1. Introduction
The source of COVID-19, officially designated by the World Health Organization, is infection with the SARS-CoV-2 virus (severe acute respiratory syndrome coronavirus 2) [
1].
Infection with the SARS-CoV-2 virus can result in a respiratory disease that mainly attacks the lungs, provoking symptoms ranging in severity from slight or moderate to severe, including fever, headaches, fatigue, dry cough, myalgia, and diarrhea. However, recent clinical studies have indicated that this type of pathogen has a vast infectious capacity to spread into the extrapulmonary tissues, provoking multi-organ insufficiency in patients with severe impairment. The capacity of the SARS-CoV-2 infection to invade the central nervous system and the peripheral nervous system currently represents a major concern [
2].
Recent studies have reported certain neurological pathologies associated with SARS-CoV-2 virus infection. These studies have classified certain manifestations connected to the central nervous system, such as headaches, vertigo, impaired consciousness, acute cerebrovascular disease, and epilepsy, in addition to other symptoms related to the peripheral nervous system, such as hyposmia, anosmia, hypogeusia, ageusia, myalgia, and Guillain-Barre syndrome [
3]. The most frequent neurological complication that has appeared in the SARS-CoV-2 infection is ischemic stroke [
4].
A thoracic computed tomography (CT) scan is recommended for cases of suspected or confirmed SARS-CoV-2 infection, due to its association with major lung disease, with the aim of evaluating and following its progression. Compared to the thoracic CT-scanning, thoracic radiography (X-rays) is not as reliable, and cannot be used to identify disease symptoms in the early stages, but in moderate to advanced phases, it may indicate the evolution of acute respiratory distress. Moreover, real-time polymerase chain reaction (RT-PCR) tests are used to diagnose infection with the SARS-CoV-2 virus. Imaging investigations based on CT-scanning have proven useful for diagnosis, even if an initial RT-PCR test was falsely negative [
5].
The study was performed within a 10-month period, between 1 October 2020, and 31 August 2021, within the Neurology Department and Laboratory of Magnetic Resonance Imaging of “Sf. Andrei” Emergency Hospital in Constanta. The Constanta County Emergency Clinical Hospital’s Ethics Committee for Clinical Studies (registration number 34/26.11.2021) authorized this study, which followed the guidelines of the Declaration of Helsinki. Prior to enrollment, all individuals provided written informed consent.
Following subjective and objective clinical examinations, and based on paraclinical investigations, the study group consisted of 150 cases of patients admitted to the neurology department of the hospital with various neurological diseases and who were declared to be positively infected with the virus according to the presence of ribonucleic acid (RNA) SARS-CoV-2, as determined by RT-PCR test.
3. Discussion
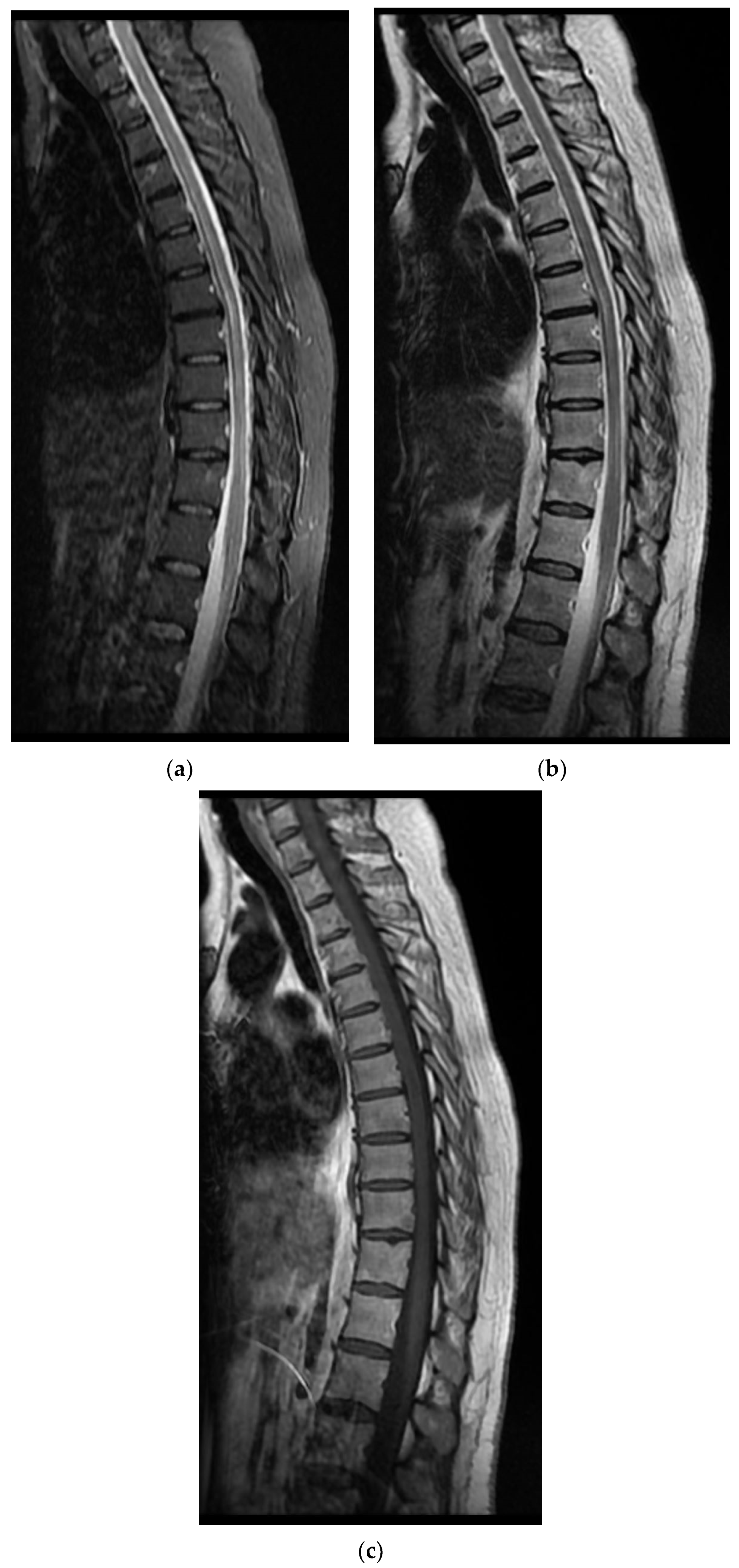
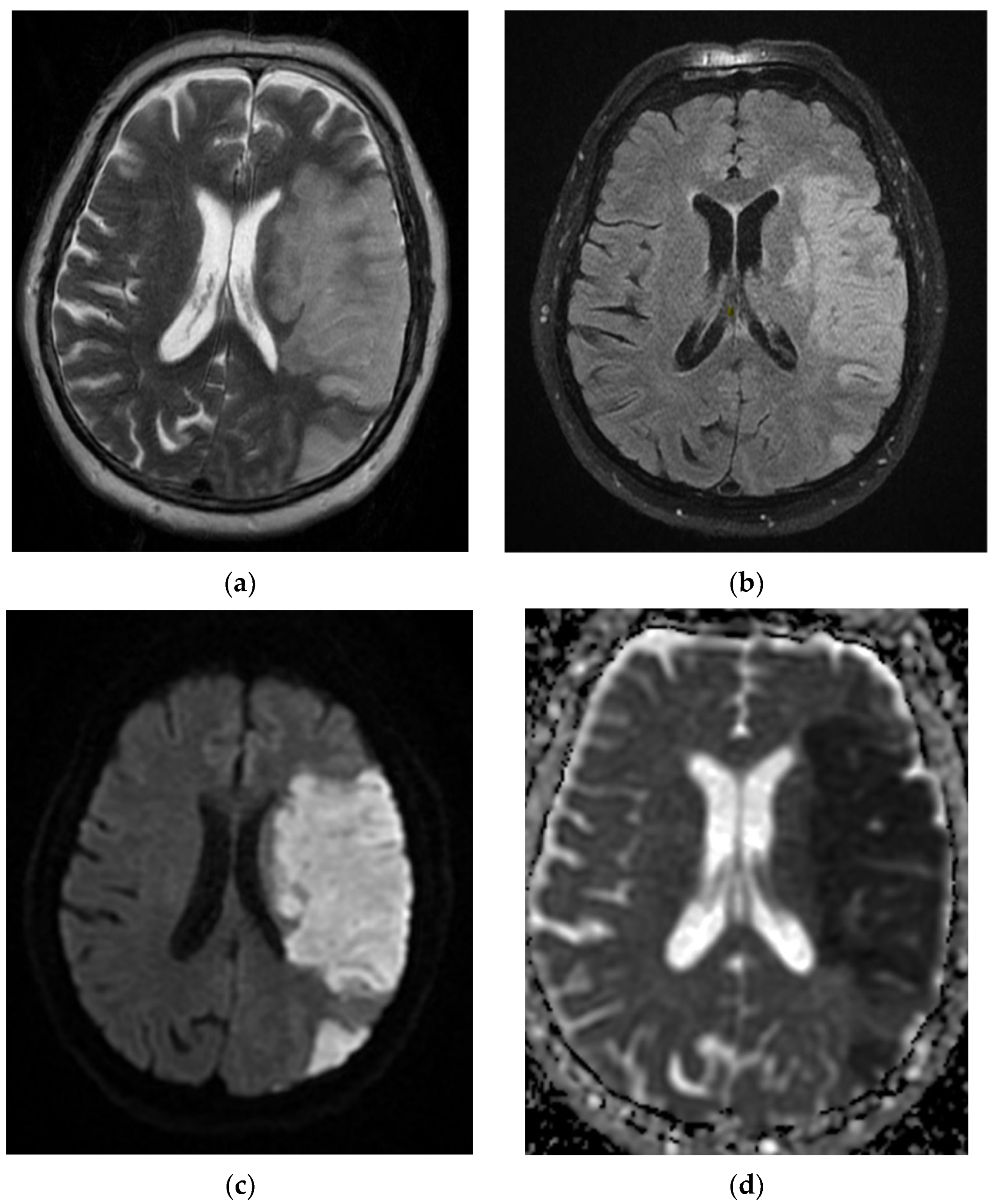
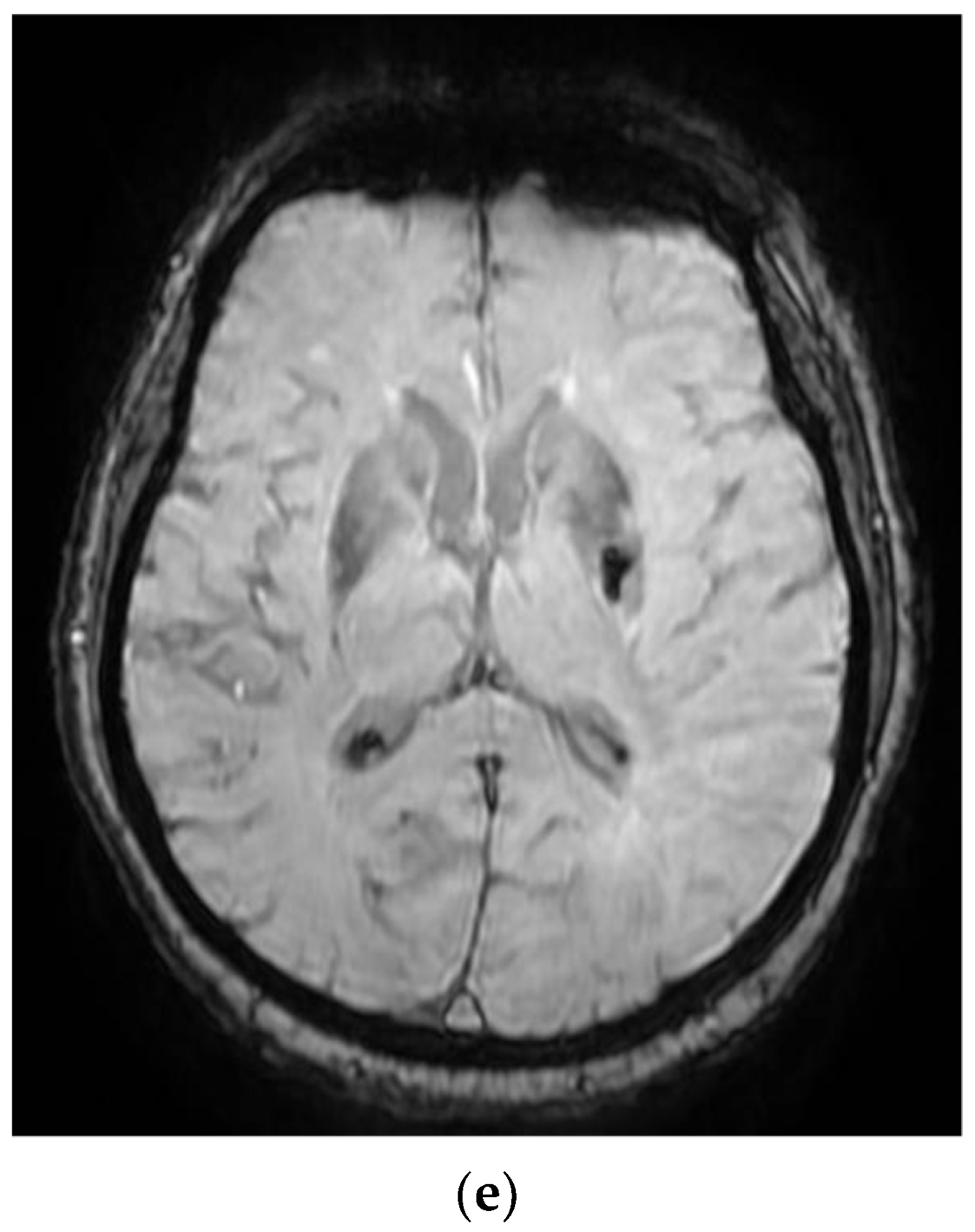
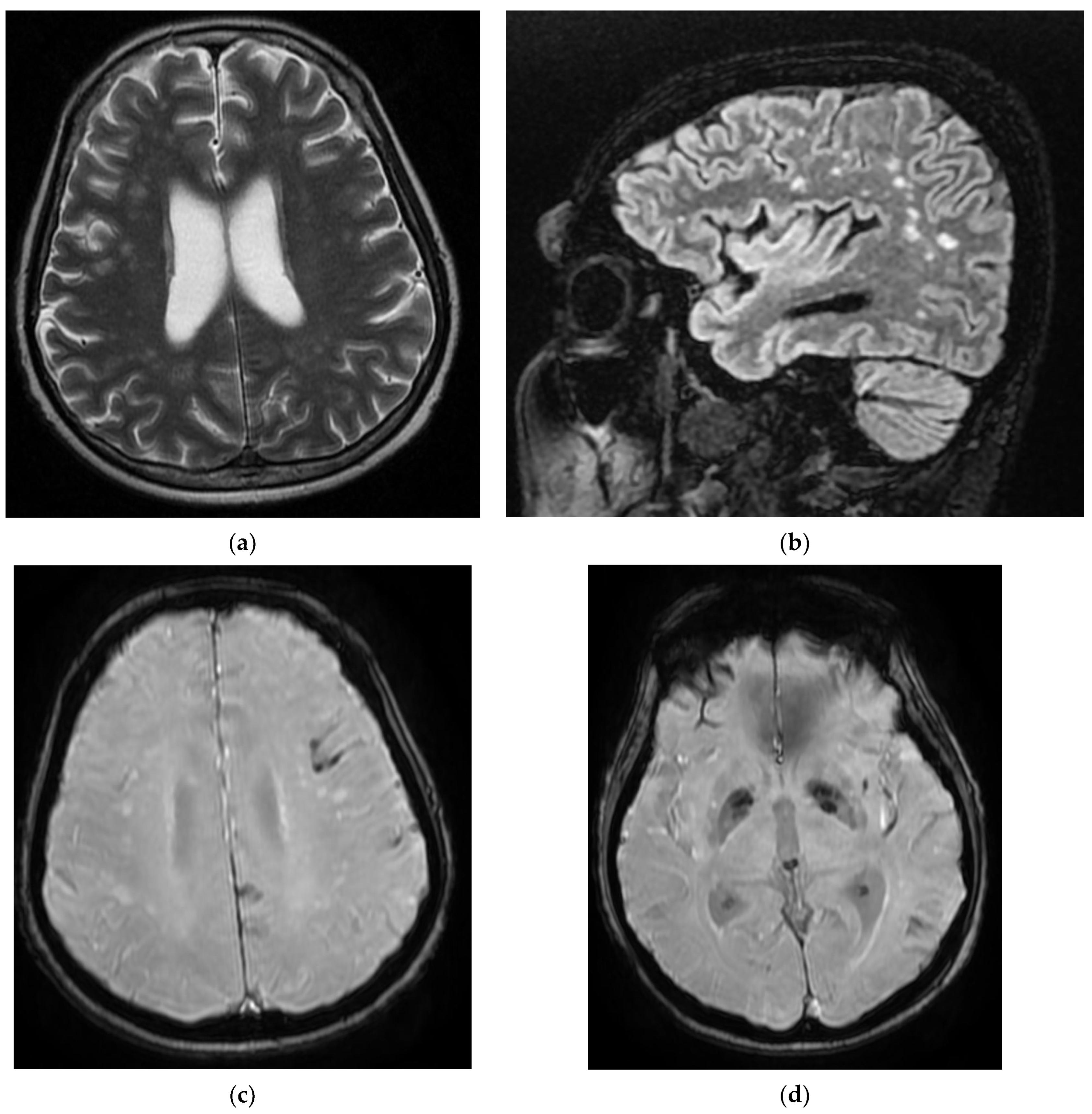
The COVID-19 patients in our 10 case reports presented with a complex panel of neurological diagnostics, including myelitis with paraparesis, acute ischemic stroke in various territories with hemiplegia, cerebrovascular disease with involuntary movements, seizures, and left transverse–sigmoid–jugular venous subacute thrombosis.
Cerebrovascular disease, in addition to certain other neurological features, has often been associated with acute SARS-CoV-2 infection. Numerous pathophysiological mechanisms have been postulated to explain the SARS-CoV-2-related prothrombotic condition, as both direct and indirect consequences of the viral infection. Aside from hypercoagulable characteristics, it is hypothesized that SARS-CoV-2-related endothelitis and microangiopathy lead to hemorrhagic stroke. Consequently, intracranial hemorrhage in COVID-19 patients could be the result of hemorrhagic transformation of ischemic stroke, original hemorrhagic stroke, or traumatic intracranial hemorrhage.
The processes underlying the apparition of these neurological symptoms remain unknown. Numerous ideas have been advanced since SARS-CoV-2 was first detected, such as that the neuroinvasion of the virus comes from its ability to enter via the olfactory groove or directly into the nervous system via circulation [
6,
7]. However, these results might be the result of secondary immunological processes and a severe inflammatory state induced by infection, or of significant hypoxia caused by critical illness and concomitant disorders [
6,
7].
We have identified various neurological pathologies which can be correlated to the positive diagnosis of the RNA SARS-CoV-2 testing by RT-PCR tests or which represent only incidental findings following a clinical or paraclinical examination by magnetic resonance imaging.
The types of disorders encountered during the study are acute stroke, subacute stroke, hemorrhagic stroke, ischemic stroke that then becomes hemorrhagic, carotid transitory ischemic stroke, vertebrobasilar insufficiency, cerebrovascular disease, venous thrombosis, demyelinating lesions, sequela lesions, secondary determinations, tumoral formation, myelitis, seizures, Guillain–Barre syndrome, paraesthetica syndrome, paraparesis, myasthenia gravis, multiple sclerosis, Rasmussen’s encephalitis, movement lacunar stroke, amnestic syndrome, and disk protrusion.
The most frequent pathology was ischemia, which is strongly connected to a diagnosis of COVID-19 and is represented by cerebral strokes with various ages and types of evolution, with a total number of 85 cases of cerebral strokes, 44 cases of acute cerebral strokes, 36 cases of subacute cerebral strokes, and 5 cases of carotid transitory ischemic stroke. This classification might also include four cases of ischemic ictus, two cases of movement lacunar stroke, two cases of amnestic syndrome, three cases of stroke sequela, and two cases of sequela lesions. Among the patients who had been diagnosed only with the cerebrovascular disorder, we found six cases and four cases of demyelinating lesions, which might have had a vascular-ischemic sublayer. We also encountered a case of vertebrobasilar syndrome.
The hemorrhagic stroke associated with the SARS-CoV-2 virus occupied a significant place in a group of 26 cases, of which 20 patients presented with a hemorrhagic acute stroke and another 6 patients presented with a hemorrhagic stroke transformed from an ischemic stroke.
Moreover, the neoplasia pathology associated with COVID-19 had substantial representation, as we found three cases with tumoral formations and five cases with secondary determinations. We found two cases of venous cerebral thrombosis associated with SARS-CoV-2 infection and three cases of convulsive crisis.
The range of neurological pathologies associated with the infection of SARS-CoV-2 is vast, and we might include other pathologies here, such as myelitis, Guillain–Barre syndrome, paresthesia, paraparesis, myasthenia gravis, multiple sclerosis, Rasmussen’s encephalitis, and disk protrusion.
Ghannam et al. indicated that infection with the SARS-CoV-2 virus results not only in respiratory disease, and that neurological complications are frequently experienced. Associated neurological pathologies are often encountered, including ischemic and hemorrhagic strokes, Guillain–Barre syndrome, encephalitis, and convulsions. In a studio located in Wuhan, China, out of 214 cases with SARS-CoV-2 infection, 78 had neurological complications. Patients with severe SARS-CoV-2 infection have a higher risk of developing neurological complications. The manifestations point to the central nervous system and peripheral nervous system, and symptoms such as headaches, vertigo, muscular weakness, sensory alteration, and impaired consciousness may also appear [
8].
As part of the classification according to age groups, it was noticed that the greatest number of cases were of patients aged 70–80 years, representing 58 out of the 150 cases that were evaluated.
This age group was followed by 60–70-year-olds, with 40 cases, followed by the 80–90-year-old age group, in which we found 26 cases. In these first three groups, ischemic vascular pathology was most frequently presented. Next, we found the group of 50–60-year-olds, with 17 cases, where inflammatory pathologies and venous thrombosis were the most frequently presented.
For the other age intervals, the number of cases decreased dramatically, with one case for the group of 30–40 years, seven cases for 40–50 years, and one case for 90–100 years.
Sullivan et al. evaluated neurological pathologies according to patient age, individual age, or the age interval of the group, with the aim of classifying the frequency of neurological complications associated with SARS-CoV-2 and that affect children (under the age of 19 years), young adults (between 19 and 50 years), and adults (over the age of 50). The patients with an average age between 60 and 69 years presented the greatest number of associated neurological disorders, and the patients aged equal to or under 9 years presented the lowest association. Patients over the age of 50 years presented the greatest number of cerebrovascular disorders. The most frequent associated neurological pathology was observed in over half of the patients in this group [
9].
Patients with COVID-19 displayed a predominance of respiratory and nervous system symptoms. Among several patients of the latter, there were complaints of loss of smell and taste, ataxia, and impairment to peripheral nervous system, which might reflect the SARS-CoV-2 virus presenting with neurotoxicity.
Six key clock genes, including
CLOCK,
BMAL1,
PER1,
PER2,
CRY1, and
CRY2, control circadian rhythm. Clock genes are involved in the regulation of metabolic and immunological responses, including the release of pro-inflammatory interleukins. As a result, lifestyle modifications, including adjustments in the light regime, a reduction in the amplitude of room temperature, a change in the timing of eating, and the allocation of a food according to its calorific value throughout the day, contribute to metabolic abnormalities and the apparition of a low-intensity systemic inflammatory process [
10]. Additionally, the circadian clock governs fundamental bodily processes, including lung capacity and sleeping as well as activities in the neural tissue that contribute to neurological and psychiatric illnesses, such as auto-aggression and neuropathic pain. Additionally, several studies have discovered a link between the development of certain symptoms and particular circadian chronotypes that might aid in the creation of chronotherapy and enhance therapy by administering medication in line with the patient’s circadian rhythm [
11,
12].
Sleep phase abnormalities were the most prevalent circadian rhythm abnormalities. Boiko et al. [
11] discovered that COVID-19 infection in antecedents increased patients’ susceptibility to developing circadian rhythm abnormalities, including delayed sleep phase disorder. Additionally, it was shown that individuals with COVID-19 exhibit elevated levels of trait and state anxiety. The high incidence of delayed sleep phase disorder might be a result of both the neurotropic properties of SARS-CoV-2 and isolation linked with the COVID-19 outbreak. Therefore, the impact of a modification in light exposure on everyday activities was detected under lockdown settings, meaning a change of the rhythm by three or more hours. This has resulted in decreased exposure to natural light, which has a detrimental effect on the main circadian oscillator, as well as physical and nutritional activities. Amongst circadian rhythm abnormalities, delayed sleep phase disturbance is most prevalent in the post-COVID-19 era and is related to an increased degree of anxiety in these individuals.
Global Impact of the COVID-19 Pandemic on Different Areas in Low- and Middle-Income Countries
Formerly, it was thought that the SARS-CoV-2 virus was limited to the respiratory system, mostly impacting the lungs; nevertheless, new investigations have demonstrated the virus’s multisystem impact, most notably impacting brain tissue. COVID-19 illness may indeed be associated with a variety of mental disorders, including post-traumatic stress disorder, obsessive–compulsive disorder, anxiety, delirium, and depression, either directly or indirectly. It has the potential to exacerbate pre-existing mental health problems or to precipitate the genesis of new psychiatric diseases [
13]. Increasing COVID-19 instances, elevated illness burden, and a lack of social support may all contribute to short-term mental health concerns, while economic losses also present because mandated lockdowns could have a long-term effect on people’s mental health [
14].
Due to a global scarcity of frontline staff dedicated to containing the epidemic, several governments have reassigned psychiatrists to critical care settings to handle COVID-19 patients. As a result, mental hospital outpatient departments were closed, resulting in a massive increase in mental health difficulties in some countries. In these cases, imposed lockdowns and restrictive restrictions regarding physical isolation have robbed many patients of access to essential mental health treatment [
15].
The COVID-19 pandemic has highlighted underdeveloped health systems in low- and middle-income countries (LMICs) and significant treatment disparities, at least in the area of mental health. As a result of these issues, individuals with severe mental illness die earlier, have more physical ailments, and receive less medical treatment than the general population [
16].
Additionally, it is vital to educate the public in low- and middle-income countries on the acknowledgment of mental health problems as diseases, the importance of social and familial assistance, and the importance of avoiding social stigma of those who suffer from mental health disorders.
Most neurological symptoms have been shown to develop early throughout the course of the disease (in some studies, the median time to hospital admission was 1–2 days) [
15,
16]. Several individuals lacking classic COVID-19 manifestations (fever, coughing, anorexia, and diarrhea) presented to the hospital with solely neurological manifestations, as in our study. As a result of the impact of SARS-CoV-2 infection on neurological diseases, we must closely monitor patients with COVID-19 for neurological symptoms, particularly those with serious infections that could have led to their mortality. Additionally, during the COVID-19 epidemic era, clinicians must include SARS-CoV-2 infection as a differential diagnosis whenever meeting patients with these neurological signs to minimize late or incorrect diagnosis and to limit the spread.
The purpose of this research was to provide a complete assessment of neurological symptoms related with SARS-CoV-2 infection and to detail the course of disease and outcomes of COVID-19 individuals who developed neurological symptoms in 10 representative patients from Constanta Clinical County Hospital, which is situated in a low–middle-income country. This work may provide critical new clinical information on COVID-19, assisting physicians in raising awareness of its association with neurological symptoms and diagnosis of COVID-19 infection in low- and middle-income countries.
It is particularly significant to note that, in our study, contrary to other studies, the patients firstly presented with neurological features, and COVID-19 infection was subsequently discovered. Moreover, quick clinical decline or aggravation may be accompanied with a neurological event, including stroke in patients with severe COVID-19, contributing to the disease’s high mortality rate. Additionally, doctors might include SARS-CoV-2 infection as a differential diagnosis when meeting patients with these neurological signs during the COVID-19 pandemic period to prevent late diagnosis or misdiagnosis as well as to limit the spread. To facilitate future clinical care, additional precise epidemiological data and further pathophysiology findings are required.
Global restrictions imposed to prevent and control the spread of a new COVID-19 wave resulted in a financial crisis in LMICs, restricting access to food and other basic requirements due to border closures. The combined consequences of poverty, climate change, and the COVID-19 epidemic have exacerbated food insecurity in some LMICs. COVID-19, thus, worsened an already-existing food crisis in these countries due to the imposition of government restrictions and lockdown measures that restricted work options and income.
Food insecurity is a major socioeconomic and public health problem in low- and middle-income nations. It is associated with adverse health effects and a reduction in self-reported health status, decreased micronutrient intake, fruit and vegetable consumption, weight gain, and birth abnormalities. As with challenges experienced by other resource-related issues (e.g., housing instability, energy uncertainty), inequality and poverty might exacerbate nutritional deficiencies, illness, and disease management. Individuals who experience poverty have much worse health outcomes and less access to healthcare than those who do not. Poor nutrition may exacerbate pre-existing illnesses, such as inadequate glucose control in diabetic patients, final renal disease in patients with chronic kidney disease, as well as affect the treatment of other chronic diseases. COVID-19′s presence in LMICs has restricted access to healthcare and impacted attempts to treat, diagnose, immunize, and monitor other infectious diseases. Food instability may further aggravate health problems and expenditures for families with children that have specific healthcare requirements, or for persons with disabilities.
A number of examples can be provided depicting the impact of the COVID-19 pandemic on LMICs.
Afghanistan’s continuous struggle has created several difficulties for the country’s population. Afghanistan has seen a significant rise in food shortfalls because of its reliance on neighboring nations during the epidemic [
17]. Individuals attain food security when they have continuous physical and economic access to an adequate supply of safe and nutritious food that meets their dietary demands and preferences. Food scarcity, political unrest, and the third wave of COVID-19 have made it impossible to obtain basic supplies. Consequently, folks are forced to contend with the COVID-19 pandemic amid economic collapse and despair. At this crucial point, worldwide efforts are essential to ameliorate food security.
The growth in the number of instances of the illness has the potential to overwhelm the health system, as does noncompliance with social distance measures and the introduction of variants of concern in LMICs. This rise in the transmission curve may also create conditions favorable for the emergence of further changes in the virus’ structure and DNA. As a result, genomic monitoring methods are essential to detect and describe these variants as well as to determine if the vaccines against the virus that are currently in use are efficacious.
The development of efficient and dependable infectious disease monitoring systems is critical for establishing a high-quality public healthcare system and reducing the mortality rates in low- and middle-income countries. Monitoring helps facilitate the accessibility of records and knowledge and decreases the burden and propagation of unfavorable healthcare events. This allows for a rapid response in public health, efficient implementation of methods and countermeasures, and a review of suggested treatments, the rapid detection of new illnesses, promoting health security and stability for people living in LMICs.
Healthcare workers (HCWs) have been critical in containing the pandemic and mitigating its effects. Increased working hours and frequent exposure to critically ill patients have major consequences for the health and wellbeing of physicians, which have previously been disregarded.
Infectious disease epidemics have always posed a threat to public health, especially in Africa, where outbreaks have exploded in recent years [
18]. Although several infectious diseases have emerged in Africa, such as Ebola and certain other epidemic-prone infections, insufficient focus has been placed on the development of health surveillance systems. The inadequacy of the region’s healthcare monitoring techniques have only recently been identified. Africa suffers from a shifting epidemiology of disease, a deficient healthcare system, and a scarcity of resources. Only a vigilant monitoring system can ensure that the best use of its available resources are made in an effective and strategically managed manner. Measures are needed to rapidly detect potential public health threats. This could be accomplished via the use of appropriate, efficient, and lengthy surveillance methods.
Dengue fever is a serious public health concern in Africa [
18] and the COVID-19 pandemic has exacerbated this concern. COVID-19 accelerates the transmission of a variety of illnesses, including Zika, yellow fever, measles, mucormycosis, Lassa fever, and HIV, as has been seen in several nations on the African continent. The limits imposed in response to the COVID-19 pandemic have resulted in the suspension of vector management initiatives that aid in the management of these diseases. To avert further public health disasters, urgent and interdisciplinary measures to dengue fever epidemic management in African nations are necessary.
COVID-19 cases have impoverished Nigeria’s healthcare system and resulted in additional neglect of persons suffering with mental illness [
18]. In general, there is a demand for equitable access to healthcare resources, but there is a need for adequate attention and treatment for mental health patients, which is rising in Nigeria.
The COVID-19 epidemic has hit public health emergencies in Bangladesh, a low–middle-income nation in South Asia. The resulting surge of sickness cases may generate an overburdening of the health system. This rise in the contagion curve may also encourage further alterations in the virus’ structure and DNA. It is important to find, monitor, and characterize these polymorphisms and determine the efficacy of existing vaccinations against these variants.
India’s healthcare sector is suffering significant difficulties as a consequence of the lack of resources to combat the COVID-19 pandemic, with HCWs also suffering the consequences [
19]. There is an urgent need to address these flaws in the healthcare system to provide a consistent and ongoing supply of high-quality treatments in India.























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}