
Dental Education Challenges during the COVID-19 Pandemic Period in Italy: Undergraduate Student Feedback, Future Perspectives, and the Needs of Teaching Strategies for Professional Development

 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. The New Teaching Methods
2.2. Sample and Questionnaire
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
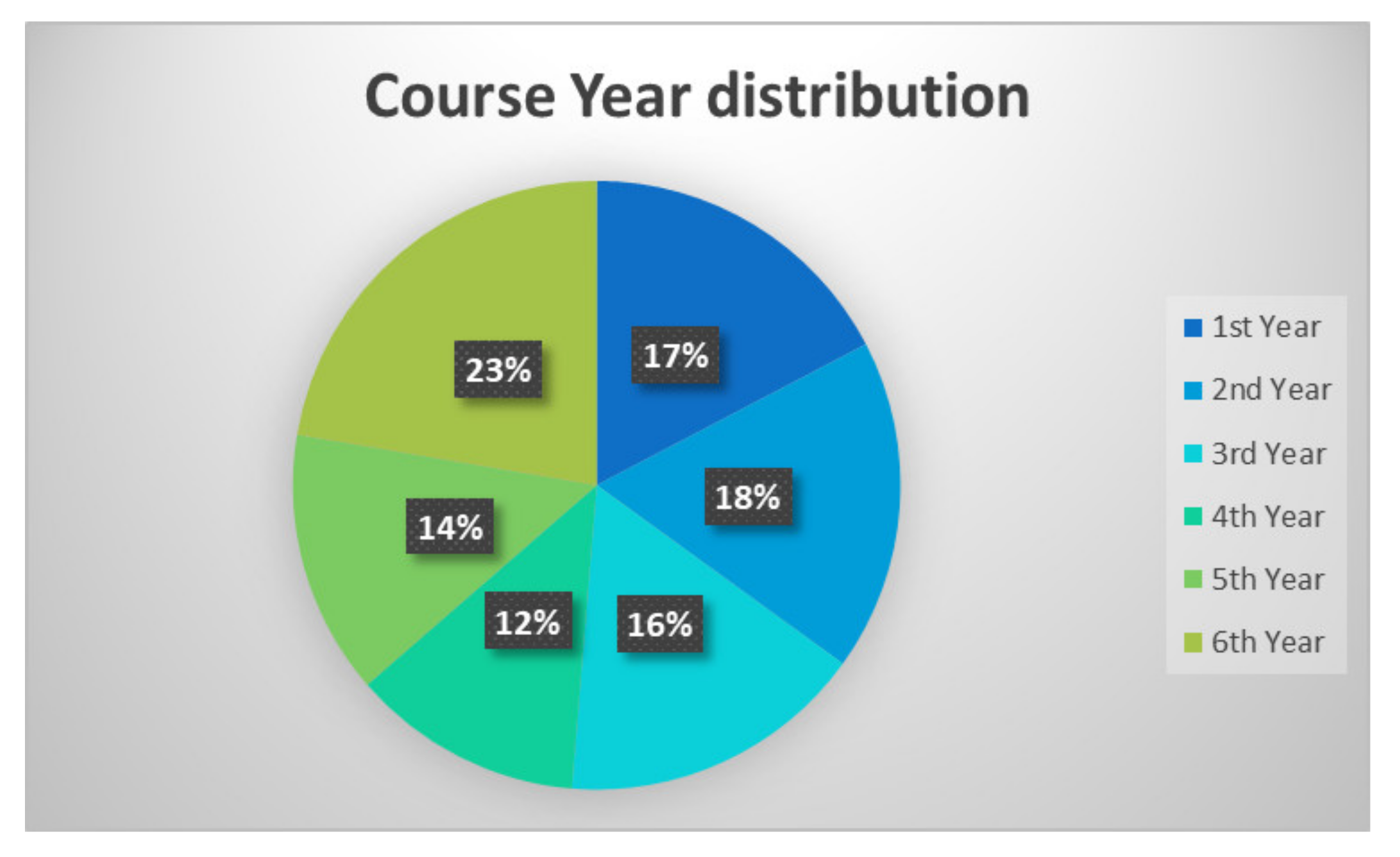
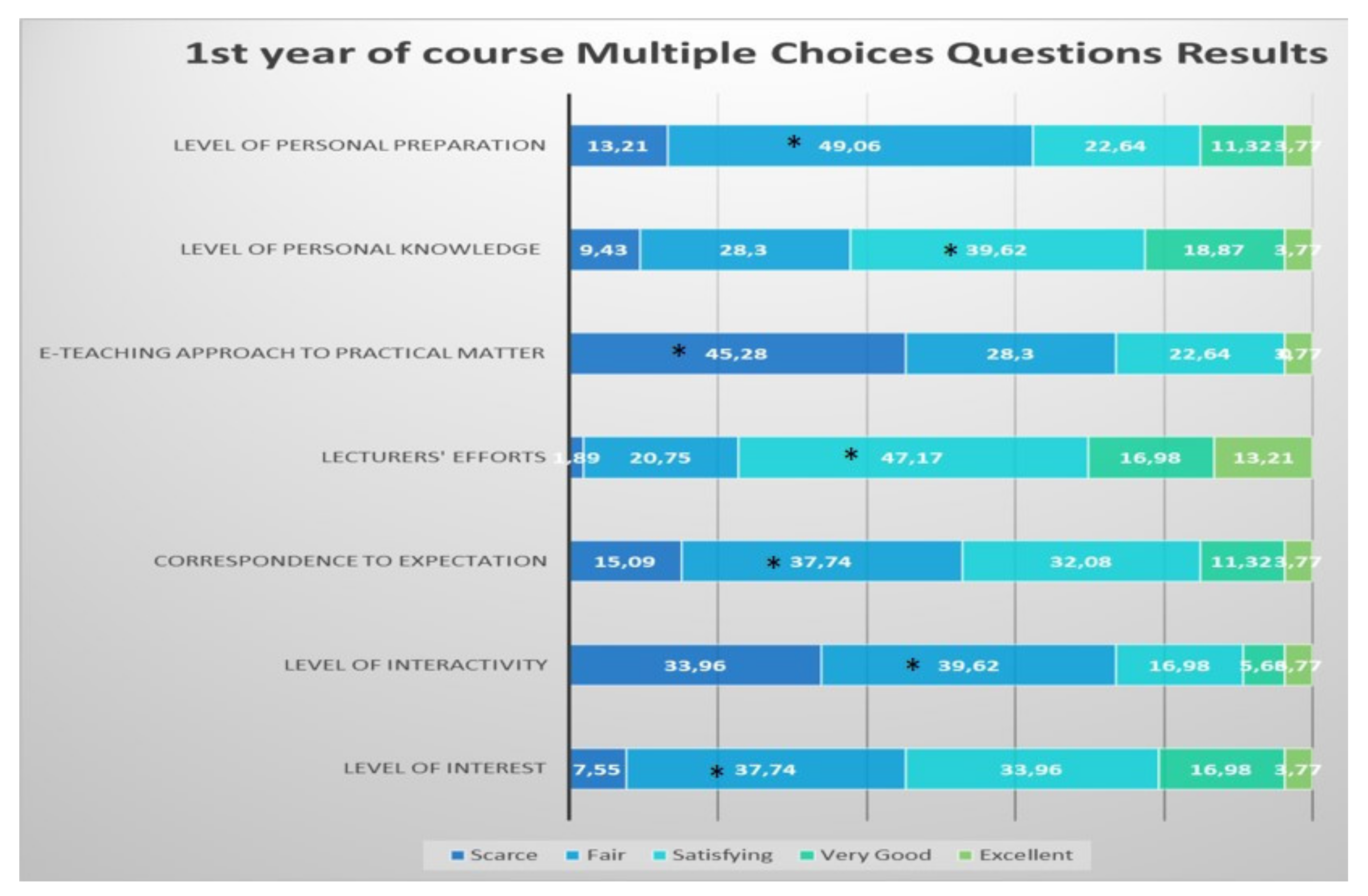
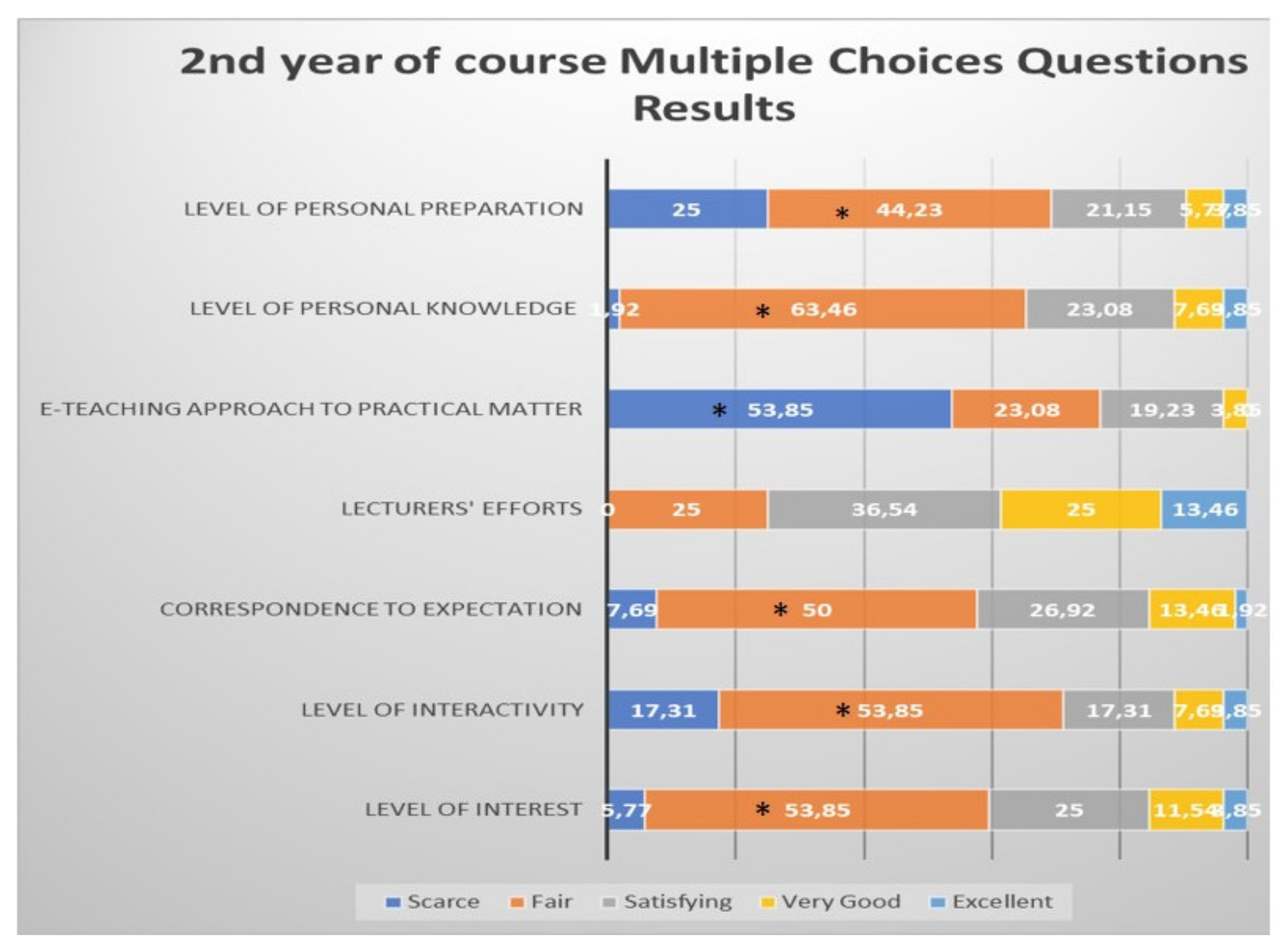
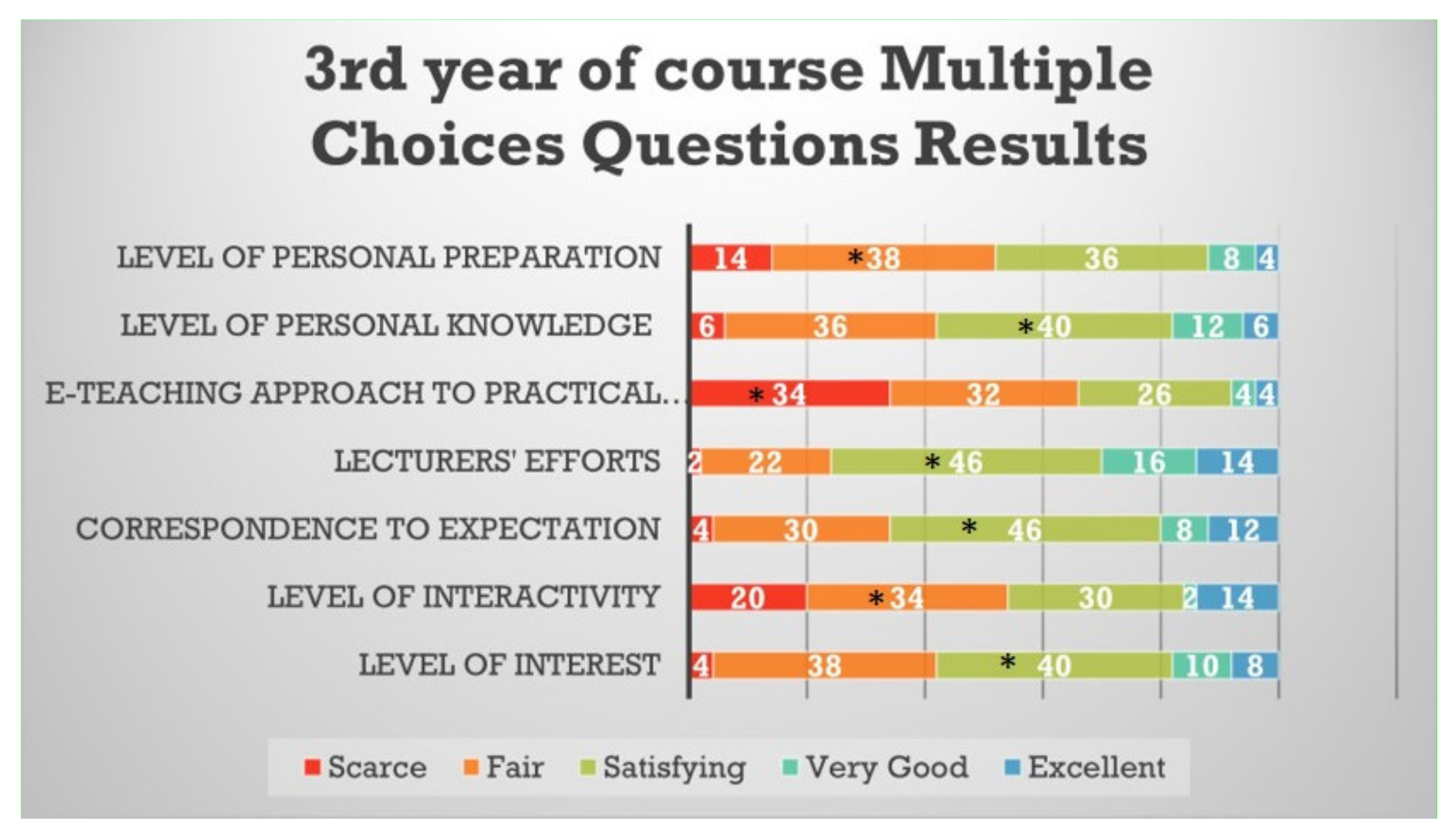
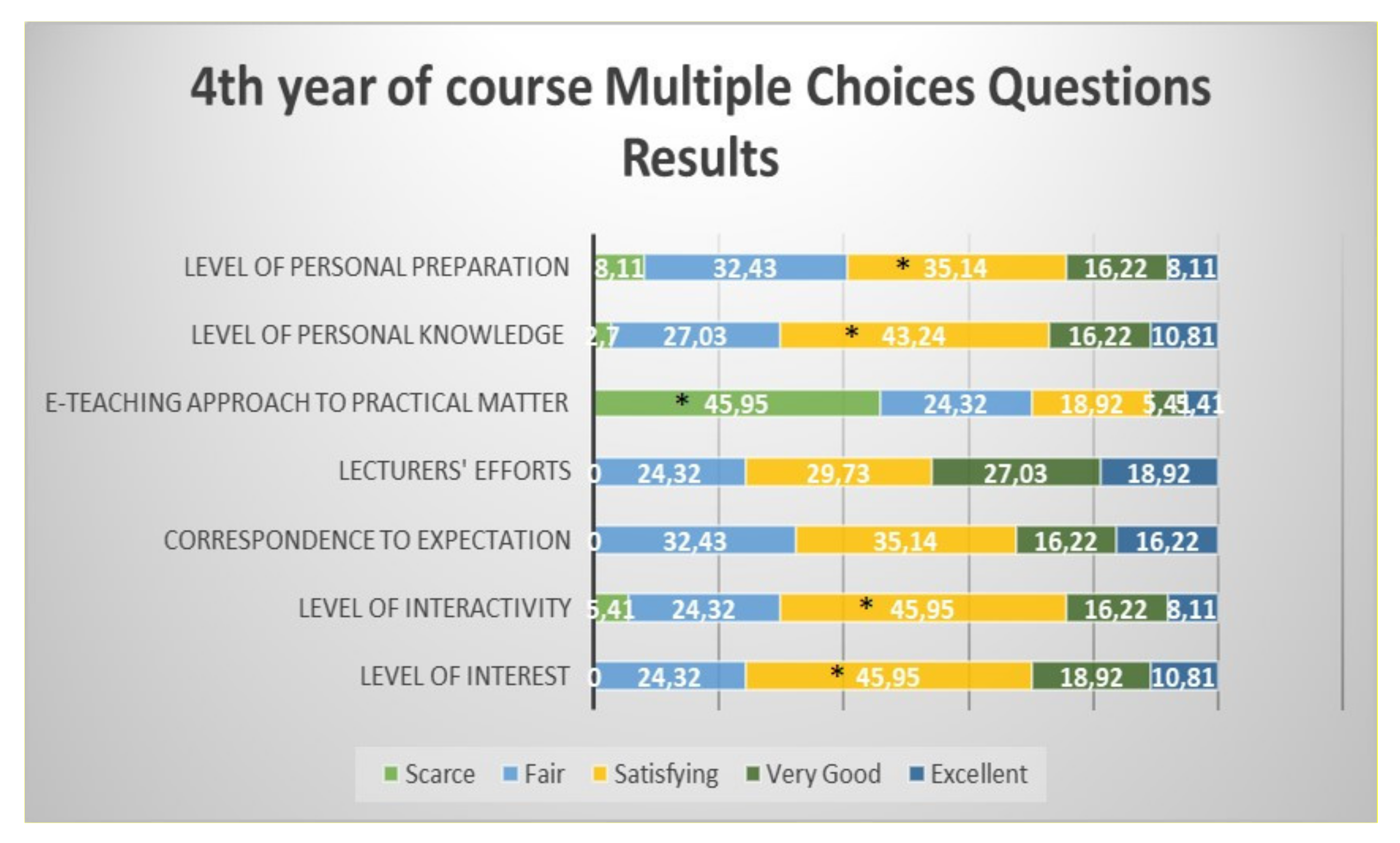
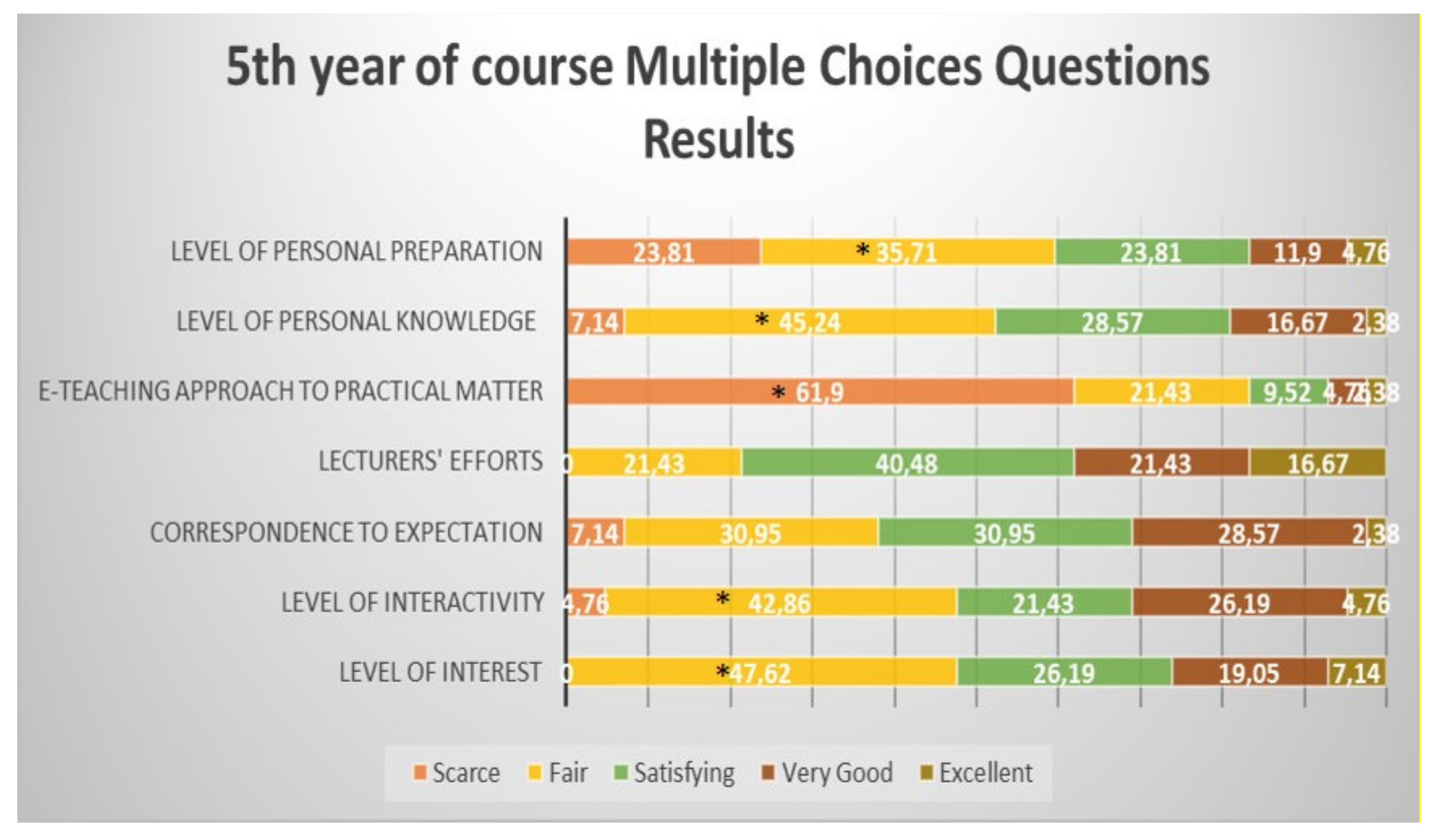
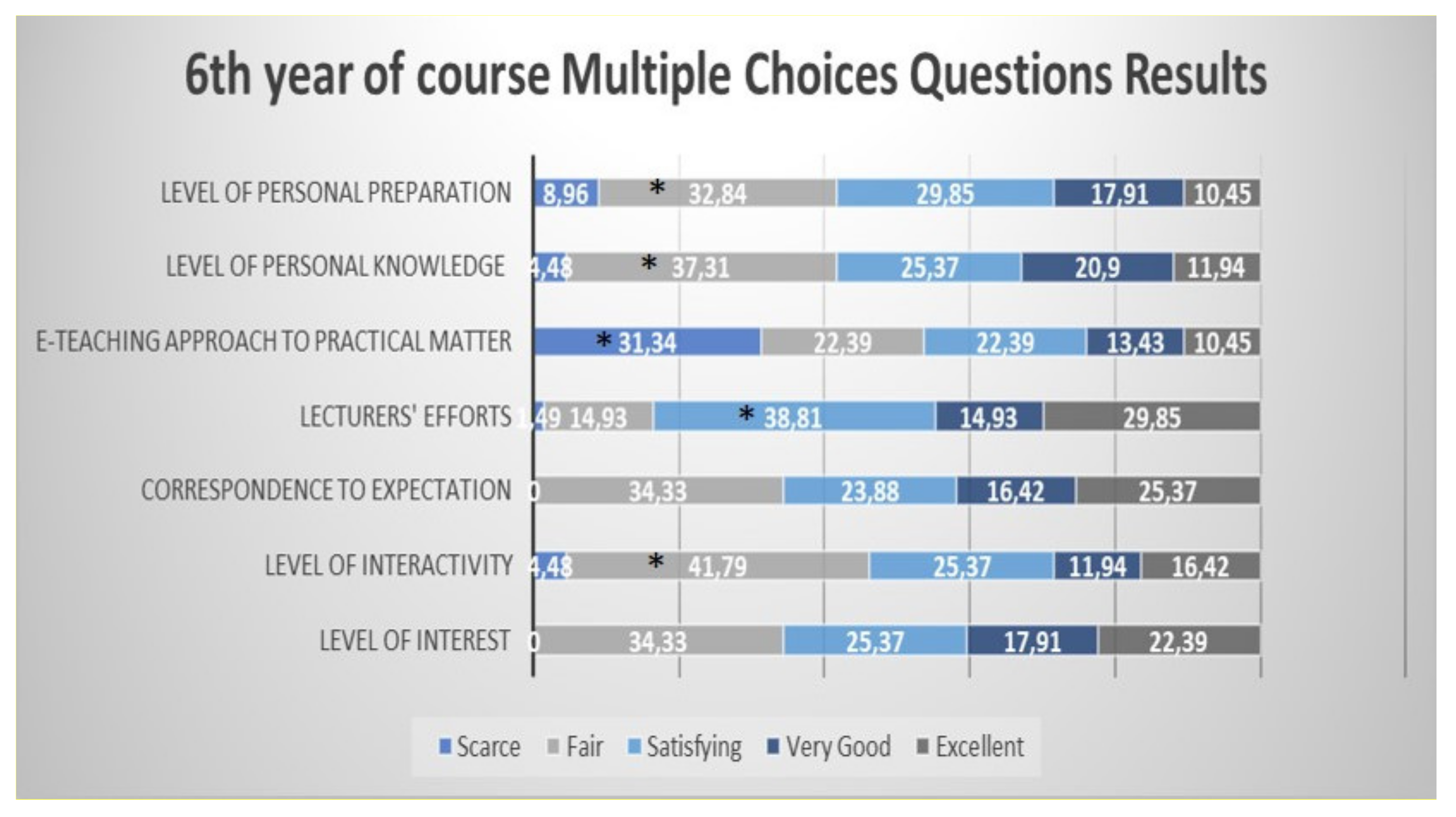
3.1. Demographic Characteristics and Results from the Different Years of Course
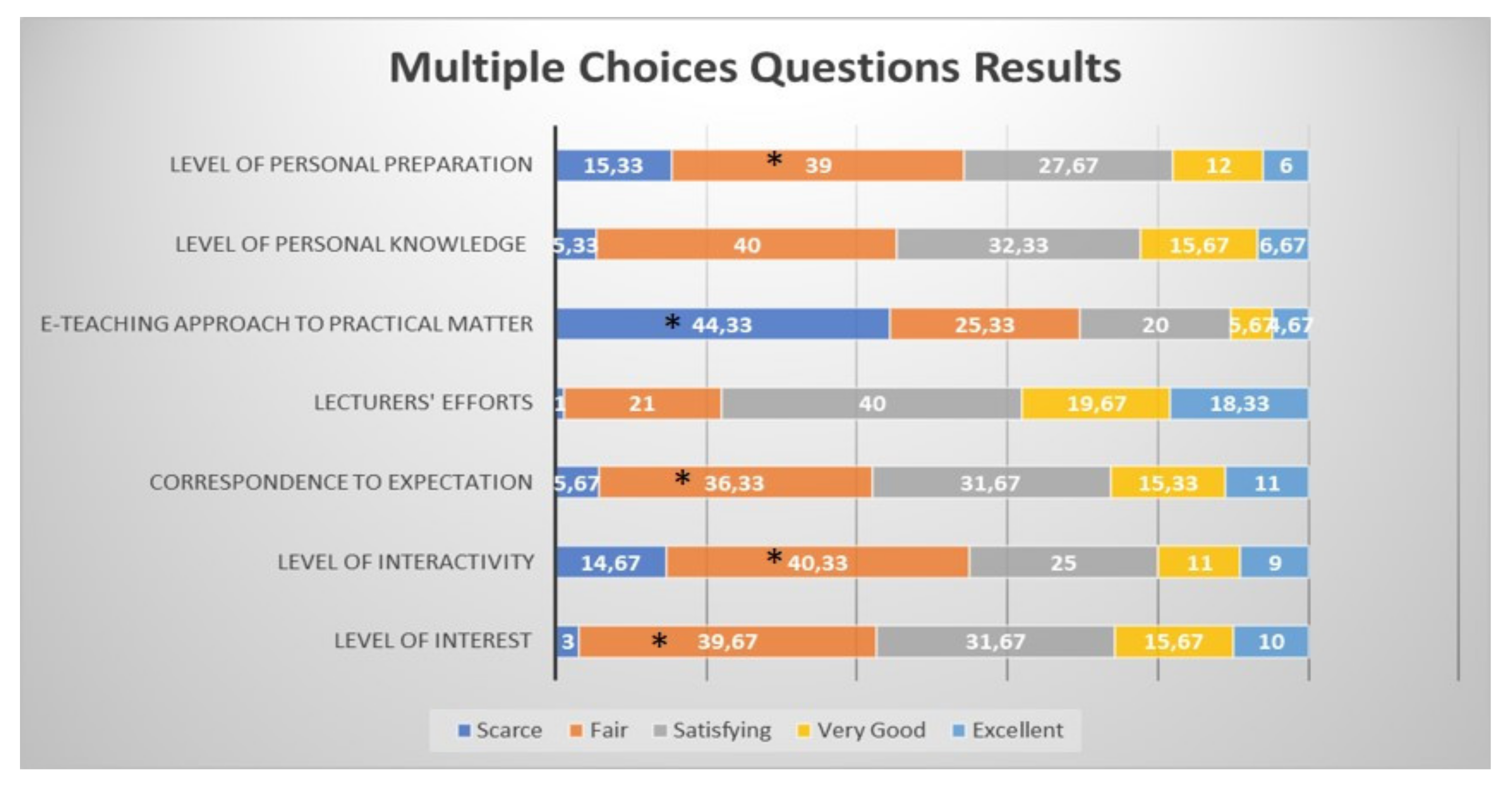
3.2. The Combined Results
3.3. The Stakeholder Mapping Matrix
3.4. The Open-Ended Questions: The Voices of the Students
4. Discussion
4.1. The Main Issue from the Survey: How Did We Fill the Gap?
4.2. The Educational Theories before the Pandemic
- (1)
- Active and involving experience;
- (2)
- Reflective observation, with elaboration of the experienced moments from many points of views;
- (3)
- Abstract conceptualization, where the created concepts integrate the observations themselves;
- (4)
- Active actualizations in new situations that are derived from the past experience.
- (1)
- Live observation;
- (2)
- Verbal instructions, with actions and behavioral actions;
- (3)
- Symbolic model.
4.3. The Pandemic and Dental Education: Italy and Europe and Their Differences
4.4. Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel Coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Bianchi, S.; Gatto, R.; Fabiani, L. Effects of the SARS-COV-2 pandemic on medical education in Italy: Considerations and tips. Euromediterr. Biomed. J. 2020, 15, 100–101. [Google Scholar] [CrossRef]
- Prezioso, C.; Pietropaolo, V. COVID-19: Update of the Italian situation. J. Neurovirology 2020, 26, 834–837. [Google Scholar] [CrossRef]
- Lewin, K.M. Contingent reflections on coronavirus and priorities for educational planning and development. Prospects 2020, 49, 17–24. [Google Scholar] [CrossRef]
- Quinn, B.; Field, J.; Gorter, R.; Akota, I.; Manzanares, M.C.; Paganelli, C.; Davies, J.; Dixon, J.; Gabor, G.; Amaral Mendes, R.; et al. COVID-19: The immediate response of European academic dental institutions, and future implications for dental education. Eur. J. Dent. Educ. 2020, 24, 811–814. [Google Scholar] [CrossRef]
- Nicolucci, A. [Selecting statistical test] Guida alla scelta dei test statistici. G. Ital. Diabetol. Metab. 2018, 38, 54–59. [Google Scholar]
- Schlenz, M.A.; Schmidt, A.; Wöstmann, B.; Krämer, N.; Schulz-Weidner, N. Students’ and lecturers’ perspective on the implementation of online learning in dental education due to SARS-CoV-2 (COVID-19): A cross-sectional study. BMC Med. Educ. 2020, 20, 354. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, K.J.; Nahar, R.; Parlani, S.; Murthy, V.J. A cross-sectional virtual survey to evaluate the outcome of online dental education system among undergraduate dental students across India amid COVID-19 pandemic. Eur. J. Dent. Educ. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hattar, S.; Al Hadidi, A.; Sawair, F.A.; Alraheam, I.A.; El-Ma’aita, A.; Wahab, F.K. Impact of COVID-19 pandemic on dental education: Online experience and practice expectations among dental students at the University of Jordan. BMC Med. Educ. 2021, 21, 151. [Google Scholar] [CrossRef]
- Bianchi, S.; Bernardi, S.; Perilli, E.; Cipollone, C.; Di Biasi, J.; Macchiarelli, G. Evaluation of effectiveness of digital technologies during anatomy learning in nursing school. Appl. Sci. 2020, 10, 2357. [Google Scholar] [CrossRef] [Green Version]
- Bentata, Y. The COVID-19 pandemic and international federation of medical students’ association exchanges: Thousands of students deprived of their clinical and research exchanges. Med. Educ. Online 2020, 25, 1783784. [Google Scholar] [CrossRef] [PubMed]
- Consorti, F. Didattica Professionalizzante nei Corsi di Laurea in Medicina; Edra: Milano, Italy, 2018. [Google Scholar]
- Kaufman, M.D. ABC of learning and teaching in medicine. Applying educational theory in practice. BMJ 2003, 326, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Ericsson, K.A.; Krampe, R.T.; Tesh-Romer, C. The role of deliberate practice in the acquisition of expert performance. Psycological Rev. 1993, 100, 363–406. [Google Scholar] [CrossRef]
- Kolb, D.A. Experential Learning: Experience as the Source of Learning and Development; Prentice-Hall: Hoboken, NJ, USA, 1984. [Google Scholar]
- Bandura, A. Social Learning Theory; Prentice Hall: Englewood Cliffs, NJ, USA, 1977. [Google Scholar]
- Iyer, P.; Aziz, K.; Ojcius, D.M. Impact of COVID-19 on dental education in the United States. J. Dent. Educ. 2020, 84, 718–722. [Google Scholar] [CrossRef]
- Desai, B.K. Clinical implications of the COVID-19 pandemic on dental education. J. Dent. Educ. 2020, 84, 512. [Google Scholar] [CrossRef]
- Bohner, L.; Maus, M.; Kleinheinz, J.; Hanisch, M. 2019-nCoV: Measures adopted at the Departments of Oral Surgery and Radiology during the period of an uncontrolled transmission increase. Dent. J. 2020, 8, 57. [Google Scholar] [CrossRef] [PubMed]
- Mladenovic, R.; Bukumiric, Z.; Mladenovic, K. Influence of a dedicated mobile application on studying traumatic dental injuries during student isolation. J. Dent. Educ. 2020, 1–3. [Google Scholar] [CrossRef]
- Stoopler, E.T.; Tanaka, T.I.; Sollecito, T.P. Hospital-based dental externship during COVID-19 pandemic: Think virtual! Spec. Care Dent. 2020, 40, 393–394. [Google Scholar] [CrossRef]
- Sajdłowski, D.; Świątkowski, W.; Rahnama, M. Dental Education in COVID-19 Pandemic. World J. Surg. Surg. Res. 2021, 4, 1283. [Google Scholar]
- Hung, M.; Licari, F.W.; Hon, E.S.; Lauren, E.; Su, S.; Birmingham, W.C.; Wadsworth, L.L.; Lassetter, J.H.; Graff, T.C.; Harman, W.; et al. In an era of uncertainty: Impact of COVID-19 on dental education. J. Dent. Educ. 2020, 1–9. [Google Scholar] [CrossRef]
- Turkyilmaz, I.; Hariri, N.H.; Jahangiri, L. Student’s perception of the impact of e-learning on dental education. J. Contemp. Dent. Pract. 2019, 20, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.S.; Hong, G.; Paganelli, C.; Phantumvanit, P.; Chang, W.J.; Shieh, Y.S.; Hsu, M.L. Innovation of dental education during COVID-19 pandemic. J. Dent. Sci. 2021, 16, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Pinchi, V.; Varvara, G.; Pradella, F.; Focardi, M.; Donati, M.D.; Norelli, G. Analysis of professional malpractice claims in implant dentistry in Italy from insurance company technical reports, 2006 to 2010. Int. J. Oral Maxillofac. Implant. 2014, 29, 77–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question Number | Question |
|---|---|
| 1 | Consent acceptance |
| 2 | Gender |
| 3 | Age |
| 4 | Year of course |
| 5 | How would you describe the level of interest for the at-a-distance lectures through the platform we used? |
| 6 | How would you describe the interactivity levels during the lectures? |
| 7 | Have your expectations regarding the at-a-distance lecture contents been satisfied? |
| 8 | How would you describe the lecturers” efforts to guarantee the teaching even during the emergency period? |
| 9 | How would you describe the at-a-distance approaches to the aspects that require the development of practical skills? |
| 10 | How would you describe the cultural knowledge you have acquired during the COVID-19 emergency period? |
| 11 | How adequate would you describe your level of preparation compared to the lectures attended in the pre-COVID-19 period? |
| 12 | Points of strength of the at-a-distance lectures |
| 13 | Limitations of the at-a-distance lectures |
| Question | Answer | n | Kruskal-Wallis Test | ||
|---|---|---|---|---|---|
| Chi-Square | DF | p-Value | |||
| Level of Interest | Fair | 119 | 21.0816 | 4 | 0.0003 |
| Satisfying | 96 | ||||
| Very Good | 47 | ||||
| Excellent | 30 | ||||
| Scarce | 9 | ||||
| Level of Interactivity | Fair | 121 | 31.1323 | 4 | <0.0001 |
| Satisfying | 76 | ||||
| Very Good | 33 | ||||
| Excellent | 27 | ||||
| Scarce | 44 | ||||
| Correspondence to expectations | Fair | 109 | 26.4313 | 4 | <0.0001 |
| Satisfying | 96 | ||||
| Very Good | 33 | ||||
| Excellent | 46 | ||||
| Scarce | 17 | ||||
| Lecturers’ efforts | Fair | 63 | 6.3095 | 4 | 0.1772 |
| Satisfying | 121 | ||||
| Very Good | 59 | ||||
| Excellent | 55 | ||||
| Scarce | 3 | ||||
| E-teaching approach to the practical matter | Fair | 76 | 14.0712 | 4 | 0.0071 |
| Satisfying | 61 | ||||
| Very Good | 133 | ||||
| Excellent | 17 | ||||
| Scarce | 14 | ||||
| Level of personal Knowledge | Fair | 120 | 4.8898 | 4 | 0.2988 |
| Satisfying | 98 | ||||
| Very Good | 16 | ||||
| Excellent | 47 | ||||
| Scarce | 20 | ||||
| Level of personal preparation | Fair | 117 | 9.0823 | 4 | 0.0591 |
| Satisfying | 46 | ||||
| Very Good | 36 | ||||
| Excellent | 84 | ||||
| Scarce | 18 | ||||
| Strengths | Limitations |
|---|---|
| The e-learning and e-teaching in these difficult months have allowed us to continue our learning path. In addition, we have had more time available to dedicate to other activities (e.g., reading, fitness) | Lack of fundamental internships |
| Feasibility of timetables | Low quality internet connections |
| Possibility to follow the lectures again at different times during the day, as the presentations are available | Direct interactions with the lecturers are obviously low and for some courses it is fundamental to better understand some topics. Even though the lecturers tried their best to overcome this limitation, the normal approach is not the same. For example, it was not possible to use the microscopes and observe the histology slides. |
| Better concentration and the possibility to record the lectures | I am not happy about the internships. Indeed, the dental profession is extremely practical and after the COVID-19 pandemic, it will be urgent to reorganize to attend the clinic. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varvara, G.; Bernardi, S.; Bianchi, S.; Sinjari, B.; Piattelli, M. Dental Education Challenges during the COVID-19 Pandemic Period in Italy: Undergraduate Student Feedback, Future Perspectives, and the Needs of Teaching Strategies for Professional Development. Healthcare 2021, 9, 454. https://doi.org/10.3390/healthcare9040454
Varvara G, Bernardi S, Bianchi S, Sinjari B, Piattelli M. Dental Education Challenges during the COVID-19 Pandemic Period in Italy: Undergraduate Student Feedback, Future Perspectives, and the Needs of Teaching Strategies for Professional Development. Healthcare. 2021; 9(4):454. https://doi.org/10.3390/healthcare9040454
Chicago/Turabian StyleVarvara, Giuseppe, Sara Bernardi, Serena Bianchi, Bruna Sinjari, and Maurizio Piattelli. 2021. "Dental Education Challenges during the COVID-19 Pandemic Period in Italy: Undergraduate Student Feedback, Future Perspectives, and the Needs of Teaching Strategies for Professional Development" Healthcare 9, no. 4: 454. https://doi.org/10.3390/healthcare9040454