
COVID-19 Vaccination Attitudes, Perceptions, and Side Effect Experiences in Malaysia: Do Age, Gender, and Vaccine Type Matter?

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population and Sample Size
2.3. Ethical Approval
2.4. Study Instrument
2.5. Statistical Analysis
3. Results
3.1. General Information of Study Participants
3.2. Vaccination Attitudes and Adherence to Preventive Measures among Study Participants
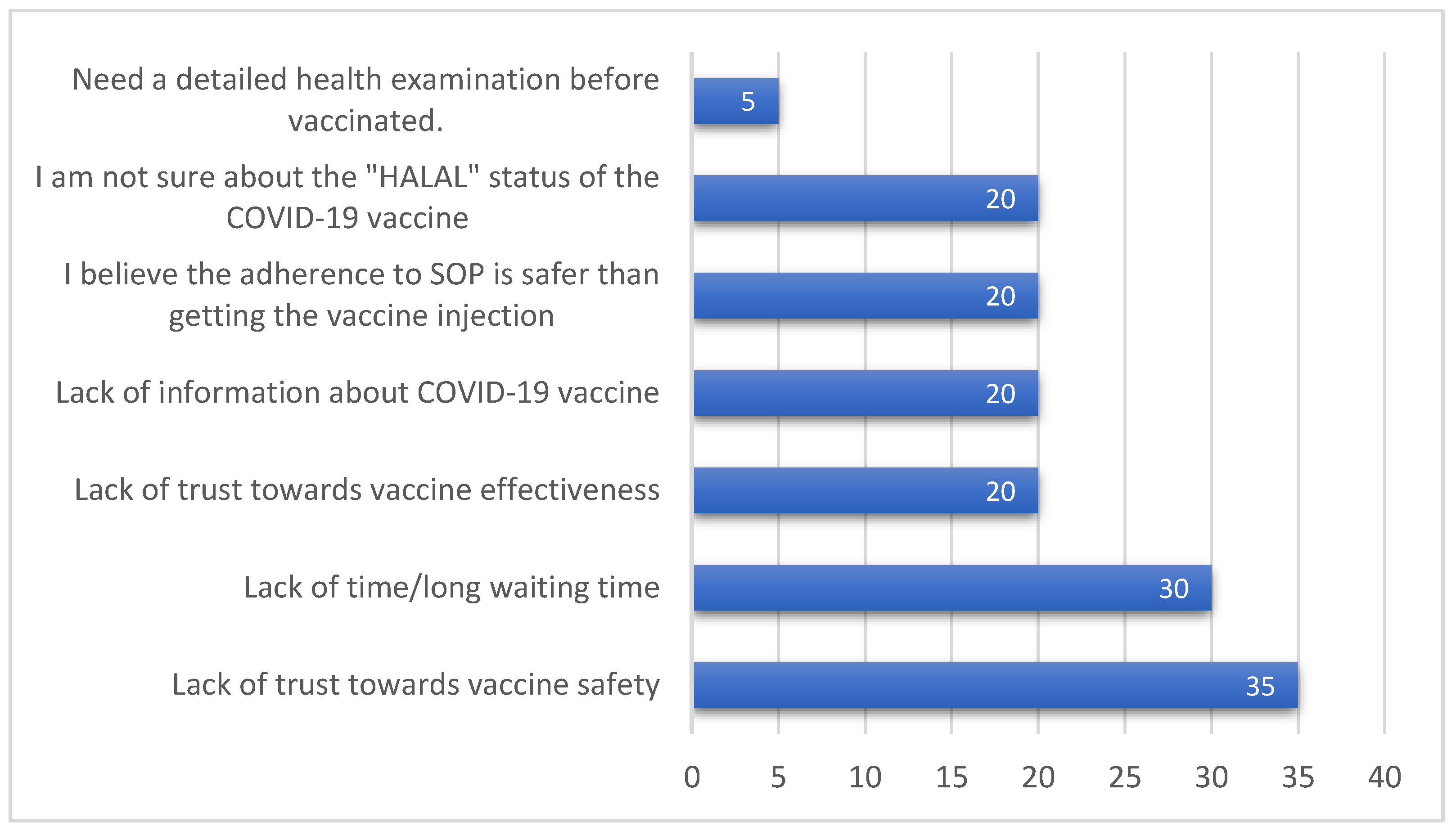
3.3. Vaccine Hesitancy Prevalence and Reasons
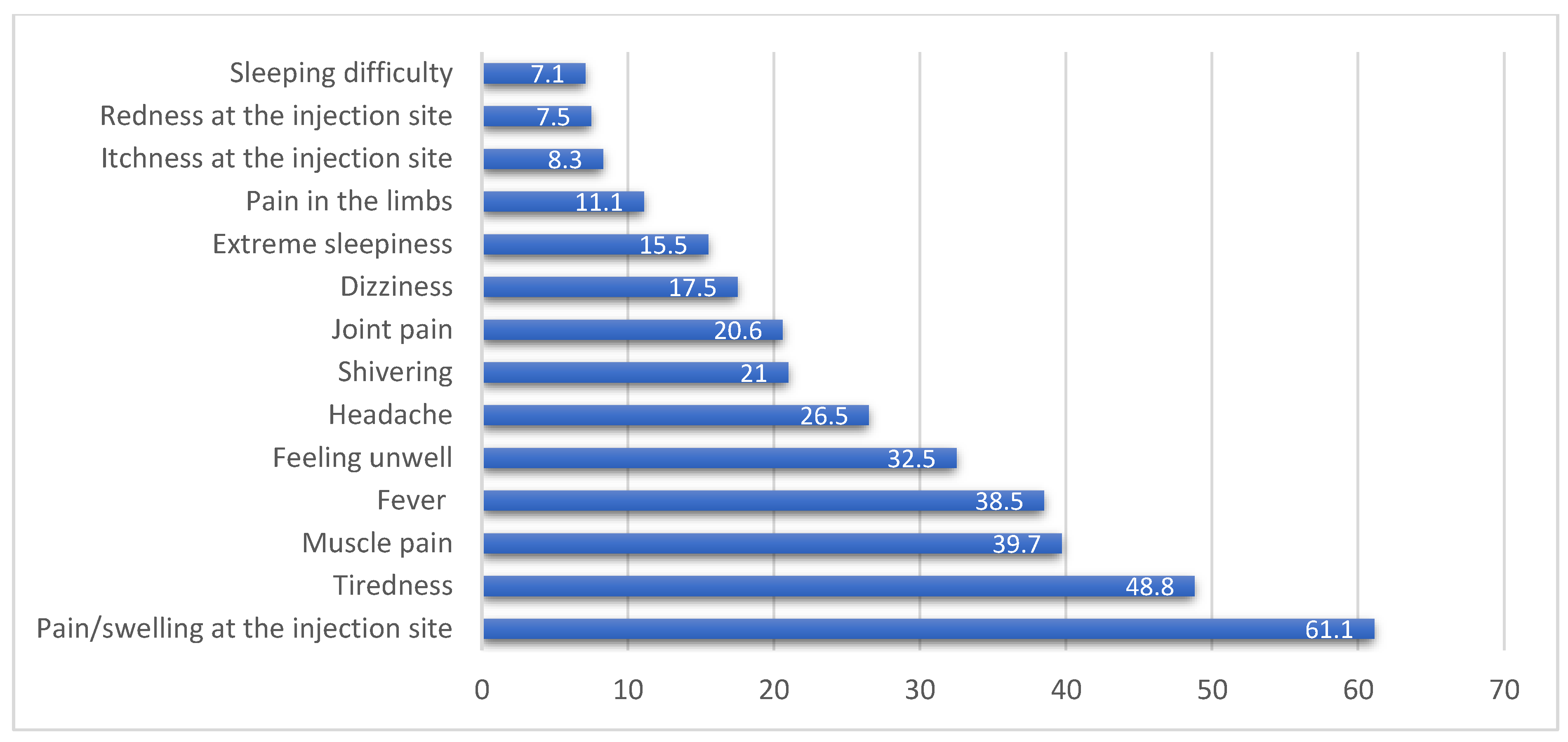
3.4. Vaccine Types, Side Effects, and Sources of Vaccine-Related Information
3.5. Gender and Perception on Receiving Adequate Vaccine-Related Information
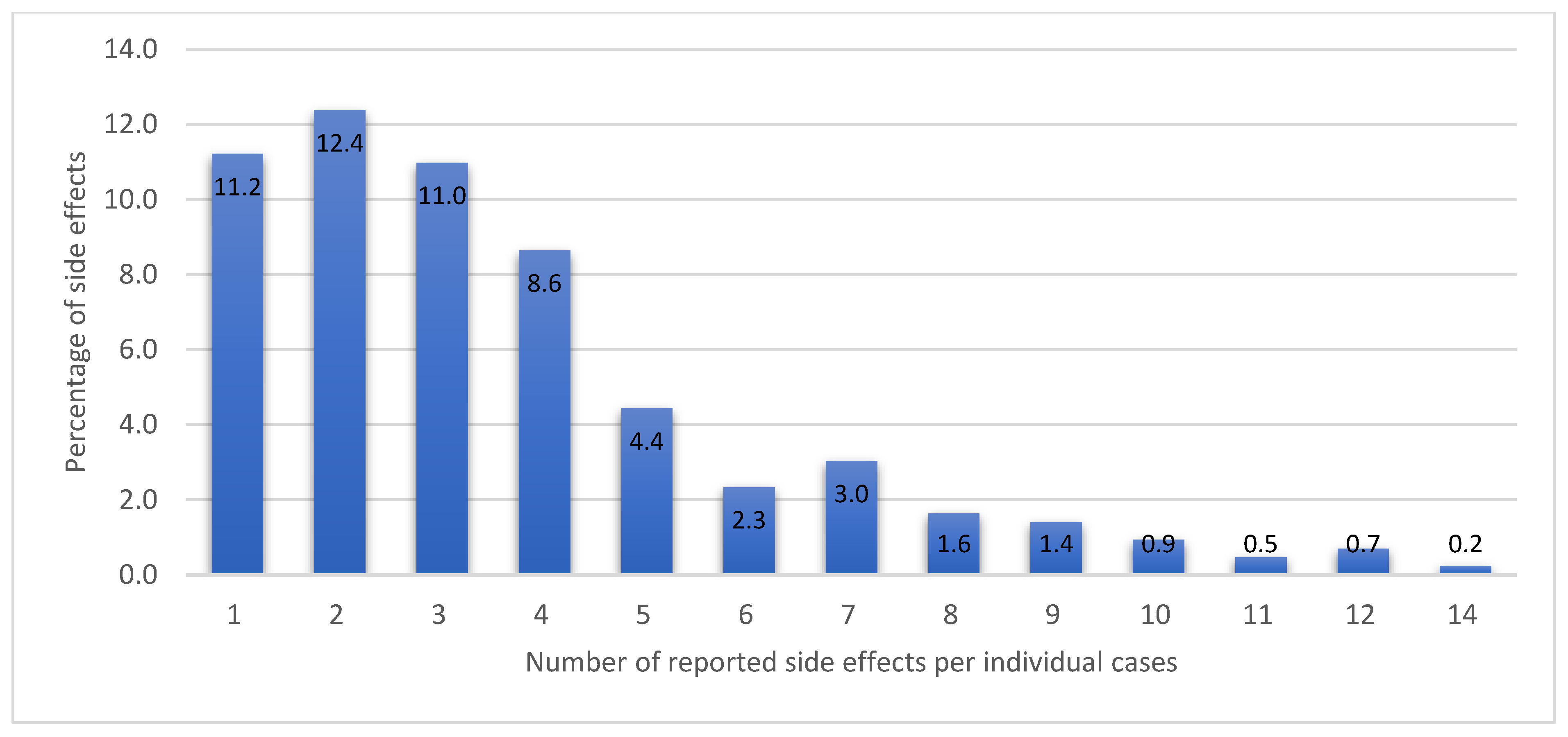
3.6. Types of Vaccines, Side Effects Occurrence with First or Second Doses, Number of Experienced Side Effects
3.7. Logistic Regression of Age, Gender, Vaccine Type, and the Experiencing of Vaccine-Related Side Effects
4. Discussion
4.1. Vaccination Acceptance, Attitudes, and Sources of Information
4.2. Vaccination Perceptions and Behaviors in the Post-Vaccination Era
4.3. Perceived Concerns towards Vaccination
4.4. Experiences of Vaccine-Related Side Effects
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; El-harakeh, A.; Bognanni, A.; Lotfi, T.; Loeb, M.; et al. Physical Distancing, Face Masks, and Eye Protection to Prevent Person-to-Person Transmission of SARS-CoV-2 and COVID-19: A Systematic Review and Meta-Analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Stefanati, A.; D’Anchera, E.; de Motoli, F.; Savio, M.; Toffoletto, M.V.; Gabutti, G. Value of Immunizations during the COVID-19 Emergency. Int. J. Environ. Res. Public Health 2021, 18, 778. [Google Scholar] [CrossRef]
- Ministry of Health (MOH) Malaysia. National COVID-19 Immunisation Programme the Special Committee for Ensuring Access to COVID-19 Vaccine Supply (Jkjav) 18 February 2021; Ministry of Health (MOH): Kuala Lumpur, Malaysia, 2021. [Google Scholar]
- Habersaat, K.B.; Jackson, C. Understanding Vaccine Acceptance and Demand—And Ways to Increase Them. Bundesgesundheitsblatt-Gesundh.-Gesundh. 2020, 63, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Dubé, È.; Farrands, A.; Lemaitre, T.; Boulianne, N.; Sauvageau, C.; Boucher, F.D.; Tapiero, B.; Quach, C.; Ouakki, M.; Gosselin, V.; et al. Overview of Knowledge, Attitudes, Beliefs, Vaccine Hesitancy and Vaccine Acceptance among Mothers of Infants in Quebec, Canada. Hum. Vaccines Immunother. 2019, 15, 113–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Napolitano, F.; D’Alessandro, A.; Angelillo, I.F. Investigating Italian Parents’ Vaccine Hesitancy: A Cross-Sectional Survey. Hum. Vaccines Immunother. 2018, 14, 1558–1565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bianco, A.; Mascaro, V.; Zucco, R.; Pavia, M. Parent Perspectives on Childhood Vaccination: How to Deal with Vaccine Hesitancy and Refusal? Vaccine 2019, 37, 984–990. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Ministry of Health Malaysia Vaccinations in Malaysia. COVIDNOW. Available online: https://covidnow.moh.gov.my/vaccinations/ (accessed on 1 October 2021).
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.A.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 Vaccine Acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Society, M.P. Immunisation Advocacy Chapter. Available online: https://www.mps.org.my/newsmaster.cfm?&menuid=37&action=view&retrieveid=7962 (accessed on 14 July 2021).
- Verger, P.; Peretti-Watel, P. Understanding the Determinants of Acceptance of COVID-19 Vaccines: A Challenge in a Fast-Moving Situation. Lancet Public Health 2021, 6, e195–e196. [Google Scholar] [CrossRef]
- Ministry of Health Malaysia. Clinical Guidelines on COVID-19 Vaccination in Malaysia; Ministry of Health (MOH): Kuala Lumpur, Malaysia, 2021. [Google Scholar]
- Ministry of Health (MOH). MySejahtera. Available online: https://mysejahtera.malaysia.gov.my/intro/ (accessed on 11 August 2021).
- Hum, W.L.; Hsien, C.C.M.; Nantha, Y.S. A Review of Smoking Research in Malaysia. Med. J. Malays. 2016, 71, 29–41. [Google Scholar]
- Elnaem, M.H.; Cheema, E. Caring for Patients with Diabetes during COVID-19 Pandemic: Important Considerations for Pharmacists. Res. Soc. Adm. Pharm. RSAP 2021, 17, 1938–1941. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A Global Survey of Potential Acceptance of a COVID-19 Vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Soyeon, S.; Kim, K.-A.; Kim, M.; Oh, J.; Chu, S.H.; Choi, J. Measurement of Digital Literacy Among Older Adults: Systematic Review. J. Med. Internet Res. 2021, 23, e26145. Available online: https://www.jmir.org/2021/2/e26145 (accessed on 6 August 2021). [CrossRef]
- Schmidt, H.; Gostin, L.O.; Williams, M.A. Is It Lawful and Ethical to Prioritize Racial Minorities for COVID-19 Vaccines? JAMA 2020, 324, 2023–2024. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2021, 9, 16. [Google Scholar] [CrossRef]
- di Giuseppe, G.; Pelullo, C.P.; della Polla, G.; Montemurro, M.V.; Napolitano, F.; Pavia, M.; Angelillo, I.F. Surveying Willingness toward SARS-CoV-2 Vaccination of Healthcare Workers in Italy. Expert Rev. Vaccines 2021, 20, 881–889. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Yau, P.S.Y.; Dong, D.; Wong, S.Y.S.; Yeoh, E.K. Change of Willingness to Accept COVID-19 Vaccine and Reasons of Vaccine Hesitancy of Working People at Different Waves of Local Epidemic in Hong Kong, China: Repeated Cross-Sectional Surveys. Vaccines 2021, 9, 62. [Google Scholar] [CrossRef]
- Latkin, C.A.; Dayton, L.; Yi, G.; Colon, B.; Kong, X. Mask Usage, Social Distancing, Racial, and Gender Correlates of COVID-19 Vaccine Intentions among Adults in the US. PLoS ONE 2021, 16, e0246970. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Pang, Y.; Lyu, Z.; Wang, R.; Wu, X.; You, C.; Zhao, H.; Manickam, S.; Lester, E.; Wu, T.; et al. The COVID-19 Vaccines: Recent Development, Challenges and Prospects. Vaccines 2021, 9, 349. [Google Scholar] [CrossRef]
- Patil, U.; Kostareva, U.; Hadley, M.; Manganello, J.A.; Okan, O.; Dadaczynski, K.; Massey, P.M.; Agner, J.; Sentell, T. Health Literacy, Digital Health Literacy, and COVID-19 Pandemic Attitudes and Behaviors in U.S. College Students: Implications for Interventions. Int. J. Environ. Res. Public Health 2021, 18, 3301. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- Machida, M.; Nakamura, I.; Kojima, T.; Saito, R.; Nakaya, T.; Hanibuchi, T.; Takamiya, T.; Odagiri, Y.; Fukushima, N.; Kikuchi, H.; et al. Acceptance of a COVID-19 Vaccine in Japan during the COVID-19 Pandemic. Vaccines 2021, 9, 210. [Google Scholar] [CrossRef] [PubMed]
- Dula, J.; Mulhanga, A.; Nhanombe, A.; Cumbi, L.; Júnior, A.; Gwatsvaira, J.; Siewe Fodjo, J.N.; de Moura Villela, E.F.; Chicumbe, S.; Colebunders, R. COVID-19 Vaccine Acceptability and Its Determinants in Mozambique: An Online Survey. Vaccines 2021, 9, 828. [Google Scholar] [CrossRef]
- Razai, M.S.; Chaudhry, U.A.R.; Doerholt, K.; Bauld, L.; Majeed, A. COVID-19 Vaccination Hesitancy. BMJ 2021, 373, n1138. [Google Scholar] [CrossRef]
- Tao, L.; Lu, M.; Wang, X.; Han, X.; Li, S.; Wang, H. The Influence of a Community Intervention on Influenza Vaccination Knowledge and Behavior among Diabetic Patients. BMC Public Health 2019, 19, 1747. [Google Scholar] [CrossRef]
- Chen, H.; Zhang, X.; Wang, W.; Zhang, R.; Du, M.; Shan, L.; Li, Y.; Wang, X.; Liu, Y.; Zhang, W.; et al. Effect of an Educational Intervention on Human Papillomavirus (HPV) Knowledge and Attitudes towards HPV Vaccines among Healthcare Workers (HCWs) in Western China. Hum. Vaccines Immunother. 2020, 17, 443–450. [Google Scholar] [CrossRef]
- di Giuseppe, G.; Pelullo, C.P.; della Polla, G.; Pavia, M.; Angelillo, I.F. Exploring the Willingness to Accept SARS-CoV-2 Vaccine in a University Population in Southern Italy, September to November 2020. Vaccines 2021, 9, 275. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Pokorná, A.; Attia, S.; Klugarová, J.; Koščík, M.; Klugar, M. Prevalence of COVID-19 Vaccine Side Effects among Healthcare Workers in the Czech Republic. J. Clin. Med. 2021, 10, 1428. [Google Scholar] [CrossRef]
- Riad, A.; Sağıroğlu, D.; Üstün, B.; Pokorná, A.; Klugarová, J.; Attia, S.; Klugar, M. Prevalence and Risk Factors of CoronaVac Side Effects: An Independent Cross-Sectional Study among Healthcare Workers in Turkey. J. Clin. Med. 2021, 10, 2629. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- He, Q.; Mao, Q.; Zhang, J.; Bian, L.; Gao, F.; Wang, J.; Xu, M.; Liang, Z. COVID-19 Vaccines: Current Understanding on Immunogenicity, Safety, and Further Considerations. Front. Immunol. 2021, 12, 669339. [Google Scholar] [CrossRef] [PubMed]
- Wise, J. COVID-19: European Countries Suspend Use of Oxford-AstraZeneca Vaccine after Reports of Blood Clots. BMJ 2021, 372, n699. [Google Scholar] [CrossRef]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Malayala, S.V. Side Effects of BNT162b2 MRNA COVID-19 Vaccine: A Randomized, Cross-Sectional Study with Detailed Self-Reported Symptoms from Healthcare Workers. Int. J. Infect. Dis. 2021, 106, 376–381. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Reactions and Adverse Events of the Pfizer-BioNTech COVID-19 Vaccine|CDC. Available online: https://www.cdc.gov/vaccines/covid-19/info-by-product/pfizer/reactogenicity.html (accessed on 31 July 2021).
- Repajic, M.; Lai, X.L.; Xu, P.; Liu, A. Bell’s Palsy after Second Dose of Pfizer COVID-19 Vaccination in a Patient with History of Recurrent Bell’s Palsy. Brain Behav. Immun.-Health 2021, 13, 100217. [Google Scholar] [CrossRef]
- Albert, E.; Aurigemma, G.; Saucedo, J.; Gerson, D.S. Myocarditis Following COVID-19 Vaccination. Radiol. Case Rep. 2021, 16, 2142–2145. [Google Scholar] [CrossRef]
- Grimm, P. Social desirability bias. In Wiley International Encyclopedia of Marketing; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2010. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Number | Percentage (%) | |
|---|---|---|
| Age | ||
| 18–30 | 115 | 26.9 |
| 31–45 | 189 | 44.2 |
| 46–59 | 68 | 15.9 |
| 60 or more | 56 | 13.0 |
| Race | ||
| Malay | 394 | 92.1 |
| Chinese | 14 | 3.2 |
| Indian | 3 | 0.7 |
| Others | 17 | 4.0 |
| Gender | ||
| Male | 144 | 33.6 |
| Female | 284 | 66.4 |
| Smoking status | ||
| Non-smoker | 364 | 85.0 |
| Ex-smoker | 36 | 8.5 |
| Current smoker | 28 | 6.5 |
| Highest education level | ||
| Doctorate | 29 | 6.8 |
| Masters | 62 | 14.5 |
| Degree/Diploma (Uni/college) | 224 | 52.3 |
| Uni Student | 53 | 12.4 |
| Secondary Edu | 58 | 13.6 |
| Informal Edu | 2 | 0.4 |
| Occupation | ||
| Public sector | 200 | 46.7 |
| Private sector | 89 | 20.8 |
| Self-employed | 38 | 8.9 |
| Unemployed | 46 | 10.8 |
| Student | 30 | 7.0 |
| Pensioner | 25 | 5.8 |
| Chronic diseases | ||
| Yes | 89 | 20.8 |
| No | 339 | 79.2 |
| Having family members/relatives diagnosed with COVID-19 infection? | ||
| Yes | 125 | 29.2 |
| No | 303 | 70.8 |
| Diagnosed with COVID-19 infection before the vaccine availability? | ||
| Yes | 12 | 2.8 |
| No | 416 | 97.2 |
| Total | 428 | 100.0 |
| Number | Percentage (%) | |
|---|---|---|
| Please rate your adherence level to the recommended SOP, e.g., wearing a mask, physical distancing, and regular use of hand sanitizers: | ||
| Fair | 1 | 0.2 |
| Good | 15 | 3.5 |
| High | 141 | 32.9 |
| Very high | 271 | 63.3 |
| The National COVID-19 Vaccination Program is currently ongoing. Have you registered to be vaccinated? | ||
| Yes | 422 | 98.6 |
| No | 6 | 1.4 |
| Mode of registration for vaccination *: | ||
| MySejahtera App | 349 | 81.5 |
| Employer | 63 | 14.7 |
| Both (App + Employer) | 6 | 1.4 |
| Others (walk-in/Az voluntary program) | 6 | 1.4 |
| Please rate your confidence level regarding the effectiveness of COVID-19 vaccines: | ||
| Low | 3 | 0.7 |
| Fair | 6 | 1.4 |
| Good | 53 | 12.4 |
| High | 173 | 40.4 |
| Very High | 193 | 45.1 |
| Do you believe that you have received accurate and sufficient information regarding the COVID-19 vaccine? | ||
| Yes | 343 | 80.1 |
| No | 16 | 3.7 |
| Not sure | 69 | 16.1 |
| Do you know that COVID-19 infection could still happen after completing the recommended vaccination dose? | ||
| Yes | 416 | 97.2 |
| No | 3 | 0.7 |
| Not sure | 9 | 2.1 |
| Do you know the severity of Covid19 complications to vaccinated Covid19 patients is lesser than unvaccinated Covid19 patients? | ||
| Yes | 404 | 94.4 |
| No | 5 | 1.2 |
| Not sure | 19 | 4.4 |
| Number | Percentage (%) | |
|---|---|---|
| Select the type of vaccine that you have received: | ||
| Pfizer-BioNTech (Cominarty®) | 178 | 53.6 |
| Sinovac (CoronaVac®) | 90 | 27.1 |
| Oxford-AstraZeneca (ChAdOx1-S) | 64 | 19.3 |
| Total | 332 | 100.0 |
| The month you received the COVID-19 vaccine: | ||
| February 2021 | 3 | 1.0 |
| March 2021 | 54 | 17.6 |
| April 2021 | 31 | 10.1 |
| May 2021 | 39 | 12.8 |
| June 2021 | 86 | 28.1 |
| July 2021 | 93 | 30.4 |
| Total | 306 | 100.0 |
| Did you experience any side effects after receiving the vaccine? | ||
| Yes | 252 | 76.8 |
| No | 76 | 23.2 |
| Total | 328 | 100.0 |
| Were the side effects occurred more with the first dose or second dose? | ||
| More with First dose | 50 | 24.4 |
| More with Second dose | 80 | 39.0 |
| No difference | 75 | 36.6 |
| Total | 205 | 100.0 |
| Please rate the severity of the side effects that occurred after vaccination: | ||
| Minor | 103 | 40.9 |
| Mild | 69 | 27.4 |
| Moderate | 54 | 21.4 |
| Moderately severe | 24 | 9.5 |
| Severe | 2 | 0.8 |
| Total | 252 | 100.0 |
| Choose the most accurate statement that reflects your adherence to SOP “physical distancing and wearing a face mask” compared to before receiving your vaccine: | ||
| I feel safer removing face mask more frequently compared to before vaccination. | 4 | 1.2 |
| I feel safer, but my adherence to SOP is the same as before vaccination. | 305 | 95.0 |
| I do not feel or practice the SOP related to COVID-19 infection differently. | 12 | 3.8 |
| Total | 321 | 100.0 |
| What is your main source of information regarding the COVID-19 vaccination? | ||
| Official website of Ministry of Health and MySejahtera application. | 197 | 53.7 |
| World Health Organization (WHO). | 32 | 8.7 |
| Social media. | 81 | 22.1 |
| Internet sources such as Google & YouTube. | 44 | 12.0 |
| Family and friends | 12 | 3.2 |
| Peer-reviewed scientific papers | 1 | 0.3 |
| Total | 367 | 100.0 |
| p-Value | Odds Ratio (OR) | 95% CI | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Age (18–30) | 0.000 | 7.403 | 2.640 | 20.761 |
| Age (31–45) | 0.001 | 3.461 | 1.617 | 7.406 |
| Age (46–59) | 0.002 | 4.391 | 1.720 | 11.214 |
| Gender (Male) | 0.030 | 0.510 | 0.278 | 0.936 |
| Vaccine Type (Pfizer-BioNTech (Cominarty®)) | 0.109 | 0.447 | 0.167 | 1.198 |
| Vaccine Type (Sinovac (CoronaVac®)) | 0.000 | 0.082 | 0.030 | 0.227 |
| Constant | 0.002 | 4.962 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elnaem, M.H.; Mohd Taufek, N.H.; Ab Rahman, N.S.; Mohd Nazar, N.I.; Zin, C.S.; Nuffer, W.; Turner, C.J. COVID-19 Vaccination Attitudes, Perceptions, and Side Effect Experiences in Malaysia: Do Age, Gender, and Vaccine Type Matter? Vaccines 2021, 9, 1156. https://doi.org/10.3390/vaccines9101156
Elnaem MH, Mohd Taufek NH, Ab Rahman NS, Mohd Nazar NI, Zin CS, Nuffer W, Turner CJ. COVID-19 Vaccination Attitudes, Perceptions, and Side Effect Experiences in Malaysia: Do Age, Gender, and Vaccine Type Matter? Vaccines. 2021; 9(10):1156. https://doi.org/10.3390/vaccines9101156
Chicago/Turabian StyleElnaem, Mohamed Hassan, Nor Hidayah Mohd Taufek, Norny Syafinaz Ab Rahman, Nor Ilyani Mohd Nazar, Che Suraya Zin, Wesley Nuffer, and Christopher John Turner. 2021. "COVID-19 Vaccination Attitudes, Perceptions, and Side Effect Experiences in Malaysia: Do Age, Gender, and Vaccine Type Matter?" Vaccines 9, no. 10: 1156. https://doi.org/10.3390/vaccines9101156