | 2 (1–4) 2.7 ± 2.0 | 0.84 |
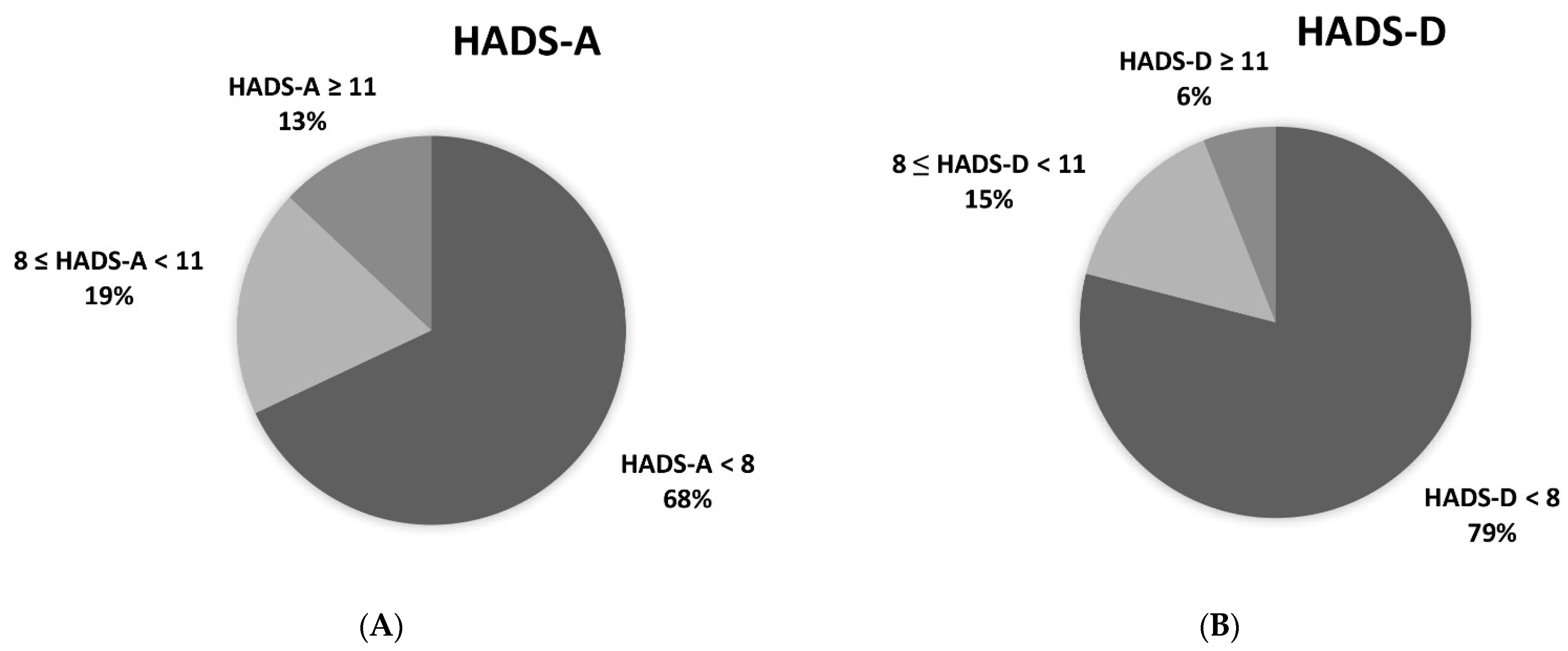
| Patients with HADS-A ≥ 8 points | 71 (32%) | 45 (31%) | 26 (34%) | 0.58 |
| Patients with HADS-A ≥ 11 points | 29 (13%) | 22 (15%) | 22 (15%) | 0.22 |
| Patients with HADS-D ≥ 8 points | 46 (21%) | 28 (19%) | 18 (24%) | 0.41 |
| Patients with HADS-D ≥ 11 points | 14 (6%) | 8 (5%) | 6 (8%) | 0.47 |
| Patients with HADS-A ≥ 8 points or HADS-D ≥ 8 points | 84 (38%) | 53 (36%) | 31 (41%) | 0.56 |
| FCV-19S Median (IQR) | p-Value | HADS-A Median (IQR) | p-Value | HADS-D Median (IQR) | p-Value | |
|---|---|---|---|---|---|---|
| PH type | 0.12 | 0.54 | 0.49 | |||
| All types of PAH | 19 (13–24) 18.9 ± 7.4 | 6 (3–9) 6.0 ± 3.7 | 4 (1–7) 4.5 ± 3.6 | |||
| IPAH | 20 (12–27) | 5 (3–9) | 3 (1–7) | |||
| PAH-CHD | 18 (15–23) | 7 (4–9) | 3.5 (1–7) | |||
| PAH-CTD | 20 (14–27) | 7 (4–9) | 5 (3–8) | |||
| PAH-porto-pulmonary | 23 (17–24) | 6 (4–7) | 1 (1–2) | |||
| Heritable PAH | 21 (18–21) | 6 (5–7) | 1 (1–4) | |||
| CTEPH | 17 (12.5–23) | 6 (2.5–9) | 4 (1–7) | |||
| Gender | 0.024 * | 0.026 * | 0.42 | |||
| female | 20 (15–25) | 6 (3–9) | 4 (1–7) | |||
| male | 17 (12–23) | 5 (2–8) | 3 (1–7) | |||
| Age | 0.023 * | 0.48 | 0.003 ** | |||
| <65 years | 18 (13–22) | 6 (3–9) | 3 (1–7) | |||
| ≥65 years | 22 (15–27) | 5 (3–9) | 5 (3–8) | |||
| WHO functional class | 0.15 | 0.09 | <0.001 *** | |||
| 1–2 | 17.5 (13–23) | 5 (3–8) | 3 (1–6) | |||
| 3–4 | 20 (14–25) | 6 (3–10) | 5 (3–9) | |||
| History of COVID-19 | 0.84 | 0.006 ** | 0.003 ** | |||
| yes | 19 (13–23) | 8 (5–10) | 7 (2–9) | |||
| no | 18.5 (13–24) | 5 (3–8) | 3 (1–7) | |||
| Vaccination against COVID-19 | 0.16 | 0.27 | 0.86 | |||
| yes | 19.5 (14–25.5) | 5 (2–9) | 3.5 (1–7) | |||
| no | 18 (12–23) | 6 (3–8) | 4 (1–7) |
| Univariate Analysis | p-Value | Multivariate Analysis | p-Value | |
|---|---|---|---|---|
| HADS-A ≥ 8 OR (95%CI) | HADS-A ≥ 8 OR (95%CI) | |||
| FCV-19S ≥ median | 5 (2.6–9.4) | 0.0000 * | 6.4 (2–20) | 0.002 * |
| History of COVID-19 | 3.1 (1.5–6.4) | 0.002 * | 3.5 (1.5–7.7) | 0.02 * |
| Vaccination against COVID-19 | 1.1 (0.6–2) | 0.67 | ||
| WHO functional class 3–4 | 1.7 (0.9–2.9) | 0.07 | ||
| History of depression (drugs or psychotherapy) | 1.9 (0.8–4.2) | 0.11 | ||
| Age ≥ 65 years | 1.1 (0.6–1.9) | 0.78 | ||
| Female gender | 1.4 (0.8–2.6) | 0.22 |
| Univariate Analysis | p-Value | Multivariate Analysis | p-Value | |
|---|---|---|---|---|
| HADS-D ≥ 8 OR (95%CI) | HADS-D ≥ 8 OR (95%CI) | |||
| FCV-19S ≥ median | 2.1 (1–4.2) | 0.02 * | 1.9 (0.9–3.9) | 0.06 |
| History of COVID-19 | 3.4 (1.6–7.3) | 0.002 * | 3.2 (1.4–7) | 0.004 * |
| Vaccination against COVID-19 | 1 (0.5–1.9) | 0.9 | ||
| WHO functional class 3–4 | 2.7 (1.4–5.3) | 0.003 * | 2.4 (1.2–4.8) | 0.01 * |
| History of depression (drugs or psychotherapy) | 1.6 (0.6–3.8) | 0.32 | ||
| Age ≥ 65 years | 1.6 (0.8–3.1) | 0.1 | ||
| Female gender | 0.7 (0.2–2.2) | 0.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wieteska-Miłek, M.; Szmit, S.; Florczyk, M.; Kuśmierczyk-Droszcz, B.; Ryczek, R.; Dzienisiewicz, M.; Torbicki, A.; Kurzyna, M. Fear of COVID-19, Anxiety and Depression in Patients with Pulmonary Arterial Hypertension and Chronic Thromboembolic Pulmonary Hypertension during the Pandemic. J. Clin. Med. 2021, 10, 4195. https://doi.org/10.3390/jcm10184195
Wieteska-Miłek M, Szmit S, Florczyk M, Kuśmierczyk-Droszcz B, Ryczek R, Dzienisiewicz M, Torbicki A, Kurzyna M. Fear of COVID-19, Anxiety and Depression in Patients with Pulmonary Arterial Hypertension and Chronic Thromboembolic Pulmonary Hypertension during the Pandemic. Journal of Clinical Medicine. 2021; 10(18):4195. https://doi.org/10.3390/jcm10184195
Chicago/Turabian StyleWieteska-Miłek, Maria, Sebastian Szmit, Michał Florczyk, Beata Kuśmierczyk-Droszcz, Robert Ryczek, Milena Dzienisiewicz, Adam Torbicki, and Marcin Kurzyna. 2021. "Fear of COVID-19, Anxiety and Depression in Patients with Pulmonary Arterial Hypertension and Chronic Thromboembolic Pulmonary Hypertension during the Pandemic" Journal of Clinical Medicine 10, no. 18: 4195. https://doi.org/10.3390/jcm10184195