
Pregnancy Outcomes in SARS-CoV-2-Positive Patients: A 20-Month Retrospective Analysis of Delivery Cases
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
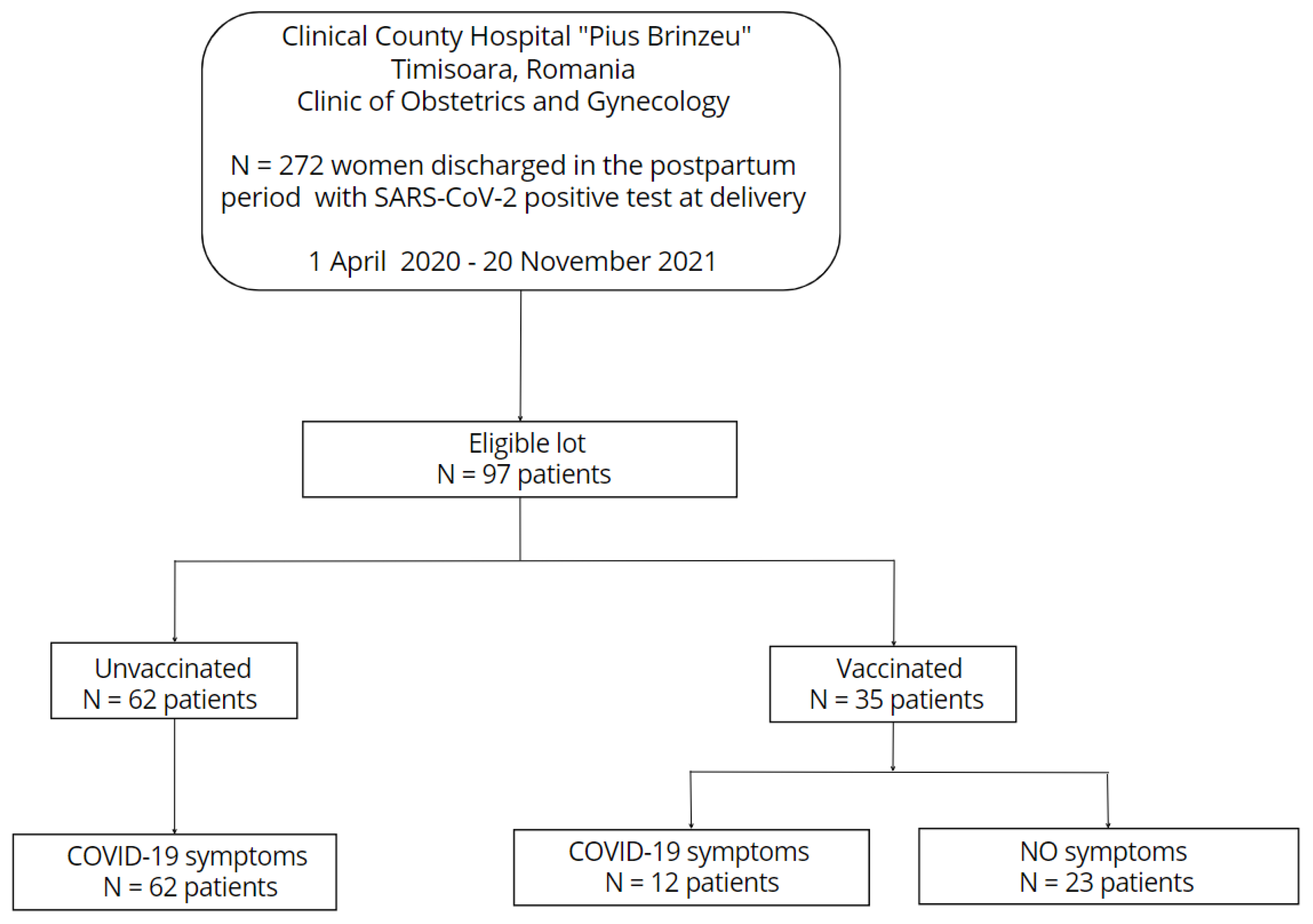
2.1. Study Design and Population
2.2. Outcome Measures
2.3. Data Analysis
3. Results
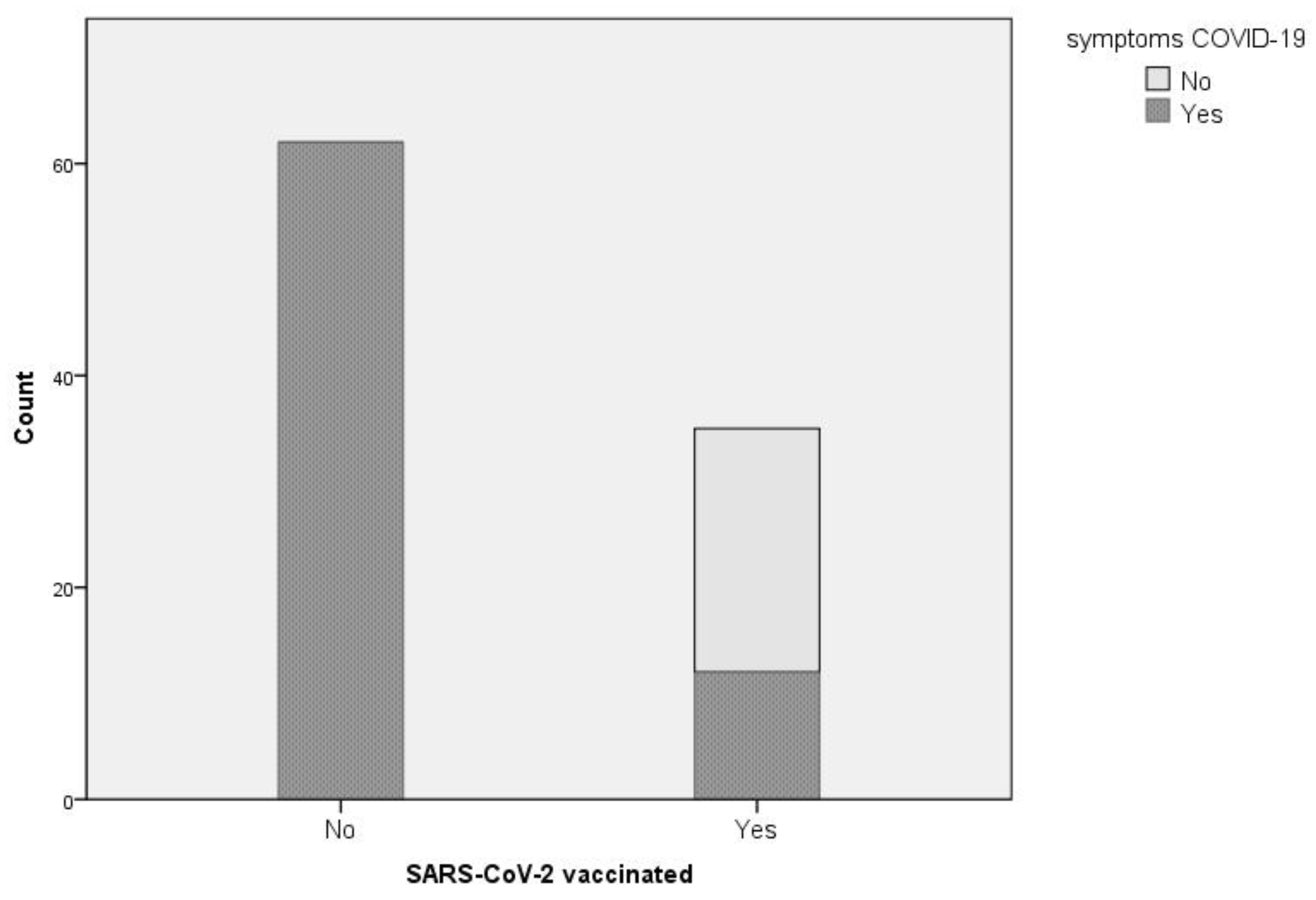
3.1. COVID-19 Symptoms in SARS-CoV-2-positive Women
3.2. Maternal Characteristics
3.3. Laboratory Findings in SARS-CoV-2-Infected Patients
3.4. Management of COVID-19 Disease
3.5. Pregnancy Outcomes
4. Discussions
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- La Verde, M.; Riemma, G.; Torella, M.; Cianci, S.; Savoia, F.; Licciardi, F.; Scida, S.; Morlando, M.; Colacurci, N.; De Franciscis, P. Maternal death related to COVID-19: A systematic review and meta-analysis focused on maternal co-morbidities and clinical characteristics. Int. J. Gynaecol. Obstet. 2021, 154, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Della Gatta, A.N.; Rizzo, R.; Pilu, G.; Simonazzi, G. Coronavirus disease 2019 during pregnancy: A systematic review of reported cases. Am. J. Obstet. Gynecol. 2020, 223, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Carp-Veliscu, A.; Mehedintu, C.; Frincu, F.; Bratila, E.; Rasu, S.; Iordache, I.; Bordea, A.; Braga, M. The Effects of SARS-CoV-2 Infection on Female Fertility: A Review of the Literature. Int. J. Environ. Res. Public Health 2022, 16, 984. [Google Scholar] [CrossRef] [PubMed]
- Blavatnik School of Government, University of Oxford. Coronavirus Government Response Tracker. Available online: https://www.bsg.ox.ac.uk/research/covid-19-government-response-tracker (accessed on 7 November 2022).
- Evans, D.B.; Tandon, A.; Murray, C.J.L.; Lauer, J.A. Comparative Efficiency of National Health Systems: Cross National Econometric Analysis. BMJ 2001, 323, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Allotey, J.; Fernandez, S.; Bonet, M.; Stallings, E.; Yap, M.; Kew, T.; Zhou, D.; Coomar, D.; Sheikh, J.; Lawson, H.; et al. Clinical Manifestations, Risk Factors, and Maternal and Perinatal Outcomes of Coronavirus Disease 2019 in Pregnancy: Living Systematic Review and Meta-Analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.Y.; DeSisto, C.L.; Simeone, R.M.; Ellington, S.; Galang, R.R.; Oduyebo, T.; Gilboa, S.M.; Lavery, A.M.; Gundlapalli, A.v.; Shapiro-Mendoza, C.K. Adverse Pregnancy Outcomes, Maternal Complications, and Severe Illness Among US Delivery Hospitalizations With and Without a Coronavirus Disease 2019 (COVID-19) Diagnosis. Clin. Infect. Dis. 2021, 73, S24–S31. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, D.J.; Rasmussen, S.A. An Update on COVID-19 and Pregnancy. Am. J. ObstetGynecol. 2022, 226, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Hantoushzadeh, S.; Shamshirsaz, A.A.; Aleyasin, A.; Seferovic, M.D.; Aski, S.K.; Arian, S.E.; Pooransari, P.; Ghot-bizadeh, F.; Aalipour, S.; Soleimani, Z.; et al. Maternal Death Due to COVID-19. Am. J. ObstetGynecol. 2020, 223, 109.e1–109.e6. [Google Scholar] [CrossRef]
- Pashaei, Z.; SeyedAlinaghi, S.; Qaderi, K.; Barzegary, A.; Karimi, A.; Mirghaderi, S.P.; Mirzapour, P.; Tantuoyir, M.M.; Dadras, O.; Ali, Z.; et al. Prenatal and neonatal complications of COVID-19: A system-atic review. Health Sci. Rep. 2022, 15, e510. [Google Scholar] [CrossRef]
- Kumar, P.; Fadila; Prasad, A.; Akhtar, A.; Chaudhary, B.K.; Tiwari, L.K.; Chaudhry, N. Vertical Transmission and Clinical Outcome of the Neonates Born to SARS-CoV-2-Positive Mothers: A Tertiary Care Hospital-Based Ob-servational Study. BMJ Paediatr. Open 2021, 5, e001193. [Google Scholar] [CrossRef]
- Farmer, M.L. A Neonate With Vertical Transmission of COVID-19 and Acute Respiratory Failure. Adv. Neonatal Care 2021, 21, 482–492. [Google Scholar] [CrossRef]
- Bakhle, A.; Sreekumar, K.; Baracho, B.; Sardessai, S.; Silveira, M.P. Cavitary Lung Lesions in a Neonate: Potential Manifestation of COVID-19 Related Multisystem Inflammatory Syndrome. Pediatr. Pulmonol. 2022, 57, 311–314. [Google Scholar] [CrossRef]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; do Cao, J.; Benachi, A.; de Luca, D. Transplacental Transmission of SARS-CoV-2 Infection. Nat. Commun. 2020, 11, 3572. [Google Scholar] [CrossRef]
- Kappanayil, M.; Balan, S.; Alawani, S.; Mohanty, S.; Leeladharan, S.P.; Gangadharan, S.; Jayashankar, J.P.; Jagadeesan, S.; Kumar, A.; Gupta, A.; et al. Multisystem Inflammatory Syndrome in a Neonate, Temporally Associated with Prenatal Exposure to SARS-CoV-2: A Case Report. Lancet Child Adolesc. Health 2021, 5, 304–308. [Google Scholar] [CrossRef]
- Resta, L.; Vimercati, A.; Cazzato, G.; Fanelli, M.; Scarcella, S.V.; Ingravallo, G.; Colagrande, A.; Sablone, S.; Stolfa, M.; Arezzo, F.; et al. SARS-CoV-2, Placental Histopathology, Gravity of Infection and Immunopathology: Is There an Association? Viruses 2022, 18, 1330. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention COVID-19 Vaccines While Pregnant or Breastfeeding. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/pregnancy.html (accessed on 9 November 2022).
- Australian Government; Department of Health and Aged Care Pregnancy. Breastfeeding and COVID-19 Vaccines. Available online: https://www.health.gov.au/initiatives-and-programs/covid-19-vaccines/who-can-get-vaccinated/pregnant-women (accessed on 9 November 2022).
- ANSM Covid-19 Vaccines and Pregnant Women. Available online: https://ansm.sante.fr/dossiers-thematiques/covid-19-vaccins-et-femmes-enceintes (accessed on 9 November 2022).
- Romanian Government Vaccination against COVID-19, Fertility, Pregnancy and Breastfeeding. Available online: https://vaccinare-covid.gov.ro/vaccinarea-impotriva-covid-19-fertilitatea-sarcina-si-alaptarea/ (accessed on 9 November 2022).
- Kadali, R.A.K.; Janagama, R.; Peruru, S.R.; Racherla, S.; Tirumala, R.; Madathala, R.R.; Gajula, V. Adverse Effects of COVID-19 Messenger RNA Vaccines among Pregnant Women: A Cross-Sectional Study on Healthcare Workers with Detailed Self-Reported Symptoms. Am. J. Obs. 2021, 225, 458–460. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 MRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Huang, W.Y.; Sheridan, S.; Sit, C.H.; Chen, X.K.; Wong, S.H. COVID-19 Pandemic Brings a Sedentary Lifestyle in Young Adults: A Cross-Sectional and Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 6035. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Biron-Shental, T.; Makov-Assif, M.; Key, C.; Kohane, I.S.; Hernán, M.A.; Lipsitch, M.; Her-nandez-Diaz, S.; Reis, B.Y.; et al. Effectiveness of the BNT162b2 MRNA COVID-19 Vaccine in Pregnancy. Nat. Med. 2021, 27, 1693–1695. [Google Scholar] [CrossRef]
- Bookstein Peretz, S.; Regev, N.; Novick, L.; Nachshol, M.; Goffer, E.; Ben-David, A.; Asraf, K.; Doolman, R.; Levin, E.G.; Regev Yochay, G.; et al. Short-term Outcome of Pregnant Women Vaccinated with BNT162b2 MRNA COVID-19 Vaccine. Ultrasound Obstet. Gynecol. 2021, 58, 450–456. [Google Scholar] [CrossRef]
- Goldshtein, I.; Nevo, D.; Steinberg, D.M.; Rotem, R.S.; Gorfine, M.; Chodick, G.; Segal, Y. Association Between BNT162b2 Vaccination and Incidence of SARS-CoV-2 Infection in Pregnant Women. JAMA 2021, 326, 728. [Google Scholar] [CrossRef] [PubMed]
- Piekos, S.N.; Price, N.D.; Hood, L.; Hadlock, J.J. The Impact of Maternal SARS-CoV-2 Infection and COVID-19 Vaccination on Maternal-Fetal Outcomes. Reprod. Toxicol. 2022, 114, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Fell, D.B.; Dimanlig-Cruz, S.; Regan, A.K.; Håberg, S.E.; Gravel, C.A.; Oakley, L.; Alton, G.D.; Török, E.; Dhinsa, T.; Shah, P.S.; et al. Risk of Preterm Birth, Small for Gestational Age at Birth, and Stillbirth after Covid-19 Vac-cination during Pregnancy: Population Based Retrospective Cohort Study. BMJ 2022, 378, e071416. [Google Scholar] [CrossRef] [PubMed]
- Berman Institute of Bioethics & Center for Immunization Research, Johns Hopkins University. COVID-19 Maternal Immunization Tracker (COMIT): COVID-19 Vaccine Policies for Pregnant and Lactating People Worldwide. Available online: https://www.comitglobal.org/ (accessed on 7 November 2022).
- Romanian Government Ministry of Health Order, No. 555/2020 on the Approval of the Plan of Measures for the Preparation of Hospitals in the Context of the COVID19 Coronavirus Epidemic, of the List of Hospitals That Provide Medical Assistance to Patients Test Positive for the SARS-CoV-2 Virus in Phase I and Phase II and The List of Support Hospitals for Patients Tested Positive or Suspected with the SARS-CoV-2 Virus. The Official Moni-tor of Romania 2020. Available online: https://legislatie.just.ro/Public/DetaliiDocument/224705 (accessed on 15 August 2022).
- de Oliveira, K.B.; de Oliveira, O.J. Making Hospitals Sustainable: Towards Greener, Fairer and More Prosperous Services. Sustainability 2022, 14, 9730. [Google Scholar] [CrossRef]
- Bogaert, K.C.; Lieb, W.E.; Glazer, K.B.; Wang, E.; Stone, J.L.; Howell, E.A. Stress and the Psychological Impact of the COVID-19 Pandemic on Frontline Obstetrics and Gynecology Providers. Am. J. Perinatol. 2022, 29, 1596–1604. [Google Scholar] [CrossRef]
- Bredicean, C.; Tamasan, S.C.; Lungeanu, D.; Giurgi-Oncu, C.; Stoica, I.-P.; Panfil, A.-L.; Vasilian, C.; Secosan, I.; Ursoniu, S.; Patrascu, R. Burnout Toll on Empathy Would Mediate the Missing Professional Support in the COVID-19 Outbreak. Risk Manag. Policy 2021, 14, 2231–2244. [Google Scholar] [CrossRef]
- La Verde, M.; Torella, M.; Riemma, G.; Narciso, G.; Iavarone, I.; Gliubizzi, L.; Palma, M.; Morlando, M.; Colacurci, N.; De Franciscis, P. Incidence of gestational diabetes mellitus before and after the Covid-19 lockdown: A retrospective cohort study. J. Obstet. Gynaecol. Res. 2022, 48, 1126–1131. [Google Scholar] [CrossRef]
- Khalil, A.; von Dadelszen, P.; Ugwumadu, A.; Draycott, T.; Magee, L.A. Effect of COVID-19 on maternal and neonatal services. Lancet Glob. Health 2021, 9, e112. [Google Scholar] [CrossRef]
- Prabhu, M.; Cagino, K.; Matthews, K.; Friedlander, R.; Glynn, S.; Kubiak, J.; Yang, Y.; Zhao, Z.; Baergen, R.; DiPace, J.; et al. Pregnancy and Postpartum Outcomes in a Universally Tested Population for SARS-CoV-2 in New York City: A Prospective Cohort Study. BJOG 2020, 127, 1548–1556. [Google Scholar] [CrossRef]
- Ishqeir, A.; Nir, A.; Aptowitzer, I.; Godfrey, M. Increased Incidence of Persistent Pulmonary Hypertension of the Newborn Following Third Trimester Maternal COVID-19 Infection. Eur. Heart J. 2021, 42, 1843. [Google Scholar] [CrossRef]
- Vousden, N.; Bunch, K.; Morris, E.; Simpson, N.; Gale, C.; O’Brien, P.; Quigley, M.; Brocklehurst, P.; Kurinczuk, J.J.; Knight, M. The Incidence, Characteristics and Outcomes of Pregnant Women Hospitalized with Symptomat-ic and Asymptomatic SARS-CoV-2 Infection in the UK from March to September 2020: A National Cohort Study Using the UK Obstetric Surveillance System (UKOSS). PLoS ONE 2021, 16, e0251123. [Google Scholar] [CrossRef]
- Chi, H.; Chiu, N.-C.; Tai, Y.-L.; Chang, H.-Y.; Lin, C.-H.; Sung, Y.-H.; Tseng, C.-Y.; Liu, L.Y.-M.; Lin, C.-Y. Clinical Features of Neonates Born to Mothers with Coronavirus Disease-2019: A Systematic Review of 105 Neonates. J. Microbiol. Immunol. Infect. 2021, 54, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Collier, A.Y.; McMahan, K.; Yu, J.; Tostanoski, L.H.; Aguayo, R.; Ansel, J.; Chandrashekar, A.; Patel, S.; Apraku-Bondzie, E.; Sellers, D.; et al. Immunogenicity of COVID-19 MRNA Vaccines in Pregnant and Lactating Women. JAMA 2021, 325, 2370. [Google Scholar] [CrossRef] [PubMed]
- Engjom, H.; van den Akker, T.; Aabakke, A.; Ayras, O.; Bloemenkamp, K.; Donati, S.; Cereda, D.; Overtoom, E.; Knight, M. Severe COVID-19 in Pregnancy Is Almost Exclusively Limited to Unvaccinated Women—Time for Policies to Change. Lancet Reg. Health Eur. 2022, 13, 100313. [Google Scholar] [CrossRef]
- Dragomir, C.; Popescu, R.; Bernad, E.S.; Boia, M.; Iacob, D.; Dima, M.A.; Laza, R.; Soldan, N.; Bernad, B.-C.; Se-menescu, A.E.; et al. The Influence of Maternal Psychological Manifestations on the Mother–Child Couple dur-ing the Early COVID-19 Pandemic in Two Hospitals in Timisoara, Romania. Medicina 2022, 58, 1540. [Google Scholar] [CrossRef] [PubMed]
- Goldshtein, I.; Steinberg, D.M.; Kuint, J.; Chodick, G.; Segal, Y.; Shapiro Ben David, S.; Ben-Tov, A. Association of BNT162b2 COVID-19 Vaccination During Pregnancy With Neonatal and Early Infant Outcomes. JAMA Pediatr. 2022, 176, 470. [Google Scholar] [CrossRef]
- Prabhu, M.; Murphy, E.A.; Sukhu, A.C.; Yee, J.; Singh, S.; Eng, D.; Zhao, Z.; Riley, L.E.; Yang, Y.J. Antibody Re-sponse to SARS-CoV-2 MRNA Vaccines in Pregnant Women and Their Neonates. Available online: https://www.biorxiv.org/content/10.1101/2021.04.05.438524v1 (accessed on 9 November 2022).
- Kayem, G.; Lecarpentier, E.; Deruelle, P.; Bretelle, F.; Azria, E.; Blanc, J.; Bohec, C.; Bornes, M.; Ceccaldi, P.-F.; Chalet, Y.; et al. A Snapshot of the Covid-19 Pandemic among Pregnant Women in France. J. GynecolObstet Hum. Reprod. 2020, 49, 101826. [Google Scholar] [CrossRef]
- Siqueira, T.S.; de Souza, E.K.G.; Martins-Filho, P.R.; Silva, J.R.S.; Gurgel, R.Q.; Cuevas, L.E.; Santos, V.S. Clinical Characteristics and Risk Factors for Maternal Deaths Due to COVID-19 in Brazil: A Nationwide Population-Based Cohort Study. J. Travel Med. 2022, 29, taab199. [Google Scholar] [CrossRef]
- Levitan, D.; London, V.; McLaren, R.A.; Mann, J.D.; Cheng, K.; Silver, M.; Balhotra, K.S.; McCalla, S.; Loukeris, K. Histologic and Immunohistochemical Evaluation of 65 Placentas From Women With Polymerase Chain Reac-tion–Proven Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection. Arch. Pathol. Lab. Med. 2021, 145, 648–656. [Google Scholar] [CrossRef]
- Ramírez-Rosas, A.; Benitez-Guerrero, T.; Corona-Cervantes, K.; Vélez-Ixta, J.M.; Zavala-Torres, N.G.; Cuenca-Leija, J.; Martínez-Pichardo, S.; Landero-Montes-de-Oca, M.E.; Bastida-González, F.G.; Zárate-Segura, P.B.; et al. Study of Perinatal Transmission of SARS-CoV-2 in a Mexican Public Hospital. Int. J. Infect. Dis. 2021, 113, 225–232. [Google Scholar] [CrossRef]
- Craina, M.; Iacob, D.; Dima, M.; Bernad, S.; Silaghi, C.; Moza, A.; Pantea, M.; Gluhovschi, A.; Bernad, E. Clinical, Laboratory, and Imaging Findings of Pregnant Women with Possible Vertical Transmission of SARS-CoV-2—Case Series. Int. J. Env. Res. Public Health 2022, 19, 10916. [Google Scholar] [CrossRef] [PubMed]
- Shams, T.; Alhashemi, H.; Madkhali, A.; Noorelahi, A.; Allarakia, S.; Faden, Y.; Alhasani, A.; Alzahrani, K.; Alrefai, A.; Ghilan, N.; et al. Comparing Pregnancy Outcomes between Symptomatic and Asymptomatic COVID-19 Positive Unvaccinated Women: Multicenter Study in Saudi Arabia. J. Infect. Public Health 2022, 15, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Richtmann, R.; Torloni, M.R.; Oyamada Otani, A.R.; Levi, J.E.; Crema Tobara, M.; de Almeida Silva, C.; Dias, L.; Miglioli-Galvão, L.; Martins Silva, P.; Macoto Kondo, M. Fetal deaths in pregnancies with SARS-CoV-2 infection in Brazil: A case series. Case Rep. Womens Health 2020 12, e00243. [CrossRef]
- Favre, G.; Mazzetti, S.; Gengler, C.; Bertelli, C.; Schneider, J.; Laubscher, B.; Capoccia, R.; Pakniyat, F.; Ben Jazia, I.; Eggel-Hort, B.; et al. Decreased Fetal Movements: A Sign of Placental SARS-CoV-2 Infection with Perinatal Brain Injury. Viruses 2021, 15, 2517. [Google Scholar] [CrossRef] [PubMed]
- Farhan, F.S.; Nori, W.; Al Kadir, I.T.A.; Hameed, B.H. Can Fetal Heart Lie? Intrapartum CTG Changes in COVID-19 Mothers. J. Obstet. Gynaecol. India 2022, 72, 479–484. [Google Scholar] [CrossRef]
- Jaiswal, N.; Puri, M.; Agarwal, K.; Singh, S.; Yadav, R.; Tiwary, N.; Tayal, P.; Vats, B. COVID-19 as an independent risk factor for subclinical placental dysfunction. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 259, 7–11. [Google Scholar] [CrossRef] [PubMed]
- AbdelMassih, A.; Fouda, R.; Essam, R.; Negm, A.; Khalil, D.; Habib, D.; Tadros, M.A. COVID-19 during pregnancy should we really worry from vertical transmission or rather from fetal hypoxia and placental insufficiency? A systematic review. Egypt. Pediatr. Assoc. Gaz 2021, 69, 12. [Google Scholar] [CrossRef]
- Mithal, L.B.; Otero, S.; Shanes, E.D.; Goldstein, J.A.; Miller, E.S. Cord Blood Antibodies Following Maternal Coronavirus Disease 2019 Vaccination during Pregnancy. Am. J. Obs. 2021, 225, 192–194. [Google Scholar] [CrossRef]
- Definition and categorization of the timing of mother-to-child transmission of SARS-CoV-2. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-mother-to-child-transmission-2021.1 (accessed on 1 September 2022).



{kind=link}
{kind=link}
| Patient Characteristics | SARS-CoV-2-Positive Patients | |||
|---|---|---|---|---|
| Unvaccinated | Vaccinated | |||
| Symptoms + | Symptoms + | Symptoms − | p-Value (b),(c) | |
| Variable (a),(b),(c) | N = 62 | N = 12 | N = 23 | |
| Maternal age [years] (a),(b) | 29.90 ± 5.51 | 27.83 ± 3.38 | 27.61 ± 4.28 | 0.077 |
| 30 (26–35) | 26.5 (25–30) | 27 (25–30) | ||
| Hospitalization days (b) | 7 (5–13) | 9 (6–10.5) | 5 (4–7) | 0.032 * |
| (d) COVID-19 symptoms vs. non-symptoms, p = 0.014 * | ||||
| Rural area (c) | 24 (38.7%) | 6 (50%) | 7 (30.4%) | 0.531 |
| Gesta (b) | 2 (1–2) | 1 (1–2) | 1 (1–3) | 0.376 |
| Para (b) | 2 (1–2) | 1 (1–2) | 1 (1–2) | 0.458 |
| Smoker (c) | 11 (17.7%) | 5 (41.7%) | 6 (26.1%) | 0.195 |
| Initial weight (b) | 59.5 (55–65) | 63 (60.5–70.5) | 63 (60.5–67) | 0.039 * |
| (d) vaccinated vs. unvaccinated, p = 0.011 * | ||||
| (d) COVID-19 symptoms vs. non-symptoms among vaccinated, p = 0.824 | ||||
| Admission weight (b) | 70 (65–78) | 74 (69–80.5) | 74 (70–78) | 0.217 |
| Weight gain in pregnancy (b) | 11.5 (8–14) | 9 (8–12) | 11 (8.5–12) | 0.339 |
| BMI (b) | 22.46 (21.05–23.77) 2 missing values | 24.76 (22.36–25.68) | 23.95 (22.46–25.13) | 0.012 * |
| (d) vaccinated vs. unvaccinated, p = 0.004 ** | ||||
| (d) COVID-19 symptoms vs. non-symptoms among vaccinated, p = 0.482 | ||||
| Comorbidities and Treatments | SARS-CoV-2-Positive Patients | |||
|---|---|---|---|---|
| Unvaccinated | Vaccinated | |||
| Symptoms + | Symptoms + | Symptoms − | p-Value (a) | |
| Variable (a) | N = 62 | N = 12 | N = 23 | |
| Presence of at least one comorbidity (a) | 38 (61.2%) | 7 (58.3%) | 17 (73.9%) | 0.517 |
| Thyroid disease (a) | 4 (6.5%) | − | 2 (8.7%) | 0.726 |
| Thrombophilia (a) | 2 (3.2%) | − | 1 (4.3%) | >0.999 |
| Anemia (a) | 31 (50.0%) | 7 (75%) | 15 (65.2%) | 0.178 |
| Gestational diabetes (a) | 5 (8.1%) | 1 (8.3%) | − | 0.433 |
| Pregnancy hypertension (a) | 9 (14.5%) | − | − | − |
| Renal disease (a) | − | − | 1 (4.3%) | − |
| Chronic hypertension (a) | − | − | 1 (4.3%) | − |
| Cardiac disease (a) | − | − | 1 (4.3%) | − |
| Iron supplements (a) | 17 (27.4%) | − | 4 (17.4%) | 0.095 |
| Vaginal progesterone (a) | 13 (21%) | − | 13 (13%) | 0.172 |
| Vitamin supplements (a) | 18 (29%) | 2 (16.7%) | 10 (43.5%) | 0.260 |
| Aspirin (a) | 2 (3.2%) | − | − | − |
| Investigations | SARS-CoV-2-Positive Patients | |||
|---|---|---|---|---|
| Unvaccinated | Vaccinated | |||
| Symptoms + | Symptoms + | Symptoms − | p-Value (a), | |
| Variable (a) | N = 62 | N = 12 | N = 23 | |
| Leucocytes (a) | n = 62 | n = 11 | n = 22 | 0.691 |
| 9.300 (7.570–12.500) | 9.500 (8.550–11.390) | 10.650 (9.100–11.700) | ||
| Thrombocytes (a) | n = 62 | n = 11 | n = 22 | 0.649 |
| 215,000 (172,000–269,000) | 236,000 (189,500–266,000) | 213,500.50 (187,000–240,000) | ||
| PCR (a) | n = 50 | n = 11 | n = 17 | 0.005 ** |
| 14.15 (8.90–69.80) | 44.00 (18.80–73.60) | 8.90 (6.80–14.60) | ||
| D-Dimer (a) | n = 38 | n = 10 | n = 9 | 0.386 |
| 915.50 (450.00–1361.00) | 851.50 (497.00–1125.00) | 525.00 (394.00–1013.00) | ||
| COVID-19-Related Complications | SARS-CoV-2-Positive Patients | |||
|---|---|---|---|---|
| Not vaccinated | Vaccinated | |||
| Symptoms + | Symptoms + | Symptoms − | p-Value (a) | |
| Variable (a) | N = 62 | N = 12 | N = 23 | |
| High flow oxygen therapy (a) | 7 (11.3%) | 1 (8.3%) | − | 0.236 |
| Extracorporeal membrane oxygenation (a) | 2 (3.2%) | − | − | 0.690 |
| ICU transfer (a) | 12 (19.4%) | 1 (16.7%) | − | 0.070 |
| Endo-tracheal Intubation days (a) | − | |||
| 2 days | 1 (1.6%) | − | − | |
| 8 days | 1 (1.6%) | − | − | |
| 15 days | 2 (3.2%) | − | − | |
| 25 days | 1 (1.6%) | − | − | |
| 28 days | 1 (1.6%) | − | − | |
| 29 days | 1 (1.6%) | − | − | |
| Delivery and Newborn | SARS-CoV-2-Positive Patients | |||
|---|---|---|---|---|
| Not Vaccinated | Vaccinated | |||
| Symptoms + | Symptoms + | Symptoms − | p-Value (a),(b) | |
| Variable (a),(b) | N = 62 | N = 12 | N = 23 | |
| Gestational age at delivery (a) | 38 (36–40) | 38.5 (34–39.5) | 39 (38–39.5) | 0.747 |
| Prematurity (b) | 16 (25.8%) | 4 (33.3%) | 5(21.7%) | 0.886 |
| <28 weeks (b) | 2 (3%) | − | − | |
| 28–32 weeks (b) | 7 (11.3%) | 1 (8.3%) | 3 (13%) | |
| 32–37 weeks (b) | 7 (11.3%) | 3 (25%) | 2 (8.69%) | |
| Term delivery (b) | 46(74.1%) | 8 (66.6%) | 18 (78.2%) | |
| Gender F (b) | 33 (53.2%) | 5 (41.7%) | 10 (43.5%) | 0.615 |
| Maternal death (b) | 5 (8.1%) | − | − | − |
| IUFD (b) | 3 (4%) | − | − | − |
| C-section (b) | 40 (64.5%) | 10 (83.3%) | 15 (65.2%) | 0.481 |
| Emergency C−section due to COVID-19 complications | 15 (28.8%) | 1 (8.3%) | − | 0.007 ** |
| Newborn COVID-19 (b) | 2 (2.32%) | − | − | − |
| Birth weight [g] (a) | 3150 (2610–3380) | 3495 (2590–3670) | 3310 (2750–3600) | 0.285 |
| 5 min Apgar Index (a) | 9 (8–9) for 61 newborns 1 missing value | 8 (7–9) | 8 (8–9) | 0.438 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moza, A.; Bernad, E.S.; Lungeanu, D.; Craina, M.; Bernad, B.C.; Hogea, L.; Paul, C.; Muresan, C.; Nitu, R.; Iacob, D. Pregnancy Outcomes in SARS-CoV-2-Positive Patients: A 20-Month Retrospective Analysis of Delivery Cases. Medicina 2023, 59, 341. https://doi.org/10.3390/medicina59020341
Moza A, Bernad ES, Lungeanu D, Craina M, Bernad BC, Hogea L, Paul C, Muresan C, Nitu R, Iacob D. Pregnancy Outcomes in SARS-CoV-2-Positive Patients: A 20-Month Retrospective Analysis of Delivery Cases. Medicina. 2023; 59(2):341. https://doi.org/10.3390/medicina59020341
Chicago/Turabian StyleMoza, Andreea, Elena S. Bernad, Diana Lungeanu, Marius Craina, Brenda C. Bernad, Lavinia Hogea, Corina Paul, Cezara Muresan, Razvan Nitu, and Daniela Iacob. 2023. "Pregnancy Outcomes in SARS-CoV-2-Positive Patients: A 20-Month Retrospective Analysis of Delivery Cases" Medicina 59, no. 2: 341. https://doi.org/10.3390/medicina59020341