Article Text

Statistics from Altmetric.com
A 65-year-old obese male, with no other comorbidities, was admitted to our intensive care unit for acute respiratory failure due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. The patient was mechanically ventilated (intermittent positive pressure ventilation autoflow mode with tidal volume of 6 mL/kg, positive end expiratory pressure (PEEP) 12 cmH2O, respiratory rate 20 breaths/min and fractional inspired oxygen (FiO2) to the lowest level to maintain arterial pO2 in a range of 55–60 mm Hg) for 7 days before his condition abruptly worsened. He became haemodynamically unstable with changes in the cardiac electrical activity and hypotension unresponsive to catecholamines. An initial plain chest X-ray revealed widespread subcutaneous emphysema. Chest-CT demonstrated a massive tension pneumomediastinum. Mediastinal decompression was performed via two incisions, one at the sternal notch and one below the xiphoid process (figure 1). The posterior wall of the sternum was liberated of pericardial fat using blunt dissection with fingers and peanut sponge forceps. A chest tube was placed from the inferior incision and connected to a suction system to avoid any recurrence (figure 2). A laminar drain was inserted from the superior incision into the pretracheal space and connected to a closed system to reduce aerosolisation (Biotrol System 2 bag, B. Braun Medical). After the procedure the ventilation mode was modified, reducing the PEEP to 8 cmH2O and respiratory rate to 16 increasing the FiO2 to 80%. The patient was haemodynamically stable and remained on mechanical ventilation for 6 more days followed by cycles of non-invasive ventilation for a further 5 days at which point the two tubes were removed and the incisions closed with simple interrupted sutures. He was transferred to a respiratory ward where he went on to make a full recovery and was discharged 2 weeks later. Tension pneumomediastinum is a life-threatening condition especially in critically ill patients. One of the most common situations in which it occurs is prolonged invasive and non-invasive ventilation with high end-expiratory pressure.1 Due to the high number of patients with SARS-CoV-2 related respiratory infections being treated with this type of ventilation, we are seeing an increasing number of tension pneumomediastinum cases.
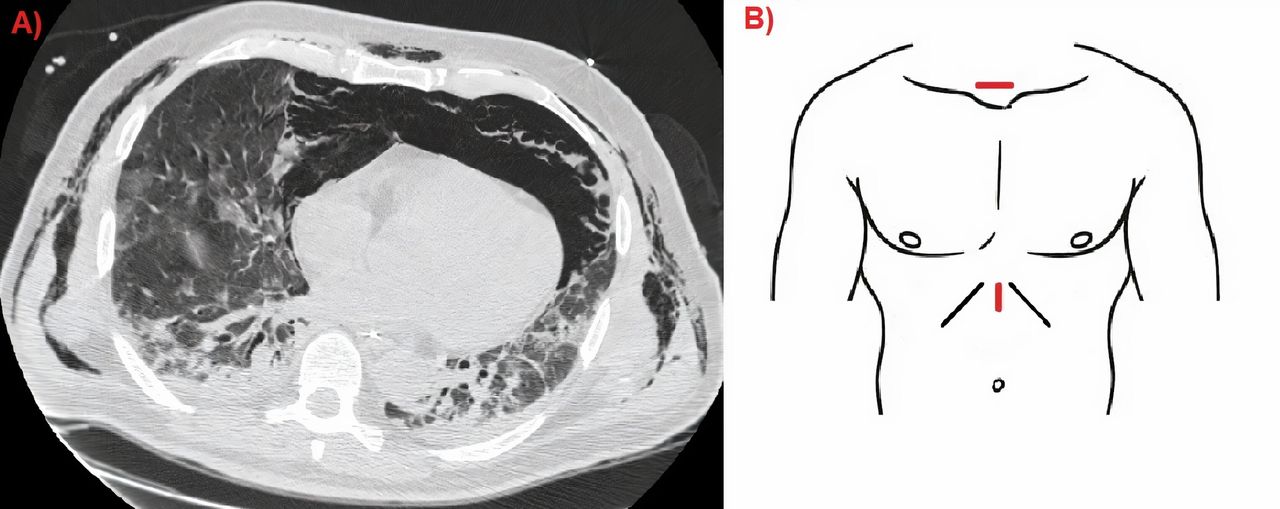
(A) Chest-CT scan of a patient with COVID-19 with a tension pneumomediastinum. (B) Scheme of the surgical incision to decompress the mediastinum.

{kind=link}
{kind=link}
CT scan showing significant radiological improvement with correct placement of the chest drain. (1) Chest tube. (2) Nasogastric tube.
Air leakage from the alveolus occurs due to a pressure gradient between the alveolus and the perivascular sheaths. If the pressure gradient is maintained, the air tracks along the vascular sheaths to the mediastinum.1 2 Due to increasing mediastinal pressure a compression of the great vessels occurs, leading to decreased venous return, hypotension and finally to cardiac collapse.3 The initial diagnosis may be difficult due to associated subcutaneous emphysema that covers the underlying disease on chest X-ray. Treatment may be conservative, reducing the airway pressures, allowing permissive hypercapnia and increasing the oxygen percentage of the airflow to denitrogenate the mediastinal space.1 2 Considering the fragility of patients with COVID-19, this approach is often insufficient, thus surgery may be necessary. In our experience, the approach we described immediately improves the clinical condition of the patient with very low risks of complications, even for an inexperienced thoracic surgeon.(figure 2)
Footnotes
Contributors Conception and design: AC, VP, APC; administrative support: FS, VP; provision of study materials or patients: AC, MS; collection and assembly of data: AC, APC; data analysis and interpretation: APC, MS, FS; manuscript writing: AC, VP, APC; final approval of manuscript: all authors. All authors discussed the results and contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves