


Abstract
Background: Little is known about the relationship between workplace support and mental health and burnout among health care professionals (HCPs) during the COVID-19 pandemic. In this cohort study, we sought to evaluate the association between perceived level of (and changes to) workplace support and mental health and burnout among HCPs, and to identify what constitutes perceived effective workplace support.
Methods: Online surveys at baseline (July–September 2020) and follow-up 4 months later assessed the presence of generalized anxiety disorder (using the 7-item Generalized Anxiety Disorder scale [GAD-7]), clinical insomnia, major depressive disorder (using the 9-item Patient Health Questionnaire), burnout (emotional exhaustion and depersonalization) and mental well-being (using the Short Warwick-Edinburgh Mental Wellbeing Score). Both surveys assessed self-reported level of workplace support (single-item Likert scale). For baseline and follow-up, independently, we developed separate logistic regression models to evaluate the association of the level of workplace support (tricohotomized as unsupported, neither supported nor unsupported and supported) with mental health and burnout. We also developed linear regression models to evaluate the association between the change in perceived level of workplace support and the change in mental health scores from baseline and follow-up. We used thematic analyses on free-text entries of the baseline survey to evaluate what constitutes effective support.
Results: At baseline (n = 1422) and follow-up (n = 681), HCPs who felt supported had reduced risk of anxiety, depression, clinical insomnia, emotional exhaustion and depersonalization, compared with those who felt unsupported. Among those who responded to both surveys (n = 681), improved perceived level of workplace support over time was associated with significantly improved scores on measures of anxiety (adjusted β −0.13, 95% confidence interval [CI] −0.25 to −0.01), depression (adjusted β −0.17, 95% CI −0.29 to −0.04) and mental well-being (adjusted β 0.19, 95% CI 0.10 to 0.29), independent of baseline level of support. We identified 5 themes constituting effective workplace support, namely concern or understanding for welfare, information, tangible qualities of the workplace, leadership and peer support.
Interpretation: We found a significant association between perceived level of (and changes in) workplace support and mental health and burnout of HCPs, and identified potential themes that constitute perceived workplace support. Collectively, these findings can inform changes in guidance and national policies to improve mental health and burnout among HCPs. Trial registration: ClinicalTrials.gov, no. NCT04433260
The COVID-19 pandemic has posed serious risks to the mental health of health care professionals (HCPs), which, if not addressed, will affect staffing and service provision in the future.1,2 Their potential vulnerability to mental health issues could be explained by the unique challenges faced by them, including vicarious trauma,3 moral injury4–7 and increased risk of infection.8 Long working hours, discrimination for working in hospitals and workplace practices may also be contributing factors.9 Results of meta-analyses and other studies have attested to this considerable toll, with high reported prevalence of anxiety (26.1%),10 depression (24.0%)11 and burnout (49.4%)12 among HCPs during the pandemic. As such, high-quality research is needed to identify factors and strategies associated with improved mental health outcomes in HCPs.2
Workplace support is one potential strategy. Regarding previous viral outbreaks, Brooks and colleagues endorsed the critical role of managers or employers in ensuring clear communication, supportive environments, specialized training, and psychological support systems.13 Concerningly, a cross-sectional survey of HCPs in the United Kingdom, conducted during the first wave of the COVID-19 pandemic in the UK (data collected between Mar. 30, 2020, and May 5, 2020), found that most respondents perceived the support for their well-being to be inadequate.14 This study and other qualitative studies also highlight the perceived value of organizational support to the mental health of HCPs.14–19 Some cross-sectional quantitative studies support an association between workplace support and mental health among HCPs,20–24 but these studies are cross-sectional,20–25 small,21,25 offer a noncomprehensive assessment of mental health (neglecting issues such as burnout)20,22 or only focus on qualitative or quantitative aspects of support.15,16,20–25 Therefore, to inform national and global policy and workplace practices, robust, high-quality studies using comprehensive mental health assessments of mental health over time are needed.26
In the current study (part of the COVID-19 and Physical and Emotional Well-being of Healthcare Professionals [CoPEHCP] project),27 we sought to evaluate the relationship between perceived workplace support and mental health, including generalized anxiety disorder (GAD), clinical insomnia, major depressive disorder (MDD), burnout (i.e., emotional exhaustion and depersonalization), and well-being during the pandemic. We also sought to evaluate whether change in perceived level of workplace support was associated with improved mental health and well-being over a 4-month period, and explore what workplace support HCPs want or have found helpful.
Methods
Study design and population
The protocol is published.27 The study involved multiple online surveys, distributed to HCPs based in and outside of the UK. We included people aged 18 years or older who self-identified as HCP staff. Recruitment was facilitated by health service employers who invited employees by an email that contained a link to the survey (SurveyMonkey). Participants were those who responded to that invite.
Participants gave electronic consent for the baseline survey and, at the end of the survey, they were asked if they consented to receiving follow-up surveys. Further consent was given at the follow-up survey.
Data collection
We distributed the baseline survey in July 2020, and it was available to complete until September 2020. In the UK, this corresponded to the first wave of COVID-19. The baseline survey gathered information such as age, gender, ethnicity, relationship status, educational attainment and current mental health and physical health diagnosis (a multiple-choice closed-ended item) (Appendix 1, available at www.cmajopen.ca/content/11/1/E191/suppl/DC1).
We assessed our primary predictor, workplace support, by asking, “Do you think you received adequate support directly from your supervisors/line managers/direct employers? (Mark on scale, with 1 as no support and 10 as full and professional support).” We converted responses into 3 categories, labelled as “felt unsupported,” (scores 1–3) “felt neither supported nor unsupported,” (scores 4–6) and “felt supported” (scores 7–10). Those who felt unsupported served as the reference group in cross-sectional analyses. A subsequent free-text item elicited qualitative data about what support they found most helpful or felt would be helpful.
We distributed the follow-up survey at the end of December 2020 (about 4 months later, during the second peak of the pandemic in the UK) to those who completed the baseline assessment. It was available to complete until mid-March 2021. The follow-up survey included the same mental health assessments and assessment of level of workplace support (excluding the free-text item). For transparency, owing to an error in survey coding, the support item at follow-up provided a score between 0 and 100 (as opposed to 1–10, as in the baseline survey), which we similarly collapsed into a 3-level response (0–30, 31–60 and 61–100 being labelled as “felt unsupported,” “felt neither supported nor unsupported” and “felt supported,” respectively).
Outcomes
At each survey, we assessed for the presence of GAD (using the 7-item Generalized Anxiety Disorder scale [GAD-7]),28 clinical insomnia (using the 7-item Insomnia Severity Index [ISI]),29 MDD (using the 9-item Patient Health Questionnaire [PHQ-9]),30 emotional exhaustion and depersonalization (using single respective 7-point scale items),31 and mental well-being (Short Warwick-Edinburgh Mental Wellbeing Score [SWEMWBS]).32
A score of 10 or higher on the GAD-7 and PHQ-9 indicates the presence of GAD and MDD, respectively.28,30 A score of 15 or higher on the ISI indicates insomnia.29 A score of 4 or higher indicates burnout characterized by emotional exhaustion or depersonalization, for their respective scales.31 A score of 21 or higher on the SWEMWBS indicates average-to-high well-being.32
Statistical analysis
We conducted statistical analyses using STATA version 17.0. We compared baseline characteristics of participants who completed the baseline survey only with those who also completed the follow-up survey.
At each survey time point, we separately assessed for the cross-sectional association between the perceived level of support and the presence of GAD, clinical insomnia, MDD, medium-to-high mental well-being, emotional exhaustion, and depersonalization, according to validated cut-offs. We developed logistic regression models to estimate crude and adjusted odds ratios (ORs) with 95% confidence intervals (CIs) and global p values for trends across levels of support (compared with the reference category of feeling unsupported), adjusted for prespecified risk factors (age, gender, time since COVID-19 peak in the participant’s region, highest level of education, relationship status, number of people in household, currently diagnosed mental health condition [yes or no], currently diagnosed physical health condition [yes or no] and HCP role, including physicians, [reference group] health care assistants, nurses and midwives, and allied health professionals).
For the cohort analysis of those who responded to both baseline and follow-up surveys, we calculated the change in mental health and burnout by subtracting the baseline score from the follow-up score on the respective measures. We calculated changes in perceived workplace support by subtracting the baseline score from the follow-up score (follow-up score was rescaled by dividing by 10). We conducted separate unadjusted and adjusted (adjusted for collected risk factors and for perceived level of support at baseline) linear regression models to assess the association between the change in perceived level of workplace support and change in mental health and burnout scores over time.
Thematic analysis
Four authors (J.G., I.S., I.M., C.K.) analyzed the free-text item using thematic analysis.33 They analyzed responses inductively, meaning that no preselected themes were used to start with, and the analysis was data-driven. We collated the raw data into an Excel table and the 4 analysts familiarized themselves with the data. Initial codes were generated for each data entry, which were shared among the researchers before refining them into a coding dictionary. They excluded any data entries with limited detail on support type. They reviewed and amalgamated data entries and refined codes into key themes (based on salience and apparent importance to the participants) and subthemes to best describe the data.
Ethics approval
The study was approved by the Cambridge East Research Ethics Committee (20/EE/0166) and was registered in ClinicalTrials.gov (NCT04433260).
Results
Overall, 1574 HCPs completed the baseline assessment and, among them, 744 (47.3%) responded to the follow-up survey (Figure 1, Table 1).

Study flowchart. Note: HCP = health care professional.
Characteristics of health care professionals at baseline and follow-up
Most of the 1574 HCPs at baseline were based in the UK (n = 1321, 83.9%). Of those based outside the UK (n = 253, 16.1%), most were based in North America (37.2%) followed by Asia (34.4%) and Europe (17.4%). Reporting the non-UK country where they were based was optional; of the 202 respondents who reported this, 70 (34.7%) were in the United States, followed by 63 (31.2%) from India. A total of 30 different countries were represented among participants based outside the UK.
The characteristics of respondents who completed only the baseline survey (n = 830) were mostly similar to those who responded to both surveys (n = 744), except for significant differences in ethnicity, gender and number of people living in the household (Table 1). The baseline-only group had relatively higher proportions of participants of Asian ethnicity, male gender and larger households (Table 1).
Mental health outcomes were not significantly different between baseline-only respondents and those who responded to both surveys (Table 1). At baseline (n = 1574, specific number varies for each outcome), 284 (19.9%) of 1429 HCPs met the criteria for GAD, 228 (16.1%) of 1418 HCPs for clinical insomnia, 354 (24.7%) of 1434 HCPs for MDD, 580 (41.9%) of 1386 HCPs for emotional exhaustion, and 186 (13.4%) of 1386 HCPs for depersonalization. At follow-up (n = 744, specific number varies for each outcome), we observed increased or sustained outcome rates for GAD (n = 142 [19.9%] of 713), clinical insomnia (n = 125 [17.6%] of 712), MDD (n = 182 [25.5%] of 713), emotional exhaustion (n = 282 [39.8%] of 708) and depersonalization (n = 83 [11.7%] of 708).
Perceived level of support at baseline and follow-up
Overall, 1422 participants provided valid data on perceived level of support at baseline and, of these, 681 provided similar data at follow-up. As per our predefined 3-level categories measuring perceived support, 689 (48.5%) respondents reported feeling supported at baseline, with similar observations made in the follow-up sample (n = 360, 52.9%); 312 (21.9%) participants in the baseline sample and 167 (24.5%) in the follow-up sample felt unsupported (Appendix 2, Supplementary Table 1 and Supplementary Figures 1–3, available at www.cmajopen.ca/content/11/1/E191/suppl/DC1, for distribution of responses for both surveys and for the change in perceived support from baseline to follow-up).

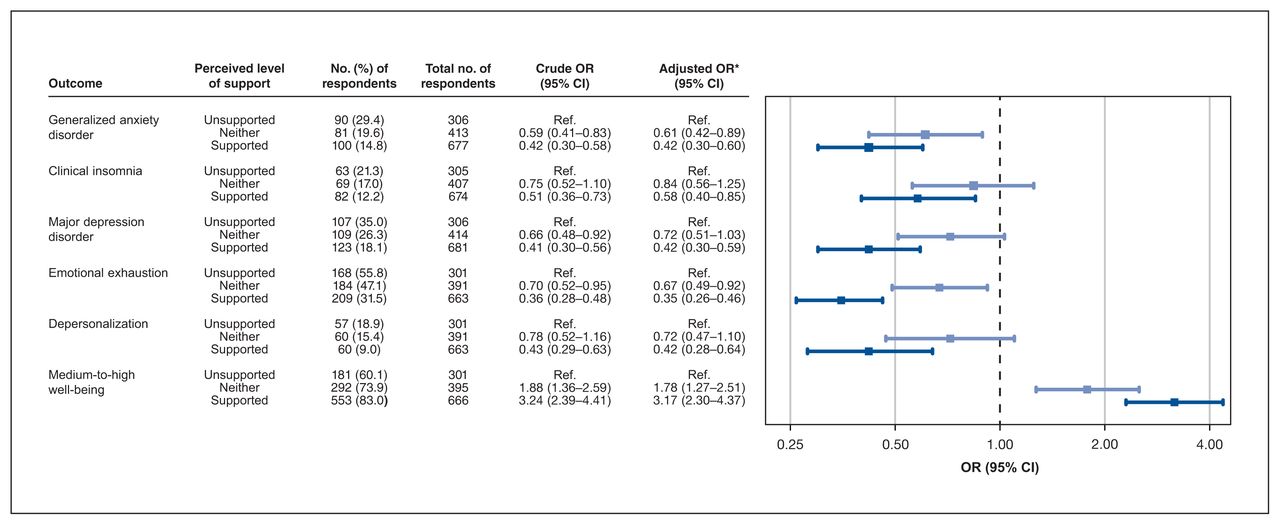
Forest plot of the odds ratios (ORs) (risk) of mental health and burnout by perceived level of workplace support among health care professionals at baseline (n = 1422). Note: CI = confidence interval, Ref. = reference category. *Adjusted for age, gender, time elapsed since COVID-19 peak in subject’s region, highest level of education, relationship status, number living in household, current mental health diagnosis, current physical health diagnosis and role.

Forest plot of the odds ratio (ORs) (risk) of mental health and burnout by perceived level of workplace support among health care professionals at follow-up (n = 681). Note: CI = confidence interval, Ref. = reference category. *Adjusted for age, gender, time elapsed since COVID-19 peak in subject’s region, highest level of education, relationship status, number living in household, current mental health diagnosis, current physical health diagnosis and role.
Of the 1422 participants reporting level of support at baseline, a higher proportion of those who completed only the baseline survey (n = 741) reported feeling unsupported at baseline compared with participants who continued to follow-up (n = 681) (24.3% v. 19.4%), and a lower proportion of baseline-only participants reported feeling supported at baseline, compared with participants who continued to follow-up (45.1% v. 52.1%) (p < 0.05).
Relationship between support and mental health and burnout
At baseline, there was a statistically significant relationship between level of support and each mental health and burnout outcome (p for trends were all < 0.001, except for clinical insomnia, p = 0.013) (Figure 2). Compared with respondents who felt unsupported, those who felt supported were significantly less likely to meet the criteria for GAD (adjusted OR 0.42, 95% CI 0.30–0.60), clinical insomnia (adjusted OR 0.58, 95% CI 0.40–0.85), MDD (adjusted OR 0.42, 95% CI 0.30–0.59), emotional exhaustion (adjusted OR 0.35, 95% CI 0.26–0.46) and depersonalization (adjusted OR 0.42, 95% CI 0.28–0.64), and more likely to have medium-to-high mental well-being (adjusted OR 3.17, 95% CI 2.30–4.37).
Based on 681 follow-up responses (Figure 3, median 4.9 mo after baseline survey), respondents who felt supported were significantly less likely to have clinical insomnia (adjusted OR 0.46, 95% CI 0.27–0.79), MDD (adjusted OR 0.44, 95% CI 0.28–0.69), emotional exhaustion (adjusted OR 0.45, 95% CI 0.30–0.68) and depersonalization (adjusted OR 0.31, 95% CI 0.19–0.50), and more likely to have medium-to-high mental well-being (adjusted OR 2.63, 95% CI 1.69–4.09), than those who felt unsupported. We observed a 39% reduction in the odds of meeting the criteria for GAD (adjusted OR 0.61, 95% CI 0.37–1.01) when comparing HCPs who felt supported with those who felt unsupported.
Change in level of workplace support and improvement in mental health outcomes over time
Among respondents with both baseline and follow-up data (n = 681), we observed consistent associations between the change in perceived level of support and the change in scores on some, but not all, mental health outcomes (Table 2). Separate adjusted linear regression models showed that a whole unit increase in change in perceived level of support (i.e., an increase of 1 on a scale ranging from −9.9 to 10.0) was inversely associated with a change in GAD-7 (β −0.13, 95% CI −0.25 to −0.01) and PHQ-9 scores (β −0.17, 95% CI −0.29 to −0.04), and positively associated with a change in SWEMWBS scores (β 0.19, 95% CI 0.10 to 0.29). We did not observe any significant associations between change in perceived level of support and the change in ISI (p = 0.067) or emotional exhaustion and depersonalization scores (p = 0.139).
Linear regressions for the association between change in perceived level of support and change in mental health, burnout and well-being scores among health care professionals from baseline to follow-up
What constitutes effective support?
We included 860 free-text entries in the thematic analysis of what qualities or aspects of workplace support are perceived as most helpful. We identified 5 overarching themes, namely concern or recognition regarding welfare, information, tangible qualities of the workplace, leadership and peer support (Table 3).
Workplace support themes
Interpretation
We found that, during the pandemic, HCPs who felt supported at baseline (v. those who felt unsupported) had a significantly lower risk of GAD, clinical insomnia, MDD, emotional exhaustion, depersonalization and low mental well-being. We also observed this trend at follow-up 4 months after baseline, showing the consistency and reliability of these findings. Improvement in perceived support was significantly associated with improved GAD, MDD and well-being scores (independent of baseline perceived level of support), but not for insomnia or burnout. Our qualitative results illustrated what qualities of workplace support were perceived to be helpful during the pandemic, which can inform the design of intervention studies to establish a causal relationship between workplace support and mental health.
This study builds on and validates previous cross-sectional studies that have shown associations between workplace support and mental health outcomes in HCPs during the COVID-19 pandemic20–22 and previous outbreaks.34 A small cohort study in routine work environment showed that level of coworker and managerial support was inversely associated with general mental distress.35 Our study builds on this, as we observed strong associations between changes in workplace support and changes in mental health and well-being scores over time. Either improved or diminished levels of workplace support could be driving this association.
Most policy and guidance suggests that improving workplace support could benefit general mental health, and our findings support this regarding depression, anxiety, and well-being among HCPs.36,37 Although we observed a trend for reduced insomnia and burnout scores with improved perceived support over time, these associations were nonsignificant, which highlights the relevance of changes in workplace support to distinct mental health issues. Workplace factors not accounted for in this analysis (e.g., long working hours) could be more likely to affect burnout and insomnia.
Our qualitative findings are consistent with previous guidance for health care systems. The World Health Organization has advised how HCPs and their managers can promote their psychosocial well-being during the COVID-19 pandemic, including care of basic needs, up-to-date staff communication, buddy systems, psychological first aid and staff access to mental health support services.36 Our findings also mirror previous reviews that showed that clear communication through horizontal (peer-to-peer) and vertical (manager-to-employee) networks can buffer against the psychological impact of disease outbreaks and epidemics.26 Many participants reported that daily updates were useful as a means of support. In the UK, Enabling Quality Improvement in Practice (https://equiptowerhamlets.nhs.uk/) encourages embedding daily huddles into work practice for safety and improvement; we suggest these daily huddles include a mental well-being check-in element.
Limitations
We collected data between July and December 2020, at the trough and second peak of the COVID-19 pandemic in the UK, respectively. Although the pandemic is ongoing, our findings remain relevant owing to the fluctuating levels of cases and persistent mental health burden for HCPs. Although we accounted for the time since the COVID-19 peak in participants’ regions, non-UK participants may have experienced different public health policies, which may be a confounder. Our survey was conducted online, which could potentially create selection bias. Respondents may not be representative of all HCPs (e.g., female and white HCPs were more likely to respond at follow-up). However, our observed rates of mental health outcomes were similar to other large surveys in the UK’s general population,38 and we did not observe significant differences on mental health measures between baseline-only and follow-up participants. Therefore, we anticipate our findings to be generalizable to the health care workforce, regardless of possible self-selection bias. Bidirectionality remains relevant, despite reporting data at 2 time points; HCPs with lower mental health scores may perceive workplace support to be lower because their needs are greater. Related to this, our measure of perceived workplace support is not validated. As such, it is uncertain whether this measure objectively assesses changes in workplace support, and what specific aspects of support are involved. Researchers can draw on these findings to improve the design of studies evaluating the associations between workplace support and mental health over time. Finally, most free-text responses were generated using a double-barrelled question asking what support was useful and what was desired. This does not invalidate the themes, but we were unable to concretely distinguish between what support was helpful and what was lacking.
Conclusion
We found consistent associations between perceived level of workplace support and the mental health and well-being of HCPs during the COVID-19 pandemic. Improvement in the level of perceived workplace support was associated with improved anxiety, depression and well-being scores over time but not insomnia or burnout scores. Further studies are required to understand the workplace factors associated with insomnia and burnout among HCPs during the pandemic, to understand the causal relationship between perceived workplace support and mental health among HCPs and to verify whether improved or diminished workplace support drives the association between workplace support and changes in mental health. Our findings could inform important changes in guidance and national policies targeted at improving mental well-being among HCPs during current and future pandemics.
Acknowledgements
The authors acknowledge the extensive support received from the Barts Education Academy and William Harvey Research Institute for sharing some of their resources needed to conduct this study. In particular, they wish to acknowledge the excellent contribution of Ade Alele and Amrita Ahluwalia from William Harvey Research Institute, and Julekha Khanam from Barts Health NHS Trust.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
CoPE-HCP clinical investigators: Ashish Kotecha, Royal Devon and Exeter Hospital, Exeter, Devon, UK; Abhishek Kumar, Wrightington, Wigan and Leigh NHS Foundation Trust, UK; Azara Janmohamed, St. George’s University Hospitals NHS Foundation Trust, London, UK; Satheesh Nair, Glan Clwyd Hospital, Betsi Cadwaladr University Health Board, Wales, UK
Contributors: Imrana Siddiqui, Jaya Gupta, Sher Ng, Carmela Maniero, Sotiris Antoniou, Rehan Khan, Vikas Kapil, Mohammed Khanji and Ajay Gupta conceived and designed the study. George Collett, Thomas Godec and Ajay Gupta organized and managed the data. Imrana Siddiqui, Jaya Gupta, George Collett, Iris McIntosh, Christina Komodromos, Thomas Godec and Ajay Gupta contributed to analysis and interpretation. Imrana Siddiqui, Jaya Gupta, George Collett, Iris McIntosh, Christina Komodromos, Thomas Godec and Ajay Gupta drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work. Imrana Siddiqui and Jaya Gupta contributed equally to this manuscript.
Funding: This study was funded in part by Barts Charity. The funders had no role in the study design, data collection, data analysis, data interpretation or writing of the report.
Data sharing: Anonymized data, data dictionary and survey materials will be made available upon request. Study protocol is available at https://doi.org/10.3389/fpsyg.2021.616280.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/1/E191/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use) and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.