D-Dimers Level as a Possible Marker of Extravascular Fibrinolysis in COVID-19 Patients

 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Methods
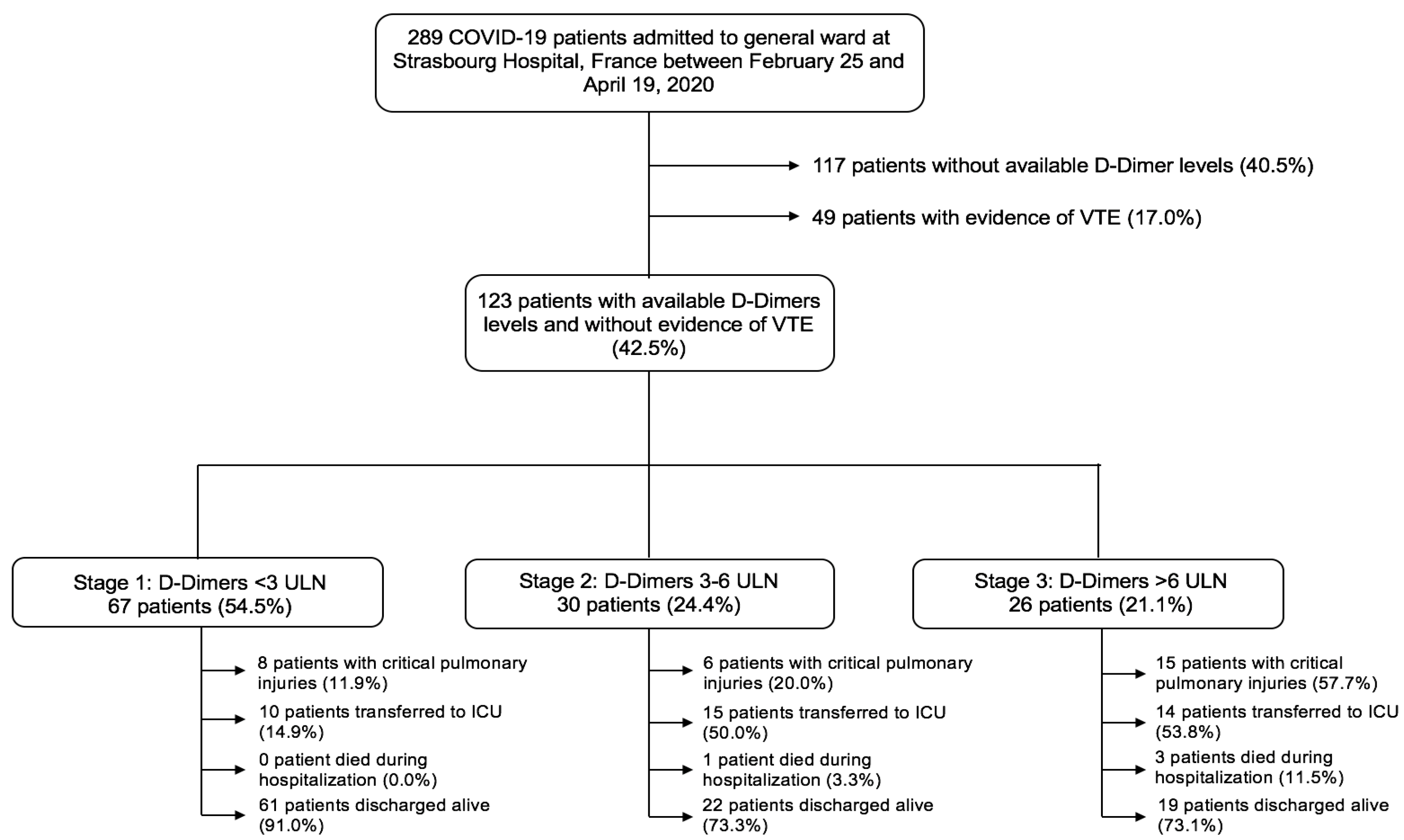
2.1. Study Population
2.2. Data Collection
2.3. Study Definitions
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
3.1. Characteristics
3.2. Chest CT Findings, Lactates and Oxygen Demand
3.3. Predictors of Critical Pulmonary Injuries
3.4. Outcomes
4. Discussion
4.1. Extravascular Fibrinolysis during COVID-19
4.2. Clinical Implications
4.3. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lim, W.; van der Eerden, M.M.; Laing, R.; Boersma, W.; Karalus, N.; Town, G.; Lewis, S.; Macfarlane, J. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Cooley, C.M.; Marrie, R.J.; Kapoor, W.N. A Prediction Rule to Identify Low-Risk Patients with Community-Acquired Pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.D.; Singanayagam, A.; Scally, C.; Hill, A.T. Admission D-dimer can identify low-risk patients with community-acquired pneumonia. Ann. Emerg. Med. 2009, 53, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Querol-Ribelles, J.M.; Tenias, J.M.; Grau, E.; Querol-Borras, J.M.; Climent, J.L.; Gomez, E.; Martinez, I. Plasma d-dimer levels correlate with outcomes in patients with community-acquired pneumonia. Chest 2004, 126, 1087–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.F.; Su, F.; Lin, X.J.; Dai, B.; Kong, L.F.; Zhao, H.W.; Kang, J. Serum D-dimer changes and prognostic implication in 2009 novel influenza A(H1N1). Thromb. Res. 2011, 127, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Giannis, D.; Ziogas, I.A.; Gianni, P. Coagulation disorders in coronavirus infected patients: COVID-19, SARS-CoV-1, MERS-CoV and lessons from the past. J. Clin. Virol. 2020, 127, 104362. [Google Scholar] [CrossRef]
- Marchandot, B.; Sattler, L.; Jesel, L.; Matsushita, K.; Schini-Kerth, V.; Grunebaum, L.; Morel, O. COVID-19 Related Coagulopathy: A Distinct Entity? J. Clin. Med. 2020, 9, 1651. [Google Scholar] [CrossRef]
- Marchandot, B.; Trimaille, A.; Curtiaud, A.; Matsushita, K.; Jesel, L.; Morel, O. Thromboprophylaxis: Balancing Evidence and Experience During the COVID-19 Pandemic. J. Thromb. Thrombolysis 2020, 50, 799–808. [Google Scholar] [CrossRef]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Fagot Gandet, F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Leonard-Lorant, I.; Delabranche, X.; Severac, F.; Helms, J.; Pauzet, C.; Collange, O.; Schneider, F.; Labani, A.; Bilbault, P.; Moliere, S.; et al. Acute Pulmonary Embolism in COVID-19 Patients on CT Angiography and Relationship to D-Dimer Levels. Radiology 2020, 201561. [Google Scholar] [CrossRef] [Green Version]
- Fauvel, C.; Weizman, O.; Trimaille, A.; Mika, D.; Pommier, T.; Pace, N.; Douair, A.; Barbin, E.; Fraix, A.; Bouchot, O.; et al. Pulmonary embolism in COVID-19 patients: A French multicentre cohort study. Eur. Heart J. 2020, 41, 3058–3068. [Google Scholar] [CrossRef] [PubMed]
- Trimaille, A.; Curtiaud, A.; Marchandot, B.; Matsushita, K.; Sato, C.; Leonard-Lorant, I.; Sattler, L.; Grunebaum, L.; Ohana, M.; Von Hunolstein, J.J.; et al. Venous thromboembolism in non-critically ill patients with COVID-19 infection. Thromb. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, R.C. COVID-19 update: Covid-19-associated coagulopathy. J. Thromb. Thrombolysis 2020, 50, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Yan, X.; Fan, Q.; Liu, H.; Liu, X.; Liu, Z.; Zhang, Z. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J. Thromb. Haemost. 2020, 18, 1324–1329. [Google Scholar] [CrossRef]
- Thachil, J. All those D-dimers in COVID-19. J. Thromb. Haemost. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Favaloro, E.J. D-dimer is Associated with Severity of Coronavirus Disease 2019: A Pooled Analysis. Thromb. Haemost. 2020, 120, 876–878. [Google Scholar] [CrossRef] [Green Version]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, C.; Dreyfus, I.; Driggin, E.; Der Nigoghossian, C.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-up. J. Am. Coll. Cardiol. 2020. [Google Scholar] [CrossRef]
- Wagers, S.S.; Norton, R.J.; Rinaldi, L.M.; Bates, J.H.T.; Sobel, B.E.; Irvin, C.G. Extravascular fibrin, plasminogen activator, plasminogen activator inhibitors, and airway hyperresponsiveness. J. Clin. Investig. 2004, 114, 104–111. [Google Scholar] [CrossRef] [Green Version]
- WHO 2019 nCoV Surveillance Guidance. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/331506/WHO-2019-nCoV-SurveillanceGuidance-2020.6-eng.pdf?sequence=1&isAllowed=y (accessed on 21 July 2020).
- Thachil, J.; Cushman, M.; Srivastava, A. A Proposal for Staging COVID-19 Coagulopathy. J. Thromb. Haemost. 2020. [Google Scholar] [CrossRef]
- Revel, M.-P.; Parkar, A.P.; Prosch, H.; Silva, M.; Sverzellati, N.; Gleeson, F.; Brady, A. COVID-19 patients and the radiology department—Advice from the European Society of Radiology (ESR) and the European Society of Thoracic Imaging (ESTI). Eur. Radiol. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lillicrap, D. Disseminated intravascular coagulation in patients with 2019-nCoV pneumonia. J. Thromb. Haemost. 2020, 18, 786–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poissy, J.; Goutay, J.; Caplan, M.; Parmentier Duburcq, T.; Lassalle, F.; Jeanpierre, E.; Rauch, A.; Labreuche, J.; Susen, S. Pulmonary Embolism in COVID-19 Patients: Awareness of an Increased Prevalence. Circulation 2020. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- McGonagle, D.; O’Donnell, J.S.; Sharif, K.; Emery, P.; Bridgewood, C. Immune mechanisms of pulmonary intravascular coagulopathy in COVID-19 pneumonia. Lancet Rheumatol. 2020. [Google Scholar] [CrossRef]
- Günther, A.; Mosavi, P.; Heinemann, S.; Ruppert, C.; Muth, H.; Markart, P.; Grimminger, F.; Walmrath, D.; Temmesfeld-Wollbrück, B.; Seeger, W. Alveolar fibrin formation caused by enhanced procoagulant and depressed fibrinolytic capacities in severe pneumonia. Comparison with the acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2020, 161, 454–462. [Google Scholar] [CrossRef]
- Fuchs-Buder, T.; de Moerloose, P.; Ricou, B.; Reber, G.; Vifian, C.; Nicod, L.; Romand, J.A.; Suter, P.M. Time course of procoagulant activity and D dimer in bronchoalveolar fluid of patients at risk for or with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 1996, 153, 163–167. [Google Scholar] [CrossRef]
- Seeger, W.; Elssner, A.; Günther, A.; Krämer, H.J.; Kalinowski, H.O. Lung surfactant phospholipids associate with polymerizing fibrin: Loss of surface activity. Am. J. Respir. Cell Mol. Biol. 1993, 9, 213–220. [Google Scholar] [CrossRef]
- Hofstra, J.-J.H.; Haitsma, J.J.; Juffermans, N.P.; Levi, M.; Schultz, M.J. The role of bronchoalveolar hemostasis in the pathogenesis of acute lung injury. Semin. Thromb. Hemost. 2008, 34, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Shetty, S.; Padijnayayveetil, J.; Tucker, T.; Stankowska, D.; Idell, S. The fibrinolytic system and the regulation of lung epithelial cell proteolysis, signaling, and cellular viability. Am. J. Physiol. Lung Cell. Mol. Physiol. 2008, 295, 967–975. [Google Scholar] [CrossRef] [PubMed]
- Francis, C.W.; Kessler, C.M.; Goldhaber, S.Z.; Kovacs, M.J.; Monreal, M.; Huisman, M.V.; Bergqvist, D.; Ortel, T.L.; Spyropoulos, A.C.; Pabinger, I.; et al. Treatment of venous thromboembolism in cancer patients with dalteparin for up to 12 months: The DALTECAN Study. J. Thromb. Haemost. 2015, 13, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- Turato, G.; Zuin, R.; Saetta, M. Pathogenesis and pathology of COPD. Respiration 2001, 68, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Henry, B.M. Chronic obstructive pulmonary disease is associated with severe coronavirus disease 2019 (COVID-19). Respir. Med. 2020, 167, 105941. [Google Scholar] [CrossRef] [PubMed]
- Matthay, M.A.; Zemans, R.L.; Zimmerman, G.A.; Arabi, Y.M.; Beitler, J.R.; Mercat, A.; Herridge, M.; Randolph, A.G.; Calfee, C.S. Acute respiratory distress syndrome. Nat. Rev. Dis. Primer 2019, 5, 1–22. [Google Scholar] [CrossRef]
- Hardy, M.; Lecompte, T.; Douxfils, J.; Lessire, S.; Dogné, J.M.; Chatelain, B.; Testa, S.; Gouin-Thibault, I.; Gruel, Y.; Medcalf, R.L.; et al. Management of the thrombotic risk associated with COVID-19: Guidance for the hemostasis laboratory. Thromb. J. 2020, 18, 17. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| D-Dimers Staging at Peak | p Value | |||
|---|---|---|---|---|
| Stage 1 <3 ULN (n = 67) | Stage 2 3–6 ULN (n = 30) | Stage 3 >6 ULN (n = 26) | ||
| Age—yr | 57 ± 16 | 62 ± 16 | 63 ± 16 | 0.120 |
| Male—n (%) | 35 (52.2) | 16 (53.3) | 21 (80.8) | 0.035 |
| BMI > 30 kg/m2—n (%) | 21 (35.6) | 12 (44.4) | 7 (26.9) | 0.412 |
| Hypertension—n (%) | 23 (34.3) | 17 (56.7) | 12 (46.2) | 0.109 |
| Diabetes—n (%) | 9 (13.4) | 7 (23.3) | 3 (11.5) | 0.379 |
| Dyslipidemia—n (%) | 14 (20.9) | 8 (26.7) | 10 (38.5) | 0.222 |
| Smoking—n (%) | 3 (4.5) | 0 (0.0) | 1 (3.8) | 0.507 |
| Heart Failure—n (%) | 1 (1.5) | 0 (0.0) | 4 (15.4) | 0.004 |
| CKD a—n (%) | 2 (3.0) | 2 (6.7) | 4 (15.4) | 0.094 |
| COPD—n (%) | 9 (13.4) | 0 (0.0) | 0 (0.0) | 0.017 |
| Active cancer—n (%) | 1 (1.5) | 2 (6.7) | 0 (0.0) | 0.206 |
| Thromboprophylaxis—n (%) | 66 (98.5) | 30 (100.0) | 25 (96.2) | 0.521 |
| Standard—n (%) | 41 (61.2) | 21 (70) | 10 (38.5) | 0.047 |
| Reinforced—n (%) | 12 (17.9) | 5 (16.7) | 7 (26.9) | 0.556 |
| Therapeutic—n (%) | 13 (19.4) | 4 (13.3) | 8 (30.8) | 0.260 |
| D-Dimers Staging at Peak | p Value | |||
|---|---|---|---|---|
| Stage 1 <3 ULN (n = 67) | Stage 2 3–6 ULN (n = 30) | Stage 3 >6 ULN (n = 26) | ||
| At admission | ||||
| Lactate—mmol/L | 0.95 ± 0.29 | 1.22 ± 0.73 | 1.39 ± 0.67 | 0.010 |
| Leukocytes—×109 per L | 6.87 ± 3.27 | 6.87 ± 2.37 | 7.63 ± 3.70 | 0.563 |
| Lymphocytes—×109 per L | 1.13 ± 0.50 | 0.92 ± 0.31 | 0.81 ± 0.39 | 0.003 |
| Platelet—×109 per L | 224 ± 104 | 203 ± 81 | 229 ± 89 | 0.539 |
| CRP—mg/L | 89 ± 78 | 104 ± 62 | 152 ± 92 | 0.003 |
| Fibrinogen—g/L | 6.2 ± 1.8 | 6.5 ± 1.3 | 6.6 ± 1.1 | 0.636 |
| aPTT—IU | 1.1 ± 0.2 | 1.0 ± 0.1 | 1.3 ± 0.7 | 0.208 |
| eGFR—mL/min/1.73m2 | 90 ± 23 | 70 ± 26 | 67 ± 31 | 0.009 |
| BNP—pg/mL | 75 ± 123 | 78 ± 106 | 669 ± 1253 | 0.001 |
| During Hospitalization | ||||
| Leukocytes peak—×109 per L | 11.30 ± 25.12 | 11.48 ± 5.74 | 13.83 ± 8.48 | 0.843 |
| Platelets peak—×109 per L | 399 ± 190 | 401 ± 137 | 415 ± 157 | 0.923 |
| CRP peak—mg/L | 125 ± 88 | 155 ± 88 | 202 ± 91 | 0.001 |
| Fibrinogen peak—g/L | 6.6 ± 1.6 | 7.5 ± 1.7 | 8.1 ± 2.6 | 0.036 |
| D-Dimers Staging at Peak | p Value | |||
|---|---|---|---|---|
| Stage 1 <3 ULN (n = 67) | Stage 2: 3–6 ULN (n = 30) | Stage 3 >6 ULN (n = 26) | ||
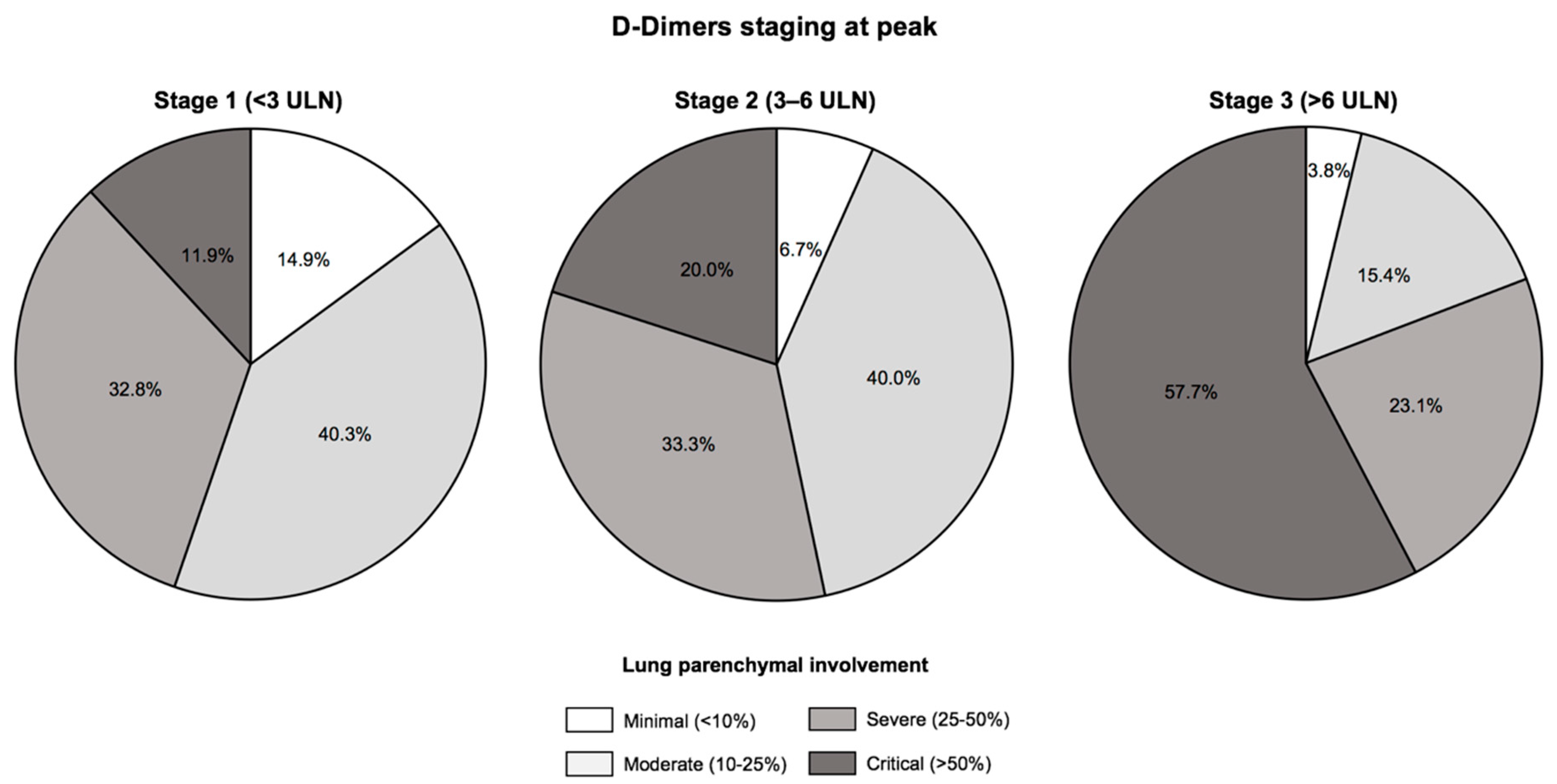
| Critical pulmonary injuries (>50%)—n (%) | 8 (11.9) | 6 (20.0) | 15 (57.7) | <0.001 |
| Transfer to ICU or in-hospital death—n (%) | 10 (14.9) | 15 (50.0) | 15 (57.7) | <0.001 |
| ICU Transfer—n (%) | 10 (14.9) | 14 (46.7) | 14 (53.8) | <0.001 |
| In-hospital death—n (%) | 0 (0.0) | 1 (3.3) | 3 (11.5) | 0.019 |
| Maximal oxygen flow rate—L/min | 0.8 ± 0.3 | 2.1 ± 0.4 | 7.4 ± 4.6 | <0.001 |
| Discharged alive—n (%) | 61 (98.4) | 22 (84.6) | 19 (82.6) | 0.018 |
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| OR [95%CI] | p Value | OR [95%CI] | p Value | |
| Age | 1.00 [0.98–1.02] | 0.563 | ||
| Male | 1.59 [0.78–3.24] | 0.193 | ||
| BNP at admission | 1.00 [0.99–1.00] | 0.940 | ||
| Fibrinogen at admission | 1.46 [1.03–2.06] | 0.030 | ||
| Fibrinogen at peak | 1.22 [0.96–1.55] | 0.095 | ||
| CRP at admission | 1.01 [1.00–1.01] | <0.001 | ||
| CRP at peak | 1.00 [1.00–1.01] | <0.001 | 1.00 [0.99–1.00] | 0.288 |
| Leukocytes at admission | 1.06 [0.96–1.18] | 0.222 | ||
| Leukocytes at peak | 1.00 [0.98–1.02] | 0.503 | ||
| Lymphocytes at admission | 0.38 [0.15–0.92] | 0.033 | 0.79 [0.24–2.52] | 0.694 |
| Procalcitonin at admission | 0.96 [0.84–1.09] | 0.582 | ||
| D-Dimers staging on admission | 2.37 [1.35–4.16] | 0.003 | ||
| D-Dimers staging at peak | 3.16 [1.82–5.48] | <0.001 | 2.70 [1.50–4.86] | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trimaille, A.; Thachil, J.; Marchandot, B.; Curtiaud, A.; Leonard-Lorant, I.; Carmona, A.; Matsushita, K.; Sato, C.; Sattler, L.; Grunebaum, L.; et al. D-Dimers Level as a Possible Marker of Extravascular Fibrinolysis in COVID-19 Patients. J. Clin. Med. 2021, 10, 39. https://doi.org/10.3390/jcm10010039
Trimaille A, Thachil J, Marchandot B, Curtiaud A, Leonard-Lorant I, Carmona A, Matsushita K, Sato C, Sattler L, Grunebaum L, et al. D-Dimers Level as a Possible Marker of Extravascular Fibrinolysis in COVID-19 Patients. Journal of Clinical Medicine. 2021; 10(1):39. https://doi.org/10.3390/jcm10010039
Chicago/Turabian StyleTrimaille, Antonin, Jecko Thachil, Benjamin Marchandot, Anaïs Curtiaud, Ian Leonard-Lorant, Adrien Carmona, Kensuke Matsushita, Chisato Sato, Laurent Sattler, Lelia Grunebaum, and et al. 2021. "D-Dimers Level as a Possible Marker of Extravascular Fibrinolysis in COVID-19 Patients" Journal of Clinical Medicine 10, no. 1: 39. https://doi.org/10.3390/jcm10010039