
sTREM-1 Predicts Disease Severity and Mortality in COVID-19 Patients: Involvement of Peripheral Blood Leukocytes and MMP-8 Activity



 , , , , , , , , , ,
, , , , , , , , , ,  and add
Show full author list
and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Design and Participants
2.3. Severity Assessment
2.4. Laboratory Methods
2.5. Cytokine Measurements
2.6. Detection of Plasma sTREM-1 and MMP-8
2.7. Analysis of TREM-1-Positive Cells
2.8. Statistical Analysis
2.9. Ethical Approval
3. Results
3.1. Demographic Data, Clinical and Laboratory Characteristics
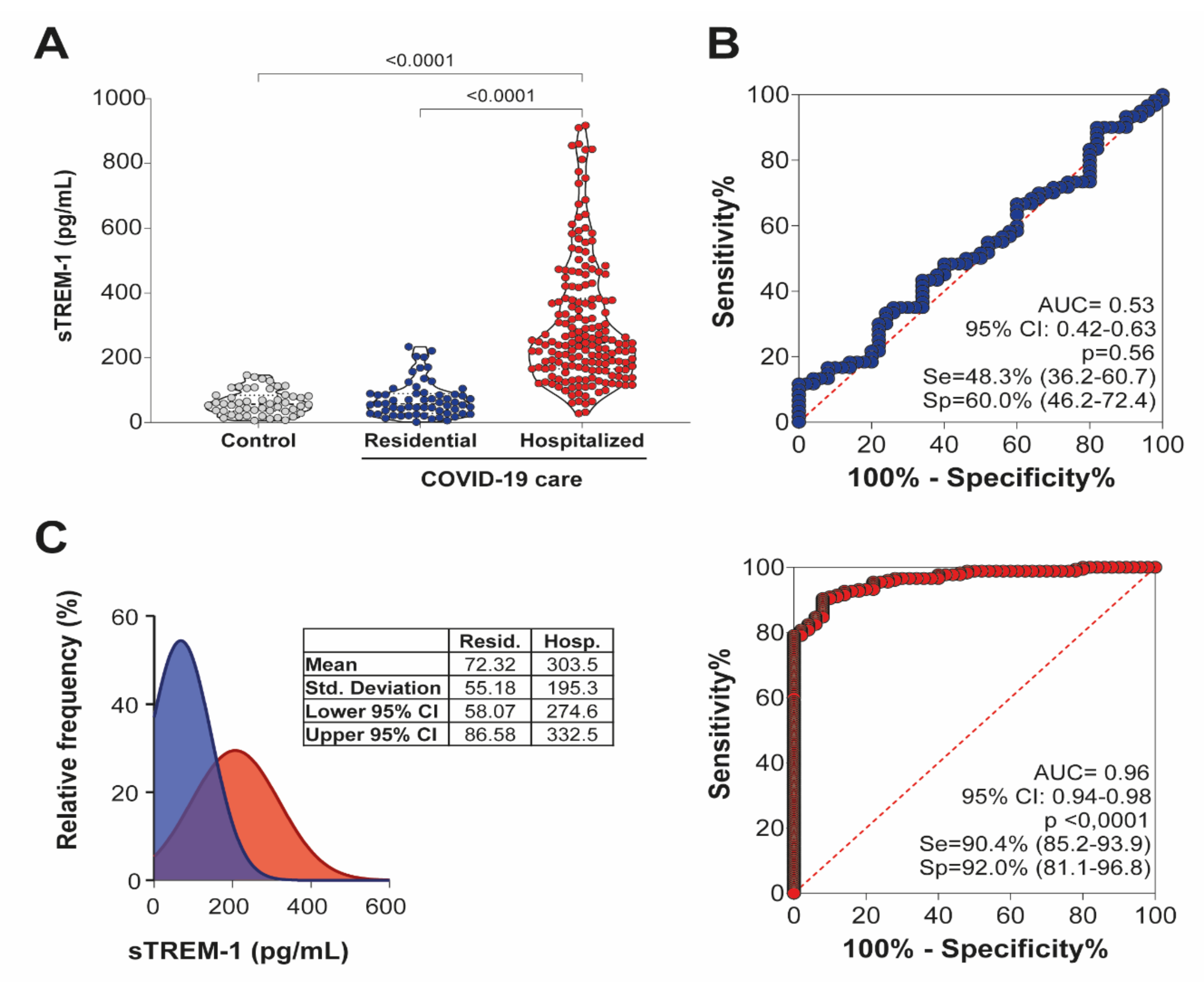
3.2. Significant Association between sTREM-1 Release and Disease Severity
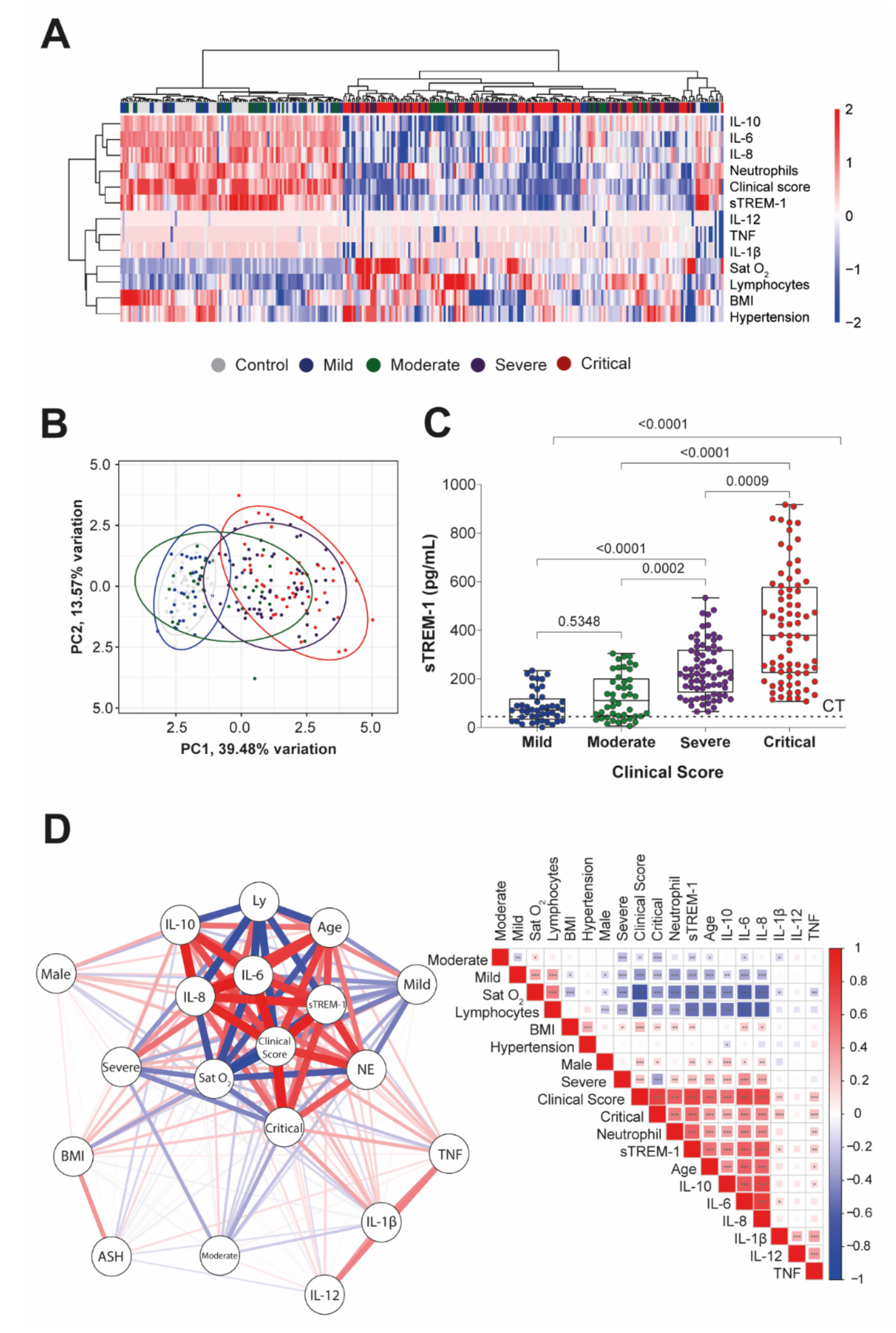
3.3. sTREM-1 Levels Increase with Clinical Disease Severity and Correlate with Comorbidities and the Production of Inflammatory Mediators in Patients with COVID-19
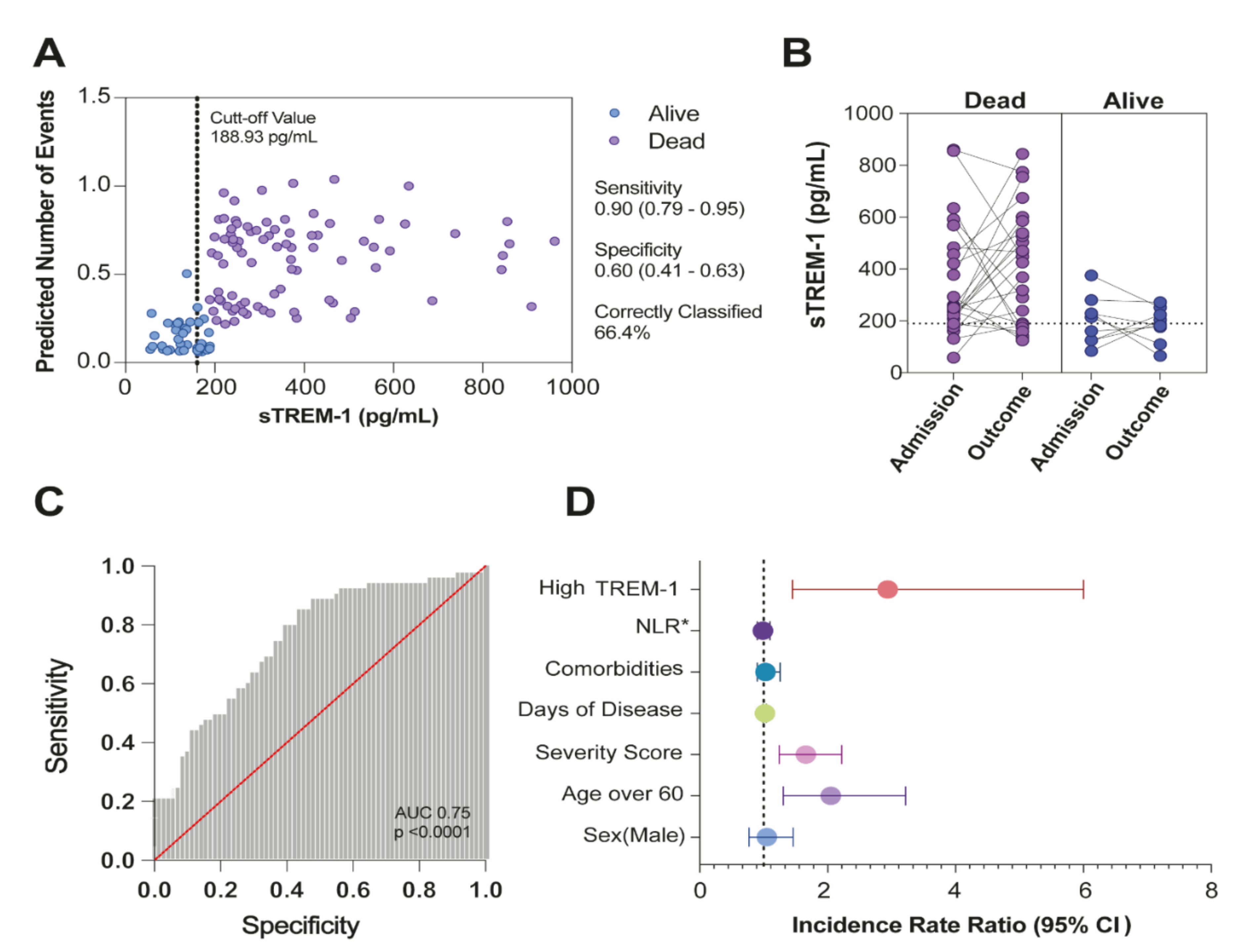
3.4. Multivariate Regression Analysis for the Prediction of Death and the Incidence Rate Ratio Value of sTREM-1 for the Expectation of Mortality Risk in COVID-19 Patients
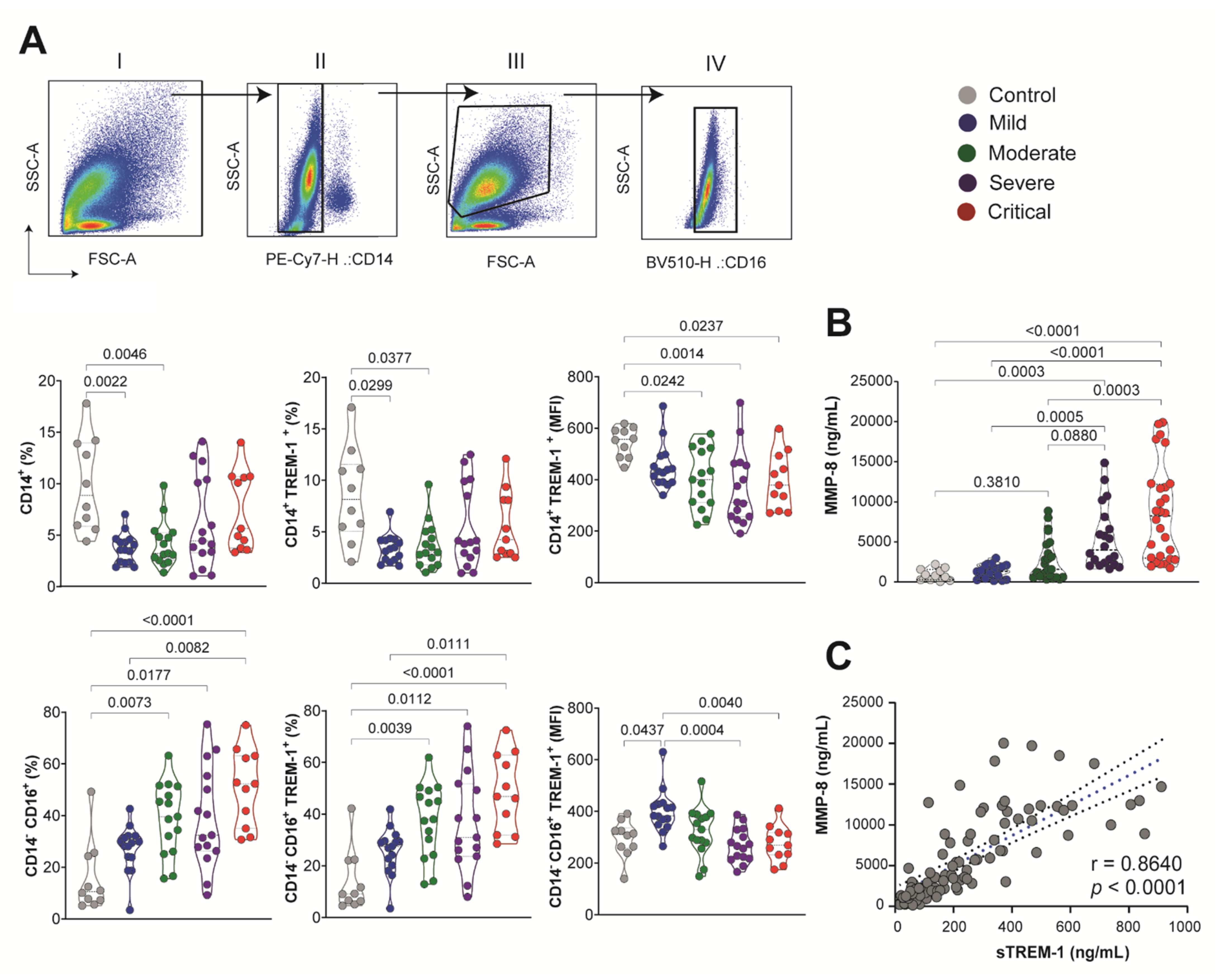
3.5. sTREM-1 Was Released from the Surface of Peripheral Blood Leukocytes and Was Correlated with MMP-8 Expression in the COVID-19 Patient
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. IMUNOCOVID Study Group
References
- Velavan, T.P.; Meyer, C.G. The COVID-19 Epidemic. Trop. Med. Int. Health 2020, 25, 278–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, D.; Zhou, F.; Sun, W.; Chen, L.; Lan, L.; Li, H.; Xiao, F.; Li, Y.; Kolachalama, V.B.; Li, Y.; et al. Relationship Between Serum SARS-CoV-2 Nucleic Acid(RNAemia) and Organ Damage in COVID-19 Patients: A Cohort Study. Clin. Infect. Dis. 2020, 73, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Becker, R.C. COVID-19 Update: Covid-19-Associated Coagulopathy. J. Thromb. Thrombolysis 2020, 50, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Lighter, J.; Phillips, M.; Hochman, S.; Sterling, S.; Johnson, D.; Francois, F.; Stachel, A. Obesity in Patients Younger than 60 Years Is a Risk Factor for Covid-19 Hospital Admission. Clin. Infect. Dis. 2020, 71, 896–897. [Google Scholar] [CrossRef] [Green Version]
- Henry, B.M.; de Oliveira, M.H.S.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, Biochemical and Immune Biomarker Abnormalities Associated with Severe Illness and Mortality in Coronavirus Disease 2019 (COVID-19): A Meta-Analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [Green Version]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Yao, Y.; Cao, J.; Wang, Q.; Shi, Q.; Liu, K.; Luo, Z.; Chen, X.; Chen, S.; Yu, K.; Huang, Z.; et al. D-Dimer as a Biomarker for Disease Severity and Mortality in COVID-19 Patients: A Case Control Study. J. Intensive Care 2020, 8, 1–11. [Google Scholar] [CrossRef]
- Adukpo, S.; Gyan, B.A.; Ofori, M.F.; Dodoo, D.; Velavan, T.P.; Meyer, C.G. Triggering Receptor Expressed on Myeloid Cells 1 (TREM-1) and Cytokine Gene Variants in Complicated and Uncomplicated Malaria. Trop. Med. Int. Health 2016, 21, 1592–1601. [Google Scholar] [CrossRef]
- Hommes, T.J.; Dessing, M.C.; Van’t Veer, C.; Florquin, S.; Colonna, M.; de Vos, A.F.; van der Poll, T. Role of Triggering Receptor Expressed on Myeloid Cells-1/3 in Klebsiella-Derived Pneumosepsis. Am. J. Respir. Cell Mol. Biol. 2015, 53, 647–655. [Google Scholar] [CrossRef]
- De Oliveira Matos, A.; dos Santos Dantas, P.H.; Figueira Marques Silva-Sales, M.; Sales-Campos, H. The Role of the Triggering Receptor Expressed on Myeloid Cells-1 (TREM-1) in Non-Bacterial Infections. Crit. Rev. Microbiol. 2020, 46, 237–252. [Google Scholar] [CrossRef]
- Dos Santos Dantas, P.H.; de Oliveira Matos, A.; da Silva Filho, E.; Silva-Sales, M.; Sales-Campos, H. Triggering Receptor Expressed on Myeloid Cells-1 (TREM-1) as a Therapeutic Target in Infectious and Noninfectious Disease: A Critical Review. Int. Rev. Immunol. 2020, 39, 188–202. [Google Scholar] [CrossRef]
- Weber, B.; Schuster, S.; Zysset, D.; Rihs, S.; Dickgreber, N.; Schürch, C.; Riether, C.; Siegrist, M.; Schneider, C.; Pawelski, H.; et al. TREM-1 Deficiency Can Attenuate Disease Severity without Affecting Pathogen Clearance. PLoS Pathog. 2014, 10, e1003900. [Google Scholar] [CrossRef] [Green Version]
- Yuan, Z.; Fan, X.; Staitieh, B.; Bedi, C.; Spearman, P.; Guidot, D.M.; Sadikot, R.T. HIV-Related Proteins Prolong Macrophage Survival through Induction of Triggering Receptor Expressed on Myeloid Cells-1. Sci. Rep. 2017, 7, 42028. [Google Scholar] [CrossRef] [Green Version]
- Tammaro, A.; Derive, M.; Gibot, S.; Leemans, J.C.; Florquin, S.; Dessing, M.C. TREM-1 and Its Potential Ligands in Non-Infectious Diseases: From Biology to Clinical Perspectives. Pharmacol. Ther. 2017, 177, 81–95. [Google Scholar] [CrossRef]
- Cao, C.; Gu, J.; Zhang, J. Soluble Triggering Receptor Expressed on Myeloid Cell-1 (STREM-1): A Potential Biomarker for the Diagnosis of Infectious Diseases. Front. Med. 2017, 11, 169–177. [Google Scholar] [CrossRef]
- Gómez-Piña, V.; Soares-Schanoski, A.; Rodríguez-Rojas, A.; del Fresno, C.; García, F.; Vallejo-Cremades, M.T.; Fernández-Ruiz, I.; Arnalich, F.; Fuentes-Prior, P.; López-Collazo, E. Metalloproteinases Shed TREM-1 Ectodomain from Lipopolysaccharide-Stimulated Human Monocytes. J. Immunol. 2007, 179, 4065–4073. [Google Scholar] [CrossRef] [Green Version]
- Jedynak, M.; Siemiatkowski, A.; Mroczko, B.; Groblewska, M.; Milewski, R.; Szmitkowski, M. Soluble TREM-1 Serum Level Can Early Predict Mortality of Patients with Sepsis, Severe Sepsis and Septic Shock. Arch. Immunol. Et Ther. Exp. 2018, 66, 299–306. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.T.; Lee, L.N.; Ho, C.C.; Shu, C.C.; Ruan, S.Y.; Tsai, Y.J.; Wang, J.Y.; Yu, C.J. High Serum Levels of Procalcitonin and Soluble TREM-1 Correlated with Poor Prognosis in Pulmonary Tuberculosis. J. Infect. 2014, 68, 440–447. [Google Scholar] [CrossRef] [Green Version]
- Da Silva-Neto, P.V.; de Carvalho, J.C.S.; Pimentel, V.E.; Pérez, M.M.; Carmona-Garcia, I.; Neto, N.T.; Oliveira, C.N.S.; Fraga-Silva, T.F.C.; Milanezi, C.M.; Rodrigues, L.C.; et al. Prognostic Value of STREM-1 in COVID-19 Patients: A Biomarker for Disease Severity and Mortality. medRxiv 2020, 1, 1–28. [Google Scholar] [CrossRef]
- Van-Singer, M.; Brahier, T.; Ngai, M.; Wright, J.; Weckman, A.M.; Erice, C.; Meuwly, J.Y.; Hugli, O.; Kain, K.C.; Boillat-Blanco, N. COVID-19 Risk Stratification Algorithms Based on STREM-1 and IL-6 in Emergency Department. J. Allergy Clin. Immunol. 2021, 147, 99–106.e4. [Google Scholar] [CrossRef]
- Nooijer, A.H.; Grondman, I.; Lambden, S.; Kooistra, E.J.; Janssen, N.A.F.; Kox, M.; Pickkers, P.; Joosten, L.A.B.; van de Veerdonk, F.L.; Derive, M.; et al. Increased STREM-1 Plasma Concentrations Are Associated with Poor Clinical Outcomes in Patients with COVID-19. Biosci. Rep. 2021, 41, 41. [Google Scholar] [CrossRef]
- Wei, P.-F. Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 7). Chin. Med. J. 2020, 133, 1087–1095. [Google Scholar] [CrossRef]
- Wan, S.; Xiang, Y.; Fang, W.; Zheng, Y.; Li, B.; Hu, Y.; Lang, C.; Huang, D.; Sun, Q.; Xiong, Y.; et al. Clinical Features and Treatment of COVID-19 Patients in Northeast Chongqing. J. Med. Virol. 2020, 92, 797–806. [Google Scholar] [CrossRef]
- Epskamp, S.; Cramer, A.O.J.; Waldorp, L.J.; Schmittmann, V.D.; Borsboom, D. Qgraph: Network Visualizations of Relationships in Psychometric Data. J. Stat. Softw. 2012, 48, 1–18. [Google Scholar]
- Blighe, K.; Lun, A. PCAtools: Everything Principal Components Analysis. 2021. Available online: https://bioconductor.org/packages/release/bioc/vignettes/PCAtools/inst/doc/PCAtools.html (accessed on 26 November 2021).
- Yang, P.; Ding, Y.; Xu, Z.; Pu, R.; Li, P.; Yan, J.; Liu, J.; Meng, F.; Huang, L.; Shi, L.; et al. Epidemiological and Clinical Features of COVID-19 Patients with and without Pneumonia in Beijing, China. medRxiv 2020, 1, 1–31. [Google Scholar] [CrossRef] [Green Version]
- Zumla, A.; Hui, D.S.; Azhar, E.I.; Memish, Z.A.; Maeurer, M. Reducing Mortality from 2019-NCoV: Host-Directed Therapies Should Be an Option. Lancet 2020, 395, e35–e36. [Google Scholar] [CrossRef] [Green Version]
- Zheng, H.; Heiderscheidt, C.A.; Joo, M.; Gao, X.; Knezevic, N.; Mehta, D.; Sadikot, R.T. MYD88-Dependent and -Independent Activation of TREM-1 via Specific TLR Ligands. Eur. J. Immunol. 2010, 40, 162–171. [Google Scholar] [CrossRef]
- Chen, L.C.; Laskin, J.D.; Gordon, M.K.; Laskin, D.L. Regulation of TREM Expression in Hepatic Macrophages and Endothelial Cells during Acute Endotoxemia. Exp. Mol. Pathol. 2008, 84, 145–155. [Google Scholar] [CrossRef] [Green Version]
- Dimopoulou, I.; Pelekanou, A.; Mavrou, I.; Savva, A.; Tzanela, M.; Kotsaki, A.; Kardara, M.; Orfanos, S.E.; Kotanidou, A.; Giamarellos-Bourboulis, E.J. Early Serum Levels of Soluble Triggering Receptor Expressed on Myeloid Cells-1 in Septic Patients: Correlation with Monocyte Gene Expression. J. Crit. Care 2012, 27, 294–300. [Google Scholar] [CrossRef]
- Gibot, S.; Levy, B.; Bene, M.-C.; Faure, G.; Bollaert, P.-E. Soluble Triggering Receptor Expressed on Myeloid Cells and the Diagnosis of Pneumonia. N. Engl. J. Med. 2004, 350, 451–458. [Google Scholar] [CrossRef]
- Yuan, Z.; Syed, M.; Panchal, D.; Joo, M.; Bedi, C.; Lim, S.; Onyuksel, H.; Rubinstein, I.; Colonna, M.; Sadikot, R.T. TREM-1-Accentuated Lung Injury via MiR-155 Is Inhibited by LP17 Nanomedicine. Am. J. Physiol. Lung Cell Mol. Physiol. 2016, 310, 426–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotchkiss, R.S.; Monneret, G.; Payen, D. Immunosuppression in Sepsis: A Novel Understanding of the Disorder and a New Therapeutic Approach. Lancet Infect. Dis. 2013, 13, 260–268. [Google Scholar] [CrossRef] [Green Version]
- Richard-Greenblatt, M.; Boillat-Blanco, N.; Zhong, K.; Mbarack, Z.; Samaka, J.; Mlaganile, T.; Kazimoto, T.; D’Acremont, V.; Kain, K.C. Prognostic Accuracy of Soluble Triggering Receptor Expressed on Myeloid Cells (STREM-1)-Based Algorithms in Febrile Adults Presenting to Tanzanian Outpatient Clinics. Clin. Infect. Dis. 2020, 70, 1304–1312. [Google Scholar] [CrossRef] [PubMed]
- Amrun, S.N.; Tan, J.J.L.; Rickett, N.Y.; Cox, J.A.; Lee, B.; Griffiths, M.J.; Solomon, T.; Perera, D.; Ooi, M.H.; Hiscox, J.A.; et al. TREM-1 Activation Is a Potential Key Regulator in Driving Severe Pathogenesis of Enterovirus A71 Infection. Sci. Rep. 2020, 10, 3810–3813. [Google Scholar] [CrossRef]
- Aldasoro Arguinano, A.A.; Dadé, S.; Stathopoulou, M.; Derive, M.; Coumba Ndiaye, N.; Xie, T.; Masson, C.; Gibot, S.; Visvikis-Siest, S. TREM-1 SNP Rs2234246 Regulates TREM-1 Protein and MRNA Levels and Is Associated with Plasma Levels of L-Selectin. PLoS ONE 2017, 12, e0182226. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.; Li, L.; Xu, M.; Wu, J.; Luo, D.; Zhu, Y.S.; Li, B.X.; Song, X.Y.; Zhou, X. Prognostic Value of Interleukin-6, C-Reactive Protein, and Procalcitonin in Patients with COVID-19. J. Clin. Virol. 2020, 127, 104370. [Google Scholar] [CrossRef]
- Taniguchi, K.; Karin, M. IL-6 and Related Cytokines as the Critical Lynchpins between Inflammation and Cancer. Semin. Immunol. 2014, 26, 54–74. [Google Scholar] [CrossRef]
- Han, H.; Ma, Q.; Li, C.; Liu, R.; Zhao, L.; Wang, W.; Zhang, P.; Liu, X.; Gao, G.; Liu, F.; et al. Profiling Serum Cytokines in COVID-19 Patients Reveals IL-6 and IL-10 Are Disease Severity Predictors. Emerg. Microbes Infect. 2020, 9, 1123–1130. [Google Scholar] [CrossRef]
- McKinstry, K.K.; Strutt, T.M.; Buck, A.; Curtis, J.D.; Dibble, J.P.; Huston, G.; Tighe, M.; Hamada, H.; Sell, S.; Dutton, R.W.; et al. IL-10 Deficiency Unleashes an Influenza-Specific Th17 Response and Enhances Survival against High-Dose Challenge. J. Immunol. 2009, 182, 7353–7363. [Google Scholar] [CrossRef] [Green Version]
- Kang, Z.; Luo, S.; Gui, Y.; Zhou, H.; Zhang, Z.; Tian, C.; Zhou, Q.; Wang, Q.; Hu, Y.; Fan, H.; et al. Obesity Is a Potential Risk Factor Contributing to Clinical Manifestations of COVID-19. Int. J. Obes. 2020, 44, 2479–2485. [Google Scholar] [CrossRef]
- Vardhana, S.A.; Wolchok, J.D. The Many Faces of the Anti-COVID Immune Response. J. Exp. Med. 2020, 217, e20200678. [Google Scholar] [CrossRef]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Sta-plin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Weiss, G.; Lai, C.; Fife, M.E.; Grabiec, A.M.; Tildy, B.; Snelgrove, R.J.; Xin, G.; Lloyd, C.M.; Hussell, T. Reversal of TREM-1 Ectodomain Shedding and Improved Bacterial Clearance by Intranasal Metalloproteinase Inhibitors. Mucosal. Immunol. 2017, 10, 1021–1030. [Google Scholar] [CrossRef]
- Heinzelmann, M.; Mercer-Jones, M.; Cheadle, W.G.; Polk, H.C. CD14 Expression in Injured Patients Correlates with Outcome. Ann. Surg. 1996, 224, 91–96. [Google Scholar] [CrossRef]
- Klesney-Tait, J.; Turnbull, I.R.; Colonna, M. The TREM Receptor Family and Signal Integration. Nat. Immunol. 2006, 7, 1266–1273. [Google Scholar] [CrossRef]
- Shimizu, T.; Kanai, K.-I.; Kyo, Y.; Suzaki, H.; Asano, K.; Hisamitsu, T. Effect of Tranilast on Matrix Metalloproteinase Production from Neutrophils In-Vitro. J. Pharm. Pharmacol. 2010, 58, 91–99. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Variable | Healthy Controls N = 50 | All Patients N = 237 | COVID-19 Care | p-Value | |
|---|---|---|---|---|---|
| Residential N = 60 | Hospitalized N = 177 | ||||
| Demographic characteristics | |||||
| Age mean ± SD, (IQR) | 35 ± 14.7 (19–80) | 57 ± 19 (16–96) | 37 ± 12 (16–71) | 63 ± 16.4 (20–96) | a <0.0001 c,d <0.0001 |
| Sex, No. (%) | |||||
| Male | 22 (44) | 84 (35.4) | 21 (35) | 63 (36) | d 0.006 |
| Female | 28 (56) | 153 (64.6) | 39 (65) | 114 (64) | |
| Comorbidities or coexisting disorders, No. (%) | |||||
| Hypertension | 7 (14) | 116 (48.9) | 4 (3.4) | 112 (96.6) | a,c,d <0.0001 |
| Cardiovascular diseases | 5 (18.5) | 22 (81.5) | 8 (36.4) | 14 (63.6) | a 0.7947 b 0.7685 c 0.5760 d 0.2084 |
| Diabetes mellitus | 4 (5.8) | 65 (94.2) | 5 (7.7) | 60 (92.3) | a 0.0031 c 0.0002 d <0.0001 |
| History of smoking | 3 (10) | 27 (90) | 6 (22.2) | 21 (77.8) | a 0.2189 b >0.1 c 0.1227 d 0.0692 |
| History of stroke | - | 10 (4.2) | - | 10 (5.6) | - |
| Neurological diseases | - | 12 (5.0) | 2 (16.7) | 10 (83.3) | d 0.7353 |
| Cancer | - | 7 (2.9) | - | 7 (3.9) | - |
| BMI (kg/m2) | 26.5 ± 5.2 (15.4–43.2) | 28.4 ± 7.0 (15.7–65.7) | 27.2 ± 5.6 (17.7–43.8) | 29.4 ± 7.3 (18.4–65.7) | a 0.0053 c 0.0008 d 0.0480 |
| Presenting symptoms, No. (%) | |||||
| Dyspnea | - | 137 (57.8) | 19 (31.6) | 118 (66.6) | a,b,c,d <0.0001 |
| Fever | - | 78 (32.9) | 1 (1.7) | 77 (43.5) | a,c,d <0.0001 |
| Myalgia | - | 52 (21.9) | - | 52 (29.4) | - |
| Diarrhea | - | 56 (23.6) | 22 (36.7) | 34 (19.21) | d 0.0082 |
| Cough | - | 161 (67.9) | 43 (71.7) | 118 (66.7) | d <0.0001 |
| Hyperactive delirium | - | 15 (6.3) | - | 15 (8.5) | - |
| Dysgeusia | - | 60 (25.3) | 40 (66.7) | 20 (11.3) | d <0.0001 |
| Anosmia | - | 67 (28.3) | 41 (68.3) | 26 (14.7) | d <0.0001 |
| Laboratory findings, mean ± SD, (IQR) | |||||
| Erythrocytes × 109/L | 4.6 ± 0.6 (3.6–5.8) | 4.4 ± 0.8 (2.0–5.9) | 4.8 ± 0.4 (3.7–5.8) | 4.2 ± 0.8 (2.0–5.9) | a 0.0078 c,d <0.0001 |
| Hemoglobin (g/dL) | 14.5 ± 1.6 (10.5–17.5) | 13.1 ± 2.6 (6.6–18.2) | 14.5 ± 1.3 (12.0–17.7) | 12.4 ± 2.6 (6.6–18.2) | a,c,d <0.0001 |
| Leukocytes × 109/L | 7.5 ± 1.8 (4.1–13.2) | 9.0 ± 5.6 (1.6–33) | 7.3 ± 2.1 (3.2–13.5) | 10.2 ± 6.0 (1.6–33) | c,d <0.0001 a 0.0088 |
| Neutrophils × 109/L | 4.2 ± 1.4 (2.4–9.8) | 7.0 ± 5.0 (1.4–26.1) | 4.1 ± 1.9 (1.6–11.0) | 8.3 ± 5.0 (1.4–26.1) | a,c,d <0.0001 |
| Lymphocytes × 109/L | 1.2 ± 0.7 (1.2–5.0) | 1.3 ± 0.9 (0.1–4.2) | 2.3 ± 0.6 (1.1–4.3) | 1.0 ± 0.7 (0.1–4.1) | a,c,d <0.0001 |
| RNL | 1.8 ± 1.0 (0.9–6.3) | 5.6 ± 6.4 (0.1–30.7) | 1.7 ± 1.0 (0.5–7.9) | 7.3 ± 6.4 (0.2–30.7) | a,c,d <0.0001 |
| Monocytes × 109/L | 0.5 ± 0.2 (0.1–1.4) | 0.5 ± 0.3 (0.1–1.9) | 0.5 ± 0.1 (0.2–0.9) | 0.5 ± 0.4 (0.1–1.9) | a,b,c,d >0.1 |
| Platelets × 109/L | 214 ± 51.8 (129–370) | 244 ± 98.1 (50–635) | 227 ±66.3 (119–474) | 245 ± 105.8 (50–635) | a,b,d >0.1 c 0.0775 |
| Hospital support, No. (%) | |||||
| Infirmary | - | 95 (40) | - | 95 (53.7) | - |
| Intensive care unit (ICU) | - | 82 (34.6) | - | 82 (46.3) | - |
| Hospitalization data, No. | |||||
| Hospitalization days, mean (IQR) | - | 9 (1–30) | - | 9 (1–30) | - |
| Respiratory support upon assessment (%) | |||||
| Nasal-cannula oxygen | - | 65 (27.4) | - | 65 (36.7) | - |
| Oxygen masks/noninvasive | - | 30 (12.6) | - | 30 (16.9) | - |
| Invasive mechanical ventilation | - | 70 (29.5) | - | 70 (39.5) | - |
| Oxygen saturation mean ± SD (IQR) | 99 ± 2.4 (89–99) | 93 ± 8.7 (54–99) | 98 ± 1.8 (92–99) | 91 ± 8.9 (54–99) | a,c,d <0.0001 |
| Medications No. (%) | |||||
| Glucocorticoid | - | 156 (61.6) | 10 (16.7) | 146 (82.5) | d <0.0001 |
| Azithromycin | - | 149 (68.6) | 18 (30.0) | 127 (71.7) | d <0.0001 |
| Ceftriaxone | - | 84 (33.7) | 0.4 (6.7) | 80 (45.2) | d <0.0001 |
| Oseltamivir | - | 80 (30.4) | 0.8 (13.3) | 72 (40.7) | d <0.0001 |
| Colchicine | - | 0.5 (2.1) | - | 0.5 (2.8) | - |
| Chloroquine/hydroxychloroquine | - | 18 (7.6) | - | 26 (14.7) | - |
| Anticoagulant | - | 34 (14.3) | - | 34 (19.2) | - |
| Ivermectin | - | 11 (4.6) | 11 (18.3) | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Silva-Neto, P.V.; de Carvalho, J.C.S.; Pimentel, V.E.; Pérez, M.M.; Toro, D.M.; Fraga-Silva, T.F.C.; Fuzo, C.A.; Oliveira, C.N.S.; Rodrigues, L.C.; Argolo, J.G.M.; et al. sTREM-1 Predicts Disease Severity and Mortality in COVID-19 Patients: Involvement of Peripheral Blood Leukocytes and MMP-8 Activity. Viruses 2021, 13, 2521. https://doi.org/10.3390/v13122521
da Silva-Neto PV, de Carvalho JCS, Pimentel VE, Pérez MM, Toro DM, Fraga-Silva TFC, Fuzo CA, Oliveira CNS, Rodrigues LC, Argolo JGM, et al. sTREM-1 Predicts Disease Severity and Mortality in COVID-19 Patients: Involvement of Peripheral Blood Leukocytes and MMP-8 Activity. Viruses. 2021; 13(12):2521. https://doi.org/10.3390/v13122521
Chicago/Turabian Styleda Silva-Neto, Pedro V., Jonatan C. S. de Carvalho, Vinícius E. Pimentel, Malena M. Pérez, Diana M. Toro, Thais F. C. Fraga-Silva, Carlos A. Fuzo, Camilla N. S. Oliveira, Lilian C. Rodrigues, Jamille G. M. Argolo, and et al. 2021. "sTREM-1 Predicts Disease Severity and Mortality in COVID-19 Patients: Involvement of Peripheral Blood Leukocytes and MMP-8 Activity" Viruses 13, no. 12: 2521. https://doi.org/10.3390/v13122521