Article Text

Abstract
Objectives To assess the risk of severe COVID-19 outcomes in patients with autoimmune rheumatic diseases (ARDs) and transplant recipients compared with matched general population comparators.
Design Population-based matched cohort study using administrative health data sets.
Setting British Columbia, Canada.
Participants All adults with test-positive SARS-CoV-2 infections. SARS-CoV-2-positive patients with ARDs and those with transplantation were matched to SARS-CoV-2-positive general population comparators on age (±5 years), sex, month/year of initial positive SARS-CoV-2 test and health authority.
Outcome measures COVID-19-related hospitalisations, intensive care unit (ICU) admissions, invasive ventilation and COVID-19-specific mortality. We performed multivariable conditional logistic regression models adjusting for socioeconomic status, Charlson Comorbidity Index, hypertension, rural address and number of previous COVID-19 PCR tests.
Results Among 6279 patients with ARDs and 222 transplant recipients, all SARS-CoV-2 test positive, risk of hospitalisation was significantly increased among patients with ARDs (overall ARDs (adjusted OR (aOR) 1.30; 95% CI 1.19 to 1.43)); highest within ARDs: adult systemic vasculitides (aOR 2.18; 95% CI 1.17 to 4.05) and transplantation (aOR 10.56; 95% CI 6.88 to 16.22). Odds of ICU admission were significantly increased among patients with ARDs (overall ARDs (aOR 1.30; 95% CI 1.11 to 1.51)); highest within ARDs: ankylosing spondylitis (aOR 2.03; 95% CI 1.18 to 3.50) and transplantation (aOR 8.13; 95% CI 4.76 to 13.91). Odds of invasive ventilation were significantly increased among patients with ARDs (overall ARDs (aOR 1.60; 95% CI 1.27 to 2.01)); highest within ARDs: ankylosing spondylitis (aOR 2.63; 95% CI 1.14 to 6.06) and transplantation (aOR 8.64; 95% CI 3.81 to 19.61). Risk of COVID-19-specific mortality was increased among patients with ARDs (overall ARDs (aOR 1.24; 95% CI 1.05 to 1.47)); highest within ARDs: ankylosing spondylitis (aOR 2.15; 95% CI 1.02 to 4.55) and transplantation (aOR 5.48; 95% CI 2.82 to 10.63).
Conclusions The risk of severe COVID-19 outcomes is increased in certain patient groups with ARDs or transplantation, although the magnitude differs across individual diseases. Strategies to mitigate risk, such as booster vaccination, prompt diagnosis and early intervention with available therapies, should be prioritised in these groups according to risk.
- transplant medicine
- rheumatology
- public health
- epidemiology
- COVID-19
Data availability statement
Data may be obtained from a third party and are not publicly available. These data are held by Population Data BC. Restrictions apply to the availability of these data, which were used under licence for the current study and so are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study examines the risk of COVID-19-related hospitalisation, intensive care unit admission, invasive ventilation and COVID-19-specific mortality in patients with autoimmune rheumatic diseases or transplantation.
A large administrative health data set permitted capturing all individuals in British Columbia, Canada, who had tested positive for SARS-CoV-2 infection between 6 February 2020 and 15 August 2021.
Each individual with an autoimmune rheumatic disease or transplantation was matched with as many individuals as possible, up to five, from the general population without an International Classification of Diseases code for that particular condition, of same age (±5 years), sex, month/year of initial positive SARS-CoV-2 test and local health authority.
As with other administrative data studies, uncertainties around diagnostic accuracy and misclassification are possible.
Our data set did not account for variables such as body mass index, obesity or smoking.
Introduction
The COVID-19 pandemic has resulted in over 428 million confirmed cases and 5 million deaths globally as of 24 February 2022.1 Several risk factors for the severe COVID-19 outcomes of hospitalisation, intensive care unit (ICU) admission, invasive ventilation and mortality, among those infected with the SARS-CoV-2 virus, have been identified, including age, gender and comorbidities such as diabetes, hypertension and obesity.2–4
Individuals living with autoimmune rheumatic diseases (ARDs) and those with transplantation may be at increased risk of COVID-19 infection and severe COVID-19 outcomes, given the already increased risk of other infections and use of pharmacological immunosuppression required for many of these diseases.5 6 Patients with ARDs and transplantation often have poorer health status and more comorbidities than the general population, which could further contribute to severe COVID-19 outcomes.7–9 Some observational studies have assessed severe COVID-19 outcomes in patients with rheumatic diseases and transplantation.10–16 However, few studies have been truly population based, sample sizes have typically been small, samples prone to selection bias (eg, hospitalised) are common and many studies have not accounted for important confounders (eg, socioeconomic status). Additionally, results have been conflicting, with certain studies showing increased risk among patients with rheumatic diseases and transplantation and others showing no increased risk, compared with the general population. Given these limitations, it is unknown whether and to what extent these populations are truly at increased risk of severe COVID-19 outcomes and addressing this knowledge gap is a priority for patients and providers as the pandemic continues.
We conducted a matched cohort study using British Columbia (BC), Canada administrative health databases to estimate the risk of hospitalisation, ICU admission, invasive ventilation and mortality, after adjusting for confounders in ARD and transplant patient groups following positive SARS-CoV-2 test, each compared with the general population.
Methods
Data sources
Universal healthcare coverage is available for all residents of BC, Canada (population ~5.1 million in 2020). Population Data BC provides access to all provincially funded healthcare services data since 1990, including: all outpatient medical visits,17 hospital admissions and discharges,18 demographic data,19 cancer registry20 and vital statistics.21 Furthermore, Population Data BC holds the comprehensive prescription drug database PharmaNet,22 which includes all pharmacy-dispensed medications for all BC residents since 1996.
The BC Centre for Disease Control (BCCDC) Public Health Laboratory is the reference laboratory for infectious diseases in BC. All cases of COVID-19 were confirmed by positive SARS-CoV-2 PCR test from the BCCDC23 and linked to the above administrative health data by Personal Health Number by Population Data BC.
Study sample
Among all individuals in BC who tested positive for COVID-19 between 6 February 2020 and 15 August 2021, we identified all patients who had ever been diagnosed—since database inception or registration—with: (1) ARDs: rheumatoid arthritis (RA), psoriasis/psoriatic arthritis (PsO/PsA), ankylosing spondylitis (AS), any systemic autoimmune rheumatic diseases (SARDs, including systemic lupus erythematosus (SLE), Sjogren’s syndrome (SjS), systemic sclerosis, inflammatory myositis, adult systemic vasculitides); or (2) transplantation (including solid organ and bone marrow).
All individuals meeting disease definitions were identified for the period 1990–2021 using the definitions described below. Patients with ARDs were defined with two International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) or ICD-10 codes for the given ARD at either physician visits or hospitalisation, at least 2 months apart within a 2-year period. Transplant recipients were defined with at least one ICD-9-CM or ICD-10 code for transplantation, from hospitalisation. See online supplemental table 1 for ICD codes.
Supplemental material
The index date of COVID-19 diagnosis was determined by the earliest positive PCR test. Only individuals meeting the disease definition prior to their index date were included. Each individual with an ARD or transplantation was matched with as many individuals as possible, up to five, from the general population without an ICD code for that particular condition (eg, no code for SLE in the comparator group when the patient group was individuals with SLE), of same age (±5 years), sex, month/year of initial positive SARS-CoV-2 test and local health authority.
Severe COVID-19 outcomes
Incident COVID-19-related hospitalisations, ICU admissions and use of invasive ventilation were determined using hospital discharge abstracts.18 COVID-19-related hospitalisation was defined as any hospitalisation with a COVID-19 diagnosis (ICD-10: U071) within 30 days following a positive SARS-CoV-2 test and ICU admission as the same, but with days spent in ICU >0. This 30-day time window has been used by others investigating the risk of severe COVID-19 outcomes.24–28 The following Canadian Classification of Health Intervention codes were used to identify invasive ventilation: 1.GZ.31.CAND; 1.GZ.31.CAEP; 1.GZ.31.CAPK; 1.GZ.31.CRND; 1.GZ.31.GPND in hospitalised patients. Both short-term (<96 hours) and long-term (≥96 hours) invasive ventilation were included within 30 days of a positive SARS-CoV-2 test. Deaths with a primary ICD-10 code for COVID-19 were ascertained using vital statistics.21 As a sensitivity analysis, deaths within 60 days of a positive SARS-CoV-2 test were assessed whether or not COVID-19 was listed as a cause of death, also using vital statistics.
Statistical analysis
We compared baseline characteristics of patients with ARDs or transplantation, each with matched comparators. The risk of each severe COVID-19 outcome in each patient group relative to the general population was estimated in separate models using multivariable conditional logistic regression, adjusted for age, socioeconomic status (neighbourhood income quintile based on census data), Romano modification of the Charlson Comorbidity Index (which includes diabetes),29 hypertension, rural address and number of previous COVID-19 PCR tests as a proxy for situations that increase the risk of infection. For the Charlson Comorbidity Index, points given for rheumatologic disease were excluded for patients with RA and SARDs.
Patient and public involvement
Our patient partners (BC, CK, PM and PM) were involved in the design, reporting and dissemination plans for this research project.
Results
Study population
As of 15 August 2021, there were 147 301 individuals with a positive SARS-CoV-2 test in BC. Of these, there were 6279 individuals with an ARD and 222 with transplantation, each of which were matched with up to five comparators (table 1). Mean age was 54.3 years for patients with ARDs and 54.3 years for transplant recipients. As expected, mean Charlson Comorbidity Index score was greater for patients with ARDs and transplantation relative to matched general population comparators.
Baseline characteristics of patients with autoimmune rheumatic diseases, transplant recipients and matched comparators
COVID-19-related hospitalisations
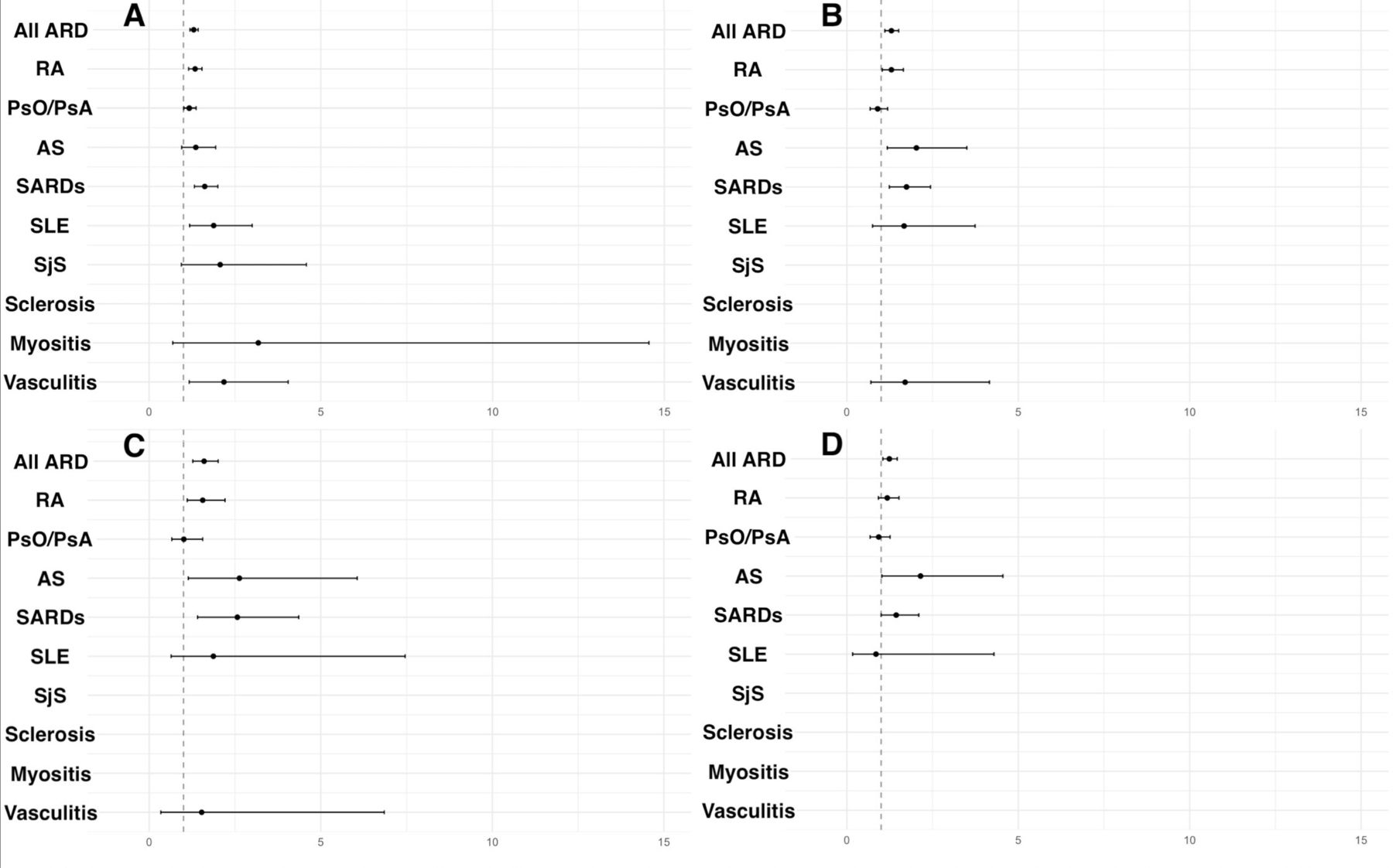
Overall, 12.4% of patients with an ARD had a COVID-19-related hospitalisation compared with 9.1% of comparators (figure 1; online supplemental table 2). The overall risk of hospitalisation was significantly higher for patients with ARDs (ie, all ARDs combined) versus comparators (adjusted OR (aOR) 1.30; 95% CI 1.19 to 1.43). The largest significant risk of hospitalisation was seen in patients with vasculitides (aOR 2.18; 95% CI 1.17 to 4.05) relative to matched comparators.

Risk of (A) hospitalisations, (B) intensive care unit (ICU) admissions, (C) invasive ventilation, and (D) COVID-19-specific mortality among patients with autoimmune rheumatic diseases compared with matched comparators from the general population. Results presented as ORs with 95% CIs. Disease groups without a point estimate were too small to be calculated. ARD, autoimmune rheumatic disease; AS, ankylosing spondylitis; PsO/PsA, psoriasis/psoriatic arthritis; RA, rheumatoid arthritis; SARD, systemic autoimmune rheumatic disease; SjS, Sjogren’s syndrome; SLE, systemic lupus erythematosus.
Over half of all COVID-19-positive transplant recipients were hospitalised (51.8%), compared with 10.0% of comparators (figure 2; online supplemental table 3). Transplant patients had more than a 10 times increase in risk of COVID-19-related hospitalisation compared with the general population (aOR 10.56; 95% CI 6.88 to 16.22).

{kind=link}
{kind=link}
Risk of (A) hospitalisations, (B) intensive care unit (ICU) admissions, (C) invasive ventilation, and (D) COVID-19-specific mortality among transplant recipients compared with matched comparators from the general population. Results presented as ORs with 95% CIs.
ICU admissions
Overall, 3.6% of patients with ARDs had a COVID-19-related ICU admission, compared with 2.6% of comparators (figure 1; online supplemental table 2). Relative to those without an ARD, the overall risk of ICU admission was increased (aOR 1.30; 95% CI 1.11 to 1.51) among patients with ARDs. The risk was significantly increased for patients with RA (aOR 1.30; 95% CI 1.03 to 1.65), AS (aOR 2.03; 95% CI 1.18 to 3.50) and SARDs (aOR 1.74; 95% CI 1.24 to 2.44).
A total of 22.1% of transplant recipients were admitted to ICU following a positive SARS-CoV-2 test relative to 3.7% of comparators (figure 2 and online supplemental table 3). The risk of ICU admission was significantly higher for transplant recipients (aOR 8.13; 95% CI 4.76 to 13.91) when compared with matched comparators.
Invasive ventilation
A total of 1.6% of patients with ARDs received invasive ventilation relative to 0.9% of matched comparators (figure 1; online supplemental table 2). The overall risk of invasive ventilation was increased for patients with ARDs versus comparators (aOR 1.60; 95% CI 1.27 to 2.01). Relative to those without an ARD, the risk of invasive ventilation was also increased for those with RA (aOR 1.56; 95% CI 1.11 to 2.21), AS (aOR 2.63; 95% CI 1.14 to 6.06) and overall SARDs (aOR 2.57; 95% CI 1.51 to 4.36).
Overall, 8.6% of transplant recipients received invasive ventilation, compared with 1.3% of comparators (figure 2; online supplemental table 3). The risk of invasive ventilation was significantly increased for transplant recipients relative to comparators (aOR 8.64; 95% CI 3.81 to 19.61).
Mortality
The case fatality rate for patients with ARDs was 3.7% compared with 2.7% in comparators (figure 1; online supplemental table 2). Overall, patients with ARDs were at increased risk of COVID-19-specific mortality (aOR 1.24; 95% CI 1.05 to 1.47). However, within individual ARDs only patients with AS were at increased risk of mortality (aOR 2.15; 95% CI 1.02 to 4.55) when compared with the general population.
Transplant recipients experienced a 12.2% case fatality rate, compared with 2.2% for comparators (figure 2 and online supplemental table 3). Transplant recipients were at significantly increased risk of COVID-19-specific mortality (aOR 5.48; 95% CI 2.82 to 10.63) when compared with the general population.
The sensitivity analysis for mortality within 60 days of a positive SARS-CoV-2 test showed results similar to COVID-19-specific mortality (online supplemental table 4).
Discussion
In this matched cohort study, with data from the entire province of BC, Canada, we found that overall, patients with ARDs or transplantation had a greater risk of severe COVID-19 outcomes compared with matched individuals without these conditions, although the magnitude differed widely across disease groups and specific outcomes. The risk of COVID-19-related hospitalisation was significantly increased for patients with some ARDs, specifically overall ARDs (30%), RA (34%), PsO/PsA (17%), SARDs (62%), SLE (88%), systemic vasculitides (118%) and transplantation (over 10 times) when compared with the general population. Moreover, the risk of ICU admission was significantly increased only for patients with overall ARDs (30%), RA (30%), AS (103%), SARDs (74%) and transplantation (over eight times). The risk of receiving mechanical ventilation was increased for those with overall ARDs (60%), RA (56%), AS (163%), SARDs (157%) and transplantation (over eight times). The risk of COVID-19-specific mortality was increased only for patients with overall ARDs (24%), AS (115%) and transplantation (over five times).
Our findings in populations with ARDs are congruent with the literature. Two studies with small sample sizes from Boston, USA (one hospital based (n=289) and one from a regional healthcare system (n=156)) found an increased risk of ICU admission among patients with ARDs compared with matched general population comparators (OR 2.08; 95% CI 1.09 to 3.96 and OR 2.92; 95% CI 1.002 to 8.49).10 11 Shin et al found a 26% increased risk of severe COVID-19 (combination of oxygen, ICU admission, invasive ventilation or death)12 among South Korean patients with ARD (n=8222) compared with matched comparators. Both Boston-based studies found no increased risk of mortality among patients with ARDs compared with matched comparators, which supports our findings.10 11 We found an increased risk of mortality among patients with AS, which could be due to persistent chest immobility and associated impaired respiratory function.30 31 Further research on severe COVID-19 outcomes in patients with AS is required.
Transplant recipients were at an increased risk of all severe COVID-19-related outcomes compared with general population comparators. A recent meta-analysis of individuals hospitalised with COVID-19 found greater ICU admission among solid organ transplant recipients compared with the general population (pooled estimate: 35.8%; 95% CI 28.7% to 43.3% versus 23.1%; 95% CI 18.0% to 28.6%), respectively, although the authors noted the limitation of significant study heterogeneity (I2=70.7% for ICU admission among solid organ transplant recipients).14 Previous studies have also found an increased risk of COVID-19-related mortality among transplant recipients; however, many of these studies have the limitation of examining only hospitalised patients,32–34 which is a sample prone to selection bias. In our analyses, over half of all transplant recipients were hospitalised for COVID-19.
One plausible explanation for this increased risk in patients with ARDs and transplantation that has been put forward is increased comorbidities.35–37 In our population, mean Charlson Comorbidity Index was 0.8 and 2.6 for patients with ARDs and transplantation, respectively, and 0.7 and 0.5 for matched comparators. However, our analyses adjusted for the Charlson Comorbidity Index (which includes diabetes), as well as hypertension. Additionally, another explanation is the possibility of increased surveillance and Berkson’s bias in this population which cannot be ruled out. This may contribute to increased hospitalisation due to perceived increased risk by clinicians.
A factor likely impacting the risk of severe outcomes was the SARS-CoV-2 vaccine. Individuals deemed ‘clinically extremely vulnerable’ were prioritised to book earlier vaccination appointments beginning 29 March 2021 in BC, which included those with solid organ, bone marrow and stem cell transplants, and those with immunosuppressant prescriptions (eg, most disease-modifying antirheumatic drugs and biologics commonly prescribed to individuals with ARDs).38 This may have contributed to effect estimates of severe COVID-19 outcomes, although there is evidence that the SARS-CoV-2 vaccine may be less effective in these populations.39 40 Unfortunately, for this study we did not have access to vaccination data.
Given the increased risk of severe COVID-19 outcomes in certain patient groups with ARDs and transplantation, there is a need for further research on the effectiveness of SARS-CoV-2 vaccination in these populations. For instance, assessing the risk of breakthrough COVID-19 infections relative to the general population as well as the most effective intervals between booster vaccines will have important clinical implications. Increased surveillance of patients by their medical care teams at rheumatology and transplant medicine practices may be important to support early diagnosis and supportive care interventions, as well as rapid treatment with new therapies including oral antiviral therapies indicated for adults with mild to moderate COVID-19. Finally, primary prevention measures such as mask mandates and paid sick leave may continue to be effective tools in reducing the number of individuals infected with SARS-CoV-2 and experiencing the resulting severe COVID-19 outcomes.
Our findings should be interpreted within the study’s limitations. First, diagnoses of ARDs and transplantation were identified using ICD codes. While uncertainty around diagnostic accuracy cannot be entirely excluded, we used strict case definitions for administrative databases. While misclassification of exposure status and comorbidities is possible, any misclassification is expected to be non-differential and bias the results towards the null, yielding conservative risk estimates. Second, although we adjusted for all known confounders available, our database did not account for variables such as body mass index, obesity or smoking. Risk factors may also vary by disease (eg, across rheumatic disease types). Third, the small sample size of some patient populations with COVID-19 did not allow us to calculate the risk for certain outcomes (eg, risk of ICU admission or mortality for myositis or SjS).
Conclusion
To the best of our knowledge, this is the largest and first truly population-based study assessing four separate COVID-19 outcomes among patients with ARDs and transplantation. We found that the risk of severe COVID-19 outcomes differed extensively across patient groups and the severe outcomes. Transplant recipients were at a substantially increased risk of severe COVID-19 outcomes, whereas patients with ARDs were at no increased risk for many outcomes and a mild or moderately increased risk for others, specifically patients with RA, PsO/PsA, AS, SARDs overall, SLE and adult systemic vasculitides. Strategies to mitigate risk, such as booster vaccination, prompt diagnosis and early intervention with available therapies,41–43 should be prioritised in these groups according to risk.
Data availability statement
Data may be obtained from a third party and are not publicly available. These data are held by Population Data BC. Restrictions apply to the availability of these data, which were used under licence for the current study and so are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
The Behavioural Research Ethics Board of The University of British Columbia approved this study (H20-01914).
Acknowledgments
We acknowledge the contributions of our patient partners (BC, CK, PM and PM) to this research project. We would like to thank the Ministry of Health of British Columbia and Population Data BC for providing access to the administrative data. Access to data provided by the data steward(s) is subject to approval, but can be requested for research projects through the data steward(s) or their designated service providers.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JAA-Z had full access to the data in this study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors have read, provided critical feedback on intellectual content and approved the final manuscript. Concept, design and planning: JAA-Z, JML, HX, DL, JAK, JE. Drafting the initial version of the manuscript: SM. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis and data verifying: JAA-Z, SM, NL. Obtained funding: JAA-Z, JML, HX, DL, JAK. JAA-Z is the guarantor of the study.
Funding This work was supported by the Michael Smith Foundation for Health Research (grant number: COV-2020-1075) and the BC SUPPORT Unit (grant number: C19-PE-V3). JAA-Z is supported by the BC Lupus Society Scholar Award and is the Walter and Marilyn Booth Research Scholar. JML receives research support through a Michael Smith Health Professional Investigator Award. DL is supported by the Mary Pack Chair in Rheumatology Research by The University of British Columbia and the Arthritis Society of Canada.
Disclaimer All inferences, opinions and conclusions drawn from this research are those of the authors and do not reflect the opinions or policies of the data stewards. No personal identifying information was made available as part of this study.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.