
Development and Validation of a Multimodal-Based Prognosis and Intervention Prediction Model for COVID-19 Patients in a Multicenter Cohort

 , , and
, , and
Abstract
:1. Introduction
2. Related Works
3. Materials and Methods
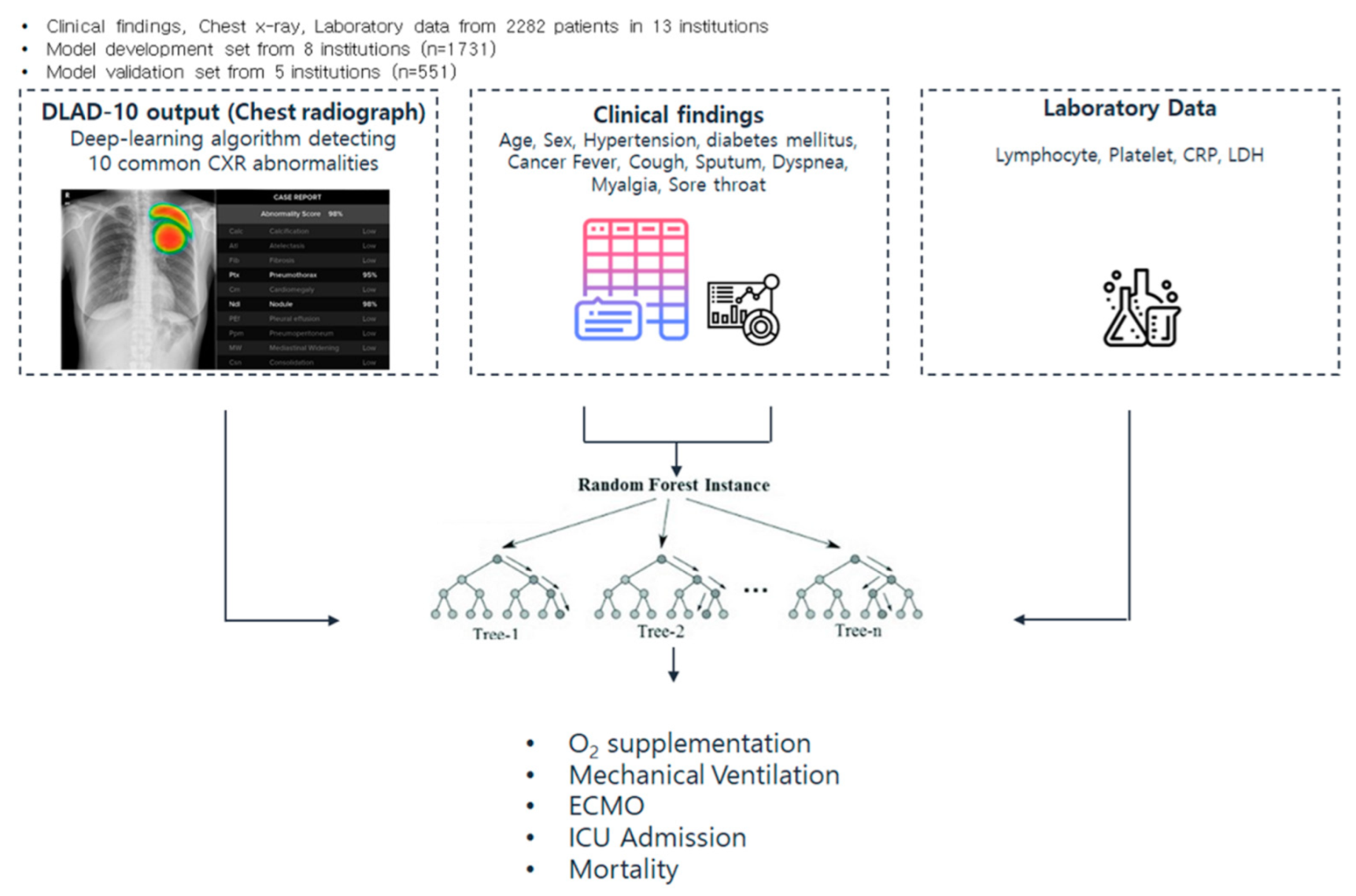
3.1. Study Population
3.2. Data Collection and Study Definition
3.3. Dataset Partitioning for Multicenter Validation
3.4. Image Feature Extraction from CXR
3.5. Prognosis Prediction Model Development
3.6. Statistical Analysis
4. Results
4.1. Patient Characteristics
4.2. Performance of Adverse Events Prediction Model
4.3. Feature Importance Analysis
5. Discussion
5.1. Benefits of Using a Feature Extractor (DLAD-10) with Clinically Defined Outputs
5.2. Benefits of Using the Two-Step Ensemble Approach with Imaging Extractor
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Algorithm for COVID-19 Triage and Referral: Patient Triage and Referral for Resource-Limited Settings during Community Transmission; WHO Regional Office for the Western Pacific: Manila, Philippines, 2020. [Google Scholar]
- Lancet. India under COVID-19 lockdown. Lancet 2020, 395, 1315. [Google Scholar] [CrossRef]
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol 2020, 215, 108427. [Google Scholar] [CrossRef] [PubMed]
- Farrell, N.M.; Hayes, B.D.; Linden, J.A. Critical medication shortages further dwindling hospital resources during COVID-19. Am. J. Emerg. Med. 2021, 40, 202–203. [Google Scholar] [CrossRef] [PubMed]
- Sen-Crowe, B.; Sutherland, M.; McKenney, M.; Elkbuli, A. A Closer Look Into Global Hospital Beds Capacity and Resource Shortages During the COVID-19 Pandemic. J. Surg. Res. 2021, 260, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Lerner, E.B.; Schwartz, R.B.; Coule, P.L.; Weinstein, E.; Cone, D.; Hunt, R.C.; Sasser, S.M.; Liu, J.M.; Nudell, N.; Wedmore, I.S.; et al. Mass Casualty Triage: An Evaluation of the Data and Development of a Proposed National Guideline. Disaster Med. Public Health Prep. 2008, 2, S25–S34. [Google Scholar] [CrossRef] [PubMed]
- Schwab, P.; Schütte, A.D.; Dietz, B.; Bauer, S. Clinical Predictive Models for COVID-19: Systematic Study. J. Med. Internet Res. 2020, 22, e21439. [Google Scholar] [CrossRef] [PubMed]
- Wynants, L.; Van Calster, B.; Collins, G.S.; Riley, R.D.; Heinze, G.; Schuit, E.; Bonten, M.M.J.; Dahly, D.L.; Damen, J.A.; Debray, T.P.A.; et al. Prediction models for diagnosis and prognosis of COVID-19: Systematic review and critical appraisal. BMJ 2020, 369, m1328. [Google Scholar] [CrossRef] [Green Version]
- Pan, P.; Li, Y.; Xiao, Y.; Han, B.; Su, L.; Su, M.; Li, Y.; Zhang, S.; Jiang, D.; Chen, X.; et al. Prognostic Assessment of COVID-19 in the Intensive Care Unit by Machine Learning Methods: Model Development and Validation. J. Med. Internet Res. 2020, 22, e23128. [Google Scholar] [CrossRef]
- Knaus, W.A.; Wagner, D.P.; Draper, E.A.; Zimmerman, J.E.; Bergner, M.; Bastos, P.G.; Sirio, C.A.; Murphy, D.J.; Lotring, T.; Damiano, A.; et al. The APACHE III prognostic system: Risk prediction of hospital mortality for critically III hospitalized adults. Chest 1991, 100, 1619–1636. [Google Scholar] [CrossRef] [Green Version]
- Monjur, O.; Bin Preo, R.; Bin Shams, A.; Raihan, M.S.; Fairoz, F. COVID-19 Prognosis and Mortality Risk Predictions from Symptoms: A Cloud-Based Smartphone Application. BioMed 2021, 1, 11. [Google Scholar] [CrossRef]
- Alkhodari, M.; Khandoker, A.H. Detection of COVID-19 in smartphone-based breathing recordings: A pre-screening deep learning tool. PLoS ONE 2022, 17, e0262448. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.-J.; Martin, I.B.K.; et al. The Role of Chest Imaging in Patient Management during the COVID-19 Pandemic: A Multinational Consensus Statement from the Fleischner Society. Radiology 2020, 296, 172–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, H.Y.F.; Lam, H.Y.S.; Fong, A.H.-T.; Leung, S.T.; Chin, T.W.-Y.; Lo, C.S.Y.; Lui, M.M.-S.; Lee, J.C.Y.; Chiu, K.W.-H.; Chung, T.W.-H.; et al. Frequency and Distribution of Chest Radiographic Findings in Patients Positive for COVID-19. Radiology 2020, 296, E72–E78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cozzi, A.; Schiaffino, S.; Arpaia, F.; Della Pepa, G.; Tritella, S.; Bertolotti, P.; Menicagli, L.; Monaco, C.G.; Carbonaro, L.A.; Spairani, R.; et al. Chest x-ray in the COVID-19 pandemic: Radiologists’ real-world reader performance. Eur. J. Radiol. 2020, 132, 109272. [Google Scholar] [CrossRef] [PubMed]
- Murphy, K.; Smits, H.; Knoops, A.J.G.; Korst, M.B.J.M.; Samson, T.; Scholten, E.T.; Schalekamp, S.; Schaefer-Prokop, C.M.; Philipsen, R.H.H.M.; Meijers, A.; et al. COVID-19 on Chest Radiographs: A Multireader Evaluation of an Artificial Intelligence System. Radiology 2020, 296, E166–E172. [Google Scholar] [CrossRef]
- Barbieri, D.; Giuliani, E.; Del Prete, A.; Losi, A.; Villani, M.; Barbieri, A. How Artificial Intelligence and New Technologies Can Help the Management of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 7648. [Google Scholar] [CrossRef]
- Jiao, Z.; Choi, J.W.; Halsey, K.; Tran, T.M.L.; Hsieh, B.; Wang, D.; Eweje, F.; Wang, R.; Chang, K.; Wu, J.; et al. Prognostication of patients with COVID-19 using artificial intelligence based on chest x-rays and clinical data: A retrospective study. Lancet Digit. Health 2021, 3, e286–e294. [Google Scholar] [CrossRef]
- Toussie, D.; Voutsinas, N.; Finkelstein, M.; Cedillo, M.A.; Manna, S.; Maron, S.Z.; Jacobi, A.; Chung, M.; Bernheim, A.; Eber, C.; et al. Clinical and Chest Radiography Features Determine Patient Outcomes in Young and Middle-aged Adults with COVID-19. Radiology 2020, 297, E197–E206. [Google Scholar] [CrossRef]
- Zargari Khuzani, A.; Heidari, M.; Shariati, S.A. COVID-Classifier: An automated machine learning model to assist in the diagnosis of COVID-19 infection in chest X-ray images. Sci. Rep. 2021, 11, 9887. [Google Scholar] [CrossRef]
- Gong, K.; Wu, D.; Arru, C.D.; Homayounieh, F.; Neumark, N.; Guan, J.; Buch, V.; Kim, K.; Bizzo, B.C.; Ren, H.; et al. A multi-center study of COVID-19 patient prognosis using deep learning-based CT image analysis and electronic health records. Eur. J. Radiol. 2021, 139, 109583. [Google Scholar] [CrossRef]
- Kim, H.W.; Capaccione, K.M.; Li, G.; Luk, L.; Widemon, R.S.; Rahman, O.; Beylergil, V.; Mitchell, R.; D’Souza, B.M.; Leb, J.S.; et al. The role of initial chest X-ray in triaging patients with suspected COVID-19 during the pandemic. Emerg. Radiol. 2020, 27, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Chau, T.-N.; Lee, P.-O.; Choi, K.-W.; Lee, C.-M.; Ma, K.-F.; Tsang, T.-Y.; Tso, Y.-K.; Chiu, M.-C.; Tong, W.-L.; Yu, W.-C.; et al. Value of initial chest radiographs for predicting clinical outcomes in patients with severe acute respiratory syndrome. Am. J. Med. 2004, 117, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, S.H.; Ham, S.-Y.; Da Nam, B.; Chae, K.J.; Lee, D.; Yoo, J.Y.; Bak, S.H.; Kim, J.Y.; Kim, K.B.; Jung, J.I.; et al. Establishment of a Nationwide Korean Imaging Cohort of Coronavirus Disease 2019. J. Korean Med. Sci. 2020, 35, e413. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Chen, S.-M.; Cocea, M. Subclass-based semi-random data partitioning for improving sample representativeness. Inf. Sci. 2018, 478, 208–221. [Google Scholar] [CrossRef]
- Nam, J.G.; Kim, M.; Park, J.; Hwang, E.J.; Lee, J.H.; Hong, J.H.; Goo, J.M.; Park, C.M. Development and validation of a deep learning algorithm detecting 10 common abnormalities on chest radiographs. Eur. Respir. J. 2020, 57, 2003061. [Google Scholar] [CrossRef]
- Ishwaran, H.; Lauer, M.S.; Blackstone, E.H.; Lu, M.; Kogalur, U.B. RandomForestSRC: Random Survival Forests Vignette. 2021. Available online: http://randomforestsrc.org/articles/survival.html (accessed on 1 January 2022).
- Han, H.; Guo, X.; Yu, H. Variable selection using mean decrease accuracy and mean decrease gini based on random forest. In Proceedings of the 2016 7th IEEE International Conference on Software Engineering and Service Science (ICSESS), Beijing, China, 26–28 August 2016. [Google Scholar]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- Li, M.; Chapman, G.B. Medical Decision Making. In The Wiley Encyclopedia of Health Psychology; Wiley Online Library, 2020; pp. 347–353. [Google Scholar]
- Viner, R.M.; Ward, J.L.; Hudson, L.D.; Ashe, M.; Patel, S.V.; Hargreaves, D.; Whittaker, E. Systematic review of reviews of symptoms and signs of COVID-19 in children and adolescents. Arch. Dis. Child 2020, 106, 802–807. [Google Scholar] [CrossRef]
- Felsenstein, S.; Herbert, J.A.; McNamara, P.S.; Hedrich, C.M. COVID-19: Immunology and treatment options. Clin. Immunol. 2020, 215, 108448. [Google Scholar] [CrossRef]
- Shams, A.B.; Raihan, M.M.S.; Khan, M.M.U.; Preo, R.B.; Monjur, O. Telehealthcare and COVID-19: A Noninvasive & Low Cost Invasive, Scalable and Multimodal Real-Time Smartphone Application for Early Diagnosis of SARS-CoV-2 Infection. arXiv 2021, arXiv:2109.07846. [Google Scholar]
- Roberts, M.; Covnet, A.; Driggs, D.; Thorpe, M.; Gilbey, J.; Yeung, M.; Ursprung, S.; Aviles-Rivero, A.I.; Etmann, C.; McCague, C.; et al. Common pitfalls and recommendations for using machine learning to detect and prognosticate for COVID-19 using chest radiographs and CT scans. Nat. Mach. Intell. 2021, 3, 199–217. [Google Scholar] [CrossRef]
- López-Cabrera, J.D.; Orozco-Morales, R.; Portal-Díaz, J.A.; Lovelle-Enríquez, O.; Pérez-Díaz, M. Current limitations to identify COVID-19 using artificial intelligence with chest x-ray imaging (part ii). The shortcut learning problem. Health Technol. 2021, 11, 1331–1345. [Google Scholar] [CrossRef] [PubMed]
- Hwang, E.J.; Hong, J.H.; Lee, K.H.; Kim, J.I.; Nam, J.G.; Kim, D.S.; Choi, H.; Yoo, S.J.; Goo, J.M.; Park, C.M. Deep learning algorithm for surveillance of pneumothorax after lung biopsy: A multicenter diagnostic cohort study. Eur. Radiol. 2020, 30, 3660–3671. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.Y.; Kim, Y.J.; Choi, W.J.; Lee, G.P.; Choi, Y.R.; Jin, K.N.; Cho, Y.J. Performance of a deep-learning algorithm for referable thoracic abnormalities on chest radiographs: A multicenter study of a health screening cohort. PLoS ONE 2021, 16, e0246472. [Google Scholar] [CrossRef]
- Hwang, E.J.; Park, S.; Jin, K.-N.; Kim, J.I.; Choi, S.Y.; Lee, J.H.; Goo, J.M.; Aum, J.; Yim, J.-J.; Cohen, J.G.; et al. Development and Validation of a Deep Learning–Based Automated Detection Algorithm for Major Thoracic Diseases on Chest Radiographs. JAMA Netw. Open 2019, 2, e191095. [Google Scholar] [CrossRef] [Green Version]
- Yoo, H.; Lee, S.H.; Arru, C.D.; Khera, R.D.; Singh, R.; Siebert, S.; Kim, D.; Lee, Y.; Park, J.H.; Eom, H.J.; et al. AI-based improvement in lung cancer detection on chest radiographs: Results of a multi-reader study in NLST dataset. Eur. Radiol. 2021, 31, 9664–9674. [Google Scholar] [CrossRef]
- Lee, J.H.; Sun, H.Y.; Park, S.; Kim, H.; Hwang, E.J.; Goo, J.M.; Park, C.M. Performance of a Deep Learning Algorithm Compared with Radiologic Interpretation for Lung Cancer Detection on Chest Radiographs in a Health Screening Population. Radiology 2020, 297, 687–696. [Google Scholar] [CrossRef]
- Jang, S.B.; Lee, S.H.; Lee, D.E.; Park, S.-Y.; Kim, J.K.; Cho, J.W.; Cho, J.; Kim, K.B.; Park, B.; Park, J.; et al. Deep-learning algorithms for the interpretation of chest radiographs to aid in the triage of COVID-19 patients: A multicenter retrospective study. PLoS ONE 2020, 15, e0242759. [Google Scholar] [CrossRef]
- Hwang, E.J.; Kim, K.B.; Kim, J.Y.; Lim, J.-K.; Nam, J.G.; Choi, H.; Kim, H.; Yoon, S.H.; Goo, J.M.; Park, C.M. COVID-19 pneumonia on chest X-rays: Performance of a deep learning-based computer-aided detection system. PLoS ONE 2021, 16, e0252440. [Google Scholar] [CrossRef]
- Hwang, E.J.; Kim, H.; Yoon, S.H.; Goo, J.M.; Park, C.M. Implementation of a Deep Learning-Based Computer-Aided Detection System for the Interpretation of Chest Radiographs in Patients Suspected for COVID-19. Korean J. Radiol. 2020, 21, 1150. [Google Scholar] [CrossRef]
- Pesapane, F.; Volonté, C.; Codari, M.; Sardanelli, F. Artificial intelligence as a medical device in radiology: Ethical and regulatory issues in Europe and the United States. Insights Imaging 2018, 9, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Rousan, L.A.; Elobeid, E.; Karrar, M.; Khader, Y. Chest x-ray findings and temporal lung changes in patients with COVID-19 pneumonia. BMC Pulm. Med. 2020, 20, 245. [Google Scholar] [CrossRef] [PubMed]
- Schneider, J.; Agus, M. Reflections on the clinical acceptance of artificial intelligence. In Multiple Perspectives on Artificial Intelligence in Healthcare; Springer: Berlin/Heidelberg, Germany, 2021; pp. 103–114. [Google Scholar]
- Sun, Q.; Qiu, H.; Huang, M.; Yang, Y. Lower mortality of COVID-19 by early recognition and intervention: Experience from Jiangsu Province. Ann. Intensiv. Care 2020, 10, 33. [Google Scholar] [CrossRef] [Green Version]
- Goyal, D.K.; Mansab, F.; Iqbal, A.; Bhatti, S. Early intervention likely improves mortality in COVID-19 infection. Clin. Med. 2020, 20, 248–250. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall (N = 2282) | Development (N = 1731) | Validation (N = 551) | p Value |
|---|---|---|---|---|
| Age (years) | 52.8 ± 19.8 | 53.5 ± 20.4 | 50.6 ± 17.9 | 0.003 |
| Sex | 0.001 | |||
| Male | 1193 (52.3) | 872 (50.4) | 321 (58.3) | |
| Female | 1089 (47.7) | 859 (49.6) | 230 (41.7) | |
| Comorbidity | ||||
| Any comorbidities | 942 (41.3) | 718 (41.5) | 224 (40.7) | 0.732 |
| Hypertension | 690 (30.2) | 531 (30.7) | 159 (28.9) | 0.418 |
| Diabetes | 419 (18.4) | 319 (18.4) | 100 (18.1) | 0.883 |
| Cardiovascular disease | 135 (5.9) | 104 (6.0) | 31 (5.6) | 0.741 |
| History of cancer | 115 (5) | 81 (4.7) | 34 (6.2) | 0.163 |
| Symptoms | ||||
| Any symptoms | 1723 (75.5) | 1246 (72.0) | 477 (86.6) | <0.001 |
| Fever | 919 (40.3) | 634 (36.6) | 285 (51.7) | <0.001 |
| Cough | 995 (43.6) | 699 (40.4) | 296 (53.7) | <0.001 |
| Sputum | 653 (28.6) | 435 (25.1) | 218 (39.6) | <0.001 |
| Dyspnea | 404 (17.7) | 276 (15.9) | 128 (23.2) | <0.001 |
| Myalgia | 550 (24.1) | 344 (19.9) | 206 (37.4) | <0.001 |
| Sore throat | 396 (17.4) | 264 (15.3) | 132 (24.0) | <0.001 |
| Initial laboratory findings | ||||
| Lymphocyte count < 1000/μL * | 615 (29.7) | 459 (30.1) | 156 (28.6) | 0.503 |
| Platelet count < 150,000/μL * | 388 (18.7) | 284 (18.6) | 104 (19.0) | 0.826 |
| LDH > 300 U/L * | 1052 (55.2) | 603 (42.8) | 449 (90.5) | <0.001 |
| CRP > 50 mg/L * | 471 (23.1) | 345 (22.9) | 126 (23.5) | 0.783 |
| Clinical outcomes | ||||
| O2 supplementation | 408 (17.9) | 323 (18.7) | 85 (15.4) | 0.085 |
| Mechanical ventilation | 117 (5.1) | 84 (4.9) | 33 (6.0) | 0.292 |
| ECMO | 32 (1.4) | 21 (1.2) | 11 (2.0) | 0.173 |
| ICU admission | 124 (5.4) | 74 (4.3) | 50 (9.1) | <0.001 |
| In-hospital mortality | 106 (4.6) | 85 (4.9) | 21 (3.8) | 0.286 |
| Adverse Event Type | Area under the ROC Curve | |||
|---|---|---|---|---|
| Clinical Findings | Laboratory Data | CXR | Combined | |
| O2 supplementation | 0.753 (0.703–0.802) | 0.757 (0.708–0.806) | 0.701 (0.648–0.754) | 0.812 (0.772–0.852) |
| Mechanical ventilation | 0.735 (0.646–0.825) | 0.852 (0.780–0.923) | 0.807 (0.726–0.888) | 0.880 (0.810–0.950) |
| ECMO | 0.664 (0.489–0.839) | 0.794 (0.627–0.960) | 0.650 (0.525–0.776) | 0.745 (0.611–0.879) |
| ICU admission | 0.708 (0.633–0.782) | 0.711 (0.607–0.815) | 0.784 (0.711–0.856) | 0.838 (0.770–0.906) |
| In-hospital mortality | 0.762 (0.655–0.869) | 0.805 (0.700–0.910) | 0.838 (0.757–0.919) | 0.877 (0.792–0.962) |
| All adverse events | 0.742 (0.696–0.788) | 0.794 (0.745–0.843) | 0.770 (0.724–0.815) | 0.854 (0.820–0.889) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.H.; Ahn, J.S.; Chung, M.J.; Jeong, Y.J.; Kim, J.H.; Lim, J.K.; Kim, J.Y.; Kim, Y.J.; Lee, J.E.; Kim, E.Y. Development and Validation of a Multimodal-Based Prognosis and Intervention Prediction Model for COVID-19 Patients in a Multicenter Cohort. Sensors 2022, 22, 5007. https://doi.org/10.3390/s22135007
Lee JH, Ahn JS, Chung MJ, Jeong YJ, Kim JH, Lim JK, Kim JY, Kim YJ, Lee JE, Kim EY. Development and Validation of a Multimodal-Based Prognosis and Intervention Prediction Model for COVID-19 Patients in a Multicenter Cohort. Sensors. 2022; 22(13):5007. https://doi.org/10.3390/s22135007
Chicago/Turabian StyleLee, Jeong Hoon, Jong Seok Ahn, Myung Jin Chung, Yeon Joo Jeong, Jin Hwan Kim, Jae Kwang Lim, Jin Young Kim, Young Jae Kim, Jong Eun Lee, and Eun Young Kim. 2022. "Development and Validation of a Multimodal-Based Prognosis and Intervention Prediction Model for COVID-19 Patients in a Multicenter Cohort" Sensors 22, no. 13: 5007. https://doi.org/10.3390/s22135007