
How Policy Mix Choices Affect the COVID-19 Pandemic Response Outcomes in Chinese Cities: An Empirical Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Sample
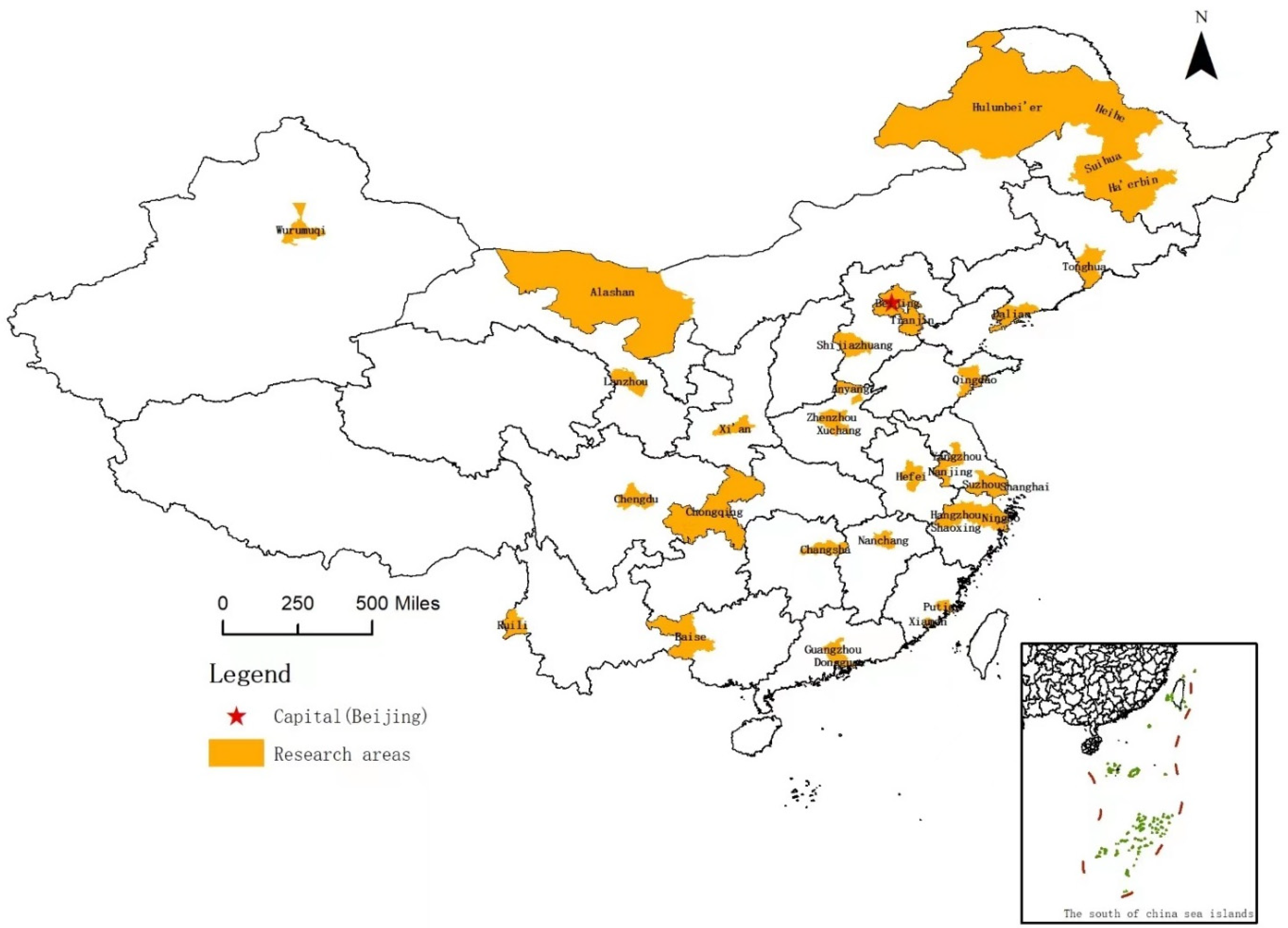
2.2. City Selection
- All 36 cities are municipal-level cities (divided into districts). According to the current Law on the Prevention and Treatment of Infectious Diseases, the municipal government is the agency responsible for responding to infectious diseases within its jurisdiction. It is the key decision-making body for pandemic management. The central or provincial governments only intervene when the municipal government is incapable of controlling the crisis. In that case, the higher levels of government primarily act as coordinators and supervisors but do not replace the municipal government in directly managing the crisis.
- These 36 cities represent different geographical locations, population sizes, economic and technological development levels, and administrative and cultural traditions; they are located in eastern, central, and western China. Among them, there are 4 municipalities directly under the central government; another 14 are provincial capitals, and the other 18 are important transportation hubs, with active international economic and trade exchange. These hubs are close to mega-cities or are border cities. Although the cities differ considerably, they all face high pressure to prevent and control the COVID-19 pandemic.
- The cities have relatively independent discretion to deal with the pandemic. Thus, our sample cities are comparable yet representative for examining the relationships between the different policy strategies that were chosen and the pandemic management outcomes of those choices.
2.3. Analysis Methods
3. Results
3.1. Identifying Policy Tools
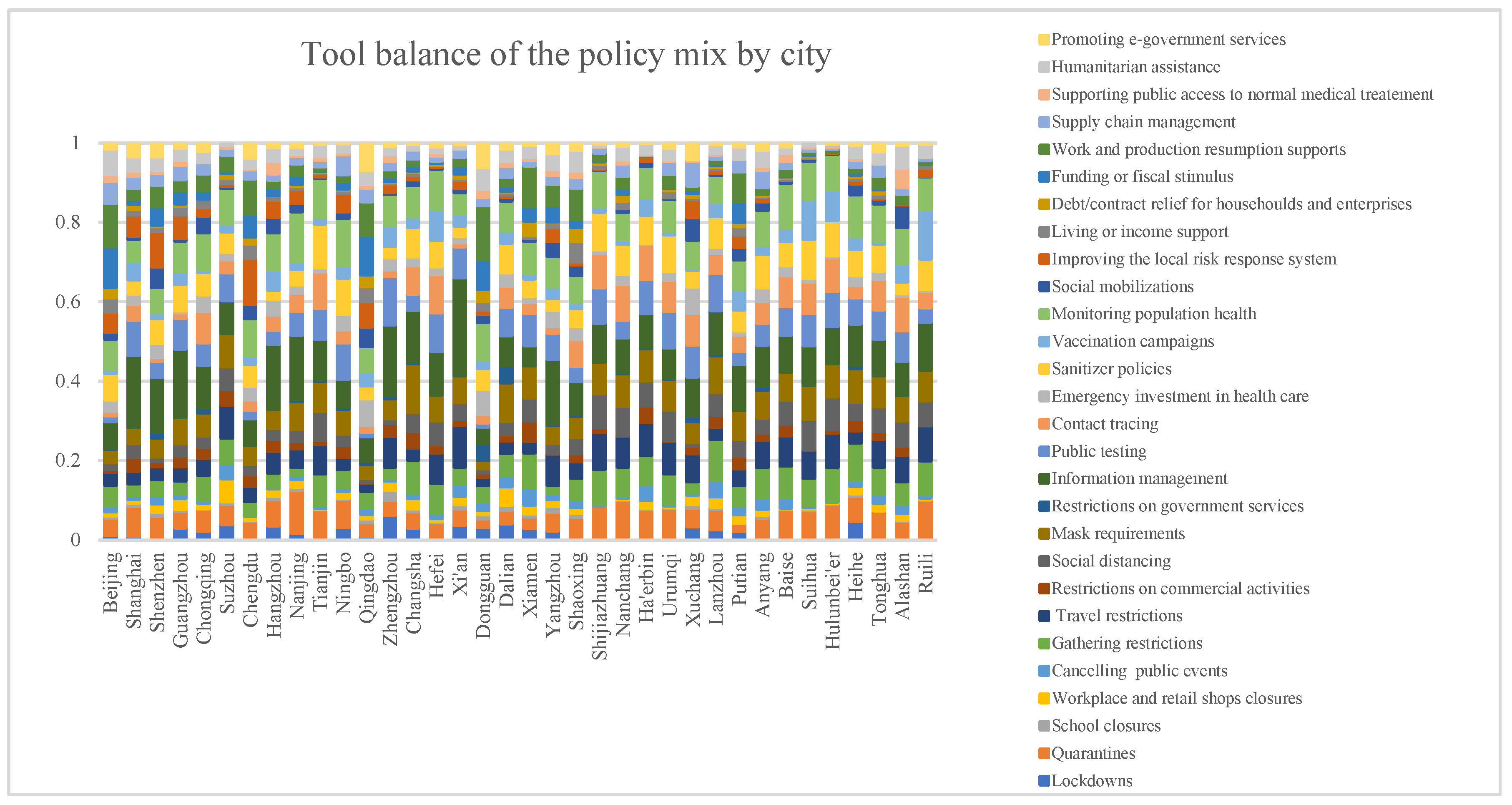
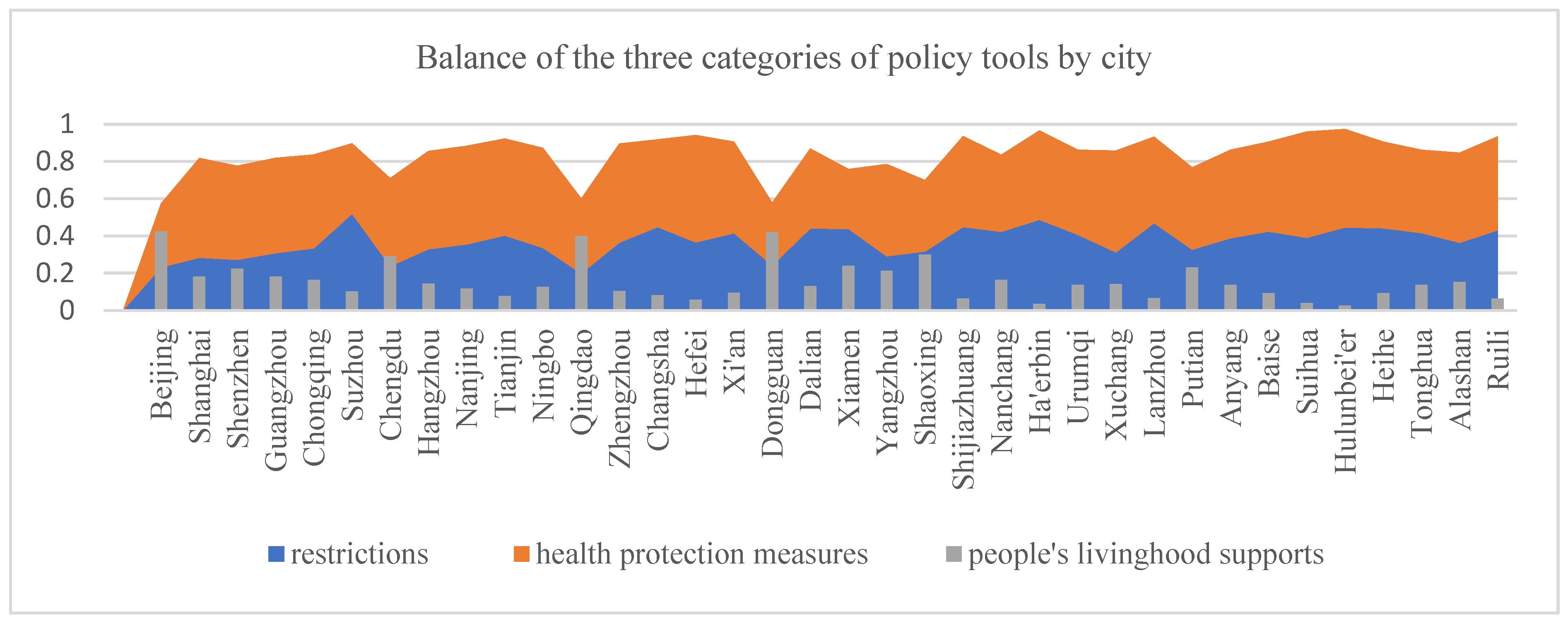
- Restrictions: These are policy tools that impose obligations, limitations, and prohibitions on individuals and collective actors [27]. These coercive measures aim to control the spread of the virus by reducing contacts and interactions. However, they can have negative effects [2] such as seriously impacting economic activity, supply chains, and public access to normal medical treatment. The restriction-based policy tools are as follows: lockdowns, quarantines, school closures, workplace and retail shop closures, canceling public events, gathering restrictions, travel restrictions, commercial activity restrictions, social distancing, mask requirements, and restrictions on government services.
- Health protection measures: These are policies aiming to protect people from the direct effects of COVID-19. These proactive measures can alter and reduce the magnitude of a pandemic [27]. Compared with restrictions, which are obligations imposed on individuals and enterprises, health protection measures are responsive policy investments by the government. This category includes the following tools: information management, public testing, contact tracing, emergency investment in health care, sanitizer policies, vaccination services, monitoring population health, social mobilization, and improving the local risk response systems.
- Socioeconomic support measures: These are policies that aim to protect the affected populations from the negative socioeconomic impacts of the pandemic and the secondary effects caused by restrictions [2]. This category consists of living/income support, debt or contract relief for households and enterprises, funding or fiscal stimulus, other work and production resumption support besides economic support, supply chain management, support for public access to normal medical treatment, other humanitarian assistance besides access to medical facilities, and the provision of e-government services.
3.2. Policy Mixes’ Tool Type Balance
3.3. Effects of Policy Mix on a City’s Pandemic Response Outcomes
- Among the policy tools, lockdowns, school closures, canceling public events, travel restrictions, social distancing, contact tracing, vaccination campaigns, improving the local risk-response systems, and supply chain management had significant negative impacts on cities’ 2-year average economic growth rates. By contrast, mask requirements, public testing, emergency investment in health care, debt/contract relief for households and enterprises, and support for public access to normal medical treatment did not have negative effects on the 2-year average economic growth rate.
- Restriction-based tools did not significantly influence the number of major outbreaks or of high-risk areas.
- Emergency investment in health care, vaccination campaigns, improving the local risk-response systems, supply chain management, and public access to normal medical treatment were negatively correlated with the numbers of major outbreaks, high-risk areas, and secondary accidents. Additionally, except for supply chain management, the others were positively correlated with the 2-year average economic growth rate.
- By comparing these three policy tool categories, we found that restrictions and socioeconomic support measures did not significantly influence the control of the pandemic. In contrast, health protection measures strongly contributed to controlling the spread of the virus. Socioeconomic support measures particularly contributed to reducing the occurrence of secondary accidents.
4. Discussion
4.1. Relation between Policy Mix and Pandemic Response Outcomes
4.2. The Importance of a Timely Lockdown
4.3. A Comprehensive Policy Mix for Compound Crises
4.4. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maggetti, M.; Trein, P. Policy integration, problem-solving, and the coronavirus disease crisis: Lessons for policy design. Policy Soc. 2022, 41, 53–67. [Google Scholar] [CrossRef]
- Capano, G.; Howlett, M.; Jarvis, D.S.L.; Ramesh, M.; Goyal, N. Mobilizing Policy (In) Capacity to Fight COVID-19: Understanding Variations in State Responses. Policy Soc. 2020, 39, 285–308. [Google Scholar] [CrossRef] [PubMed]
- Triggle, C.R.; Bansal, D.; Abu Farag, E.A.; Ding, H.; Sultan, A.A. COVID-19: Learning from Lessons To Guide Treatment and Prevention Interventions. Msphere 2020, 5, e00317-20. [Google Scholar] [CrossRef] [PubMed]
- Cairney, P. The UK government’s COVID-19 policy: Assessing evidence-informed policy analysis in real time. Br. Politics 2021, 16, 90–116. [Google Scholar] [CrossRef]
- Maor, M.; Howlett, M. Explaining variations in state COVID-19 responses: Psychological, institutional, and strategic factors in governance and public policy-making. Policy Des. Pract. 2020, 3, 228–241. [Google Scholar] [CrossRef]
- Cheng, C.; Barcelo, J.; Hartnett, A.S.; Kubinec, R.; Messerschmidt, L. COVID-19 Government Response Event Dataset (CoronaNet v.1.0). Nat. Hum. Behav. 2020, 4, 756–768. [Google Scholar] [CrossRef]
- Toshkov, D.; Carroll, B.; Yesilkagit, K. Government capacity, societal trust or party preferences: What accounts for the variety of national policy responses to the COVID-19 pandemic in Europe? J. Eur. Public Policy 2021, 29, 1009–1028. [Google Scholar] [CrossRef]
- Gonzalez-Bustamante, B. Evolution and early government responses to COVID-19 in South America. World Dev. 2021, 137, 105180. [Google Scholar] [CrossRef]
- Yan, B.; Zhang, X.M.; Wu, L.; Zhu, H.; Chen, B. Why Do Countries Respond Differently to COVID-19? A Comparative Study of Sweden, China, France, and Japan. Am. Rev. Public Adm. 2020, 50, 762–769. [Google Scholar] [CrossRef]
- Woo, J.J. Policy capacity and Singapore’s response to the COVID-19 pandemic. Policy Soc. 2020, 39, 345–362. [Google Scholar] [CrossRef]
- Mei, C.Q. Policy style, consistency and the effectiveness of the policy mix in China’s fight against COVID-19. Policy Soc. 2020, 39, 309–325. [Google Scholar] [CrossRef] [PubMed]
- Migone, A.R. The influence of national policy characteristics on COVID-19 containment policies: A comparative analysis. Policy Des. Pract. 2020, 3, 259–276. [Google Scholar] [CrossRef]
- Knill, C.; Steinebach, Y. What has happened and what has not happened due to the coronavirus disease pandemic: A systemic perspective on policy change. Policy Soc. 2022, 41, 25–39. [Google Scholar] [CrossRef]
- Capano, G. Policy design and state capacity in the COVID-19 emergency in Italy: If you are not prepared for the (un)expected, you can be only what you already are. Policy Soc. 2020, 39, 326–344. [Google Scholar] [CrossRef] [PubMed]
- Capano, G.; Howlett, M.; Jarvis, D.S.L.; Ramesh, M. Long-term policy impacts of the coronavirus: Normalization, adaptation, and acceleration in the post-COVID state. Policy Soc. 2022, 41, 1–12. [Google Scholar] [CrossRef]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef]
- OECD. The Territorial Impact of COVID-19: Managing the Crisis across Levels of Government; OECD Publishing: Paris, France, 2020. [Google Scholar] [CrossRef]
- Bouckaert, G.; Galli, D.; Kuhlmann, S.; Reiter, R.; Van Hecke, S. European Coronationalism? A Hot Spot Governing a Pandemic Crisis. Public Adm. Rev. 2020, 80, 765–773. [Google Scholar] [CrossRef]
- Nauewelaers, C.; Boekholt, P.; Mostert, B.; Cunningham, P.; Guy, K.; Hofer, R.; Rammer, C. Policy Mixes for R&D in Europe; European Commission—Directorate—General for Research: Maastricht, The Netherlands, 2009. [Google Scholar]
- Rogge, K.S.; Reichardt, K. Policy mixes for sustainability transitions: An extended concept and framework for analysis. Res. Policy 2016, 45, 132–147. [Google Scholar] [CrossRef]
- Rogge, K.S.; Kern, F.; Howlett, M. Conceptual and empirical advances in analysing policy mixes for energy transitions. Energy Res. Soc. Sci. 2017, 33, 1–10. [Google Scholar] [CrossRef]
- Schmidt, T.S.; Sewerin, S. Measuring the temporal dynamics of policy mixes—An empirical analysis of renewable energy policy mixes’ balance and design features in nine countries. Res. Policy 2019, 48, 103557. [Google Scholar] [CrossRef]
- China Center for Information Industry Development (CCID). White Paper on China’s Top 100 Digital Cities (2020). Available online: www.mtx.cn/#/report?id=684403 (accessed on 27 February 2022).
- Roberts, M.E.; Stewart, B.M.; Tingley, D. stm: An R Package for Structural Topic Models. J. Stat. Softw. 2019, 91, 1–40. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. 2020. Available online: https://www.R-project.org/ (accessed on 13 March 2022).
- Goyal, N.; Howlett, M. “Measuring the Mix” of Policy Responses to COVID-19: Comparative Policy Analysis Using Topic Modelling. J. Comp. Policy Anal. 2021, 23, 250–261. [Google Scholar] [CrossRef]
- Howlett, M. Designing Public Policies: Principles and Instruments; Routledge: London, UK; New York, NY, USA, 2010; pp. 1–236. [Google Scholar]
- Cairney, P.; Denny, E.S. Prevention Policy as the Ultimate ‘Wicked’ Problem. In Why Isn’t Government Policy More Preventive? Cairney, P., Denny, E.S., Eds.; Oxford University Press: Oxford, UK, 2020. [Google Scholar]
- Cai, C.K.; Jiang, W.Q.; Tang, N. Campaign-style crisis regime: How China responded to the shock of COVID-19. Policy Stud. 2022, 43, 599–619. [Google Scholar] [CrossRef]
- Zhao, Z.H.; Zhou, Y.; Li, W.H.; Fan, X.H.; Huang, Q.S.; Tang, Z.H.; Li, H.; Wang, J.X.; Li, J.L.; Wu, J. Discussion on China’s anti-epidemic response based on the Protocol on Prevention and Control of Coronavirus Disease 2019 from Chinese Authority. Int. J. Health Plan. Manag. 2022, 37, 1205–1220. [Google Scholar] [CrossRef] [PubMed]
- OECD. First Lessons from Government Evaluations of COVID-19 Responses: A Synthesis. 2022. Available online: www.oecd.org./coronavirus/policy-reponses/ (accessed on 12 April 2022).
- Ansell, C.; Boin, A.; Keller, A. Managing Transboundary Crises: Identifying the Building Blocks of an Effective Response System. J. Contingencies Crisis Manag. 2010, 18, 195–207. [Google Scholar] [CrossRef]
- Alkan, M.L. Viral Epidemics: Past and Future. In Managing Crises: Threats, Dilemmas, Opportunities, Springfield: Charles C Thomas; Rosenthal, U., Boin, R.A., Comfort, L.K., Eds.; Charles C Thomas: Springfield, IL, USA, 2001; pp. 267–280. [Google Scholar]
- Yuan, Z.; Dai, Z.; Chen, Y. Modelling the effects of Wuhan’s lockdown during COVID-19, China. Bull. World Health Organization. Suppl. 2020, 98, 484–494. [Google Scholar] [CrossRef]
- Phillipson, C.; Yarker, S.; Lang, L.; Doran, P.; Goff, M.; Buffel, T. COVID-19, Inequality and Older People: Developing Community-Centred Interventions. Int. J. Environ. Res. Public Health 2021, 18, 8064. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, L.; Yan, Y.; Zhou, Y.; Yin, P.; Qi, J.; Wang, L.; Pan, J.; You, J.; Yang, J. Excess mortality in Wuhan city and other parts of China during the three months of the covid-19 outbreak: Findings from nationwide mortality registries. BMJ 2022, 372, n415. [Google Scholar] [CrossRef]
- McAlearney, A.S.; Gaughan, A.A.; MacEwan, S.R.; Gregory, M.E.; Rush, L.J.; Volney, J.; Panchal, A.R. Pandemic Experience of First Responders: Fear, Frustration, and Stress. Int. J. Environ. Res. Public Health 2022, 19, 4693. [Google Scholar] [CrossRef]
- OECD. The Changing Face of Strategic Crisis Management. In OECD Reviews of Risk Management Policies; OECD Publishing: Paris, France, 2015. [Google Scholar] [CrossRef]
- OECD. Tackling the mental health impact of the COVID-19 crisis: An integrated, whole-of-society response. In OECD Policy Responses to Coronavirus (COVID-19); OECD Publishing: Paris, France, 2021. [Google Scholar] [CrossRef]
- Howlett, M.; Rayner, J. Design Principles for Policy Mixes: Cohesion and Coherence in ‘New Governance Arrangements’. Policy Soc. 2007, 26, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Howlett, M.; How, Y.P.; Rio, P.D. The parameters of policy portfolios: Verticality and horizontality in design spaces and their consequences for policy mix formulation. Environ. Plan. 2015, 33, 1233–1245. [Google Scholar] [CrossRef]
- Tonon, G. Integrated Methods in Research. In Handbook of Research Methods in Health Social Sciences; Liamputtong, P., Ed.; Springer Singapore: Singapore, 2019; pp. 681–694. [Google Scholar]
- Dooren, W.V.; Noordegraaf, M. Staging Science: Authoritativeness and Fragility of Models and Measurement in the COVID-19 Crisis. SocArXiv 2020, 80, 610–615. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Policy Tool | Illustrative Action | Prevalence |
|---|---|---|
| 1. Information management | Providing public information; requiring residents to report to their communities if they had been to risk areas | 0.104059 |
| 2. Monitoring population health | Measuring temperatures; checking health QR codes and travel codes | 0.085552 |
| 3. Mask requirements | Mask requirements in public places and collective locales such as workplaces, buses, subways, and taxis | 0.069997 |
| 4. Sanitizer policies | Disinfections in public places and collective locales; frequent hand-washing campaigns | 0.069543 |
| 5. Public testing | Mandated nucleic acid testing for urban residents every one to three days | 0.067159 |
| 6. Quarantines | Mandated isolation for close and indirect contacts; isolation or home quarantine for travelers | 0.066421 |
| 7. Gathering restrictions | Restrict gatherings to a maximum of five people; ban all social gatherings | 0.064547 |
| 8. Travel restrictions | Inner city traffic restrictions; cancel interregional travels | 0.064093 |
| 9. Contact tracing | Epidemiological survey professionals question individuals and analyze travel information using big data methods to determine virus spread paths and identify close and indirect contacts | 0.061482 |
| 10. Social distancing | Keep one meter distance in public or collective places | 0.052455 |
| 11. Vaccination campaigns | Set up free vaccination sites in individual communities; require local cadres, social workers, and medical professionals to visit households to mobilize people for COVID-19 vaccine uptake | 0.040704 |
| 12. Work and production resumption supports other than economic support | Facilitate permit approval for logistics vehicles; simplify administrative examination and approval procedures; provide employment recruitment services for enterprises | 0.029407 |
| 13. Humanitarian assistance other than access to medical facilities | Open psychological comfort hotlines; local cadres and social workers visit vulnerable groups such as elders, disabled, and migrants | 0.026284 |
| 14. Supply chain management | Enacting material supply plans; ensuring smooth transportation of medical materials and life supplies | 0.021913 |
| 15. Emergency investment in health care | Booster medical supplies; purchase protective equipment for health staff; support manufacturing of testing equipment | 0.021459 |
| 16. Improving the local risk response system | Require local governments or enterprises to improve emergency plans; enhance emergency drills and local risk screening | 0.018904 |
| 17. Restrictions on commercial activities | Limiting customer or visitor flow in shopping malls, supermarkets, cinemas, parks, and tourist spots | 0.01669 |
| 18. Social mobilization | Appeal to the voluntary participation of individuals and businesses to help fight the pandemic | 0.015782 |
| 19. Funding or fiscal stimulus | Release funds to alleviate the economic impact of COVID-19; tax reduction and exemption | 0.015441 |
| 20. Cancelling public events | Postpone sporting competitions; cancel expositions and festivities | 0.01442 |
| 21. Promoting e-government services | Provide online government services such as social insurance and online administrative examination and approval | 0.013057 |
| 22. Workplace and retail shops closures | Close retail outlets until further notice; permit only delivery and take-out at restaurants | 0.012433 |
| 23. Living or income support | Distribute daily necessities to elders, disabled persons, and migrants; distribute consumption coupons | 0.011467 |
| 24. Lockdowns | Full-scale lockdowns; district (partial) lockdowns | 0.009878 |
| 25. Supporting public access to normal medical treatment; | Open green channels for dialysis patients, cancer patients, and pregnant women for medical treatment; inform doctors to prescribe adequate medication for particular patients during the period of lockdown | 0.009424 |
| 26. Debt/contract relief for households and enterprises | Postpone households’ and enterprises’ debt and rent payments for three months; rent exemption in the period of lockdown | 0.007777 |
| 27. School closures | Close schools and universities in the period of lockdown | 0.005166 |
| 28. Restrictions on government services | Close petition reception; close marriage registration services | 0.004485 |
| N-Outbreak | N-High Risk_Areas | N-SEC. Accidents | ECO_RATE | ||
|---|---|---|---|---|---|
| Restrictions | Lockdowns | 0.152 | 1.975 | 1.010 | −0.006 ** |
| (0.195) | (1.551) | (0.807) | (0.002) | ||
| Quarantines | −0.036 | 0.038 | −0.095 | −0.000 | |
| (0.045) | (0.360) | (0.188) | (0.000) | ||
| School closures | −0.391 | −4.433 | 0.560 | −0.032 ** | |
| (1.071) | (8.530) | (4.439) | (0.009) | ||
| Workplace and retail shops closures | −0.231 | −0.606 | −0.806 | 0.001 | |
| (0.158) | (1.258) | (0.655) | (0.001) | ||
| Cancelling public events | 0.042 | 0.912 | 1.171 | −0.006 ** | |
| (0.211) | (1.682) | (0.875) | (0.002) | ||
| Gathering restrictions | −0.039 | −0.676 | −0.151 | −0.001 | |
| (0.094) | (0.748) | (0.389) | (0.001) | ||
| Travel restrictions | 0.100 | 0.412 | 0.039 | −0.004 ** | |
| (0.131) | (1.047) | (0.545) | (0.001) | ||
| Restriction on commercial activities | 0.011 | −0.125 | −0.533 | 0.003 | |
| (0.168) | (1.339) | (0.697) | (0.001) | ||
| Social distancing | −0.042 | −0.551 | 0.753 | −0.009 ** | |
| (0.324) | (2.578) | (1.342) | (0.003) | ||
| Mask requirements | 0.110 | −0.086 | −0.611 | 0.009 ** | |
| (0.263) | (2.096) | (1.091) | (0.002) | ||
| Restrictions on government services | 0.323 | −0.171 | 0.547 | 0.003 | |
| (0.188) | (1.494) | (0.778) | (0.002) | ||
| Health protection Measures | Information management | −0.024 | 0.026 | 0.057 | 0.000 |
| (0.028) | (0.226) | (0.118) | (0.000) | ||
| Public testing | 0.011 | −0.204 | −0.214 | 0.003 ** | |
| (0.104) | (0.826) | (0.430) | (0.001) | ||
| Contact tracing | −0.117 | 0.133 | 0.546 | −0.007 ** | |
| (0.238) | (1.895) | (0.986) | (0.002) | ||
| Emergency investment in health care | −0.184 | −0.434 *** | −0.373 ** | 0.005 ** | |
| (0.129) | (1.031) | (0.537) | (0.001) | ||
| Sanitizer policies | −0.000 | 0.815 | −0.252 | 0.002 | |
| (0.151) | (1.200) | (0.625) | (0.001) | ||
| Vaccination campaigns | −0.016 | −0.230 ** | −0.062 *** | −0.012 ** | |
| (0.032) | (0.256) | (0.133) | (0.000) | ||
| Monitoring population health | 0.068 | −0.046 | −0.053 | 0.000 | |
| (0.052) | (0.411) | (0.214) | (0.000) | ||
| Social mobilizations | 0.119 | 0.826 | 0.211 | 0.002 | |
| (0.188) | (1.497) | (0.779) | (0.002) | ||
| Improving the local risk response system | −0.080 | −0.558 ** | −0.293 ** | −0.003 * | |
| (0.164) | (1.307) | (0.680) | (0.001) | ||
| Socioeconomic supports | Living or income support | 0.022 | −0.911 | 0.378 | −0.003 |
| (0.161) | (1.282) | (0.667) | (0.001) | ||
| Debt/contract relief for households and enterprises | 0.171 | 0.853 | −0.715 | 0.014 ** | |
| (0.449) | (3.577) | (1.862) | (0.004) | ||
| Funding or fiscal stimulus | −0.022 | −0.547 | −0.209 | −0.001 | |
| (0.099) | (0.785) | (0.409) | (0.001) | ||
| Work and production resumption supports other than economic support | −0.005 | 0.848 | 0.201 | 0.000 | |
| (0.101) | (0.808) | (0.420) | (0.001) | ||
| Supply chain management | −0.003 | −0.236 | −0.032 ** | −0.009 ** | |
| (0.282) | (2.243) | (1.167) | (0.002) | ||
| Supporting public access to normal medical treatment | −0.046 | −0.052 *** | −1.108 ** | 0.010 ** | |
| (0.297) | (2.369) | (1.233) | (0.002) | ||
| Humanitarian assistance other than access to medical facilities | 0.000 | −0.169 | −0.396 | 0.000 | |
| (0.063) | (0.503) | (0.262) | (0.001) | ||
| Promoting e-government services | 0.142 | 1.002 | −0.222 | 0.000 | |
| (0.115) | (0.918) | (0.478) | (0.001) | ||
| Control Variables | GDP | 0.000 | 0.000 | 0.000 | 0.000 |
| (0.000) | (0.001) | (0.000) | (0.000) | ||
| Permanent population | −0.001 | −0.005 | −0.005 | 0.000 | |
| (0.001) | (0.009) | (0.005) | (0.000) | ||
| University | 0.015 | 0.154 | 0.098 | 0.000 | |
| (0.035) | (0.279) | (0.145) | (0.000) | ||
| Digital_city | 0.017 | 0.069 | −0.094 | 0.001 *** | |
| (0.027) | (0.214) | (0.111) | (0.000) | ||
| _cons | −1.385 | −10.244 | 5.165 | −0.014 | |
| (2.613) | (20.818) | (10.835) | (0.021) | ||
| p | 0.346 | 0.878 | 0.716 | 0.102 | |
| r2 | 0.951 | 0.836 | 0.890 | 0.982 | |
| F | 1.830 | 0.479 | 0.757 | 5.071 | |
| Policy Outcomes | Virus Spread Controlling | Secondary Disasters | Economic Consequences | |
|---|---|---|---|---|
| Policy Strategy | ||||
| 1. Integrated health protection and people’s livelihood support | Positive | Negative | Negative | |
| 2. Integrated restrictions and health protection measures | Positive | Positive | Positive | |
| 3. Restriction-oriented policy response | No correlation | Positive | Positive | |
| 4. Health protection-oriented strategy | Positive | No correlation | No correlation | |
| 5. Comprehensive policy mix | Positive | Negative | Negative | |
| Date | 12 March | 13 March | 14 March | 15 March | 16 March | 20 March | 21 March | 28 March | 1 April | 26 April | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cases | |||||||||||
| Shenzhen | 66 | 86 | 60 | 92 | 91 | 44 | 28 | 9 | 2 | 0 | |
| Shanghai | 65 | 169 | 139 | 202 | 158 | 758 | 896 | 4477 | 24,943 | 16,980 | |
| Lockdown | Shenzhen, start | Shenzhen, end | Shanghai, start | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, C.; Xu, T.; Ying, Z.; Li, H. How Policy Mix Choices Affect the COVID-19 Pandemic Response Outcomes in Chinese Cities: An Empirical Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8094. https://doi.org/10.3390/ijerph19138094
Shi C, Xu T, Ying Z, Li H. How Policy Mix Choices Affect the COVID-19 Pandemic Response Outcomes in Chinese Cities: An Empirical Analysis. International Journal of Environmental Research and Public Health. 2022; 19(13):8094. https://doi.org/10.3390/ijerph19138094
Chicago/Turabian StyleShi, Chunyu, Tao Xu, Zhihang Ying, and Huan Li. 2022. "How Policy Mix Choices Affect the COVID-19 Pandemic Response Outcomes in Chinese Cities: An Empirical Analysis" International Journal of Environmental Research and Public Health 19, no. 13: 8094. https://doi.org/10.3390/ijerph19138094