
New-Onset Kidney Diseases after COVID-19 Vaccination: A Case Series

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Case Presentation
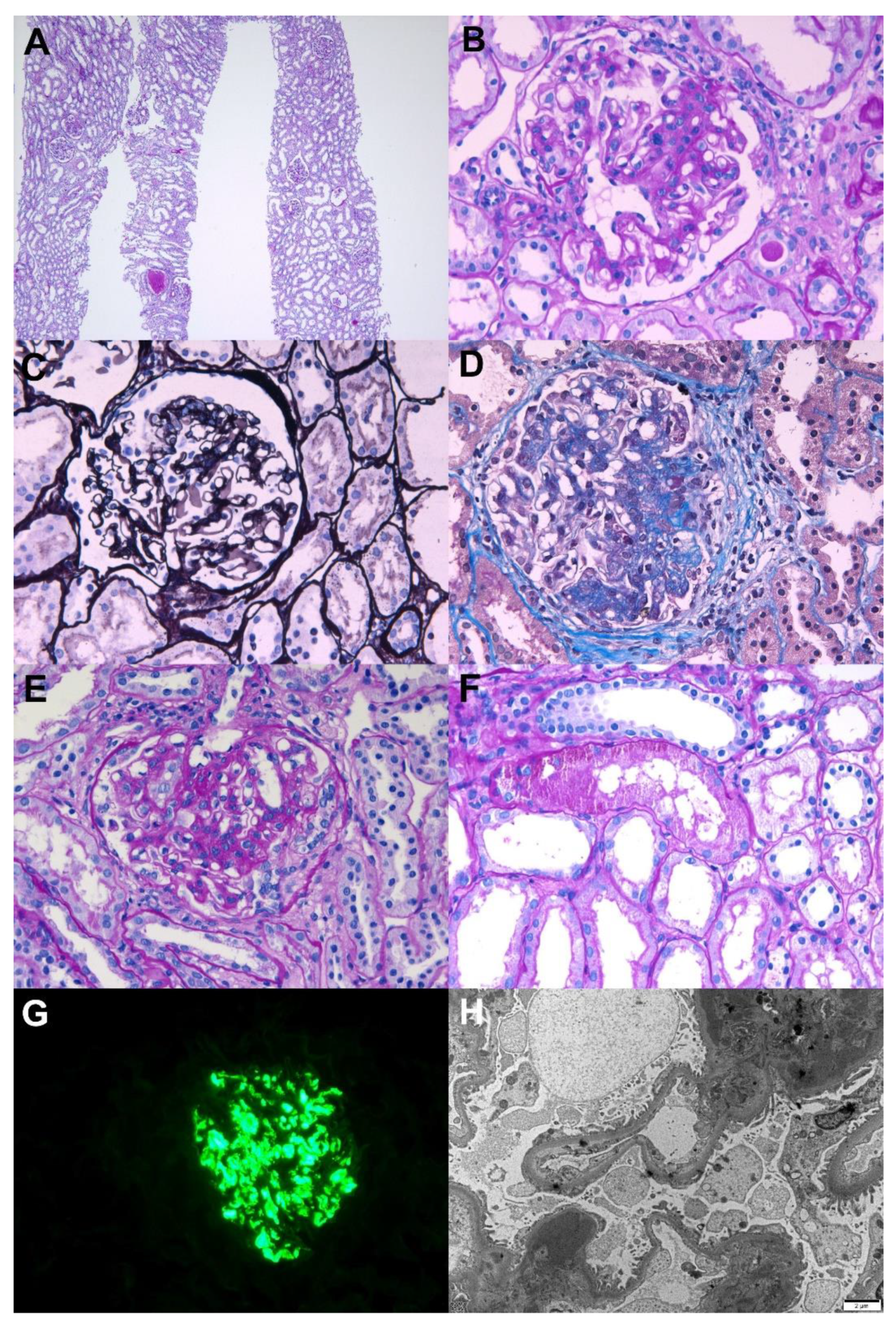
2.1. IgA Nephropathy Presenting with Painless Gross Hematuria
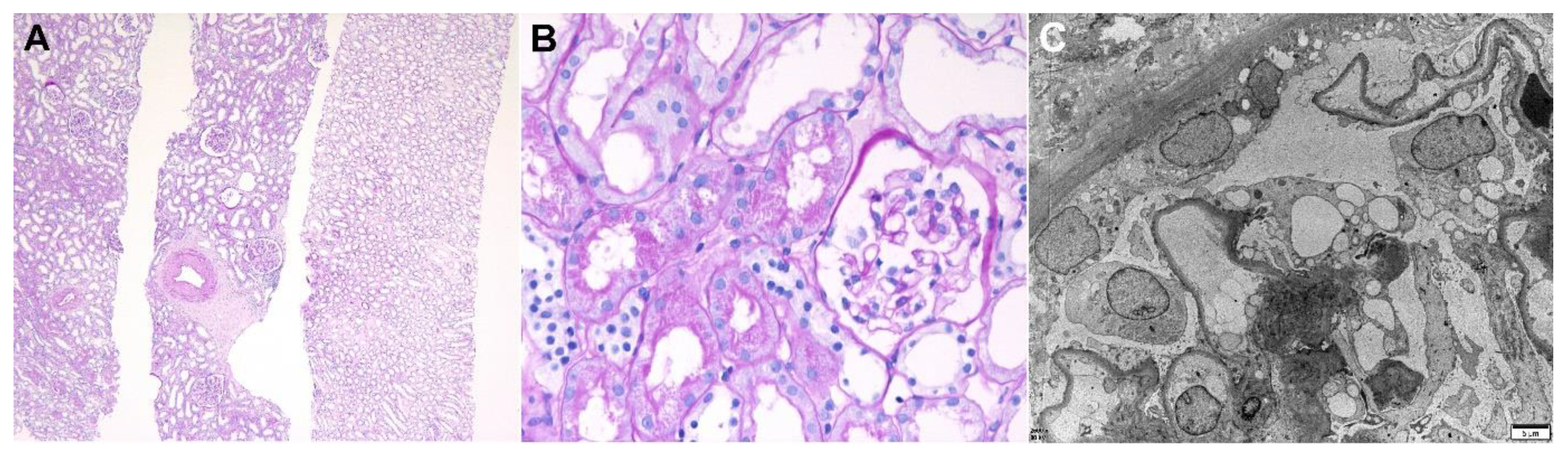
2.2. Minimal Change Disease Presenting with Nephrotic Syndrome
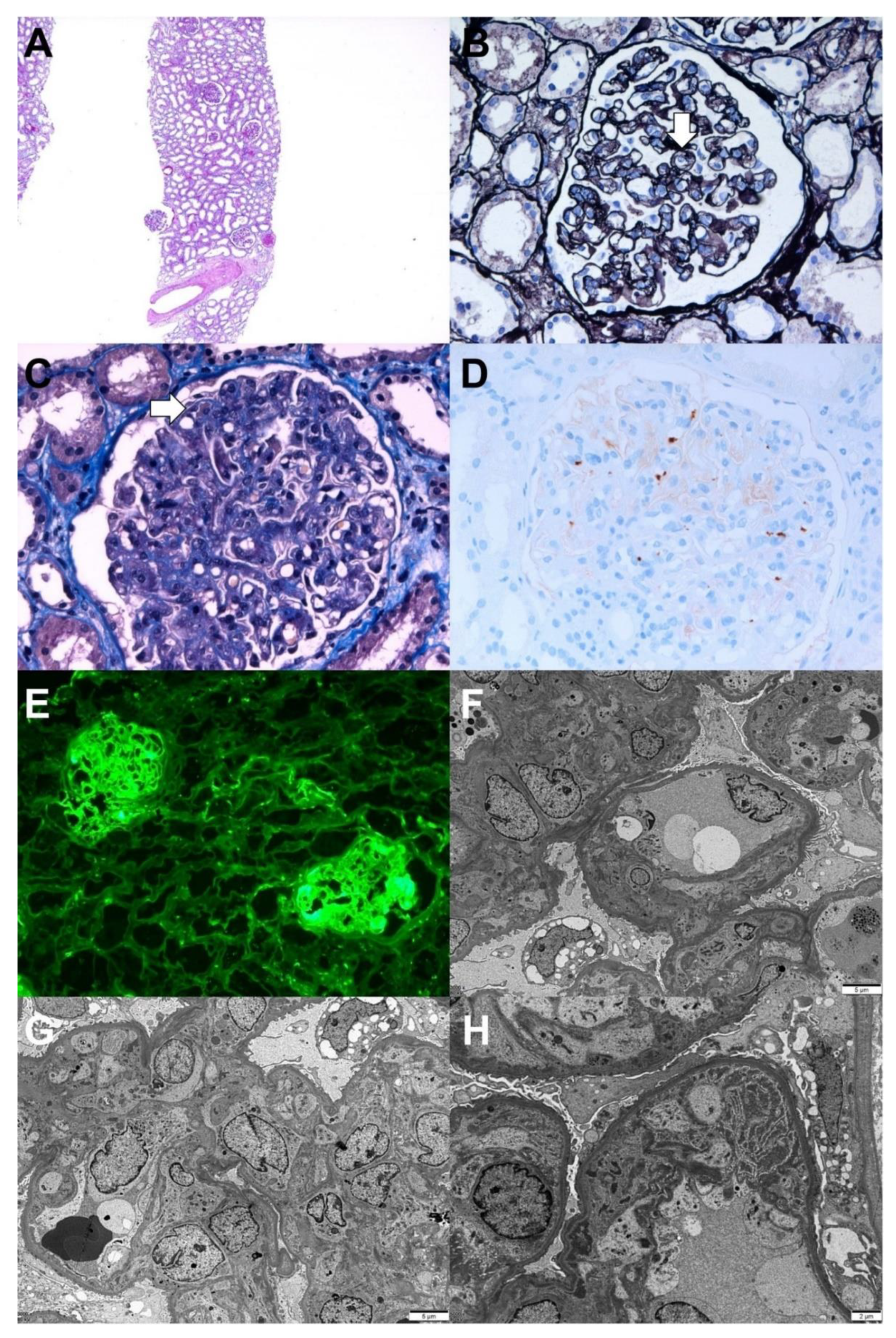
2.3. Thrombotic Microangiopathy Presenting with Acute Kidney Injury
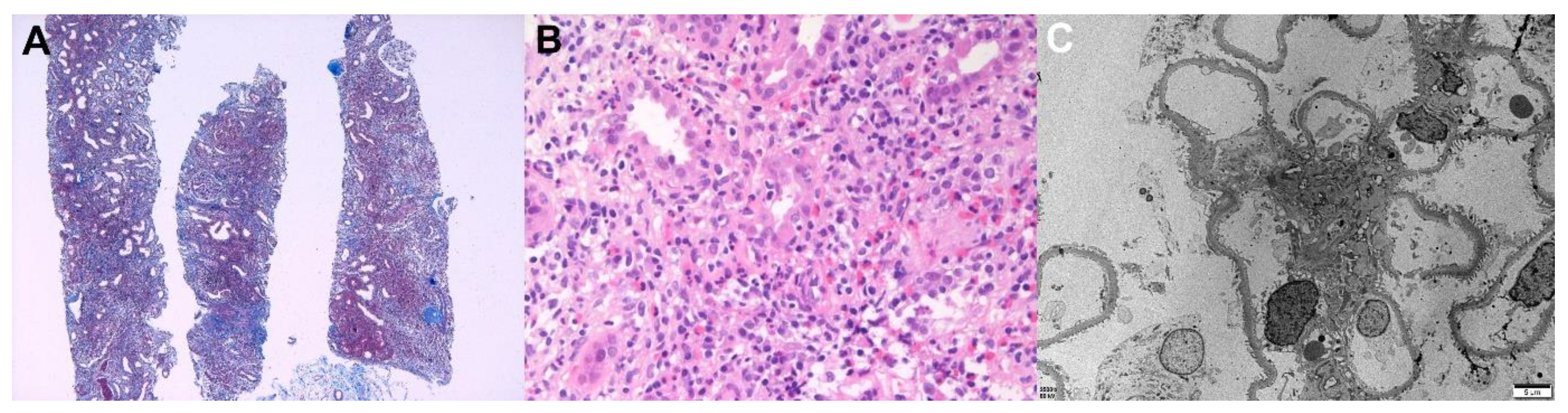
2.4. Acute Tubulointerstitial Nephritis Presenting with Acute Kidney Injury
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pilishvili, T.; Gierke, R.; Fleming-Dutra, K.E.; Farrar, J.L.; Mohr, N.M.; Talan, D.A.; Krishnadasan, A.; Harland, K.K.; Smithline, H.A.; Hou, P.C.; et al. Effectiveness of mRNA Covid-19 vaccine among U.S. Health care personnel. N. Engl. J. Med. 2021, 385, e90. [Google Scholar] [CrossRef]
- Beatty, A.L.; Peyser, N.D.; Butcher, X.E.; Cocohoba, J.M.; Lin, F.; Olgin, J.E.; Pletcher, M.J.; Marcus, G.M. Analysis of COVID-19 vaccine type and adverse effects following vaccination. JAMA Netw. Open 2021, 4, e2140364. [Google Scholar] [CrossRef]
- Lim, J.H.; Han, M.H.; Kim, Y.J.; Kim, M.S.; Jung, H.Y.; Choi, J.Y.; Cho, J.H.; Kim, C.D.; Kim, Y.L.; Park, S.H. New-onset nephrotic syndrome after Janssen COVID-19 vaccination: A case report and literature review. J. Korean Med. Sci. 2021, 36, e218. [Google Scholar] [CrossRef] [PubMed]
- Klomjit, N.; Alexander, M.P.; Fervenza, F.C.; Zoghby, Z.; Garg, A.; Hogan, M.C.; Nasr, S.H.; Minshar, M.A.; Zand, L. COVID-19 vaccination and glomerulonephritis. Kidney Int. Rep. 2021, 6, 2969–2978. [Google Scholar] [CrossRef] [PubMed]
- Bomback, A.S.; Kudose, S.; D’Agati, V.D. De novo and relapsing glomerular diseases after COVID-19 vaccination: What do we know so far? Am. J. Kidney Dis. 2021, 78, 477–480. [Google Scholar] [CrossRef] [PubMed]
- Schena, F.P.; Nistor, I. Epidemiology of IgA nephropathy: A global perspective. Semin Nephrol. 2018, 38, 435–442. [Google Scholar] [CrossRef]
- Yim, T.; Kim, S.U.; Park, S.; Lim, J.H.; Jung, H.Y.; Cho, J.H.; Kim, C.D.; Kim, Y.L.; Han, M.H.; Kim, Y.J.; et al. Patterns in renal diseases diagnosed by kidney biopsy: A single-center experience. Kidney Res. Clin. Pract. 2020, 39, 60–69. [Google Scholar] [CrossRef] [Green Version]
- Lai, K.N. Pathogenesis of IgA nephropathy. Nat. Rev. Nephrol. 2012, 8, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Vivarelli, M.; Massella, L.; Ruggiero, B.; Emma, F. Minimal change disease. Clin. J. Am. Soc. Nephrol. 2017, 12, 332–345. [Google Scholar] [CrossRef] [Green Version]
- Timmermans, S.A.M.E.G.; Busch, M.H.; Abdul-Hamid, M.A.; Frenken, L.A.M.; Aarnoudse, A.J.; van Paassen, P. Limburg Renal Registry Primary Podocytopathies following Covid-19 Vaccination. Kidney Int. Rep. 2021. [Google Scholar] [CrossRef] [PubMed]
- D’Agati, V.D.; Kudose, S.; Bomback, A.S.; Adamidis, A.; Tartini, A. Minimal change disease and acute kidney injury following the Pfizer-BioNTech COVID-19 vaccine. Kidney Int. 2021, 100, 461–463. [Google Scholar] [CrossRef] [PubMed]
- Kervella, D.; Jacquemont, L.; Chapelet-Debout, A.; Deltombe, C.; Ville, S. Minimal change disease relapse following SARS-CoV-2 mRNA vaccine. Kidney Int. 2021, 100, 457–458. [Google Scholar] [CrossRef]
- Lebedev, L.; Sapojnikov, M.; Wechsler, A.; Varadi-Levi, R.; Zamir, D.; Tobar, A.; Levin-Iaina, N.; Fytlovich, S.; Yagil, Y. Minimal change disease following the Pfizer-BioNTech COVID-19 vaccine. Am. J. Kidney Dis. 2021, 78, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Bitzan, M.; Zieg, J. Influenza-associated thrombotic microangiopathies. Pediatr. Nephrol. 2018, 33, 2009–2025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sol, M.Y. Pathology of thrombotic microangiopathy. J. Korean Soc. Pediatr. Nephrol. 2013, 17, 6–12. [Google Scholar] [CrossRef]
- Ruggenenti, P.; Noris, M.; Remuzzi, G. Thrombotic microangiopathy, hemolytic uremic syndrome, and thrombotic thrombocytopenic purpura. Kidney Int. 2001, 60, 831–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Fabritiis, M.; Angelini, M.L.; Fabbrizio, B.; Cenacchi, G.; Americo, C.; Cristino, S.; Lifrieri, M.F.; Cappuccilli, M.; Spazzoli, A.; Zambianchi, L.; et al. Renal thrombotic microangiopathy in concurrent COVID-19 vaccination and infection. Pathogens 2021, 10, 1045. [Google Scholar] [CrossRef]
- Mira, F.S.; Costa Carvalho, J.; de Almeida, P.A.; Pimenta, A.C.; Alen Coutinho, I.; Figueiredo, C.; Rodrigues, L.; Sousa, V.; Ferreira, E.; Pinto, H.; et al. A case of acute interstitial nephritis after two doses of the BNT162b2 SARS-CoV-2 vaccine. Int. J. Nephrol. Renovasc. Dis. 2021, 14, 421–426. [Google Scholar] [CrossRef]
- Koda, R.; Watanabe, H.; Tsuchida, M.; Iino, N.; Suzuki, K.; Hasegawa, G.; Imai, N.; Narita, I. Immune checkpoint inhibitor (nivolumab)-associated kidney injury and the importance of recognizing concomitant medications known to cause acute tubulointerstitial nephritis: A case report. BMC Nephrol. 2018, 19, 48. [Google Scholar] [CrossRef]
- Kawamata, M.; Akimoto, T.; Sugase, T.; Otani-Takei, N.; Miki, T.; Masuda, T.; Kobayashi, T.; Takeda, S.; Muto, S.; Nagata, D. Tubulointerstitial nephritis and uveitis syndrome: Are drugs offenders or bystanders? Clin. Med. Insights Case Rep. 2016, 9, 21–24. [Google Scholar] [CrossRef] [Green Version]
- Segal, Y.; Shoenfeld, Y. Vaccine-induced autoimmunity: The role of molecular mimicry and immune crossreaction. Cell Mol. Immunol. 2018, 15, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Caso, F.; Costa, L.; Ruscitti, P.; Navarini, L.; Del Puente, A.; Giacomelli, R.; Scarpa, R. Could Sars-coronavirus-2 trigger autoimmune and/or autoinflammatory mechanisms in genetically predisposed subjects? Autoimmun. Rev. 2020, 19, 102524. [Google Scholar] [CrossRef] [PubMed]
- Sette, A.; Crotty, S. Adaptive immunity to SARS-CoV-2 and COVID-19. Cell 2021, 184, 861–880. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, J.C.; Cunha, F.; Coutinho, I.A.; Loureiro, C.; Faria, E.; Bom, A.T. Hypersensitivity reactions to vaccines: Current evidence and standards for SARS-CoV-2 vaccines. Acta Med. Port 2021, 34, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Nassar, M.; Chung, H.; Dhayaparan, Y.; Nyein, A.; Acevedo, B.J.; Chicos, C.; Zheng, D.; Barras, M.; Mohamed, M.; Alfishawy, M.; et al. COVID-19 vaccine induced rhabdomyolysis: Case report with literature review. Diabetes Metab. Syndr. 2021, 15, 102170. [Google Scholar] [CrossRef] [PubMed]
- Gaut, J.P.; Liapis, H. Acute kidney injury pathology and pathophysiology: A retrospective review. Clin. Kidney J. 2021, 14, 526–536. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathologic Diagnosis | Age/ Sex | Clinical Presentation | Underlying Diseases | Types of Vaccine/ Manufacturer/ Dose | Symptom Onset Time/Biopsy Time after Vaccination, Days | Kidney Histopathology | Scr at Baseline, mg/dL | Scr at Biopsy, mg/dL | UPCR at Biopsy, g/gCr | Treatment | Response (Follow-Up Duration after Diagonsis) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| IgA nephropathy, Haas III (M0E1C1S1T0) | 42/F | Gross hematuria | None | mRNA/ Moderna (Cambridge, MA, USA)/ 2nd | 1/54 | LM: mesangial hypercellular with increased mesangial matrix, cellular crescent, segmental sclerosis, endocapillary proliferation IF: IgA 3+, C3 1+, kappa 2+, lambda 2+ EM: many large mesangial electron dense deposits, focal foot process loss | 0.47 at 5 weeks before biopsy | 0.45 | 1.67 | RASi | PR (11 weeks) |
| Minimal change disease | 52/M | Nephrotic syndrome | None | Vector/ Janssen (Raritan, NJ, USA)/ 1st | 7/33 | LM: normal glomeruli, intact tubules and interstitium IF: all negative EM: diffuse foot process loss | NA (normal) | 1.96 | 7.12 | High-dose steroid treatment | CR (31 weeks) |
| Chronic thrombotic microangiopathy | 69/F | Acute kidney injury | Type 2 diabetes mellitus | Vector/ AstraZeneca (Cambridge, UK)/ 1st | 2/14 | LM: diffuse thickening of the capillary wall with capillary loop doubling, hyaline thrombi in glomeruli, intact tubules and interstitium, mild infiltration of lymphocytes in the interstitium, arterial fibrointimal thickening IF: fibrinogen 3+ in the glomeruli EM: duplications of the glomerular basement membranes with cellular interpositions, endothelial swelling and hypertrophy with occlusion of the lumens, glomerular intracapillary fibrin deposition with entrapped cellular debris, diffuse foot process loss | 0.80 at 1 year before biopsy | 3.69 | 5.20 | None | SR (21 weeks) |
| Acute tubulointerstitial nephritis | 44/M | Acute kidney injury | Type 2 diabetes mellitus, chronic hepatitis B, hyperlipidemia | mRNA/ Moderna (Cambridge, MA, USA)/ 1st | 1/28 | LM: normal glomeruli, mild IF/TA, massive mixed inflammatory cell infiltrates in the tubular epithelium (tubulitis) and interstitium IF: all negative EM: normal glomeruli | 0.91 at 10 weeks before biopsy | 4.94 | 1.01 | High-dose steroid treatment | PR (11 weeks) |
| Acute tubulointerstitial nephritis with myoglobin tubular casts | 77/F | Acute kidney injury | Chronic hepatitis B, hepatocellular carcinoma, type 2 diabetes mellitus | mRNA/ Pfizer (New York, NY, USA)/ 2nd | 1/14 | LM: normal glomeruli, mild IF/TA, infiltration of the inflammatory cells in the interstitium, myoglobin casts in the tubules IF: all negative EM: electron dense granular casts in tubules, focal foot process loss | 0.98 at 12 weeks before biopsy | 11.15 | 4.63 | Low-dose steroid treatment, hemodialysis | PR (23 weeks) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, J.-H.; Kim, M.-S.; Kim, Y.-J.; Han, M.-H.; Jung, H.-Y.; Choi, J.-Y.; Cho, J.-H.; Kim, C.-D.; Kim, Y.-L.; Park, S.-H. New-Onset Kidney Diseases after COVID-19 Vaccination: A Case Series. Vaccines 2022, 10, 302. https://doi.org/10.3390/vaccines10020302
Lim J-H, Kim M-S, Kim Y-J, Han M-H, Jung H-Y, Choi J-Y, Cho J-H, Kim C-D, Kim Y-L, Park S-H. New-Onset Kidney Diseases after COVID-19 Vaccination: A Case Series. Vaccines. 2022; 10(2):302. https://doi.org/10.3390/vaccines10020302
Chicago/Turabian StyleLim, Jeong-Hoon, Mee-Seon Kim, Yong-Jin Kim, Man-Hoon Han, Hee-Yeon Jung, Ji-Young Choi, Jang-Hee Cho, Chan-Duck Kim, Yong-Lim Kim, and Sun-Hee Park. 2022. "New-Onset Kidney Diseases after COVID-19 Vaccination: A Case Series" Vaccines 10, no. 2: 302. https://doi.org/10.3390/vaccines10020302