
Questionnaire Survey of Possible Association of Allergic Diseases with Adverse Reactions to SARS-CoV-2 Vaccination

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Primary Endpoint
2.3. Population
2.4. Data Management Procedures
2.5. Statistical Methods
3. Results
3.1. Backgrounds of Vaccine Recipients
3.2. Higher Grades of Adverse Reactions in the Second than in the First Dose and in Female than in Male Recipients
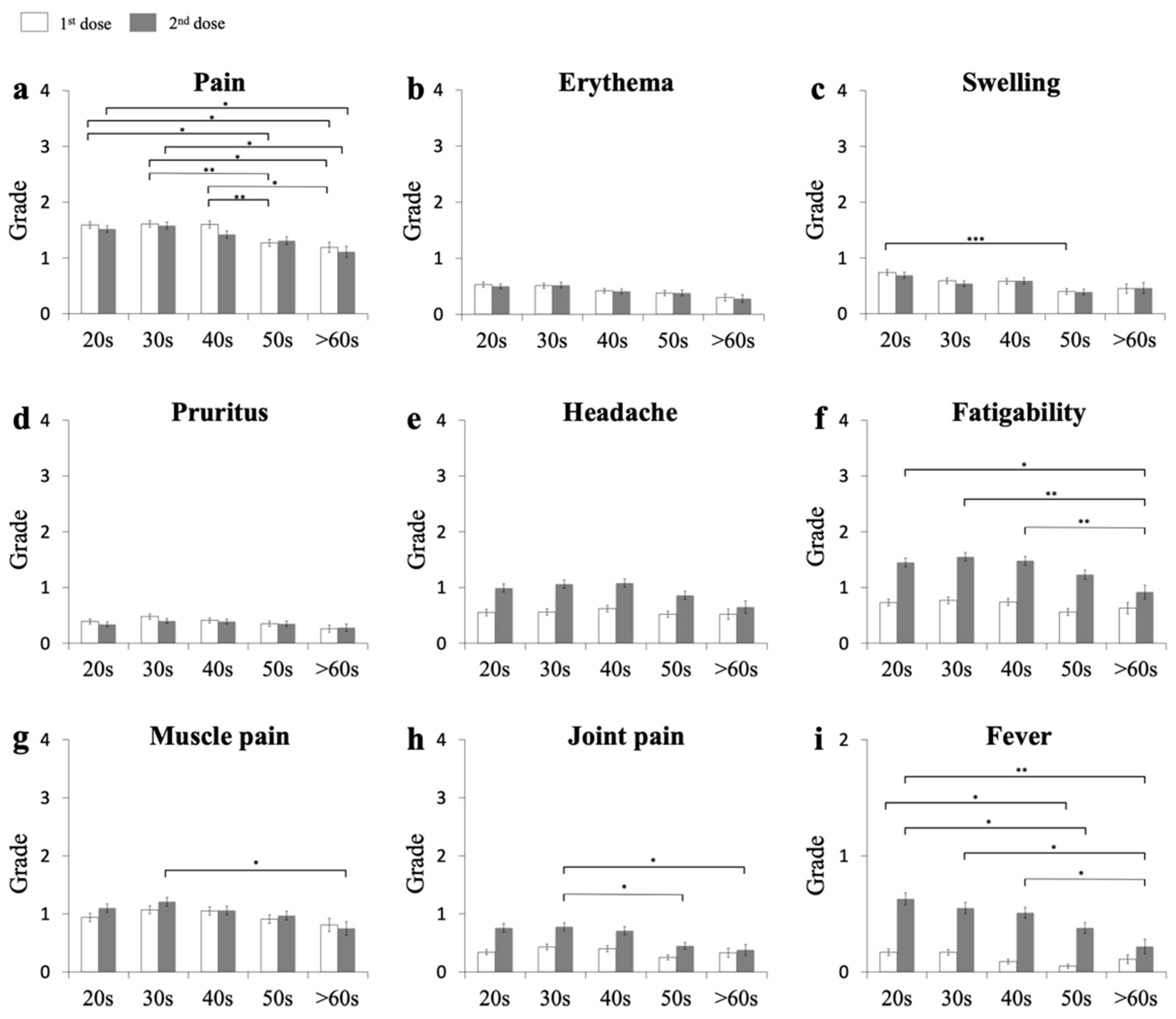
3.3. Higher Grades of Adverse Reactions in Recipients in Their 20s, 30s, and 40s than in Those in Their 50s or >60s
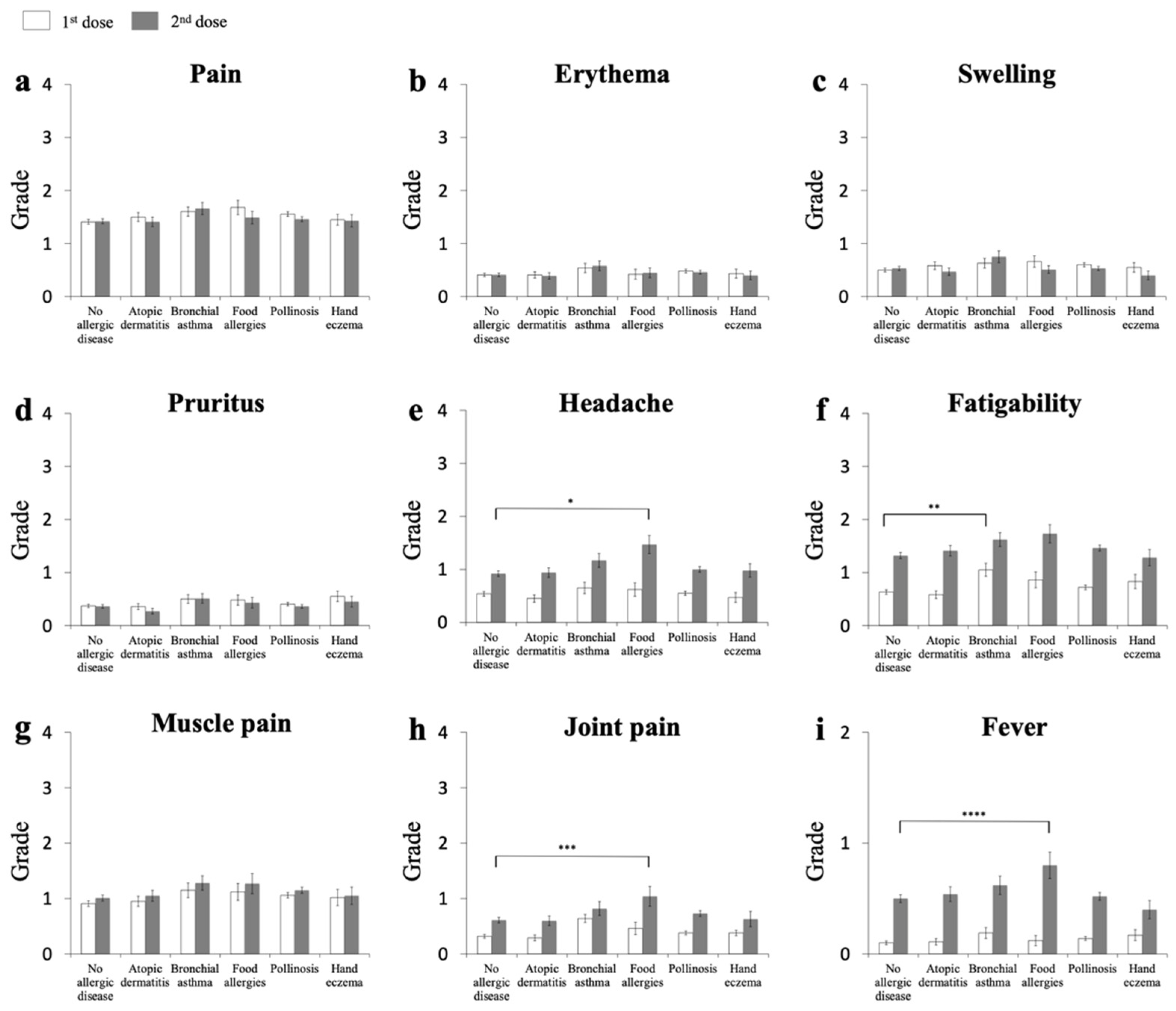
3.4. First-Dose Recipients with BA, but Not AD, FA, Pollinosis, or Hand Eczema, Show a Higher Grade of Fatigability
3.5. Second Dose Recipients with FA, but Not AD, BA, Pollinosis, or Hand Eczema, Show Higher Grades of Joint Pain and Fever
3.6. Recipients with AD Show No Higher Adverse Reactions
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez, M.G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Banerji, A.; Wickner, P.G.; Saff, R.; Stone, C.A., Jr.; Robinson, L.B.; Long, A.A.; Wolfson, A.R.; Williams, P.; Khan, D.A.; Phillips, E.; et al. mRNA vaccines to prevent COVID-19 disease and reported allergic reactions: Current evidence and suggested approach. J. Allergy Clin. Immunol. Pract. 2021, 9, 1423–1437. [Google Scholar] [CrossRef]
- Cabanillas, B.; Novak, N. Allergy to COVID-19 vaccines: A current update. Allergol. Int. 2021, 70, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Meo, S.A.; Bukhari, I.A.; Akram, J.; Meo, A.S.; Klonoff, D.C. COVID-19 vaccines: Comparison of biological, pharmacological characteristics and adverse effects of Pfizer/BioNTech and Moderna Vaccines. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1663–1669. [Google Scholar]
- Gee, J.; Marquez, P.; Su, J.; Calvert, G.M.; Liu, R.; Myers, T.; Nair, N.; Martin, S.; Clarl, T.; Markowitz, L.; et al. First month of COVID-19 vaccine safety monitoring—United States, 14 December 2020–13 January 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Caminati, M.; Guarnieri, G.; Batani, V.; Scarpieri, E.; Finocchiaro, A.; Chieco-Bianchi, F.; Senna, G.; Vianello, A. COVID-19 vaccination in patients with severe asthma on biologic treatment: Safety, tolerability, and impact on disease control. Vaccines 2021, 9, 853. [Google Scholar] [CrossRef] [PubMed]
- Balz, K.; Trassl, L.; Härtel, V.; Nelson, P.P.; Skevaki, C. Virus-induced T cell-mediated heterologous immunity and vaccine development. Front. Immunol. 2020, 11, 513. [Google Scholar] [CrossRef]
- Carli, G.; Cecchi, L.; Stebbing, J.; Parronchi, P.; Farsi, A. Is asthma protective against COVID-19? Allergy 2021, 76, 866–868. [Google Scholar] [CrossRef]
- Zhu, Z.; Hasegawa, K.; Ma, B.; Fujiogi, M.; Camargo, C.A., Jr.; Liang, L. Association of asthma and its genetic predisposition with the risk of severe COVID-19. J. Allergy Clin. Immunol. 2020, 146, 327–329. [Google Scholar] [CrossRef]
- Balz, K.; Kaushik, A.; Chen, M.; Cemic, F.; Heger, V.; Renz, H.; Nadeau, K.; Skevaki, C. Homologies between SARS-CoV-2 and allergen proteins may direct T cell-mediated heterologous immune responses. Sci. Rep. 2021, 11, 4792. [Google Scholar] [CrossRef]
- Grifoni, A.; Weiskopf, D.; Ramirez, S.I.; Mateus, J.; Dan, J.M.; Moderbacher, C.R.; Rawlings, S.A.; Sutherland, A.; Premkumar, L.; Jadi, R.S.; et al. Targets of T cell responses to SARS-CoV-2 coronavirus in humans with COVID-19 disease and unexposed individuals. Cell 2020, 181, 1489–1501. [Google Scholar] [CrossRef]
- Edwards, M.R.; Strong, K.; Cameron, A.; Walton, R.P.; Jackson, D.J.; Johnston, S.L. Viral infections in allergy and immunology: How allergic inflammation influences viral infections and illness. J. Allergy Clin. Immunol. 2017, 140, 909–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradding, P.; Richardson, M.; Hinks, T.S.C.; Howarth, P.H.; Choy, D.F.; Arron, J.R.; Wenzel, S.E.; Siddiqui, S. ACE2, TMPRSS2, and furin gene expression in the airways of people with asthma-implications for COVID-19. J. Allergy Clin. Immunol. 2020, 146, 208–211. [Google Scholar] [CrossRef]
- Jackson, D.J.; Busse, W.W.; Bacharier, L.B.; Kattan, M.; O’Connor, G.T.; Wood, R.A.; Visness, C.M.; Durham, S.R.; Larson, D.; Esnault, S.; et al. Association of respiratory allergy, asthma, and expression of the SARS-CoV-2 receptor ACE2. J. Allergy Clin. Immunol. 2020, 146, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Patrick, M.T.; Zhang, H.; Wasikowski, R.; Prens, E.P.; Weidinger, S.; Gudjonsson, J.E.; Elder, J.T.; He, K.; Tsoi, L.C. Associations between COVID-19 and skin conditions identified through epidemiology and genomic studies. J. Allergy Clin. Immunol. 2021, 147, 857–869. [Google Scholar] [CrossRef]
- Tokura, Y.; Phadungsaksawasdi, P.; Ito, T. Atopic dermatitis as Th2 disease revisited. J. Cutan. Immunol. Allergy 2018, 1, 158–164. [Google Scholar] [CrossRef] [Green Version]
- Akdis, C.A.; Arkwright, P.D.; Brüggen, M.C.; Busse, W.; Gadina, M.; Guttman-Yassky, E.; Kabashima, K.; Mitamura, Y.; Vian, L.; Wu, J.; et al. Type 2 immunity in the skin and lungs. Allergy 2020, 75, 1582–1605. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhi, Y.; Ying, S. COVID-19 and asthma: Reflection during the pandemic. Clin. Rev. Allergy Immunol. 2020, 59, 78–88. [Google Scholar] [CrossRef]
- Thomas, W.R. Hierarchy and molecular properties of house dust mite allergens. Allergol. Int. 2015, 64, 304–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Recipients |
|---|---|
| N of recipients | 955 |
| Sex | |
| Male, n (%) | 203 (21.3) |
| Female, n (%) | 734 (76.9) |
| Unknown, n (%) | 18 (1.9) |
| Age | |
| 20s, n (%) | 235 (24.6) |
| 30s, n (%) | 230 (24.1) |
| 40s, n (%) | 230 (24.1) |
| 50s, n (%) | 186 (19.5) |
| >60, n (%) | 74 (7.7) |
| No allergic disease, n (%) | 396 (41.5) |
| History of AD 1, n (%) | 132 (13.8) |
| History of BA 2, n (%) | 78 (8.2) |
| History of FA 3, n (%) | 50 (5.2) |
| History of pollinosis, n (%) | 428 (44.8) |
| History of hand eczema, n (%) | 60 (6.3) |
| Adverse Reactions | Male (n = 203 [21.3%]) | Female (n = 734 [76.9%]) | p Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| First dose | Grade * | Grade * | |||||||||
| Local injection reactions | 0 | 1 | 2 | 3 | 4 | 0 | 1 | 2 | 3 | 4 | |
| Pain, n (%) | 27 (13.3) | 89 (43.8) | 62 (30.5) | 23 (11.3) | 2 (1.0) | 92 (12.5) | 284 (38.7) | 242 (33.0) | 114 (15.5) | 2 (0.2) | 0.26 |
| Erythema, n (%) | 148 (72.9) | 40 (19.7) | 13 (6.4) | 2 (1.0) | 0 | 455 (62.0) | 213 (29.0) | 61 (8.3) | 5 (0.7) | 0 | 0.0295 |
| Swelling, n (%) | 131 (64.5) | 43 (21.2) | 13 (6.4) | 2 (1.0) | 0 | 414 (56.4) | 213 (29.0) | 99 (13.5) | 8 (1.1) | 0 | 0.13 |
| Pruritus, n (%) | 169 (83.3) | 23 (11.3) | 11 (5.4) | 0 | 0 | 487 (66.3) | 167 (22.8) | 80 (10.9) | 0 | 0 | <0.0001 |
| Systemic reactions | 0 | 1 | 2 | 3 | 4 | 0 | 1 | 2 | 3 | 4 | |
| Headache, n (%) | 164 (80.8) | 23 (11.3) | 16 (7.9) | 0 | 0 | 432 (58.9) | 166 (22.6) | 102 (13.9) | 32 (4.4) | 2 (0.2) | <0.0001 |
| Fatigability, n (%) | 140 (69.0) | 39 (19.2) | 23 (11.3) | 1 (0.5) | 0 | 382 (52.0) | 184 (25.1) | 126 (17.2) | 41 (5.6) | 1 (0.1) | 0.0001 |
| Muscle pain, n (%) | 116 (57.1) | 48 (23.6) | 26 (12.8) | 11 (5.4) | 2 (1.0) | 298 (40.6) | 176 (24.0) | 180 (24.5) | 75 (10.2) | 5 (0.7) | 0.0001 |
| Joint pain, n (%) | 173 (85.2) | 21 (10.3) | 7 (3.4) | 1 (0.5) | 1 (0.5) | 527 (71.8) | 147 (20.0) | 37 (5.0) | 22 (3.0) | 1 (0.1) | 0.0012 |
| Fever, n (%) | 184 (90.6) | 17 (8.4) | 2 (1.0) | 684 (93.2) | 82 (11.2) | 4 (0.5) | 0.415 | ||||
| Anaphylaxis (or vagal reflex), n (%) | 201 (99.0) | 2 (1.0) | 724 (98.6) | 10 (1.4) | 0.94 | ||||||
| Second dose | Grade * | Grade * | |||||||||
| Local injection reactions | 0 | 1 | 2 | 3 | 4 | 0 | 1 | 2 | 3 | 4 | |
| Pain, n (%) | 36 (17.7) | 81 (40.0) | 64 (31.5) | 21 (10.3) | 1 (0.5) | 116 (15.8) | 287 (39.1) | 209 (28.5) | 119 (16.2) | 0 | 0.086 |
| Erythema, n (%) | 150 (73.9) | 37 (18.2) | 12 (5.9) | 4 (2.0) | 0 | 472 (64.3) | 191 (26.0) | 58 (8.0) | 10 (1.4) | 0 | 0.061 |
| Swelling, n (%) | 136 (67.0) | 41 (20.2) | 21 (10.3) | 5 (2.5) | 0 | 435 (59.3) | 191 (26.0) | 88 (12.0) | 17 (2.3) | 0 | 0.24 |
| Pruritus, n (%) | 172 (84.7) | 23 (11.3) | 8 (3.9) | 0 | 0 | 507 (69.1) | 153 (20.8) | 64 (8.7) | 7 (1.0) | 0 | 0.0002 |
| Systemic reactions | 0 | 1 | 2 | 3 | 4 | 0 | 1 | 2 | 3 | 4 | |
| Headache, n (%) | 144 (70.9) | 29 (14.3) | 20 (9.9) | 9 (4.4) | 1 (0.5) | 306 (41.7) | 144 (19.6) | 182 (24.8) | 94 (12.8) | 5 (0.7) | <0.0001 |
| Fatigability, n (%) | 93 (45.8) | 43 (21.2) | 36 (17.7) | 27 (13.3) | 3 (1.5) | 194 (26.4) | 164 (22.3) | 201 (27.4) | 159 (21.7) | 13 (1.8) | <0.0001 |
| Muscle pain, n (%) | 104 (51.2) | 42 (20.7) | 39 (19.2) | 16 (7.9) | 2 (1.0) | 296 (40.3) | 160 (21.8) | 161 (21.9) | 108 (14.7) | 6 (0.8) | 0.03 |
| Joint pain, n (%) | 160 (78.8) | 21 (10.3) | 12 (5.9) | 10 (4.9) | 0 | 440 (60.0) | 123 (16.8) | 93 (12.7) | 69 (9.4) | 6 (0.8) | 0.0001 |
| Fever, n (%) | 137 (67.5) | 45 (22.2) | 21 (10.3) | 452 (61.6) | 180 (24.5) | 97 (13.2) | 0.42 | ||||
| Anaphylaxis (or vagal reflex), n (%) | 202 (99.5) | 1 (0.5) | 720 (98.1) | 11 (1.5) | 0.43 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morimoto, H.; Hayano, S.; Ozawa, N.; Ogura, Y.; Usui, H.; Usami, T.; Ohse, A.; Otsuka, M.; Miyachi, M.; Tokura, Y. Questionnaire Survey of Possible Association of Allergic Diseases with Adverse Reactions to SARS-CoV-2 Vaccination. Vaccines 2021, 9, 1421. https://doi.org/10.3390/vaccines9121421
Morimoto H, Hayano S, Ozawa N, Ogura Y, Usui H, Usami T, Ohse A, Otsuka M, Miyachi M, Tokura Y. Questionnaire Survey of Possible Association of Allergic Diseases with Adverse Reactions to SARS-CoV-2 Vaccination. Vaccines. 2021; 9(12):1421. https://doi.org/10.3390/vaccines9121421
Chicago/Turabian StyleMorimoto, Hiroki, Satoshi Hayano, Naoya Ozawa, Yasuaki Ogura, Hiroaki Usui, Takahiro Usami, Ayako Ohse, Masaki Otsuka, Masahiko Miyachi, and Yoshiki Tokura. 2021. "Questionnaire Survey of Possible Association of Allergic Diseases with Adverse Reactions to SARS-CoV-2 Vaccination" Vaccines 9, no. 12: 1421. https://doi.org/10.3390/vaccines9121421