
Targeted COVID-19 Vaccination (TAV-COVID) Considering Limited Vaccination Capacities—An Agent-Based Modeling Evaluation

 , , , , ,
, , , , ,  , , , , , , , , , , and add
Show full author list
, , , , , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Agent-Based Simulation Model
2.2. Vaccine Effectiveness, Sterilizing Effect, and Vaccination Participation Rate
2.3. Vaccination Target Groups and Prioritization Strategies
2.4. Base-Case, Scenario and Sensitivity Analyses
2.5. Model Validation
2.6. Standing Policy and Expert Panel
3. Results
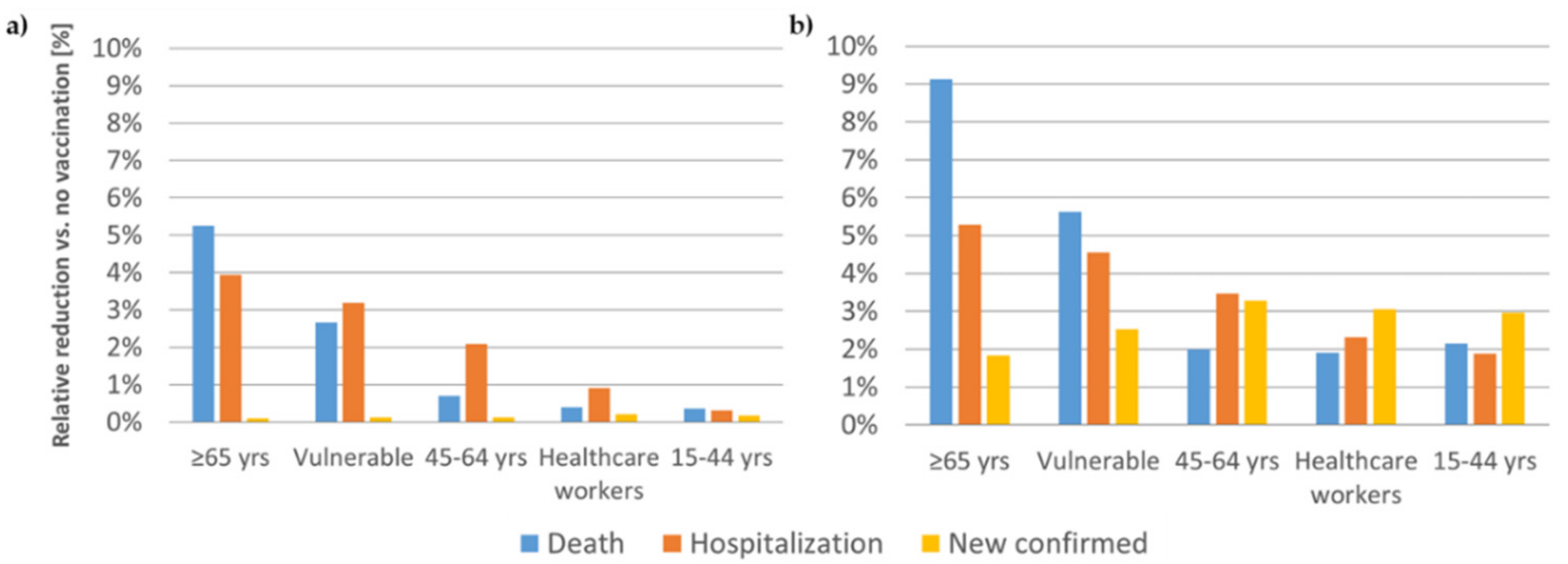
3.1. Vaccination of the First 200,000 Individuals
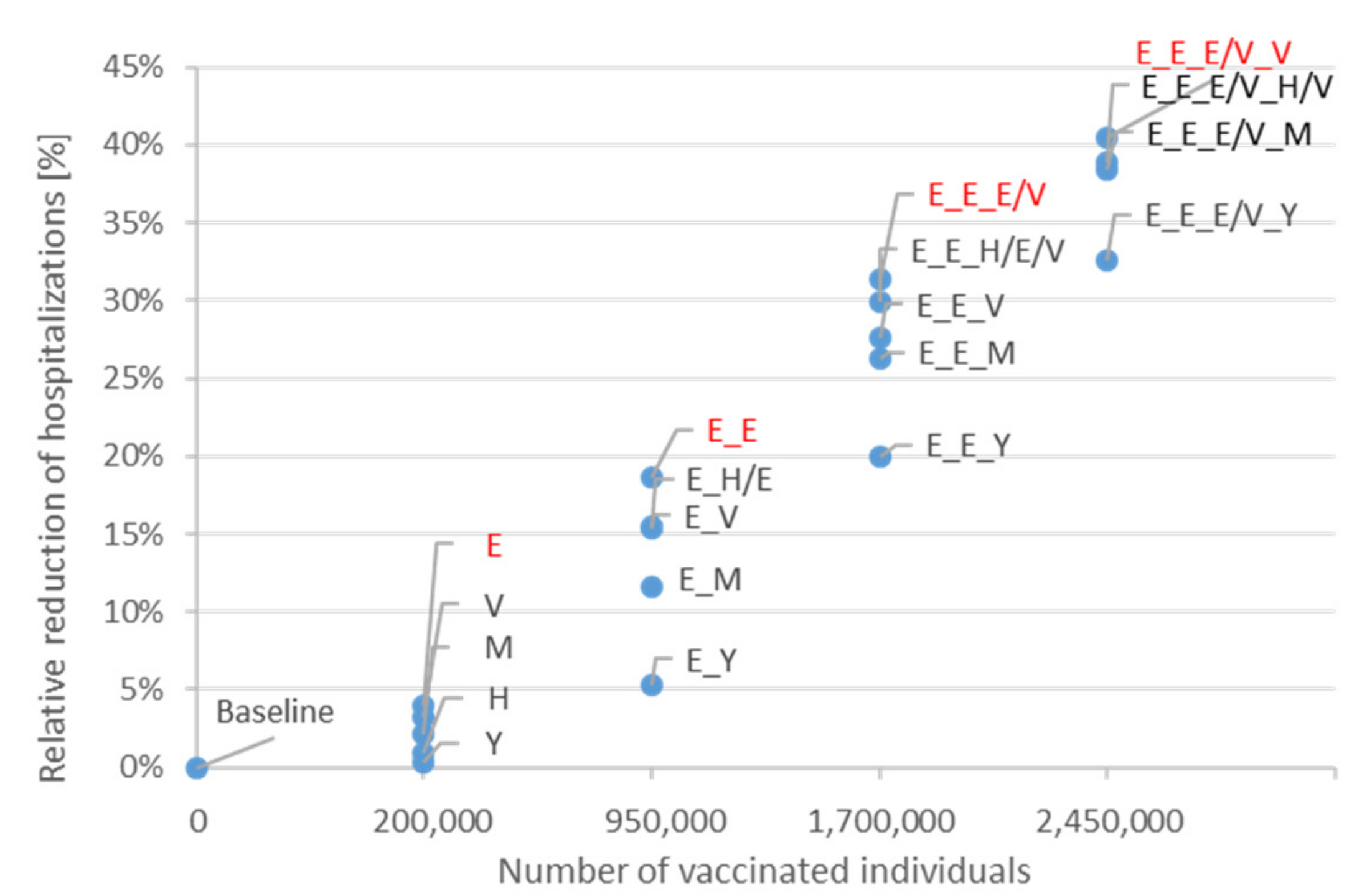
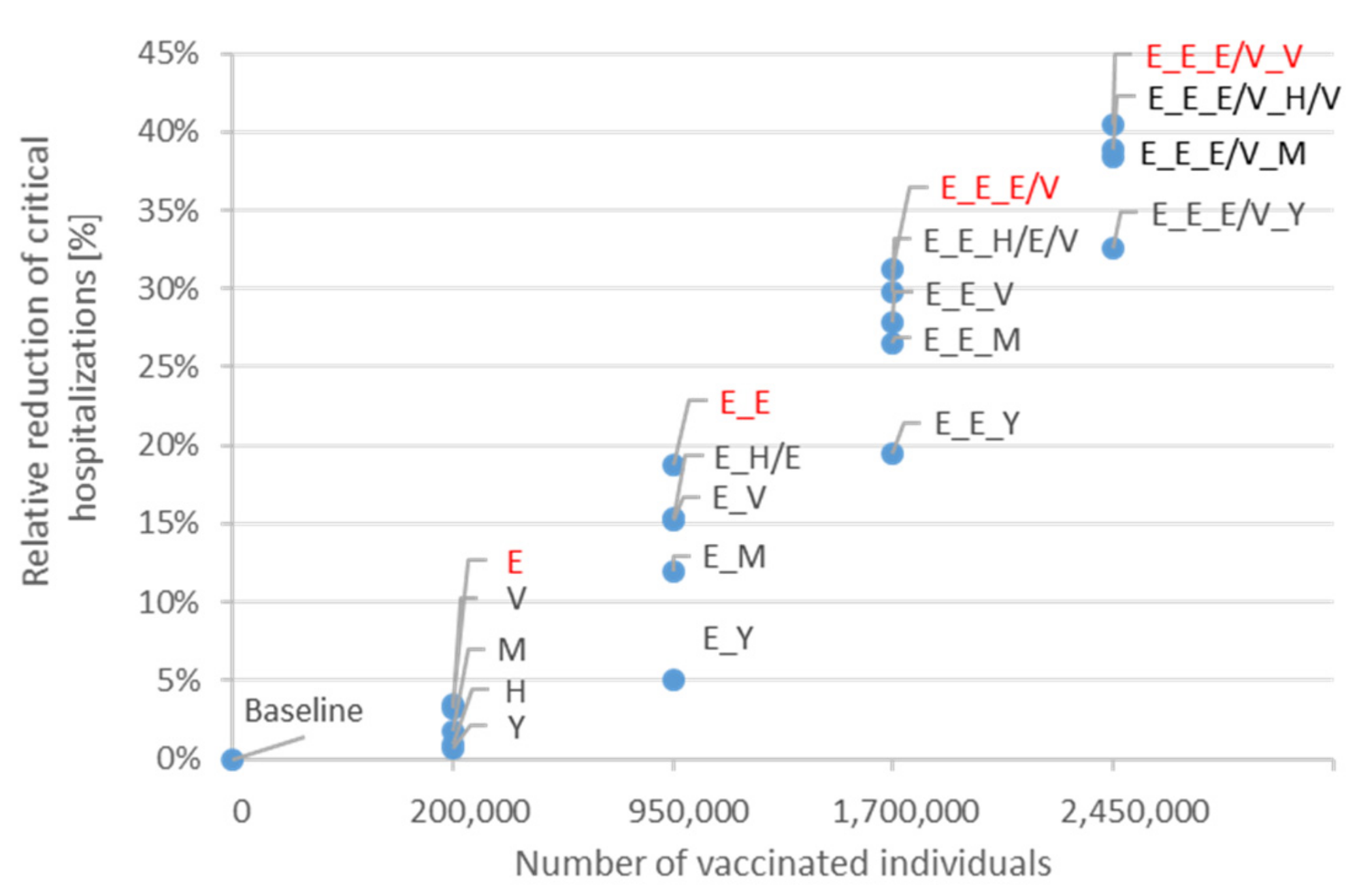
3.2. Vaccination of the First 2.45 Million Individuals
4. Discussion
4.1. Key Findings Base-Case Analysis and System-Relevant Target Group Considerations
4.2. Stepwise Optimization Vaccinating 2.5 Million Individuals and the Role of NPIs
4.3. Link to Health Policy Decision Making and Further Strengths of the Study
4.4. Limitations of the Study
4.5. Comparison of Results with Findings from Other Published Work
4.6. Ethical Considerations
4.7. Future Research Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of People (In Thousands) | Number of People Willing to be Vaccinated (In Thousands) | |
|---|---|---|
| Age 15–44 | 3400 | 2000 |
| Age 45–64 | 2700 | 2000 |
| Age 65+ | 1700 | 1500 |
| Vulnerable | 2900 | 2500 |
| Healthcare workers | 218 | 200 |
| Medical Staff in Hospitals and Physicians in Private Practice | DGKP/PFA/PA * | Non-Medical Staff in Hospitals (without DGKP/PFA/PA) ** | Total | |
|---|---|---|---|---|
| <29 | 31 | 25,971 | 3745 | 29,747 |
| 30–39 | 3867 | 39,748 | 5732 | 49,348 |
| 40–44 | 5953 | 18,628 | 2686 | 27,267 |
| 45–49 | 5415 | 21,165 | 3052 | 29,632 |
| 50–54 | 7625 | 23,155 | 3339 | 34,120 |
| 55–59 | 9517 | 18,085 | 2608 | 30,210 |
| >60 | 13,011 | 4508 | 650 | 18,169 |
| Total | 45,420 | 151,261 | 21,812 | 218,493 |
| Age-Dependent Prevalence (in %) of Risk Factors for COVID-19 Severity with Odds Ratios (OR) for Severe Symptoms | ||||||||
|---|---|---|---|---|---|---|---|---|
| Diabetes (OR: 2.04) | Chronic Kidney Disease (OR: 2.23) | Chronic Heart Disease (OR: 3.50) | Chronic Respiratory Disease (OR: 2.11) | Chronic Liver Disease (OR: 1.29) | CANCER (OR: 2.20) | Hypertension (OR: 2.83) | ||
| Age groups | 0–14 | 0.5 | 0.02 | |||||
| 15–29 | 0.7 | 0.4 | 0.8 | 1.7 | 0.3 | 0.1 | 2.4 | |
| 30–44 | 0.7 | 0.7 | 2.5 | 3.3 | 0.9 | 3.1 | 6.7 | |
| 45–59 | 5.0 | 0.9 | 10.3 | 5.9 | 2.0 | 7.6 | 23.5 | |
| 60–74 | 10.5 | 2.5 | 25.4 | 9.0 | 2.9 | 15.7 | 42.0 | |
| ≥75 | 14.6 | 5.4 | 36.9 | 8.9 | 2.3 | 17.3 | 53.7 | |
| Diabetes | Chronic Kidney Disease | Chronic Heart Disease | Chronic Respiratory Disease | Chronic Liver Disease | Cancer | Hypertension | ||
|---|---|---|---|---|---|---|---|---|
| Age groups | 0–14 | 6094 | 244 | |||||
| 15–29 | 17,197 | 4417 | 8848 | 18,713 | 3857 | 1213 | 26,500 | |
| 30–44 | 11,909 | 17,197 | 61,428 | 81,035 | 20,887 | 76,121 | 164,598 | |
| 45–59 | 43,192 | 15,312 | 175,247 | 100,474 | 33,188 | 128,995 | 399,806 | |
| 60–74 | 72,745 | 21,596 | 219,176 | 77,995 | 25,425 | 135,540 | 362,815 | |
| ≥75 | 177,951 | 37,412 | 255,900 | 61,830 | 15,847 | 120,200 | 372,041 |




References
- Ferguson, N.; Laydon, D.; Nedjati Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Bhatia, S.; Boonyasiri, A.; Cucunuba Perez, Z.U.; Cuomo-Dannenburg, G.; et al. Report 9: Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID19 Mortality and Healthcare Demand. 2020. Available online: https://standpunkt.jetzt/wp-content/uploads/2020/07/COVID19-Report-9-Imperial-College.pdf (accessed on 15 January 2021).
- Nussbaumer-Streit, B.; Mayr, V.; Dobrescu, A.I.; Chapman, A.; Persad, E.; Klerings, I.; Wagner, G.; Siebert, U.; Christof, C.; Zachariah, C.; et al. Quarantine alone or in combination with other public health measures to control COVID-19: A rapid review. Cochrane Database Syst. Rev. 2020, 4, CD013574. [Google Scholar] [PubMed]
- Viswanathan, M.; Kahwati, L.; Jahn, B.; Giger, K.; Dobrescu, A.I.; Hill, C.; Klerings, I.; Meixner, J.; Persad, E.; Teufer, B.; et al. Universal screening for SARS-CoV-2 infection: A rapid review. Cochrane Database Syst. Rev. 2020, 2020. [Google Scholar] [CrossRef]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; El-harakeh, A.; Bognanni, A.; Lotfi, T.; Loeb, M.; et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Draft Landscape of COVID-19 Candidate Vaccines 2021. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 15 January 2021).
- Krammer, F. SARS-CoV-2 vaccines in development. Nature 2020, 586, 516–527. [Google Scholar] [CrossRef]
- Sahu, K.K.; Jindal, V.; Siddiqui, A.D.; Cerny, J. Facing COVID-19 in the hematopoietic cell transplant setting: A new challenge for transplantation physicians. Blood Cells Mol. Dis. 2020, 83, 102439. [Google Scholar] [CrossRef]
- Lee, K.W.; Yap, S.F.; Ngeow, Y.F.; Lye, M.S. COVID-19 in People Living with HIV: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 3554. [Google Scholar] [CrossRef]
- Arora, M.; Lakshmi, R. Maternal vaccines-safety in pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2021. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Framework for Equitable Allocation of COVID-19 Vaccine; The National Academies Press: Washington, DC, USA, 2020. [Google Scholar]
- Kim, D.S.; Rowland-Jones, S.; Gea-Mallorqui, E. Will SARS-CoV-2 Infection Elicit Long-Lasting Protective or Sterilising Immunity? Implications for Vaccine Strategies (2020). Front. Immunol. 2020, 11, 571481. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef]
- Hall, V.J.; Foulkes, S.; Charlett, A.; Atti, A.; Monk, E.J.; Simmons, R.; Wellington, E.; Cole, M.J.; Saei, A.; Oguti, B.; et al. Do Antibody Positive Healthcare Workers Have Lower SARS-CoV-2 Infection Rates Than Antibody Negative Healthcare Workers? Large Multi-Centre Prospective Cohort Study (the SIREN Study), England: June to November 2020. medRxiv 2020. Preprint. Available online: https://www.medrxiv.org/content/10.1101/2021.01.13.21249642v1 (accessed on 16 January 2021).
- Fitzpatrick, M.C.; Galvani, A.P. Optimizing age-specific vaccination. Science 2021, 371, 890–891. [Google Scholar] [CrossRef]
- Cohen, S.A.; Chui, K.K.; Naumova, E.N. Influenza vaccination in young children reduces influenza-associated hospitalizations in older adults, 2002-2006. J. Am. Geriatr. Soc. 2011, 59, 327–332. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Who Gets Vaccinated First 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations.html (accessed on 15 January 2021).
- Mossong, J.; Hens, N.; Jit, M.; Beutels, P.; Auranen, K.; Mikolajczyk, R.; Massari, M.; Salmaso, S.; Tomba, G.S.; Wallinga, J.; et al. Social contacts and mixing patterns relevant to the spread of infectious diseases. PLoS Med. 2008, 5, e74. [Google Scholar] [CrossRef]
- Österreichisches Rotes Kreuz. Initiative Österreich Impft. 2021. Available online: https://www.xn--sterreich-impft-7sb.at/ (accessed on 15 January 2021).
- Siebert, U. When should decision-analytic modeling be used in the economic evaluation of health care? Eur. J. Health Econ. 2003, 4, 143–150. [Google Scholar] [CrossRef]
- Bicher, M.; Rippinger, C.; Urach, C.; Brunmeir, D.; Siebert, U.; Popper, N. Evaluation of Contact-Tracing Policies Against the Spread of SARS-CoV-2 in Austria—An Agent-Based Simulation. medRxiv 2020. Preprint. Available online: https://www.medrxiv.org/content/10.1101/2020.05.12.20098970v3 (accessed on 10 December 2020).
- Bicher, M.; Rippinger, C.; Brunmeir, D.; Urach, C.; Popper, N. Agent-Based COVID-19 Simulation Model. 2021. Available online: https://www.dwh.at/projects/covid-19/Covid19_Model_v20200929.pdf (accessed on 14 December 2020).
- Bicher, M.; Urach, C.; Popper, N. Gepoc ABM: A generic agent- based population model for Austria. In Proceedings of the 2018 Winter Simulation Conference, Gothenburg, Sweden, 9–12 December 2018; pp. 2656–2667. [Google Scholar]
- Rippinger, C.; Bicher, M.; Urach, C.; Brunmeir, D.; Weibrecht, N.; Zauner, G.; Sroczynski, G.; Jahn, B.; Mühlberger, N.; Siebert, U.; et al. Evaluation of undetected cases during the COVID-19 epidemic in Austria. BMC Infect. Dis. 2021, 21, 70. [Google Scholar] [CrossRef]
- Bicher, M.; Zuba, M.; Rainer, L.; Bachner, F.; Rippinger, C.; Ostermann, H.; Popper, N.; Thurner, S.; Klimek, P. Supporting Austria through the COVID-19 Epidemics with a Forecast-Based Early Warning System. medRxiv 2020. Preprint. Available online: https://www.medrxiv.org/content/10.1101/2020.10.18.20214767v2 (accessed on 11 December 2020).
- Caro, J.J.; Briggs, A.H.; Siebert, U.; Kuntz, K.M.; Ispor-SMDM Modeling Good Research Practices Task Force. Modeling good research practices—Overview: A report of the ISPOR-SMDM Modeling Good Research Practices Task Force-1. Med. Decis. Mak. 2012, 32, 667–677. [Google Scholar] [CrossRef]
- Roberts, M.; Russell, L.B.; Paltiel, A.D.; Chambers, M.; McEwan, P.; Krahn, M.; Ispor-SMDM Modeling Good Research Practices Task Force. Conceptualizing a model: A report of the ISPOR-SMDM Modeling Good Research Practices Task Force-2. Med. Decis. Mak. 2012, 32, 678–689. [Google Scholar] [CrossRef]
- Pitman, R.; Fisman, D.; Zaric, G.S.; Postma, M.; Kretzschmar, M.; Edmunds, J.; Brisson, M. Dynamic transmission modeling: A report of the ISPOR-SMDM Modeling Good Research Practices Task Force Working Group-5. Med. Decis. Mak. 2012, 32, 712–721. [Google Scholar] [CrossRef]
- Bellou, V.; Tzoulaki, I.; Evangelou, E.; Belbasis, L. Risk Factors for Adverse Clinical Outcomes in Patients with COVID-19: A Systematic Review and Meta-Analysis. medRxiv 2020. Preprint. Available online: http://medrxiv.org/content/early/2020/05/19/2020.05.13.20100495.abstract (accessed on 29 November 2020).
- Bundesministerium für Soziales, Gesundheit, Pflege und Konsumentenschutz. COVID-19-Impfungen: Anwendungsempfehlungen des Nationalen Impfgremiums, Version 2.2. 2021. Available online: https://www.sozialministerium.at/Corona-Schutzimpfung/Corona-Schutzimpfung---Fachinformationen.html (accessed on 10 January 2021).
- Rechtsinformationssystem des Bundes. Bundesrecht Konsolidiert: Gesamte Rechtsvorschrift für COVID-19-Risikogruppe-Verordnung, Fassung vom 25 February 2021. Available online: https://www.ris.bka.gv.at/GeltendeFassung.wxe?Abfrage=Bundesnormen&Gesetzesnummer=20011167 (accessed on 10 January 2021).
- Robert Koch Institut. Epidemiologischer Steckbrief zu SARS-CoV-2 und COVID-19. 2021. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Steckbrief.html;jsessionid=77C702E85C26B52BE4023A40B7BC7C2F.internet082?nn=13490888#doc13776792bodyText15 (accessed on 15 January 2021).
- Eddy, D.M.; Hollingworth, W.; Caro, J.J.; Tsevat, J.; McDonald, K.M.; Wong, J.B. Force I-SMGRPT. Model transparency and validation: A report of the ISPOR-SMDM Modeling Good Research Practices Task Force-7. Med. Decis. Mak. 2012, 32, 733–743. [Google Scholar] [CrossRef] [Green Version]
- Positionspapier der Gemeinsamen Arbeitsgruppe aus Mitgliedern der Ständigen Impfkommission, des Deutschen Ethikrats und der Nationalen Akademie der Wissenschaften Leopoldina. Wie soll der Zugang zu Einem COVID-19-Impfstoff Geregelt werden? 2020. Available online: https://www.leopoldina.org/publikationen/detailansicht/publication/wie-soll-der-zugang-zu-einem-covid-19-impfstoff-geregelt-werden-2020/ (accessed on 5 February 2021).
- Ssczerbinska, K. Could we have done better with COVID-19 in nursing homes? Eur. Geriatr. Med. 2020, 11, 639–643. [Google Scholar] [CrossRef]
- Marshall, D.A.; Burgos-Liz, L.; IJzerman, M.J.; Crown, W.; Padula, W.V.; Wong, P.K.; Pasupathy, K.S.; Higashi, M.K.; Osgood, N.D. Selecting a dynamic simulation modeling method for health care delivery research-part 2: Report of the ISPOR Dynamic Simulation Modeling Emerging Good Practices Task Force. Value Health 2015, 18, 147–160. [Google Scholar] [CrossRef] [Green Version]
- The K-Project DEXHELPP. Available online: http://dexhelpp.at/ (accessed on 1 April 2021).
- Moore, S.; Hill, E.M.; Dyson, L.; Tildesley, M.; Keeling, M.J. Modelling Optimal Vaccination Strategy for SARS-CoV-2 in the UK. medRxiv 2020. Preprint. Available online: http://medrxiv.org/content/early/2020/09/24/2020.09.22.20194183.1.abstract (accessed on 10 December 2020).
- European Medicines Agency. COVID-19 Vaccine Moderna 5791: Product Information as Approved by the CHMP on 6 January 2021, Pending Endorsement by the European Commission 2021. Available online: https://www.ema.europa.eu/en/documents/product-information/covid-19-vaccine-moderna-product-information_en.pdf (accessed on 15 January 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Bubar, K.M.; Reinholt, K.; Kissler, S.M.; Lipsitch, M.; Cobey, S.; Grad, Y.H.; Larremore, D.B. Model-Informed COVID-19 Vaccine Prioritization Strategies by Age and Serostatus. medRxiv 2020. Preprint. Available online: http://medrxiv.org/content/early/2020/12/07/2020.09.08.20190629.abstract (accessed on 10 December 2020).
- Matrajt, L.; Eaton, J.; Leung, T.; Brown, E.R. Vaccine Optimization for COVID-19, Who to Vaccinate First? 2020. medRxiv Preprint. Available online: http://medrxiv.org/content/early/2020/08/16/2020.08.14.20175257.abstract (accessed on 10 December 2020).
- Foy, B.H.; Wahl, B.; Mehta, K.; Shet, A.; Menon, G.I.; Britto, C. Comparing COVID-19 Vaccine Allocation Strategies in India: A Mathematical Modelling Study. Int. J. Infect. Dis. 2021, 103, 431–438. [Google Scholar] [CrossRef]
- Rappold, E.; Brigitte, J.; Zach, M.; Gruböck, A. Jahresbericht Gesundheitsberuferegister 2019. 2020. Available online: https://jasmin.goeg.at/1497/1/Jahresbericht_Gesundheitsberuferegister_2019_bf.pdf (accessed on 11 December 2020).
- Statistik Austria. Österreichische Gesundheitsbefragung. Hauptergebnisse des Austrian Health Interview Survey (ATHIS) und Methodische Dokumentation. Im Auftrag des Bundesministerium für Gesundheit und der Bundesgesundheitsagentur. 2014. Available online: http://www.statistik.at/web_de/services/publikationen/4/index.html?includePage=detailedView§ionName=Gesundheit&pubId=794 (accessed on 15 December 2020).
- Robert Koch Institut. Gesundheit in Deutschland. Gesundheitsberichterstattung des Bundes. 2015. Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GesInDtld/gesundheit_in_deutschland_2015.html;jsessionid=C4B3688A11A8EDF4C50483D730628F86.internet052?nn=2379316 (accessed on 11 December 2020).
- Statistik Austria—Bevölkerung nach Alter und Geschlecht 2020. Available online: https://www.statistik.at/web_de/statistiken/menschen_und_gesellschaft/bevoelkerung/bevoelkerungsstruktur/bevoelkerung_nach_alter_geschlecht/index.html (accessed on 14 December 2020).
- Gesundheitsberichterstattung des Bundes—Indikator 1 der ECHI Shortlist: Bevölkerung nach Geschlecht und Alter. 2021. Available online: https://www.gbe-bund.de/gbe/pkg_isgbe5.prc_menu_olap?p_uid=gast&p_aid=59029269&p_sprache=D&p_help=0&p_indnr=17&p_indsp=&p_ityp=H&p_fid= (accessed on 14 December 2020).


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jahn, B.; Sroczynski, G.; Bicher, M.; Rippinger, C.; Mühlberger, N.; Santamaria, J.; Urach, C.; Schomaker, M.; Stojkov, I.; Schmid, D.; et al. Targeted COVID-19 Vaccination (TAV-COVID) Considering Limited Vaccination Capacities—An Agent-Based Modeling Evaluation. Vaccines 2021, 9, 434. https://doi.org/10.3390/vaccines9050434
Jahn B, Sroczynski G, Bicher M, Rippinger C, Mühlberger N, Santamaria J, Urach C, Schomaker M, Stojkov I, Schmid D, et al. Targeted COVID-19 Vaccination (TAV-COVID) Considering Limited Vaccination Capacities—An Agent-Based Modeling Evaluation. Vaccines. 2021; 9(5):434. https://doi.org/10.3390/vaccines9050434
Chicago/Turabian StyleJahn, Beate, Gaby Sroczynski, Martin Bicher, Claire Rippinger, Nikolai Mühlberger, Júlia Santamaria, Christoph Urach, Michael Schomaker, Igor Stojkov, Daniela Schmid, and et al. 2021. "Targeted COVID-19 Vaccination (TAV-COVID) Considering Limited Vaccination Capacities—An Agent-Based Modeling Evaluation" Vaccines 9, no. 5: 434. https://doi.org/10.3390/vaccines9050434