
Prevalence and Impact of Atrial Fibrillation in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Studies Selection
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction and Quality Assessment
2.5. Outcomes Definition
2.6. Statistical Analysis
3. Results
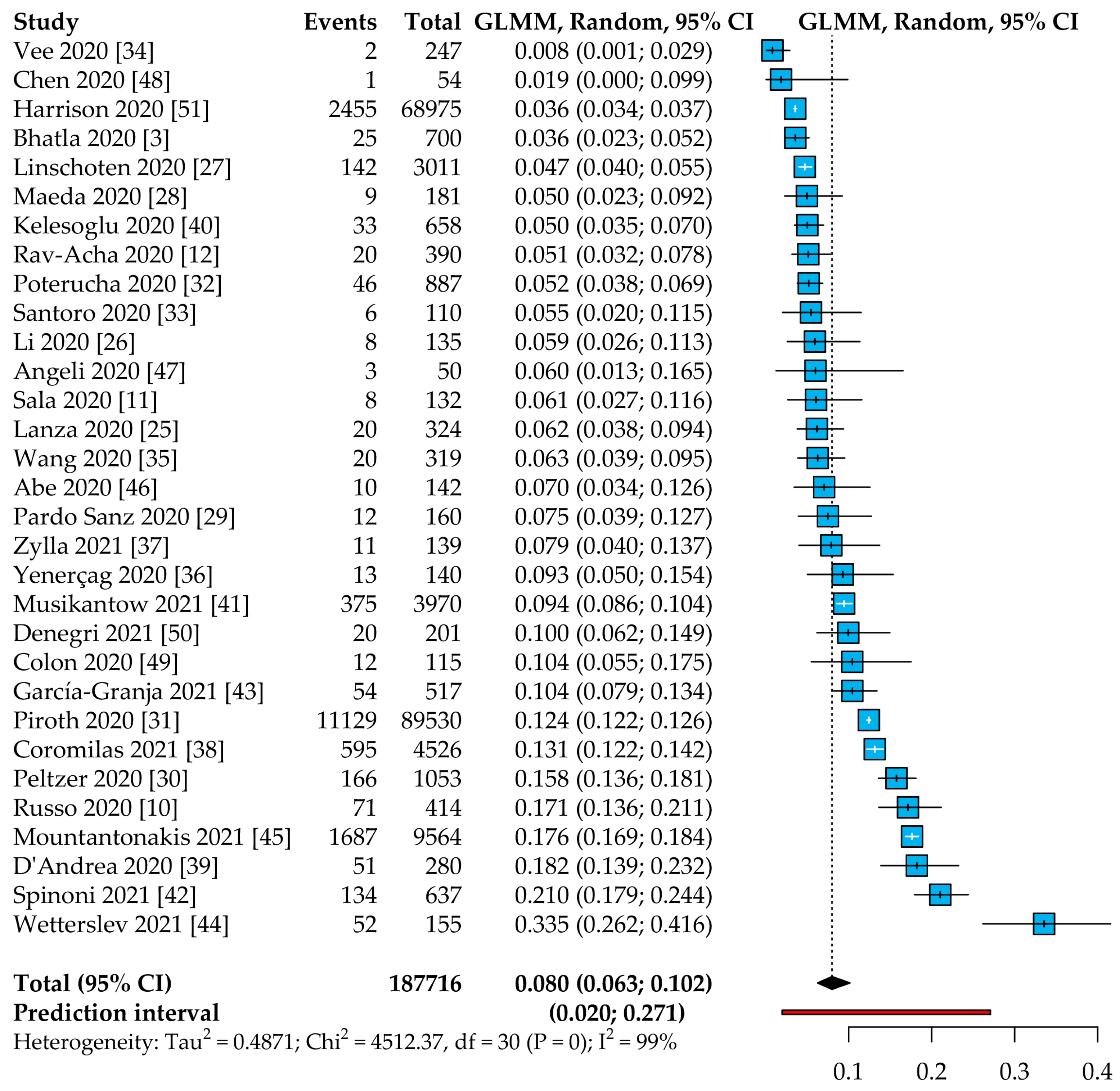
3.1. Prevalence of AF in Patients with COVID-19
3.2. Clinical Characteristics of AF Patients with COVID-19
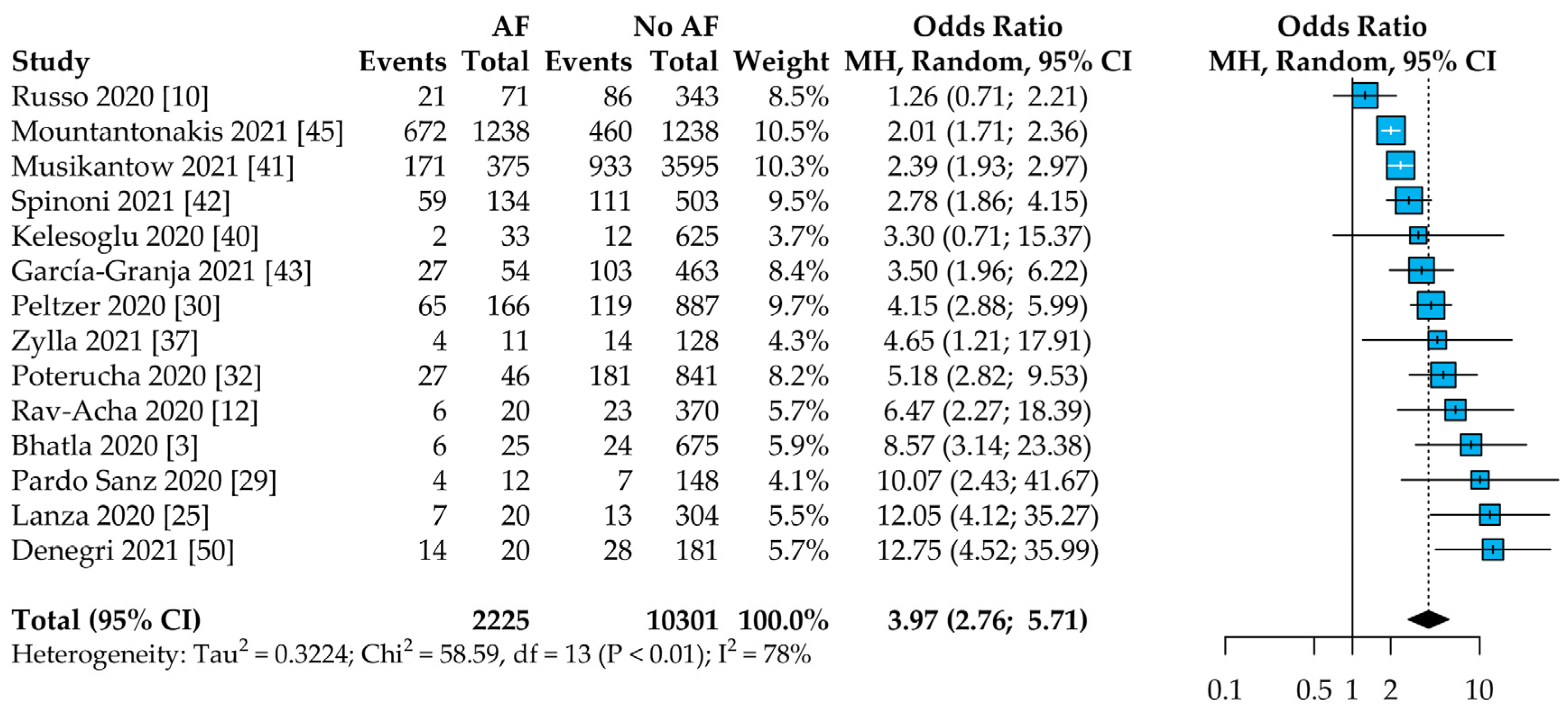
3.3. All-Cause Mortality according to AF Status
3.4. Sensitivity Analysis about New-Onset AF
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Nishiga, M.; Wang, D.W.; Han, Y.; Lewis, D.B.; Wu, J.C. COVID-19 and Cardiovascular Disease: From Basic Mechanisms to Clinical Perspectives. Nat. Rev. Cardiol. 2020, 17, 543–558. [Google Scholar] [CrossRef]
- Bhatla, A.; Mayer, M.M.; Adusumalli, S.; Hyman, M.C.; Oh, E.; Tierney, A.; Moss, J.; Chahal, A.A.; Anesi, G.; Denduluri, S.; et al. COVID-19 and Cardiac Arrhythmias. Heart Rhythm 2020, 17, 1439–1444. [Google Scholar] [CrossRef]
- Gundlund, A.; Olesen, J.B.; Butt, J.H.; Christensen, M.A.; Gislason, G.H.; Torp-Pedersen, C.; Køber, L.; Kümler, T.; Fosbøl, E.L. One-Year Outcomes in Atrial Fibrillation Presenting during Infections: A Nationwide Registry-Based Study. Eur. Heart J. 2020, 41, 1112–1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boos, C.J. Infection and Atrial Fibrillation: Inflammation Begets AF. Eur. Heart J. 2020, 41, 1120–1122. [Google Scholar] [CrossRef] [PubMed]
- Walkey, A.J.; Evans, S.R.; Winter, M.R.; Benjamin, E.J. Practice Patterns and Outcomes of Treatments for Atrial Fibrillation During Sepsis: A Propensity-Matched Cohort Study. Chest 2016, 149, 74–83. [Google Scholar] [CrossRef] [Green Version]
- Klein Klouwenberg, P.M.C.; Frencken, J.F.; Kuipers, S.; Ong, D.S.Y.; Peelen, L.M.; Van Vught, L.A.; Schultz, M.J.; Van Der Poll, T.; Bonten, M.J.; Cremer, O.L.; et al. Incidence, Predictors, and Outcomes of New-Onset Atrial Fibrillation in Critically Ill Patients with Sepsis a Cohort Study. Am. J. Respir. Crit. Care Med. 2017, 195, 205–211. [Google Scholar] [CrossRef]
- Walkey, A.J.; McManus, D. When Rhythm Changes Cause the Blues: New-Onset Atrial Fibrillation during Sepsis. Am. J. Respir. Crit. Care Med. 2017, 195, 152–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libby, P.; Lüscher, T. COVID-19 Is, in the End, an Endothelial Disease. Eur. Heart J. 2020, 41, 3038–3044. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Di Maio, M.; Mottola, F.F.; Pagnano, G.; Attena, E.; Verde, N.; Di Micco, P.; Silverio, A.; Scudiero, F.; Nunziata, L.; et al. Clinical Characteristics and Prognosis of Hospitalized COVID-19 Patients with Incident Sustained Tachyarrhythmias: A Multicenter Observational Study. Eur. J. Clin. Investg. 2020, 50, e13387. [Google Scholar] [CrossRef]
- Sala, S.; Peretto, G.; De Luca, G.; Farina, N.; Campochiaro, C.; Tresoldi, M.; Dagna, L.; Zangrillo, A.; Gulletta, S.; Della Bella, P. Low Prevalence of Arrhythmias in Clinically Stable COVID-19 Patients. PACE Pacing Clin. Electrophysiol. 2020, 43, 891–893. [Google Scholar] [CrossRef]
- Rav-Acha, M.; Orlev, A.; Itzhaki, I.; Zimmerman, S.F.; Fteiha, B.; Bohm, D.; Kurd, R.; Samuel, T.Y.; Asher, E.; Helviz, Y.; et al. Cardiac Arrhythmias amongst Hospitalised Coronavirus 2019 (COVID-19) Patients: Prevalence, Characterisation, and Clinical Algorithm to Classify Arrhythmic Risk. Int. J. Clin. Pract. 2021, 75, e13788. [Google Scholar] [CrossRef] [PubMed]
- Liao, S.C.; Shao, S.C.; Cheng, C.W.; Chen, Y.C.; Hung, M.J. Incidence Rate and Clinical Impacts of Arrhythmia Following COVID-19: A Systematic Review and Meta-Analysis of 17,435 Patients. Crit. Care 2020, 24, 690. [Google Scholar] [CrossRef]
- Yang, H.; Liang, X.; Xu, J.; Hou, H.; Wang, Y. Meta-Analysis of Atrial Fibrillation in Patients With COVID-19. Am. J. Cardiol. 2021, 144, 152–156. [Google Scholar] [CrossRef]
- Mulia, E.P.B.; Maghfirah, I.; Rachmi, D.A.; Julario, R. Atrial Arrhythmia and Its Association with COVID-19 Outcome: A Pooled Analysis. Diagnosis 2021. [Google Scholar] [CrossRef] [PubMed]
- Romiti, G.F.; Corica, B.; Cangemi, R.; Basili, S.; Raparelli, V. Need for Innovative and Timely Synthesis of Evidence during Covid-19 Outbreak. Eur. J. Intern. Med. 2020, 77, 165–166. [Google Scholar] [CrossRef]
- Viswanathan, M.; Ansari, M.T.; Berkman, N.D.; Chang, S.; Hartling, L.; McPheeters, M.; Santaguida, P.L.; Shamliyan, T.; Singh, K.; Tsertsvadze, A.; et al. Assessing the Risk of Bias of Individual Studies in Systematic Reviews of Health Care Interventions. In Methods Guide for Effectiveness and Comparative Effectiveness Reviews; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008. [Google Scholar]
- Stijnen, T.; Hamza, T.H.; Özdemir, P. Random Effects Meta-Analysis of Event Outcome in the Framework of the Generalized Linear Mixed Model with Applications in Sparse Data. Stat. Med. 2010, 29, 3046–3067. [Google Scholar] [CrossRef] [PubMed]
- IntHout, J.; Ioannidis, J.P.A.; Rovers, M.M.; Goeman, J.J. Plea for Routinely Presenting Prediction Intervals in Meta-Analysis. BMJ Open 2016, 6, e010247. [Google Scholar] [CrossRef] [Green Version]
- Riley, R.D.; Higgins, J.P.T.; Deeks, J.J. Interpretation of Random Effects Meta-Analyses. BMJ 2011, 342, 964–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavridis, D.; Salanti, G. How to Assess Publication Bias: Funnel Plot, Trim-and-Fill Method and Selection Models. Evid. Based Ment. Health 2014, 17, 30. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Harrer, M.; Cuijpers, P.; Furukawa, T.; Ebert, D.D. Dmetar: Companion R Package For The Guide “Doing Meta-Analysis in R”. 2019. Available online: http://dmetar.protectlab.org/ (accessed on 31 May 2021).
- Lanza, G.A.; De Vita, A.; Ravenna, S.E.; D’aiello, A.; Covino, M.; Franceschi, F.; Crea, F. Electrocardiographic Findings at Presentation and Clinical Outcome in Patients with SARS-CoV-2 Infection. Europace 2021, 23, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liu, T.; Tse, G.; Wu, M.; Jiang, J.; Liu, M.; Tao, L. Electrocardiograhic Characteristics in Patients with Coronavirus Infection: A Single-Center Observational Study. Ann. Noninvasive Electrocardiol. 2020, 25, 25. [Google Scholar] [CrossRef] [PubMed]
- Linschoten, M.; Peters, S.; van Smeden, M.; Jewbali, L.S.; Schaap, J.; Siebelink, H.-M.M.; Smits, P.C.; Tieleman, R.G.; van der Harst, P.; van Gilst, W.H.; et al. Cardiac Complications in Patients Hospitalised with COVID-19. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 817–823. [Google Scholar] [CrossRef]
- Maeda, T.; Obata, R.; Rizk, D.; Kuno, T. Cardiac Injury and Outcomes of Patients With COVID-19 in New York City. Heart Lung Circ. 2021, 30, 848–853. [Google Scholar] [CrossRef] [PubMed]
- Sanz, A.P.; Tahoces, L.S.; Pérez, R.O.; Ferrer, E.G.; Recalde, Á.S.; Gómez, J.L.Z. New-Onset Atrial Fibrillation during COVID-19 Infection Predicts Poor Prognosis. Cardiol. J. 2021, 28, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Peltzer, B.; Manocha, K.K.; Ying, X.; Kirzner, J.; Ip, J.E.; Thomas, G.; Liu, C.F.; Markowitz, S.M.; Lerman, B.B.; Safford, M.M.; et al. Outcomes and Mortality Associated with Atrial Arrhythmias among Patients Hospitalized with COVID-19. J. Cardiovasc. Electrophysiol. 2020, 31, 3077–3085. [Google Scholar] [CrossRef]
- Piroth, L.; Cottenet, J.; Mariet, A.S.; Bonniaud, P.; Blot, M.; Tubert-Bitter, P.; Quantin, C. Comparison of the Characteristics, Morbidity, and Mortality of COVID-19 and Seasonal Influenza: A Nationwide, Population-Based Retrospective Cohort Study. Lancet Respir. Med. 2021, 9, 251–259. [Google Scholar] [CrossRef]
- Poterucha, T.J.; Elias, P.; Jain, S.S.; Sayer, G.; Redfors, B.; Burkhoff, D.; Rosenblum, H.; DeFilippis, E.M.; Gupta, A.; Lawlor, M.; et al. Admission Cardiac Diagnostic Testing with Electrocardiography and Troponin Measurement Prognosticates Increased 30-Day Mortality in COVID-19. J. Am. Heart Assoc. 2021, 10, e018476. [Google Scholar] [CrossRef]
- Santoro, F.; Monitillo, F.; Raimondo, P.; Lopizzo, A.; Brindicci, G.; Gilio, M.; Musaico, F.; Mazzola, M.; Vestito, D.; Di Benedetto, R.; et al. QTc Interval Prolongation and Life-Threatening Arrhythmias during Hospitalization in Patients with COVID-19. Results from a Multi-Center Prospective Registry. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Vee, S.T.; Muhamad, D.B.; Nordin, N.B.; Ali, N.F.B.N.; Abdullah, N. Bin Clinical Characteristics of Severe Acute Respiratory Syndrome Coronavirus 2 (Sars-Cov2) Patients in Hospital Tengku Ampuan Afzan. Med. J. Malays. 2020, 75, 479–484. [Google Scholar]
- Wang, Y.; Chen, L.; Wang, J.; He, X.; Huang, F.; Chen, J.; Yang, X. Electrocardiogram Analysis of Patients with Different Types of COVID-19. Ann. Noninvasive Electrocardiol. 2020, 25, e12806. [Google Scholar] [CrossRef]
- Yenerçağ, M.; Arslan, U.; Şeker, O.O.; Dereli, S.; Kaya, A.; Doğduş, M.; Öztürk, Ç.E.; Akpınar, Ç.K.; Şen, A. Evaluation of P-Wave Dispersion in Patients with Newly Diagnosed Coronavirus Disease 2019. J. Cardiovasc. Med. (Hagerstown) 2021, 22, 197–203. [Google Scholar] [CrossRef]
- Zylla, M.M.; Merle, U.; Vey, J.A.; Korosoglou, G.; Hofmann, E.; Müller, M.; Herth, F.; Schmidt, W.; Blessing, E.; Göggelmann, C.; et al. Predictors and Prognostic Implications of Cardiac Arrhythmias in Patients Hospitalized for COVID-19. J. Clin. Med. 2021, 10, 133. [Google Scholar] [CrossRef] [PubMed]
- Coromilas, E.J.; Kochav, S.; Goldenthal, I.; Biviano, A.; Garan, H.; Goldbarg, S.; Kim, J.H.; Yeo, I.; Tracy, C.; Ayanian, S.; et al. Worldwide Survey of COVID-19-Associated Arrhythmias. Circ. Arrhythmia Electrophysiol. 2021, 285–295. [Google Scholar] [CrossRef]
- D’Andrea, A.; Russo, V.; Manzo, G.; Giordano, V.; Di Maio, M.; Crescibene, F.; D’Alto, M.; Bossone, E. Association of Atrial Fibrillation and Left Atrial Volume Index with Mortality in Patients with COVID-19 Pneumonia. Eur. J. Prev. Cardiol. 2020. [Google Scholar] [CrossRef]
- Kelesoglu, S.; Yilmaz, Y.; Ozkan, E.; Calapkorur, B.; Gok, M.; Dursun, Z.B.; Kilic, A.U.; Demirelli, S.; Simsek, Z.; Elcık, D. New Onset Atrial Fibrilation and Risk Faktors in COVID-19. J. Electrocardiol. 2021, 65, 76–81. [Google Scholar] [CrossRef]
- Musikantow, D.R.; Turagam, M.K.; Sartori, S.; Chu, E.; Kawamura, I.; Shivamurthy, P.; Bokhari, M.; Oates, C.; Zhang, C.; Pumill, C.; et al. Atrial Fibrillation in Patients Hospitalized With COVID-19: Incidence, Predictors, Outcomes and Comparison to Influenza. JACC Clin. Electrophysiol. 2021. [Google Scholar] [CrossRef]
- Spinoni, E.G.; Mennuni, M.; Rognoni, A.; Grisafi, L.; Colombo, C.; Lio, V.; Renda, G.; Foglietta, M.; Petrilli, I.; D’Ardes, D.; et al. Contribution of Atrial Fibrillation to In-Hospital Mortality in Patients with COVID-19. Circ. Arrhythmia Electrophysiol. 2021, 14, e009375. [Google Scholar] [CrossRef] [PubMed]
- García-Granja, P.E.; Veras, C.; Aparisi, Á.; Amat-Santos, I.J.; Catalá, P.; Marcos, M.; Cabezón, G.; Candela, J.; Gil, J.F.; Uribarri, A.; et al. Atrial Fibrillation in Patients with SARS-CoV-2 Infection. Med. Clin. (Barc). 2021. [Google Scholar] [CrossRef]
- Wetterslev, M.; Jacobsen, P.K.; Hassager, C.; Jøns, C.; Risum, N.; Pehrson, S.; Bastiansen, A.; Andreasen, A.S.; Tjelle Kristiansen, K.; Bestle, M.H.; et al. Cardiac Arrhythmias in Critically Ill Patients with Coronavirus Disease 2019: A Retrospective Population-Based Cohort Study. Acta Anaesthesiol. Scand. 2021, aas.13806. [Google Scholar] [CrossRef]
- Mountantonakis, S.E.; Saleh, M.; Fishbein, J.; Gandomi, A.; Lesser, M.; Chelico, J.; Gabriels, J.; Qiu, M.; Epstein, L.M. Atrial Fibrillation Is an Independent Predictor for In-Hospital Mortality in Patients Admitted with SARS-CoV-2 Infection. Heart Rhythm 2021, 18, 501–507. [Google Scholar] [CrossRef]
- Abe, T.; Egbuche, O.; Igwe, J.; Jegede, O.; Wagle, B.; Olanipekun, T.; Onwuanyi, A. Cardiovascular Complications in COVID-19 Patients with or without Diabetes Mellitus. Endocrinol. Diabetes Metab. 2021, 4. [Google Scholar] [CrossRef]
- Angeli, F.; Spanevello, A.; De Ponti, R.; Visca, D.; Marazzato, J.; Palmiotto, G.; Feci, D.; Reboldi, G.; Fabbri, L.M.; Verdecchia, P. Electrocardiographic Features of Patients with COVID-19 Pneumonia. Eur. J. Intern. Med. 2020, 78, 101–106. [Google Scholar] [CrossRef]
- Chen, Q.; Xu, L.; Dai, Y.; Ling, Y.; Mao, J.; Qian, J.; Zhu, W.; Di, W.; Ge, J. Cardiovascular Manifestations in Severe and Critical Patients with COVID-19. Clin. Cardiol. 2020, 43, 796–802. [Google Scholar] [CrossRef] [PubMed]
- Colon, C.M.; Barrios, J.G.; Chiles, J.W.; McElwee, S.K.; Russell, D.W.; Maddox, W.R.; Kay, G.N. Atrial Arrhythmias in COVID-19 Patients. JACC Clin. Electrophysiol. 2020, 6, 1189–1190. [Google Scholar] [CrossRef] [PubMed]
- Denegri, A.; Pezzuto, G.; D’Arienzo, M.; Morelli, M.; Savorani, F.; Cappello, C.G.; Luciani, A.; Boriani, G. Clinical and Electrocardiographic Characteristics at Admission of COVID-19/SARS-CoV2 Pneumonia Infection. Intern. Emerg. Med. 2021, 1–6. [Google Scholar] [CrossRef]
- Harrison, S.L.; Fazio-Eynullayeva, E.; Lane, D.A.; Underhill, P.; Lip, G.Y.H. Atrial Fibrillation and the Risk of 30-Day Incident Thromboembolic Events, and Mortality in Adults ≥ 50 Years with COVID-19. J. Arrhythm. 2021, 37, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Heijman, J.; Muna, A.P.; Veleva, T.; Molina, C.E.; Sutanto, H.; Tekook, M.; Wang, Q.; Abu-Taha, I.H.; Gorka, M.; Künzel, S.; et al. Atrial Myocyte NLRP3/CaMKII Nexus Forms a Substrate for Postoperative Atrial Fibrillation. Circ. Res. 2020, 127, 1036–1055. [Google Scholar] [CrossRef]
- Manjili, R.H.; Zarei, M.; Habibi, M.; Manjili, M.H. COVID-19 as an Acute Inflammatory Disease. J. Immunol. 2020, 205, 12–19. [Google Scholar] [CrossRef]
- Salama, C.; Han, J.; Yau, L.; Reiss, W.G.; Kramer, B.; Neidhart, J.D.; Criner, G.J.; Kaplan-Lewis, E.; Baden, R.; Pandit, L.; et al. Tocilizumab in Patients Hospitalized with Covid-19 Pneumonia. N. Engl. J. Med. 2021, 384, 20–30. [Google Scholar] [CrossRef]
- Huang, Q.; Wu, X.; Zheng, X.; Luo, S.; Xu, S.; Weng, J. Targeting Inflammation and Cytokine Storm in COVID-19. Pharmacol. Res. 2020, 159, 105051. [Google Scholar] [CrossRef]
- Gerotziafas, G.T.; Catalano, M.; Colgan, M.P.; Pecsvarady, Z.; Wautrecht, J.C.; Fazeli, B.; Olinic, D.M.; Farkas, K.; Elalamy, I.; Falanga, A.; et al. Guidance for the Management of Patients with Vascular Disease or Cardiovascular Risk Factors and COVID-19: Position Paper from VAS-European Independent Foundation in Angiology/Vascular Medicine. Thromb. Haemost. 2020, 120, 1597–1628. [Google Scholar] [CrossRef]
- Gencer, S.; Lacy, M.; Atzler, D.; Van Der Vorst, E.P.C.; Döring, Y.; Weber, C. Immunoinflammatory, Thrombohaemostatic, and Cardiovascular Mechanisms in COVID-19. Thromb. Haemost. 2020, 120, 1629–1641. [Google Scholar] [CrossRef]
- Bikdeli, B.; Madhavan, M.V.; Gupta, A.; Jimenez, D.; Burton, J.R.; Der Nigoghossian, C.; Chuich, T.; Nouri, S.N.; Dreyfus, I.; Driggin, E.; et al. Pharmacological Agents Targeting Thromboinflammation in COVID-19: Review and Implications for Future Research. Thromb. Haemost. 2020, 120, 1004–1024. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Yu, H.; Chen, H.; Qi, W.; Chen, L.; Chen, G.; Yan, W.; Chen, T.; Ning, Q.; Han, M.; et al. Longitudinal Changes of Inflammatory Parameters and Their Correlation with Disease Severity and Outcomes in Patients with COVID-19 from Wuhan, China. Crit. Care 2020, 24, 525. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, N.R.; Kunichoff, D.; Garshick, M.; Shah, B.; Pillinger, M.; Hochman, J.S.; Berger, J.S. C-Reactive Protein and Clinical Outcomes in Patients with COVID-19. Eur. Heart J. 2021. [Google Scholar] [CrossRef]
- Bosch, N.A.; Cimini, J.; Walkey, A.J. Atrial Fibrillation in the ICU. Chest 2018, 154, 1424–1434. [Google Scholar] [CrossRef]
- Mortensen, E.; Metersky, M.; Atuegwu, N.; Anzueto, A. New Onset Atrial Fibrillation in Patients Hospitalized with Pneumonia. Eur. Respir. J 2019, 54, OA3307. [Google Scholar]
- Cangemi, R.; Calvieri, C.; Falcone, M.; Bucci, T.; Bertazzoni, G.; Scarpellini, M.G.; Barillà, F.; Taliani, G.; Violi, F.; Battaglia, S.; et al. Relation of Cardiac Complications in the Early Phase of Community-Acquired Pneumonia to Long-Term Mortality and Cardiovascular Events. Am. J. Cardiol. 2015, 116, 647–651. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Bax, J.J.; Boriani, G.; Dan, G.A.; Fauchier, L.; Kalman, J.M.; Lane, D.A.; Lettino, M.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors Associated with COVID-19-Related Death Using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Proietti, M.; Marzona, I.; Vannini, T.; Tettamanti, M.; Fortino, I.; Merlino, L.; Basili, S.; Mannucci, P.M.; Boriani, G.; Lip, G.Y.H.; et al. Long-Term Relationship Between Atrial Fibrillation, Multimorbidity and Oral Anticoagulant Drug Use. Mayo Clin. Proc. 2019, 94, 2427–2436. [Google Scholar] [CrossRef]
- Iaccarino, G.; Grassi, G.; Borghi, C.; Ferri, C.; Salvetti, M.; Volpe Massimo, M. Age and Multimorbidity Predict Death among COVID-19 Patients: Results of the SARS-RAS Study of the Italian Society of Hypertension. Hypertension 2020, 76, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Mair, F.S.; Foster, H.M.; Nicholl, B.I. Multimorbidity and the COVID-19 Pandemic–An Urgent Call to Action. J. Comorbidity 2020, 10. [Google Scholar] [CrossRef]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Nigoghossian, C.D.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 2950–2973. [Google Scholar] [CrossRef]
- Guazzi, M.; Arena, R. Endothelial Dysfunction and Pathophysiological Correlates in Atrial Fibrillation. Heart 2009, 95, 102–106. [Google Scholar] [CrossRef]
- Bosch, N.A.; Rucci, J.M.; Massaro, J.M.; Winter, M.R.; Quinn, E.K.; Chon, K.H.; McManus, D.D.; Walkey, A.J. Comparative Effectiveness of Heart Rate Control Medications for the Treatment of Sepsis-Associated Atrial Fibrillation. Chest 2020, 159, 1452–1459. [Google Scholar] [CrossRef]
- Romiti, G.F.; Proietti, M. Impact of Rate Control in Hospitalized Patients with Atrial Fibrillation and Sepsis. Eur. J. Intern. Med. 2021. [Google Scholar] [CrossRef]
- Hertanto, D.M.; Sutanto, H.; Kencono Wungu, C. Immunomodulation as a Potent COVID-19 Pharmacotherapy: Past, Present and Future. Preprints 2021. [Google Scholar] [CrossRef]
- Romiti, G.F.; Pastori, D.; Rivera-Caravaca, J.M.; Ding, W.Y.; Gue, Y.X.; Menichelli, D.; Gumprecht, J.; Koziel, M.; Yang, P.-S.; Guo, Y.; et al. Adherence to the ‘Atrial Fibrillation Better Care’ (ABC) Pathway in Patients with Atrial Fibrillation. Thromb. Haemost. 2021. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Geographic Location | Study Type | Incl./Excl. Criteria | AF Diagnosis | N | AF | Age (Mean) | F (%) | HTN (%) | DM (%) | CRIT (%) | Previous AF (%) | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abe 2020 [46] | United States | Retrospective | Hospitalized patients | ECG changes | 142 | 9 | 58 | 50 | 73 | 50 | NA | 11 | NA |
| Angeli 2020 [47] | Italy | Retrospective | Hospitalized patients | Baseline ECG | 50 | 3 | 64 | 28 | 50 | 12 | 0 | NA | NA |
| Bhatla 2020 [3] | United States | Retrospective | Hospitalized patients | ECG changes | 700 | 25 | 50 | 55 | 50 | 26 | 11 | 6 | In-hospital mortality |
| Chen 2020 [48] | China | Retrospective | Severe hospitalized patients | ECG changes | 54 | 1 | 57.7 | 33 | 30 | 46 | 100 | NA | NA |
| Colon 2020 [49] | United States | Retrospective | Hospitalized patients | ECG, telemetry | 115 | 12 | 57.2 | 54 | 70 | 39 | 60 | 5 | NA |
| Coromilas 2021 [38] | Multinational | Retrospective | Hospitalized patients | Baseline ECG | 4526 | 595 | 62.8 | 43 | 55 | 35 | 20 | 9 | NA |
| D’Andrea 2020 [39] | Italy | Retrospective | Hospitalized patients | ECG | 280 | 51 | 66.6 | 40 | 35 | NA | NA | NA | NA |
| Denegri 2021 [50] | Italy | Retrospective | ED admission | Baseline ECG | 201 | 20 | 68.5 | 36 | 56 | 18 | 16 | 12 | 30-days mortality |
| García-Granja 2021 [43] | Spain | Retrospective | Hospitalized patients | ECG | 517 | 54 | 68.1 | 44 | 50 | 18 | 9 | 9 | In-hospital mortality |
| Harrison 2020 [51] | United States | Retrospective | Patients ≥ 50 years | ICD-10 codes | 68,975 | 2455 | 65.2 | 52 | 46 | 24 | NA | NA | NA |
| Kelesoglu 2020 [40] | Turkey | Retrospective | Hospitalized patients | ECG, telemetry | 658 | 33 | 54 | 43 | 32 | 18 | 9 | 0 | In-hospital mortality |
| Lanza 2020 [25] | Italy | Prospective | ED admission | Baseline ECG | 324 | 20 | 65.9 | 34 | 52 | 11 | 14 | NA | In-hospital mortality |
| Li 2020 [26] | China | Retrospective | Hospitalized patients | Baseline ECG | 135 | 8 | 64 * | 49 | 33 | 15 | 17 | NA | NA |
| Linschoten 2020 [27] | Multinational | Prospective | Hospitalized patients | ECG | 3011 | 142 | 67 * | 37 | 45 | 23 | 28 | NA | NA |
| Maeda 2020 [28] | United States | Retrospective | Hospitalized patients | ECG | 181 | 9 | 64.0 | 44 | 65 | 34 | 18 | 13 | NA |
| Mountantonakis 2021 [45] | United States | Retrospective | Hospitalized patients | ECG, medical notes | 9564 | 1687 | 64.8 | 41 | 63 | 40 | 20 | 7 | In-hospital mortality |
| Musikantow 2021 [41] | United States | Retrospective | Hospitalized patients | ICD-9/10 codes | 3970 | 375 | 66 * | 42 | 34 | 25 | 16 | 8 | In-hospital mortality |
| Pardo Sanz 2020 [29] | Spain | Prospective | Hospitalized patients | ECG, ECG Holter | 160 | 12 | 65.7 | 40 | 47 | 16 | 4 | 19 | In-hospital mortality |
| Peltzer 2020 [30] | United States | Retrospective | Hospitalized patients | ECG, telemetry | 1053 | 166 | 62.4 | 62 | 54 | 30 | 33 | 9 | In-hospital mortality |
| Piroth 2020 [31] | France | Retrospective | Hospitalized patients | ICD-10 codes | 89,530 | 11,129 | 65 | 47 | 33 | 19 | 16 | NA | NA |
| Poterucha 2020 [32] | United States | Retrospective | Hospitalized patients | Baseline ECG | 887 | 46 | 64.1 | 42 | 61 | 39 | NA | NA | 30-days mortality |
| Rav-Acha 2020 [12] | Israel | Retrospective | Hospitalized patients | ECG changes | 390 | 20 | 57.5 * | 45 | 30 | 20 | 10 | 7 | In-hospital mortality |
| Russo 2020 [10] | Italy | Retrospective | ED admission | Baseline ECG | 414 | 71 | 66 | 38 | 64 | 26 | NA | 17 | In-hospital mortality |
| Sala 2020 [11] | Italy | Prospective | Hospitalized patients | Baseline ECG | 132 | 8 | 65 | 33 | 45 | 20 | 0 | 12 | NA |
| Santoro 2020 [33] | Italy/Germany | Prospective | Hospitalized patients | Baseline ECG | 110 | 6 | 58 | 33 | 39 | 13 | 6 | NA | NA |
| Spinoni 2021 [42] | Italy | Retrospective | Hospitalized patients | ECG | 637 | 134 | NA | NA | NA | NA | NA | NA | In-hospital mortality |
| Vee 2020 [34] | Malaysia | Retrospective | Hospitalized patients | NA | 247 | 2 | 28 * | 30 | 11 | 7 | 2 | NA | NA |
| Wang 2020 [35] | China | Retrospective | Hospitalized patients | Baseline ECG | 319 | 20 | 65 | 52 | 44 | 23 | 30 | NA | NA |
| Wetterslev 2021 [44] | Denmark | Retrospective | Severe hospitalized patients | ECG, medical notes | 155 | 52 | 66 * | 27 | 44 | 21 | 100 | NA | NA |
| Yenerçag 2020 [36] | Turkey | Prospective | Hospitalized patients w/out AF, CKD, HF | ECG changes | 140 | 13 | 51.7 | 51 | 47 | 34 | NA | 0 | NA |
| Zylla 2021 [37] | Germany | Retrospective | Hospitalized patients | ECG changes | 139 | 11 | 61.1 | 34 | 43 | 19 | 39 | 0 | In-hospital mortality |
| Variable | Coefficient | Standard Error | Lower 95% CI | Upper 95% CI | p | R2 |
|---|---|---|---|---|---|---|
| Univariable Analysis | ||||||
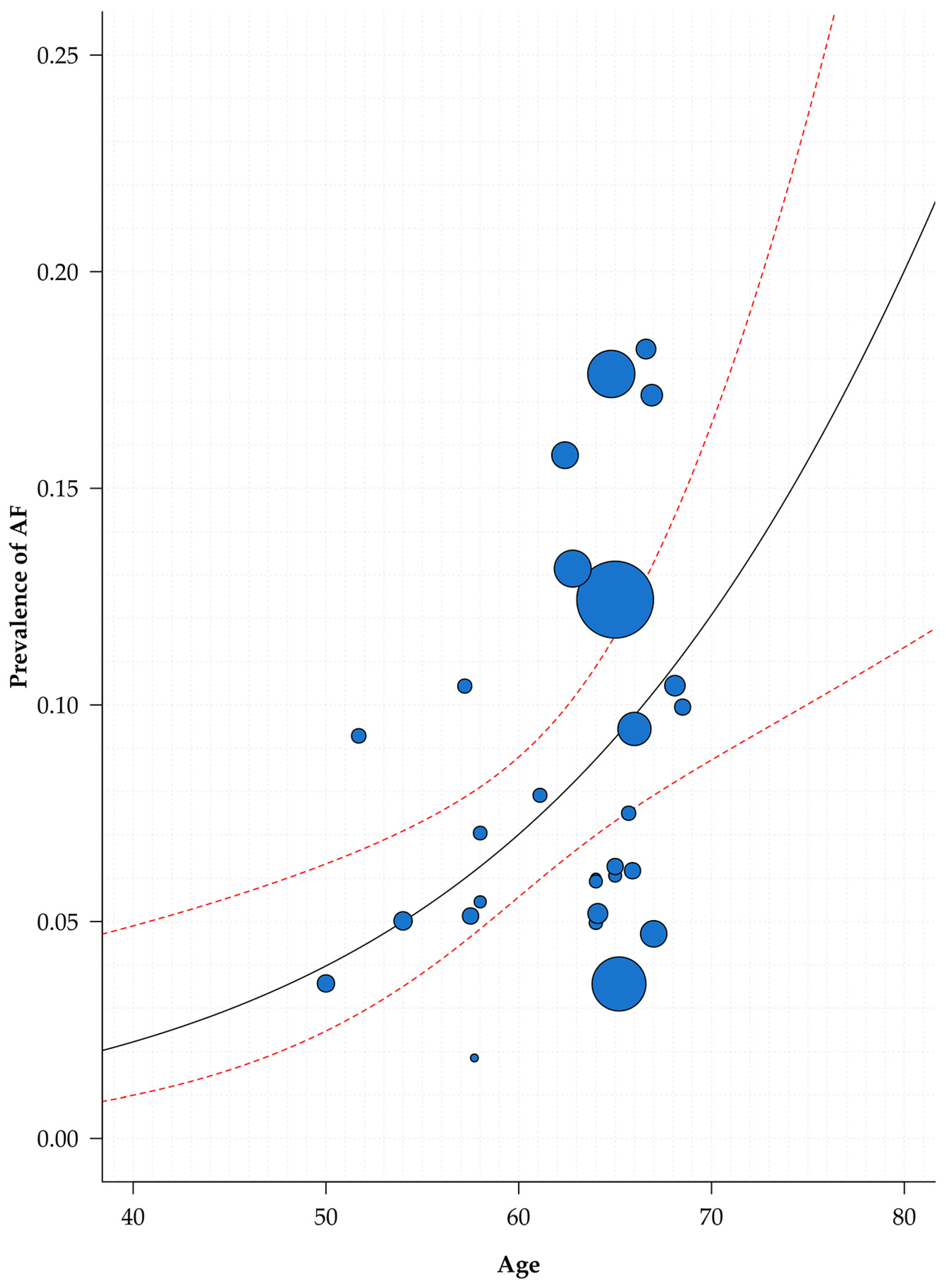
| Age | 0.054 | 0.016 | 0.021 | 0.087 | 0.003 | 0.289 |
| Female sex | 0.101 | 1.854 | −3.710 | 3.911 | 0.957 | 0.000 |
| Hypertension | 2.058 | 0.881 | 0.247 | 3.869 | 0.028 | 0.143 |
| Diabetes | 1.826 | 1.130 | −0.501 | 4.153 | 0.119 | 0.117 |
| Geographical location | 0.067 | 0.191 | ||||
| Europe (ref.) | ||||||
| North America | −0.331 | 0.277 | −0.900 | 0.238 | 0.242 | |
| Asia/other | −0.702 | 0.287 | −1.291 | −0.113 | 0.021 | |
| Multiple Analysis | 0.019 | 0.460 | ||||
| Age | 0.041 | 0.018 | 0.002 | 0.079 | 0.038 | |
| Hypertension | 0.115 | 1.357 | −2.692 | 2.922 | 0.933 | |
| Diabetes | 3.081 | 1.855 | −0.756 | 6.917 | 0.110 | |
| Geographical location | ||||||
| Europe (ref.) | ||||||
| North America | −0.676 | 0.344 | −1.387 | 0.036 | 0.062 | |
| Asia/other | −0.589 | 0.348 | −1.308 | 0.131 | 0.104 |
| Variable | N° Studies | MD | 95% CI | I2 |
| Continuous Variables | ||||
| Age | 7 | 13.2 | 10.5–15.9 | 86% |
| Variable | N° Studies | OR | 95% CI | I2 |
| Categorical Variables | ||||
| Female sex | 8 | 0.83 | 0.76–0.90 | 7% |
| Hypertension | 8 | 2.49 | 2.25–2.75 | 0% |
| Diabetes | 8 | 1.38 | 1.24–1.54 | 0% |
| CHF | 7 | 4.45 | 3.21–6.18 | 58% |
| CAD | 6 | 2.57 | 2.05–3.21 | 58% |
| Critical status | 12 | 3.62 | 2.39–5.48 | 69% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romiti, G.F.; Corica, B.; Lip, G.Y.H.; Proietti, M. Prevalence and Impact of Atrial Fibrillation in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2490. https://doi.org/10.3390/jcm10112490
Romiti GF, Corica B, Lip GYH, Proietti M. Prevalence and Impact of Atrial Fibrillation in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(11):2490. https://doi.org/10.3390/jcm10112490
Chicago/Turabian StyleRomiti, Giulio Francesco, Bernadette Corica, Gregory Y. H. Lip, and Marco Proietti. 2021. "Prevalence and Impact of Atrial Fibrillation in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 11: 2490. https://doi.org/10.3390/jcm10112490