Article Text

Abstract
Introduction The novel (COVID-19 was first reported to have originated in Wuhan, China, in December 2019. This new strain, SARS‐CoV‐2, has spread rapidly worldwide, prompting the WHO to declare the COVID-19 outbreak a global pandemic. The main objective of this cohort study is to determine the risk factors of COVID-19, the modes of COVID-19 vertical transmission, and the maternal and fetal outcomes among non-pregnant and pregnant women and their fetuses.
Methods and analysis This is a multicentre epidemiological study that will involve a prospective cohort. COVID-19 status among consulting non-pregnant and pregnant women in public hospitals in Manila, Philippines, will be determined and monitored for 6–12 months. Swab specimens from the nasopharynx, cervix, rectum, amniotic fluid, placenta, cord blood and breastmilk will be collected during consult and admission for reverse transcription-PCR (RT-PCR) testing. Blood will be collected during the postdelivery period to monitor the women and their neonates for any undue development and determine the antibody development to indicate an infective or non-infective state. Evidence of vertical transmission will be explored with the presence or absence of the virus using the maternal and fetal neonatal RT-PCR and lateral flow antibody status. Descriptive and inferential statistics will be done, including the associations between exposures and risk factors, description of clinical characteristics, and the COVID-19 status of the participants.
Ethics and dissemination The Single Joint Research Ethics Board of the Department of Health has approved this protocol (SJREB 2020-30). The study results will be disseminated through conference presentations, peer-reviewed articles, and various stakeholder public forums and activities.
- COVID-19
- obstetrics
- epidemiology
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This multicentre cohort study in the Philippines will look at the risk factors of COVID-19, the modes of COVID-19 vertical transmission, and the maternal and fetal outcomes among non-pregnant and pregnant women and their fetuses.
Our study will measure multiple outcomes from pregnant and non-pregnant women and determine whether vertical transmission of the virus can occur.
Our study design will allow us to examine the temporal relationship between COVID-19 exposure and different pregnancy outcomes.
Since this is a prospective cohort study during the pandemic, the study can be time-consuming, and potential differential lost to follow-up can introduce bias.
Introduction
Since the novel COVID-19 was first reported in Wuhan, China, in 2019, there has been a rapid increase in cases spreading throughout the world. The WHO has declared it a pandemic.1 This pandemic has had significant repercussions on the worldwide economy, triggering a massive shift in life and societal arrangements.2
COVID-19 is defined as a mild to severe respiratory illness caused by the SARS‐CoV‐2 transmitted mainly by contact with infectious substances such as respiratory droplets or aerosols, surfaces and objects that have been contaminated by the virus. The main clinical feature is manifested by fever, cough and shortness of breath that could progress to pneumonia and respiratory failure.3 There is not much established data that can indicate the risk factors to developing COVID-19.4 The usual sociodemographic characteristics, socioeconomic status and proxy variables, occupational hazards of exposure and travel exposure to areas with cases of the COVID-19 are considered as important associations.5 Sex-disaggregated data for COVID-19 showed equal distribution for males and females but based on the available data, men are more vulnerable and have a higher mortality rate than women. However, current sex-disaggregated data are incomplete and are not a strict basis of health among sexes.6
Based on the study of Knight et al on a limited population, the prevalence of COVID-19 among pregnant women admitted to the hospitals appeared to be the same or lower than the rates in the general population.7 In a WHO-China Joint Mission investigation, 147 pregnant women, both suspected and confirmed COVID-19, were tested, 8% had severe disease and 1% were in critical condition with 14% severe, 6% critical for the overall population.8 A study among pregnant women in Wuhan, China, found that their severity of COVID-19 appeared similar between pregnant and non-pregnant women.9 However, the American College of Obstetricians and Gynecologists indicated that pregnant women might be at higher risk of severe illness, morbidity or mortality compared with the general population.10 The clinical characteristics in COVID-19-infected pregnant patients are identical to those reported for COVID-19-infected non-pregnant patients in the general population. This is indicative of a relatively optimistic clinical course and outcomes for COVID-19 infection relative to SARS-CoV-1 infection.11 12
In a study in Wuhan, four neonates born to infected mothers had minimal evidence of severe outcomes. In addition, two infants developed serious clinical symptoms of facial rashes and ulceration and tachypnoea, which resolved thereafter.13 14 Another study reported that COVID-19 infection during pregnancy is probably not associated with poor maternal or perinatal outcomes and manifests a clinical presentation and severity similar to that in non-pregnant adults. However, data are insufficient to draw strong conclusions.15
There is sufficient evidence that systemic maternal viral infections could affect pregnancy outcomes.16 17 Pregnant women with SARS infection can suffer from high rates of spontaneous abortion, premature birth and intrauterine growth restriction (IUGR).18–20 While the evidence is limited, the potential risk of infected pregnant women and the fetus should be considered. In addition, there also exists a wide research gap regarding COVID-19 and the pregnant population. Furthermore, it remains unclear whether the SARS-CoV-2 can cross the blood–uterine barrier from the mother to the fetus through the transplacental route and to the infant through breast feeding to establish a vertical mode of transmission. Risk factors of COVID-19 are not well established; however, age, sex, socioeconomic status, blood type, comorbidities, among others, were reported in the literature.21 In the local context, some of these characteristics will be helpful in profiling patients, thereby aiding in the diagnosis and prognosis of this illness. However, there is also much that is unknown in pregnant breastfeeding women. Hence, this study aims to find an explanation for the viral behaviour of the COVID-19 in this assumed vulnerable population.
Study aims
The main objective of this study is to determine the risk factors of COVID-19, the modes of COVID-19 vertical transmission and maternal and fetal outcomes among non-pregnant and pregnant women and their fetuses in selected public hospitals in the City of Manila, Philippines. Specifically, this study aims to:
Determine the risk factors associated with COVID-19 in non-pregnant and pregnant women.
Describe the clinical manifestations of COVID-19 among pregnant women and non-pregnant women, including but not limited to fever, sore throat, cough, the difficulty of breathing, pneumonia and diarrhoea (gastrointestinal upset).
Determine how pregnancy affects the clinical symptoms, fetal outcomes of pregnant COVID-19-positive women and if COVID-19-positive pregnant women compared with COVID-19-negative women have poorer pregnancy, maternal and fetal outcomes including, but not limited to abortion, premature labour, congenital malformations and IUGR.
Identify the virus’s presence in the cervix, rectal swab, amniotic fluid, placenta, cord and breast milk to elucidate the sources and mechanism of vertical transmission, if any, from mother to child.
Methods and analysis
Study design and duration
This study is a prospective multicentre cohort involving five public hospitals within the City of Manila, Philippines. The data and specimen collection period will cover around 6–12 months, depending on the COVID-19 situation in the Philippines.
Research sites
Research sites will include the following hospitals: two Department of Health (DOH) hospitals, Jose Fabella Memorial Hospital, Jose Reyes Memorial Medical Center, and three Manila City local government unit (LGU) hospitals, namely Sta Ana Hospital, Justice Abad Santos General Hospital (JasGen), Ospital ng Maynila. These public hospitals were purposively chosen due to their high obstetric and gynaecological (Ob-Gyn) caseloads and the feasibility of achieving the desired recruitment numbers. In addition, these hospitals will provide access to a mix of non-COVID-19 and possible COVID-19 patients.
The Research Institute of Tropical Medicine (RITM) will be involved as the laboratory for processing specimens for the reverse transcription-PCR (RT-PCR) and providing laboratory technical support in the conduct and methods of processing of the collected specimens, including oversight of the immunofluorescence lateral flow antibody testing specifically the IgM and the IgG. Among all the nucleic acid tests, the RT-PCR method is the gold standard for the detection of some viruses and is characterised by rapid detection, high sensitivity and specificity. In addition, the RT-PCR assay is specific and a simple qualitative test.22 23 On the other hand, for immunofluorescence lateral flow antibody testing, we will use the Clungene lateral flow immunoassay kit. This kit has been commercially available in the USA under an Food and Drug Administration (FDA)-approved Emergency Use Authorisation (EUA201121).24 It is an onsite kit with a single panel for IgM/IgG more straightforward detection of COVID-19 in 10–15 min with high sensitivity and specificity for COVID-19 antibodies.25
Appropriate permissions will be obtained from the hospital research sites. In addition, relevant agreements between the principal investigator and the research team with these hospital sites, RITM, and the funding and sponsoring agencies prior to the commencement of the study will also be done.
Study population
The study population will include all pregnant or non-pregnant women who will consult in the identified hospitals, including non-pregnant women consulting for any medical and gynaecological complaints. The pregnant women will be taken at any age of gestation until delivery for follow-up.
Sampling, recruitment and study criteria
All women who will consult for any medical or Ob-Gyn condition at the Departments of Internal Medicine, Ob-Gyn emergency room or labour and delivery rooms during the study period will be included as potential participants. The predetermined number of participants based on the sample size calculation of non-pregnant and pregnant will be filled by purposively sampling women as they access services to the hospital. Once the required sample size is fulfilled in a hospital, recruitment of participants will cease in that hospital. The actual response rate will also be recorded. Participants will be asked to sign an informed consent in a private setting after explaining the study protocol.
Any disease or condition discovered during the ultrasound incidentally will be referred to the institution’s corresponding services as appropriate in order to be assessed, whether malignant or benign. If the benign uterine or adnexal lesions will not have much influence on the course of the disease, the participant will be included. However, the following women will be excluded from the study: (1) women who are less than 18 years old, (2) women who cannot or do not have informed consents, or who cannot commit to the length of time of the study, and those who will not deliver within the catchment area and (3) women with gynaecological malignant or congenital reproductive tract abnormalities or infection as seen on ultrasound. In addition, women excluded due to gynaecological malignant or congenital reproductive tract abnormalities or infection will be referred to the appropriate gynaecological subspecialty services.
Criteria for withdrawal
The participant has the right to withdraw from the project at any time without fear of compromising medical care. Moreover, the participant will be encouraged to explain why she wants to withdraw to enable the research team to document these situations. The following withdrawal criteria will be followed: (1) any decision to deliver somewhere else and (2) any physical or mental health needs that will affect her participation. If medically warranted and if adverse events relevant to the study will occur, this will be reported as soon as possible; the participant may withdraw from the study. In addition, an appropriate referral will be made to assist participants in their medical needs in coordination with the hospital research sites. The procedures will be thoroughly explained to give the participants appropriate health services.
Sample size calculation
There were no similar published studies in the Philippines at the time of the proposal, and the basis of computations were assumptions according to the research design. The sample size needed for the cohort study used a continuity correction method.26 For a two-sided 95% CI, with an 80% power and a ratio of 1, and a least extreme OR to be detected at approximately 2.0, the computed sample size was 576. Assuming an adjustment for an estimated response rate of 90%, the final sample size required will be 640. About 320 non-pregnant and 320 pregnant, seen from the identified five hospital research sites, will be purposively sampled and asked to participate in the study.
Conduct of the study
Each potential participant will undergo screening, recruitment procedures and informed consent for participation. Referral of participants will be done in cases where medical conditions or any adverse events are found during screening, recruitment, or during the conduct of the study, whether related or unrelated to the research. In addition, participants will be approached and asked to participate in the study in the respective hospital. The study will be explained to the participant, after which consent will be secured.
Women will be asked about their medical history and categorised as pregnant or non-pregnant based on a pregnancy test and/or an ultrasound. In addition, the recruited participants will answer a validated self-administered structured COVID-19 infection in adults questionnaire adapted from the New South Wales Department of Health validated (online supplemental file 1). This tool will also capture the socio-demographic characteristics. Moreover, there will be several possible risk factors to be asked, including (1) recent travel history overseas and close contact with a confirmed case of COVID-19, (2) occupation specifically if they are healthcare workers and those in aged or residential care workers and (3) elderly or those with pre-existing medical conditions.
Supplemental material
Most participants will suffer only mild symptoms, and there are indications that the older age group is at higher risk of experiencing severe symptoms. Any underlying illnesses that can increase vulnerability to respiratory disease will be ascertained, including diabetes, chronic lung disease, kidney failure and immunosuppressed conditions at a higher risk of severe disease. For COVID-19 health assessment, all participants will be tested using RT-PCR for SARS-Cov-2 using nasopharyngeal swab specimens. Women will be categorised into four groups: (1) non-pregnant and COVID-19 negative, (2) non-pregnant and COVID-19 positive, (3) pregnant and COVID-19 negative and (4) pregnant and COVID-19 positive.
The non-pregnant women who will have negative RT-PCR results will be instructed to monitor themselves at home for any signs and symptoms of COVID-19 such as fever, cough, and/or body aches, malaise or fatigue, presence of difficulty of breathing, or diarrhoea. In addition, they should prompt a medical consult and be assessed for possible retesting. At any time, should any of these women become symptomatic with these signs and symptoms of COVID-19, they will undergo a repeat nasopharyngeal swab. If they test positive for COVID-19, they will be moved to the non-pregnant (COVID-19+) group. However, no further testing will be done if the non-pregnant (COVID-19-) remains asymptomatic.
The non-pregnant (COVID-19+) group will also undergo cervical and rectal swabbing on admission, including a rapid antibody test (IgG/IgM) (see figure 1).
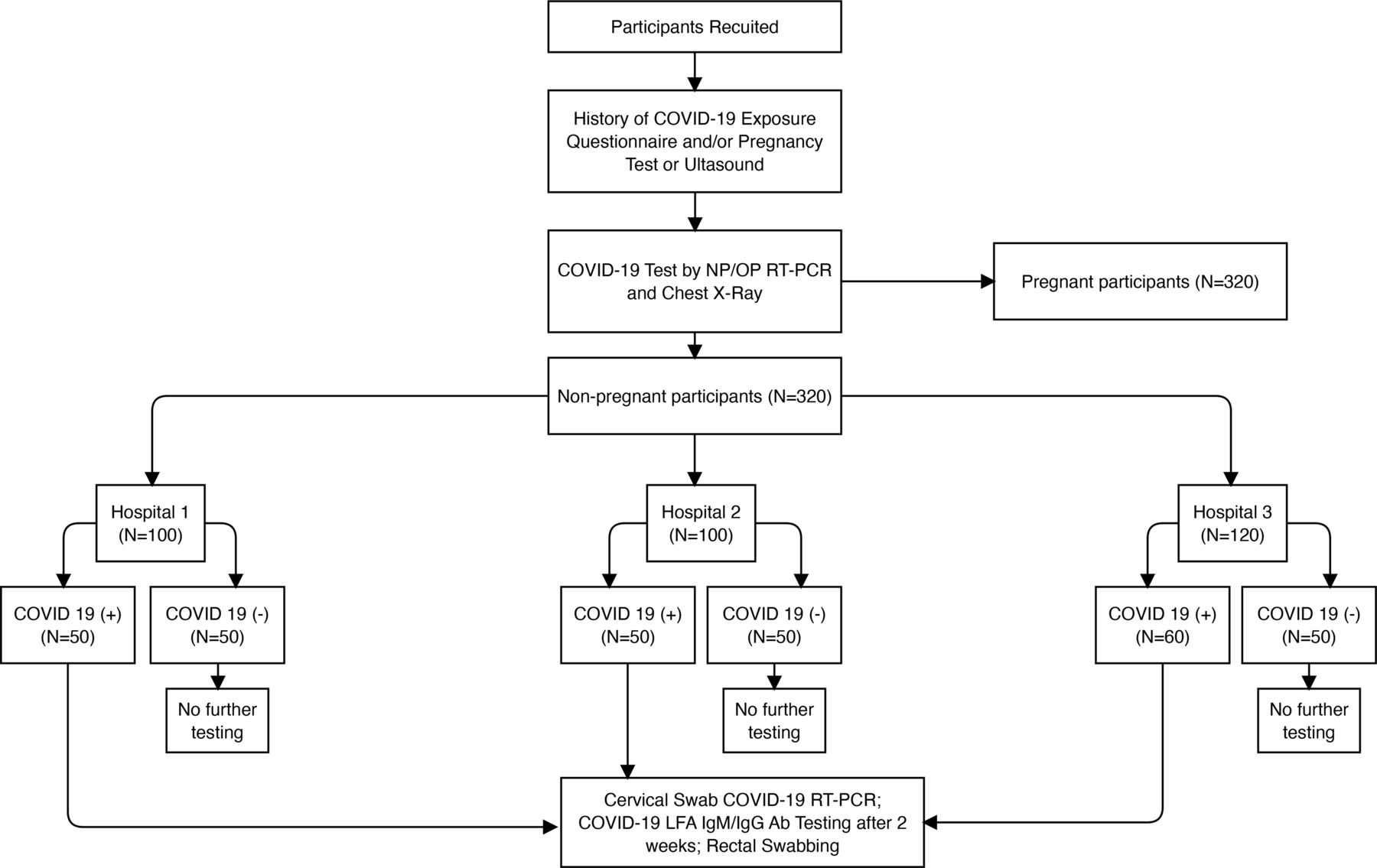
Diagrammatic flow chart for all participants. LFA, lateral flow assay; NP/OP, nasopharyngeal/oropharyngeal; RT-PCR, reverse transcription-PCR.
All pregnant (COVID-19−) women will be asked to monitor themselves at home for any signs and symptoms of COVID-19. Furthermore, if any pregnant COVID-19 negative women become symptomatic with any of the signs and symptoms of COVID-19 disease, they will also undergo a repeated nasopharyngeal swab. In addition, they will be moved to the pregnant (COVID-19+) group if they test positive for COVID-19. All deemed asymptomatic may still harbour COVID-19 because of community transmission, nasopharyngeal/oropharyngeal swab and non-conventional swab tests for RT-PCR will be done regardless of the COVID-19 status. Moreover, both the pregnant (COVID-19−) and (COVID-19+) groups will undergo RT-PCR swabs of the cervix, rectum, placenta, amniotic fluid, umbilical cord blood and breastmilk (see figure 2).

{kind=link}
{kind=link}
Algorithm for pregnant women. CS, caesarean section; NP, nasopharyngeal; RT-PCR, reverse transcription-PCR.
To summarise, all non-pregnant (COVID-19+) and pregnant (COVID-19+) women will similarly undergo the following:
Chest X-ray on admission to determine the possibility of COVID-19 and severity of the disease. The use of chest X-ray will be specifically done because many cases of COVID-19 patients are asymptomatic. There are reports that though they are asymptomatic, they exhibit some X-ray findings and further evaluation is needed. While it may not be specific for COVID-19 itself, this can serve as another tool to assess for suspected COVID-19 or any respiratory diseases in our local setting such as pulmonary tuberculosis.
Cervical swabbing for RT-PCR testing to determine if the cervix can harbour the virus, and for pregnant women, it may play a role in vertical transmission to the fetus.
Rectal swabbing to check for the presence of the virus and at what point they will test negative in comparison to the nasopharyngeal/throat swab.
SARS-Cov-2 lateral flow IgG/IgM antibody testing.
For pregnant women, the cervical swab RT-PCR test will help provide an understanding of whether transmission to the fetus can occur by vaginal birth as the baby passes through the cervix and birth canal. Thereafter, the newborn will also be tested to confirm the hypothesis of possible vertical transmission. This step may also elucidate if a caesarean section (CS) can spare the baby from the vertical transmission. As far as the research team is aware, there is no previous investigation using cervical swabbing to determine the presence of the COVID-19 virus in pregnant women. Hence, this study will test this concept.
In addition, the pregnant cohort will be taken in at any age of gestation (AOG) at the time of recruitment. The AOGs will be categorised from <12 weeks, 13–24 weeks, 24–32 weeks, >33 weeks as the effect of COVID-19 in pregnancy in the different ages of gestation is not yet known. Moreover, the pregnant (COVID-19 +and COVID-19−) women will be grouped into three categories:
Miscarriage group (up to 23 6/7 weeks)—they may come for vaginal bleeding, threatened abortion, or complete abortion. These women will undergo an amniotic fluid swab, a placental PCR swab and a fetal swab of products of conception whenever possible.
Not in labour group (from 24 weeks)—these women will undergo a Biophysical profile with Doppler to track fetal growth and detect IUGR or fetal jeopardy.
In labour/for CS group—(from 24 weeks)—on delivery, amniotic fluids and umbilical cord blood samples will be taken for RT-PCR SARS-CoV-2 testing. After the delivery of the placenta, another RT-PCR swab of the placental fetal side will be obtained. The newborn will also have nasopharyngeal and rectal sampling immediately within 2 hours after postdelivery. Breastmilk will also be sampled within 24–48 hours.
All neonates of COVID-19 positive and negative mothers will also undergo nasopharyngeal swabbing and rectal swabbing for PCR testing and capillary blood extraction for SARS-Cov-2 IgG, IgM antibody test.
The lateral flow assay (LFA) antibody test will also be used to analyse the collected samples. The results will be interpreted against the RT-PCR and the antibody test IgM and IgG of the mother on admission, during labour, and only a few hours prior to the delivery. In addition, the LFA Antibody tests will also be used for cord blood and breastmilk as they can indicate the pathway of transmission.
Statistical analysis
Descriptive statistics of the patient’s self-reported sociodemographic information, medical and clinical history, and any travel exposure, any encounter/exposure with people with COVID-19 will be calculated. Additionally, these independent variables (risk factors/sociodemographic factors) will be evaluated against the maternal outcomes of more severe disease during the course of pregnancy, the effect on the comorbidity diseases, the fetal outcomes such as abortion (miscarriage), preterm labour, congenital anomaly, IUGR among others and the pregnancy outcomes of the route of delivery to determine any correlation with maternal, pregnancy and fetal outcomes.
In addition, the patient’s RT-PCR tests will be compared with the neonatal PCR test results to determine vertical transmission. Furthermore, the mechanism of this vertical transmission will be tested. The RT-PCR of different tissues collected, such as from the cervix, rectum, amniotic fluid, placenta, cord blood and breastmilk, will be analysed against the results of the mother and child. Since the results of the RT-PCR of the mother and neonate and the results of the IgG/IgM antibody tests for the mother and neonate are dependent, the McNemar’s test will be used to examine (1) vertical transmission between mother’s RT-PCR tests and neonatal RT-PCR test, (2) IgG/IgM antibody tests between mother and neonate, and (3) IgG/IgM antibody tests outcome and RT-PCR tests between mothers and neonates.
Univariate and multivariate analyses will examine the associations between COVID-19 and possible risk factors. Logistic regression models will be used to estimate the crude and adjusted ORs with 95% CIs. Risk factor variables that are clinically relevant and sociodemographic variables will be included a priori into the logistic regression models. In addition, Wald’s test will be used to test the significance of the risk factor variables. Logistic regression analyses will be done in R (http://www.r-project.org). P values ≤0.05 will be considered statistically significant.
Participant and public involvement statement
The participants and the public were not involved in the design and implementation of the protocol.
Ethical considerations and dissemination
The study’s research protocol received ethical approval from an Independent Research Ethics following the national guidelines involving studies with the Department of Health and LGU hospitals. The data gathered and the participant information will be kept confidential and private following the Philippines’ Data Privacy Act of 2012.
Right to privacy and data protection plan
The principal investigator and research team will not disclose the identities of the participants at any time. All the information provided by the participants will be kept in confidence, and real names will be deidentified and will not appear in the study. This information will be processed and stored in a secure hard drive with password access only available to the principal investigator. All identifiable information and data will have a corresponding code number. Only the principal investigator will have access to all the records. The principal investigator will oversee the completeness and accuracy of the data collected. All sources of information will be made available for review. All study data shall be recorded, and investigators are responsible for the integrity of the data, such as accuracy, completeness, legibility, originality, timeliness and consistency.
Methods of dealing with adverse events, serious events and indemnification policy
Any adverse events will be referred to the proper specialists for management. In addition, monitoring of the conduct of the study will be performed periodically to ensure Good Clinical Practice (GCP). Investigators and other staff directly involved in the study are GCP certified as required by the ethics committee and relevant institutional ethics review committee of the participating institutions.
Dissemination
The results will be actively disseminated through conference presentations, peer-reviewed journals and various stakeholder activities.
Discussion
There remains a wide knowledge and research gap regarding COVID-19. The scarcity of literature and the enfolding public health emergency is an opportune time to understand how COVID-19 behaves in humans, particularly among pregnant and non-pregnant women. The gender differences can be seen in this emerging story among Philippine cases, which could have a beneficial impact in defining local standards of practice and improved therapeutic management.
The evolving nature of the SARS-CoV-2 virus and its behaviour that escalated to a pandemic in the past year has forged a moral and public health collaboration for medical experts, health professionals and scientists to come together and deal with one of the most challenging periods in human history and medicine. Hence, this need to find explanations will help respond to and eventually resolve this pandemic. This is further highlighted with the emerging patterns of more aggressive and highly infectious variants like the B.1.1.1.7 (UK variant), the South African variant (B.1.351), the Brazilian variant (P.1), the delta variant (B.1.617.2) and the Philippine variant (P.3), which have been associated with the recent upsurge of cases locally.27–29
Risk factors are not too clear as regards to the epidemiology of COVID-19. Age, sex, socioeconomic status, blood type, comorbidities, among others, were observed in the literature. In the local context, some of these characteristics will be helpful in profiling patients, aiding in the diagnosis and prognosis of this illness. Knowing the answers to these questions can help the medical profession manage pregnant women once COVID-19 is diagnosed in pregnancy appropriately.
As this virus spreads throughout the population, the higher the likelihood that more women will be infected, whether pregnant or not. It is therefore essential that more people receive accurate information on COVID-19. In addition, practical strategies on clinical care could be instituted if more is known about this emerging infection. For example, the study may point to whether mothers should be isolated from the baby at birth or if breast feeding can be allowed to continue, especially in low-resource settings where the mother may not have access to any other source of artificial or human milk.
The findings of this study will hopefully be used to add to the knowledge gaps in the understanding of the COVID-19 in pregnant and non-pregnant women, the risk factors, clinical manifestation and disease course. Most importantly, it can shed insights on the understanding of vertical transmission. The findings will guide policy and practice interventions in dealing with a future outbreak of SARS-COV2 or a similar infectious disease situation and/or pandemic in its acute and ongoing phase.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank the following: Research Institute of Tropical Medicine—Dr Celia Carlos; Manila City Officials Mayor Honorable Francisco 'Isko Moreno' Dumagoso; Office of the Vice Mayor Honorable Honey Lacuna-Pangan, Head of the Health Cluster, Dr Arnold Pangan, and the Manila City Councilors headed by Councilor Joel Chua. Manila City Health Department Staff—Dr Arnold Pangan, Dr Gina Pardilla, and Dr Rosalina R Tan and staff; Fabella Memorial Medical Center, 1003 Lope de Vega St, Santa Cruz, Manila, 1003 Metro Manila - Cynthia Ubaldo-Anzures and Maria Lu Andal; Jose Reyes Memorial Medical Center, Rizal Ave, Santa Cruz, Manila, Metro Manila—Leilani Coloma and Eleyneth Valencia; Ospital ng Maynila, 719 Quirino Avenue, corner Roxas Blvd, Malate, Manila, 1004 Metro Manila—Cecile Cuaresma—Cruz and Carol Martin; Sta Ana Hospital, New Panaderos Ext, Santa Ana, Manila, Metro Manila—Arlene Dominguez and Abigail Reccio; Justice Abad Santos General Hospital, Numancia St, Binondo, Manila, Metro Manila—Ryan Capitulo and Vanessa De Guzman.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors We confirm that each author has met the BMC Trials authorship requirements. EL-C and RBS contributed equally to this paper and are joint first authors. Specifically, EL-C and RBS made substantial contributions to the concept and research design. FMH, ESB, METV-U, MSFC and MUL assisted in specific components of the research design of the manuscript. ZJGR and ESB drafted the article and visualisation. All have critically revised and approved the final version of the manuscript.
Funding This research is partly funded by the Australia Awards and Alumni Engagement Program, the Philippine Obstetrical and Gynecological Society Foundation, and the Department of Science and Technology—Philippine Council for Health Research and Development (no fund grant number available).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.