
Using Latent Class Analyses to Examine Health Disparities among Young Children in Socially Disadvantaged Families during the COVID-19 Pandemic

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Methods
3. Measures
3.1. Family Hardship
3.2. Child Maltreatment
3.3. Child Psychosocial Problems
3.4. Parenting Stress
3.5. Child Physical Wellbeing
3.6. Parent-Child Activities
3.7. Child Lifestyle Practices
3.8. Demographic Covariates
4. Data Analysis
5. Results
5.1. Demographics
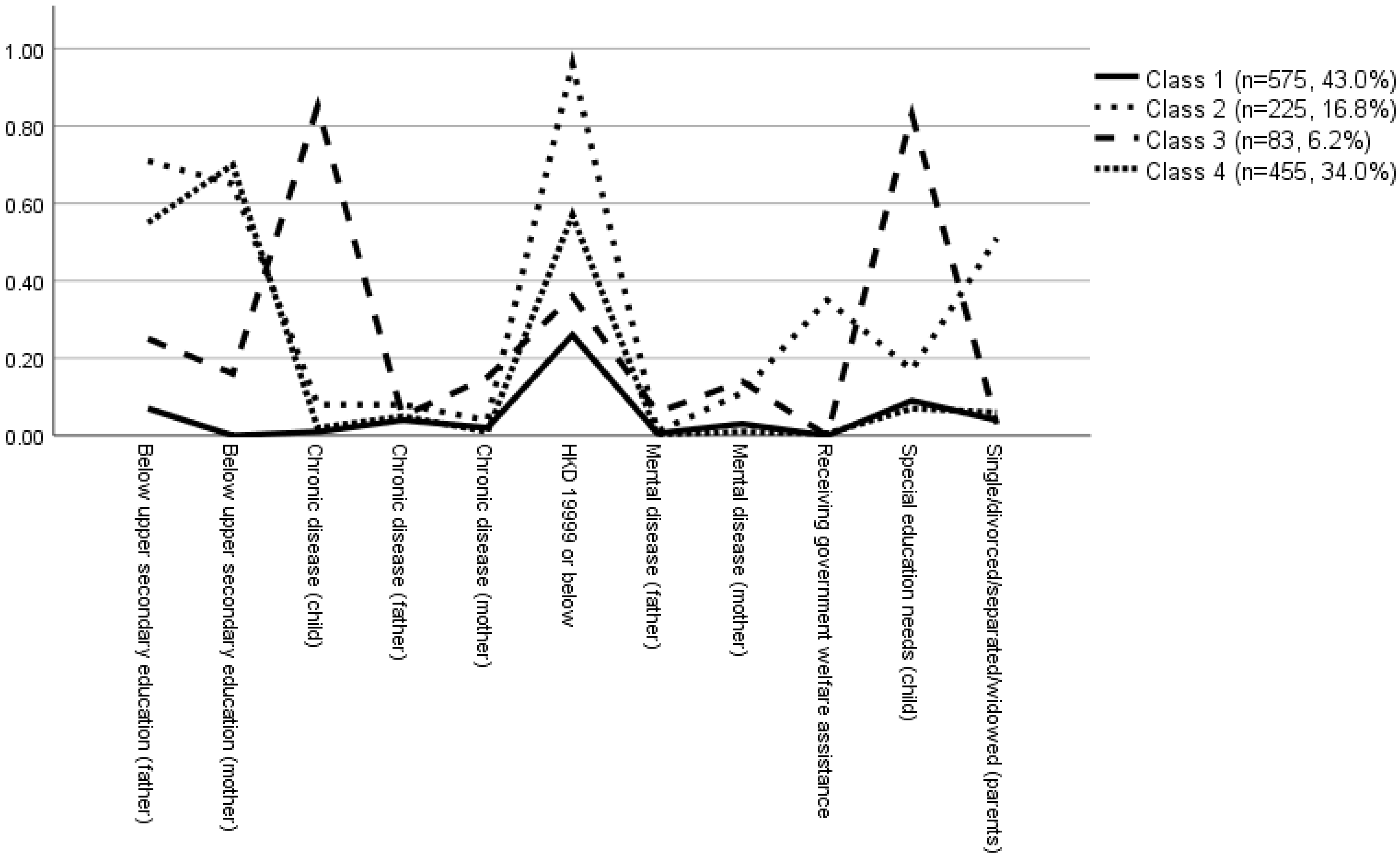
5.2. Latent Class Analysis
5.3. Comparison of the Four Classes on Parenting Behavior, Lifestyle Practices, and Wellbeing under the COVID-19 Pandemic
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Justice, L.M.; Jiang, H.; Bates, R.; Koury, A. Language Disparities Related to Maternal Education Emerge by Two Years in a Low-Income Sample. Matern. Child Health J. 2020, 24, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Toledano-Toledano, F.; Domínguez-Guedea, M.T. Psychosocial factors related with caregiver burden among families of children with chronic conditions. BioPsychoSocial Med. 2019, 13, 6. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.-M.; Leu, C.-H.; Wang, T.-M. Measurement and Determinants of Multidimensional Poverty: Evidence from Taiwan. Soc. Indic. Res. 2019, 145, 459–478. [Google Scholar] [CrossRef]
- Haveman, R.; Wolff, E.N. The concept and measurement of asset poverty: Levels, trends and composition for the U.S., 1983–2001. J. Econ. Inequal. 2004, 2, 145–169. [Google Scholar] [CrossRef]
- Shah, R.; Ali, F.M.; Finlay, A.Y.; Salek, M.S. Family reported outcomes, an unmet need in the management of a patient’s disease: Appraisal of the literature. Health Qual. Life Outcomes 2021, 19, 194. [Google Scholar] [CrossRef]
- Guo, V.Y.W.; Wong, C.K.H.; Wong, R.S.M.; Yu, E.Y.T.; Ip, P.; Lam, C.L.K. Spillover Effects of Maternal Chronic Disease on Children’s Quality of Life and Behaviors Among Low-Income Families. Patient 2018, 11, 625–635. [Google Scholar] [CrossRef]
- Masuda, R.; Lanier, P.; Hashimoto, H. The Association between Paternal Job Stress and Maternal Child Corporal Punishment: Evidence from a Population-Based Survey in Metropolitan Japan. J. Fam. Violence 2019, 34, 119–126. [Google Scholar] [CrossRef] [Green Version]
- Manthalu, G.; Nkhoma, D.; Kuyeli, S. Simple versus composite indicators of socioeconomic status in resource allocation formulae: The case of the district resource allocation formula in Malawi. BMC Health Serv. Res. 2010, 10, 6. [Google Scholar] [CrossRef] [Green Version]
- Schoon, I.; Hope, S.; Ross, A.; Duckworth, K. Family hardship and children’s development: The early years. Longitud. Life Course Stud. 2010, 1, 14. [Google Scholar]
- Xu, Y.; Bright, C.L.; Barth, R.P.; Ahn, H. Poverty and Economic Pressure, Financial Assistance, and Children’s Behavioral Health in Kinship Care. Child Maltreat. 2020, 26, 28–39. [Google Scholar] [CrossRef]
- Collins, L.M.; Lanza, S.T. Latent Class and Latent Transition Analysis: With Applications in the Social, Behavioral, and Health Sciences; John Wiley & Sons: Hoboken, NJ, USA, 2009; Volume 718. [Google Scholar]
- Li, L.-Q.; Huang, T.; Wang, Y.-Q.; Wang, Z.-P.; Liang, Y.; Huang, T.-B.; Zhang, H.-Y.; Sun, W.; Wang, Y. COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Marchi, J.; Johansson, N.; Sarkadi, A.; Warner, G. The Impact of the COVID-19 Pandemic and Societal Infection Control Measures on Children and Adolescents’ Mental Health: A Scoping Review. Front. Psychiatry 2021, 12, 711791. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Zhou, W.; Kabiri, A.; Darzi, A.; Hu, S.; Younes, H.; Zhang, L. COVID-19 and Income Profile: How People in Different Income Groups Responded to Disease Outbreak, Case Study of the United States. arXiv 2020, arXiv:2007.02160v1. [Google Scholar]
- Tso, W.W.Y.; Wong, R.S.; Tung, K.T.S.; Rao, N.; Fu, K.W.; Yam, J.C.S.; Chua, G.T.; Chen, E.Y.H.; Lee, T.M.C.; Chan, S.K.W.; et al. Vulnerability and resilience in children during the COVID-19 pandemic. Eur. Child Adolesc. Psychiatry 2020, 31, 161–176. [Google Scholar] [CrossRef]
- Lawson, M.; Piel, M.H.; Simon, M. Child Maltreatment during the COVID-19 Pandemic: Consequences of Parental Job Loss on Psychological and Physical Abuse Towards Children. Child Abus. Negl. 2020, 110, 104709. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur. Child Adolesc. Psychiatry 2021, 31, 879–889. [Google Scholar] [CrossRef]
- Blasius, J.; Brandt, M. Representativeness in Online Surveys through Stratified Samples. Bull. Sociol. Methodol. Bull. Méthodol. Sociol. 2010, 107, 5–21. [Google Scholar] [CrossRef]
- Census and Statistics Department. Thematic Report: Household Income Distribution in Hong Kong. 2016. Available online: https://www.bycensus2016.gov.hk/data/16BC_Income_Report.pdf (accessed on 12 November 2021).
- Census and Statistics Department. Population and Household Statistics Analysed by District Council District. 2021. Available online: https://www.censtatd.gov.hk/en/EIndexbySubject.html?pcode=B1130301&scode=150 (accessed on 12 November 2021).
- Centre for Health Protection. Latest Situation of Cases of COVID-19. Available online: https://www.chp.gov.hk/en/features/102997.html (accessed on 12 November 2021).
- Chung, R.Y.; Chung, G.K.; Marmot, M.; Allen, J.; Chan, D.; Goldblatt, P.; Wong, H.; Lai, E.; Woo, J.; Yeoh, E.K.; et al. COVID-19 related health inequality exists even in a city where disease incidence is relatively low: A telephone survey in Hong Kong. J. Epidemiol. Community Health 2021, 75, 616–623. [Google Scholar] [CrossRef]
- Chua, G.T.; Wong, J.S.C.; Lam, I.; Ho, P.P.K.; Chan, W.H.; Yau, F.Y.S.; Rosa Duque, J.S.; Ho, A.C.C.; Siu, K.K.; Cheung, T.W.Y.; et al. Clinical Characteristics and Transmission of COVID-19 in Children and Youths During 3 Waves of Outbreaks in Hong Kong. JAMA Netw. Open 2021, 4, e218824. [Google Scholar] [CrossRef]
- Labour and Welfare Bureau. Recipients of the Comprehensive Social Security Assistance (CSSA) Scheme by District Council Districts; Labour and Welfare Bureau: Hong Kong, China, 2015.
- Straus, M.A.; Hamby, S.L.; Finkelhor, D.; Moore, D.W.; Runyan, D. Identification of Child Maltreatment with the Parent-Child Conflict Tactics Scales: Development and Psychometric Data for a National Sample of American Parents. Child Abus. Negl. 1998, 22, 249–270. [Google Scholar] [CrossRef]
- Croft, S.; Stride, C.; Maughan, B.; Rowe, R. Validity of the Strengths and Difficulties Questionnaire in Preschool-Aged Children. Pediatrics 2015, 135, e1210–e1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, R.S.; Tung, K.T.S.; Cheng, A.W.F.; Shiu, Y.K.; Wong, W.H.S.; Tso, W.W.Y.; Ho, M.S.P.; Chan, K.L.; Ho, F.K.W.; Lo, C.K.M.; et al. Disentangling the Effects of Exposure to Maternal Substance Misuse and Physical Abuse and Neglect on Child Behavioral Problems. J. Interpers. Violence 2019, 36, 8435–8455. [Google Scholar] [CrossRef] [PubMed]
- Leung, C.; Tsang, S.K.M. The Chinese Parental Stress Scale: Psychometric Evidence Using Rasch Modeling on Clinical and Nonclinical Samples. J. Personal. Assess. 2010, 92, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W.; Burwinkle, T.M.; Seid, M.; Skarr, D. The PedsQL™* 4.0 as a Pediatric Population Health Measure: Feasibility, Reliability, and Validity. Ambul. Pediatr. 2003, 3, 329–341. [Google Scholar] [CrossRef]
- Ip, P.; Rao, N.; Bacon-Shone, J.; Li, S.L.; Ho, F.K.-W.; Chow, C.-B.; Jiang, F. Socioeconomic gradients in school readiness of Chinese preschool children: The mediating role of family processes and kindergarten quality. Early Child. Res. Q. 2016, 35, 111–123. [Google Scholar] [CrossRef]
- Buuren, S.V.; Groothuis-Oudshoorn, K. Mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 2010, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Linzer, D.A.; Lewis, J.B. poLCA: An R package for polytomous variable latent class analysis. J. Stat. Softw. 2011, 42, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Vrieze, S.I. Model selection and psychological theory: A discussion of the differences between the Akaike information criterion (AIC) and the Bayesian information criterion (BIC). Psychol. Methods 2012, 17, 228–243. [Google Scholar] [CrossRef] [Green Version]
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Struct. Equ. Model. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Bauer, D.J.; Curran, P.J. Distributional assumptions of growth mixture models: Implications for overextraction of latent trajectory classes. Psychol. Methods 2003, 8, 338. [Google Scholar] [CrossRef] [Green Version]
- Finch, H.; Bolin, J. Multilevel Modeling Using Mplus; CRC Press: Boca Raton, FL, USA, 2017. [Google Scholar]
- Djelantik, A.A.A.M.J.; Smid, G.E.; Kleber, R.J.; Boelen, P.A. Symptoms of prolonged grief, post-traumatic stress, and depression after loss in a Dutch community sample: A latent class analysis. Psychiatry Res. 2017, 247, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Arcaya, M.C.; Arcaya, A.L.; Subramanian, S.V. Inequalities in health: Definitions, concepts, and theories. Glob. Health Action 2015, 8, 27106. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Drake, B. Child maltreatment risk as a function of poverty and race/ethnicity in the USA. Int. J. Epidemiol. 2018, 47, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Qian, Y.; Fan, W. Who loses income during the COVID-19 outbreak? Evidence from China. Res. Soc. Stratif. Mobil. 2020, 68, 100522. [Google Scholar] [CrossRef]
- Wickham, S.; Anwar, E.; Barr, B.; Law, C.; Taylor-Robinson, D. Poverty and child health in the UK: Using evidence for action. Arch. Dis. Child. 2016, 101, 759. [Google Scholar] [CrossRef] [Green Version]
- Hertzman, C.; Power, C. Health and human development: Understandings from life-course research. Dev. Neuropsychol. 2003, 24, 719–744. [Google Scholar]
- Rodriguez, C.M. Parental Discipline Reactions to Child Noncompliance and Compliance: Association with Parent–Child Aggression Indicators. J. Child Fam. Stud. 2016, 25, 1363–1374. [Google Scholar] [CrossRef]
- Hertz-Palmor, N.; Moore, T.M.; Gothelf, D.; Di Domenico, G.E.; Dekel, I.; Greenberg, D.M.; Brown, L.A.; Matalon, N.; Visoki, E.; White, L.K.; et al. Association among income loss, financial strain and depressive symptoms during COVID-19: Evidence from two longitudinal studies. J. Affect. Disord. 2021, 291, 1–8. [Google Scholar] [CrossRef]
- Orben, A.; Tomova, L.; Blakemore, S.J. The effects of social deprivation on adolescent development and mental health. Lancet Child Adolesc. Health 2020, 4, 634–640. [Google Scholar] [CrossRef]
- Douglas, M.; Katikireddi, S.V.; Taulbut, M.; McKee, M.; McCartney, G. Mitigating the wider health effects of covid-19 pandemic response. BMJ 2020, 369, m1557. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Observed | Imputed |
|---|---|---|
| Age (in years), mean (SD) | 4.83 (0.99) | 4.76 (1.02) |
| Gender, n (%) | ||
| Boy | 617 (46.9) | 721 (53.9) |
| Girl | 699 (53.1) | 617 (46.1) |
| Mother having chronic disease, n (%) | ||
| Yes | 32 (2.4) | 35 (2.6) |
| No | 1285 (97.6) | 1303 (97.4) |
| Father having chronic disease, n (%) | ||
| Yes | 66 (5.0) | 66 (4.9) |
| No | 1249 (95.0) | 1272 (95.1) |
| Child having chronic disease, n (%) | ||
| Yes | 101 (7.6) | 101 (7.5) |
| No | 1227 (92.4) | 1237 (92.5) |
| Child having special educational needs, n (%) | ||
| Yes | 190 (14.4) | 190 (14.2) |
| No | 1127 (85.6) | 1148 (85.8) |
| Mother having mental disorder, n (%) | ||
| Yes | 52 (3.9) | 57 (4.3) |
| No | 1268 (96.1) | 1281 (95.7) |
| Father having mental disorder, n (%) | ||
| Yes | 12 (0.9) | 12 (0.9) |
| No | 1306 (99.1) | 1326 (99.1) |
| Maternal education level, n (%) | ||
| Below upper secondary education | 434 (33.5) | 475 (35.5) |
| Upper secondary education or above | 863 (66.5) | 863 (64.5) |
| Paternal education level, n (%) | ||
| Below upper secondary education | 416 (32.5) | 471 (35.2) |
| Upper secondary education or above | 864 (67.5) | 867 (64.8) |
| Parental marital status, n (%) | ||
| Cohabited/married | 1169 (91.5) | 1169 (87.4) |
| Single/divorced/separated/widowed | 108 (8.5) | 169 (12.6) |
| Monthly household income, n (%) | ||
| HKD 19,999 or below | 597 (46.9) | 652 (48.7) |
| Above HKD 19,999 | 676 (53.1) | 686 (51.3) |
| Receiving government welfare assistance, n (%) | ||
| Yes | 80 (6.4) | 80 (6.0) |
| No | 1177 (93.6) | 1258 (94.0) |
| Severe physical maltreatment, n (%) | ||
| Yes | 32 (2.6) | 131 (9.8) |
| No | 1207 (97.4) | 1207 (90.2) |
| Physical maltreatment, n (%) | ||
| Yes | 115 (9.3) | 218 (16.3) |
| No | 1118 (90.7) | 1120 (83.7) |
| Corporal punishment, n (%) | ||
| Yes | 836 (68.2) | 891 (66.6) |
| No | 389 (31.8) | 447 (33.4) |
| Non-violent discipline, n (%) | ||
| Yes | 1090 (89.2) | 1090 (81.5) |
| No | 132 (10.8) | 248 (18.5) |
| Psychological aggression, n (%) | ||
| Yes | 975 (79.5) | 975 (72.9) |
| No | 252 (20.5) | 363 (27.1) |
| Neglect, n (%) | ||
| Yes | 297 (24.0) | 392 (29.3) |
| No | 941 (76.0) | 946 (70.7) |
| Externalizing problems (0–20), mean (SD) | 6.99 (3.19) | 7.03 (3.10) |
| Internalizing problems (0–20), mean (SD) | 4.90 (2.76) | 4.96 (2.69) |
| Parenting stress (17–102), mean (SD) | 48.03 (11.24) | 49.82 (13.29) |
| Physical wellbeing (0–100), mean (SD) | 87.34 (13.09) | 87.18 (13.39) |
| Parent-child learning activities (0–3), mean (SD) | 1.97 (0.67) | 1.97 (0.69) |
| Parent-child recreational activities (0–3), mean (SD) | 1.63 (0.63) | 1.58 (0.67) |
| Sleep duration (hour/day), mean (SD) | 10.84 (0.87) | 11.08 (0.89) |
| Exercise duration (hour/day), mean (SD) | 1.21 (0.69) | 1.83 (0.96) |
| Electronic device use for learning (hour/day), mean (SD) | 1.09 (0.83) | 2.25 (1.07) |
| Electronic device use for gaming (hour/day), mean (SD) | 1.14 (1.06) | 2.27 (1.13) |
| No. of Classes | AIC | BIC | Adjusted BIC | Smallest Class, % | Entropy |
|---|---|---|---|---|---|
| 1 | 10,241.3 | 10,298.5 | 10,263.5 | - | - |
| 2 | 9706.1 | 9825.7 | 9752.6 | 41.7% | 0.613 |
| 3 | 9535.7 | 9717.6 | 9606.4 | 5.5% | 0.654 |
| 4 | 9465.0 | 9709.3 | 9560.0 | 5.9% | 0.633 |
| 5 | 9430.8 | 9737.6 | 9550.1 | 3.7% | 0.690 |
| Family Hardship Indicators | Class 1 | Class 2 | Class 3 | Class 4 |
|---|---|---|---|---|
| Low hardship | Poverty | Poor health | Low income | |
| (n = 611, 45.7%) | (n = 187, 14.0%) | (n = 79, 5.9%) | (n = 461, 34.5%) | |
| Having chronic disease (mother) | 0.016 | 0.044 | 0.151 | 0.008 |
| Having chronic disease (father) | 0.039 | 0.079 | 0.053 | 0.048 |
| Having chronic disease (child) | 0.008 | 0.083 | 0.846 | 0.018 |
| Having special education needs (child) | 0.086 | 0.172 | 0.833 | 0.073 |
| Having mental disorder (father) | 0.006 | 0.013 | 0.056 | 0.003 |
| Having mental disorder (mother) | 0.027 | 0.115 | 0.136 | 0.010 |
| Below upper secondary education (mother) | 0.000 | 0.649 | 0.157 | 0.695 |
| Below upper secondary education (father) | 0.075 | 0.709 | 0.246 | 0.546 |
| Parental marital status: single/divorced/separated/widowed | 0.042 | 0.509 | 0.031 | 0.062 |
| Monthly household income: HKD 19,999 or below | 0.256 | 0.959 | 0.356 | 0.572 |
| Receiving government welfare assistance | 0.000 | 0.347 | 0.000 | 0.005 |
| Class 2: Poverty (vs. Low Hardship) | Class 3: Poor Health (vs. Low Hardship) | Class 4: Low Income (vs. Low Hardship) | ||||
|---|---|---|---|---|---|---|
| OR (95%CI) | p-Value | OR (95%CI) | p-Value | OR (95%CI) | p-Value | |
| Severe physical maltreatment a | 1.49 (0.91, 2.45) | 0.113 | 0.73 (0.30, 1.75) | 0.474 | 0.86 (0.56, 1.32) | 0.480 |
| Physical maltreatment a | 1.19 (0.77, 1.83) | 0.438 | 1.32 (0.73, 2.38) | 0.359 | 0.97 (0.69, 1.35) | 0.837 |
| Corporal punishment a | 1.15 (0.81, 1.64) | 0.421 | 1.26 (0.75, 2.09) | 0.382 | 1.27 (0.98, 1.64) | 0.074 |
| Non-violent discipline a | 0.79 (0.52, 1.20) | 0.268 | 1.26 (0.64, 2.47) | 0.499 | 0.76 (0.56, 1.04) | 0.083 |
| Psychological aggression a | 1.09 (0.75, 1.59) | 0.661 | 1.99 (1.05, 3.78) | 0.035 | 0.76 (0.58, 0.998) | 0.048 |
| Neglect a | 1.73 (1.13, 2.67) | 0.013 | 1.25 (0.70, 2.25) | 0.454 | 0.77 (0.52, 1.15) | 0.206 |
| β (95%CI) | p-value | β (95%CI) | p-value | β (95%CI) | p-value | |
| Externalizing problems | 0.52 (0.01, 1.02) | 0.045 | 0.73 (0.01, 1.45) | 0.048 | −0.08 (−0.45, 0.30) | 0.694 |
| Internalizing problems | 0.59 (0.15, 1.03) | 0.008 | 0.54 (−0.09, 1.16) | 0.094 | −0.14 (−0.47, 0.18) | 0.391 |
| Parenting stress | 3.66 (1.50, 5.83) | 0.001 | 2.07 (−1.02, 5.17) | 0.189 | 1.90 (0.30, 3.50) | 0.020 |
| Physical wellbeing | −0.08 (−2.26, 2.10) | 0.945 | −1.20 (−4.32, 1.91) | 0.450 | 2.11 (0.49, 3.72) | 0.011 |
| Parent-child learning activities | −0.14 (−0.26, −0.03) | 0.012 | −0.07 (−0.23, 0.09) | 0.388 | −0.08 (−0.17, 0.00) | 0.050 |
| Parent-child recreational activities | −0.18 (−0.29, −0.07) | 0.001 | −0.06 (−0.21, 0.10) | 0.461 | −0.16 (−0.24, −0.08) | <0.001 |
| Sleep duration (hour/day) | 0.12 (−0.02, 0.27) | 0.102 | 0.19 (−0.01, 0.40) | 0.066 | 0.13 (0.02, 0.24) | 0.017 |
| Exercise duration (hour/day) | 0.07 (−0.09, 0.23) | 0.378 | −0.57 (−0.79, −0.35) | <0.001 | 0.04 (−0.08, 0.15) | 0.515 |
| Electronic device use for learning (hour/day) | −0.002 (−0.18, 0.17) | 0.979 | −0.004 (−0.25, 0.25) | 0.974 | −0.02 (−0.15, 0.11) | 0.713 |
| Electronic device use for gaming (hour/day) | 0.10 (−0.08, 0.29) | 0.267 | −0.04 (−0.30, 0.23) | 0.796 | 0.12 (−0.02, 0.26) | 0.085 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, R.S.; Tung, K.T.S.; Rao, N.; Chan, K.L.; Fu, K.-W.; Yam, J.C.; Tso, W.W.Y.; Wong, W.H.S.; Lum, T.Y.S.; Wong, I.C.K.; et al. Using Latent Class Analyses to Examine Health Disparities among Young Children in Socially Disadvantaged Families during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 7893. https://doi.org/10.3390/ijerph19137893
Wong RS, Tung KTS, Rao N, Chan KL, Fu K-W, Yam JC, Tso WWY, Wong WHS, Lum TYS, Wong ICK, et al. Using Latent Class Analyses to Examine Health Disparities among Young Children in Socially Disadvantaged Families during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(13):7893. https://doi.org/10.3390/ijerph19137893
Chicago/Turabian StyleWong, Rosa S., Keith T. S. Tung, Nirmala Rao, Ko Ling Chan, King-Wa Fu, Jason C. Yam, Winnie W. Y. Tso, Wilfred H. S. Wong, Terry Y. S. Lum, Ian C. K. Wong, and et al. 2022. "Using Latent Class Analyses to Examine Health Disparities among Young Children in Socially Disadvantaged Families during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 13: 7893. https://doi.org/10.3390/ijerph19137893