
Neurological Prognostic Factors in Hospitalized Patients with COVID-19

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Neurological Symptoms and Sings
2.3. Statistics
3. Results
3.1. Patient Characteristics
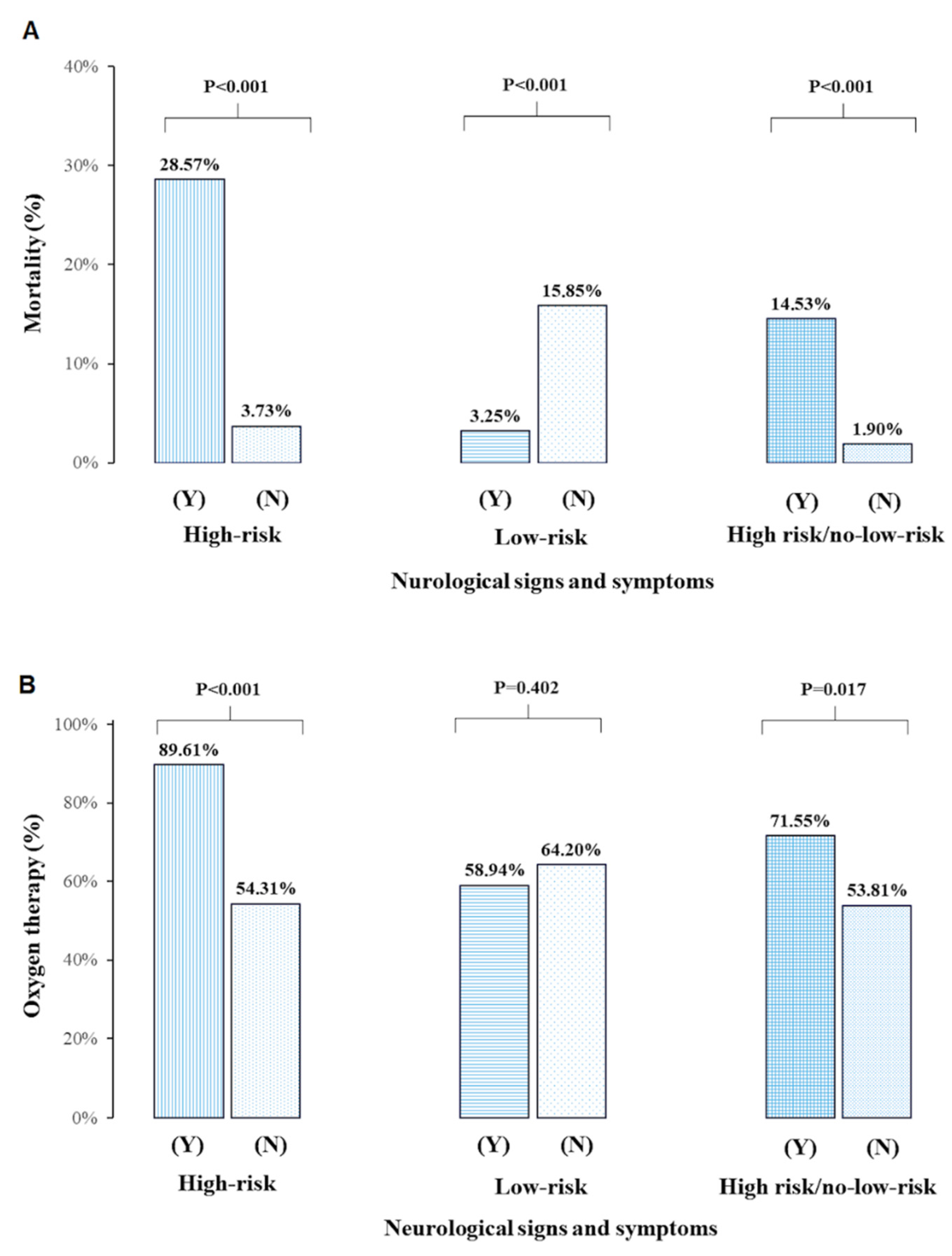
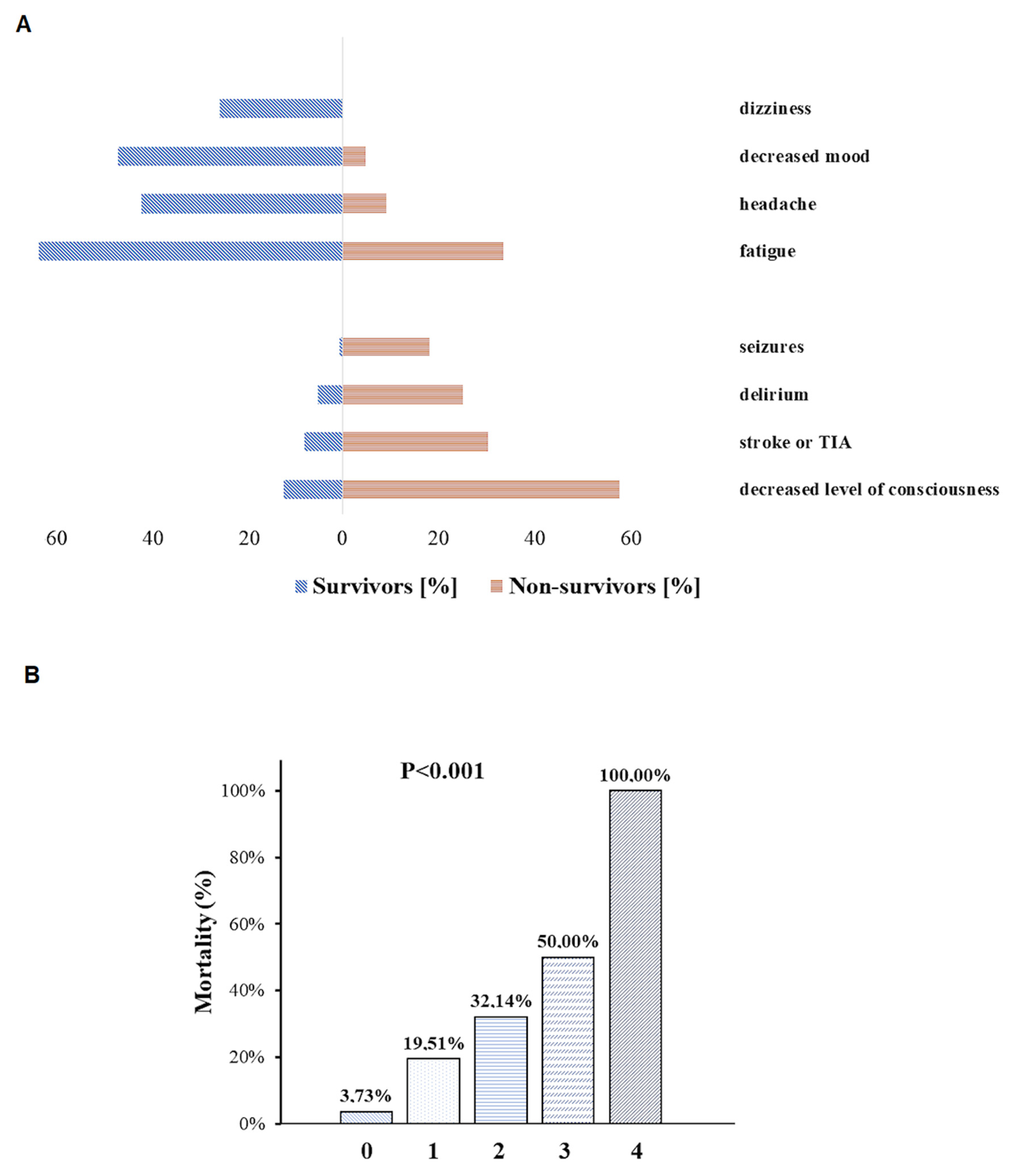
3.2. Mortality
3.3. Oxygen Therapy
3.4. The Severity of Neurological Symptoms and Signs
3.4.1. High-Risk NSS
3.4.2. Low-Risk NSS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xu, B.; Kraemer, M.U.G.; Xu, B.; Gutierrez, B.; Mekaru, S.; Sewalk, K.; Loskill, A.; Wang, L.; Cohn, E.; Hill, S.; et al. Open access epidemiological data from the COVID-19 outbreak. Lancet Infect. Dis. 2020, 20, 534. [Google Scholar] [CrossRef] [Green Version]
- Piroth, L.; Cottenet, J.; Mariet, A.-S.; Bonniaud, P.; Blot, M.; Tubert-Bitter, P.; Quantin, C. Comparison of the characteristics, morbidity, and mortality of COVID-19 and seasonal influenza: A nationwide, population-based retrospective cohort study. Lancet Respir. Med. 2021, 9, 251–259. [Google Scholar] [CrossRef]
- Ni, Y.N.; Wang, T.; Liang, B.M.; Liang, Z.A. The independent factors associated with oxygen therapy in COVID-19 patients under 65 years old. PLoS ONE 2021, 16, e0245690. [Google Scholar] [CrossRef]
- Wańkowicz, P.; Szylińska, A.; Rotter, I. Insomnia, anxiety, and depression symptoms during the COVID-19 pandemic may depend on the pre-existent health status rather than the profession. Brain Sci. 2021, 11, 1001. [Google Scholar] [CrossRef]
- Kacprzak, A.; Malczewski, D.; Domitrz, I. Headache Attributed to SARS-CoV-2 Infection or COVID-19 Related Headache—Not Migraine-like Problem-Original Research. Brain Sci. 2021, 25, 1406. [Google Scholar] [CrossRef]
- Sampaio Rocha-Filho, P.A.; Magalhães, J.E.; Fernandes Silva, D.; Carvalho Soares, M.; Marenga Arruda Buarque, L.; Dandara Pereira Gama, M.; Oliveira, F.A.A. Neurological manifestations as prognostic factors in COVID-19: A retrospective cohort study. Acta Neurol. Belg. 2022. online ahead. [CrossRef]
- Mekkawy, D.A.; Hamdy, S.; Abdel-Naseer, M.; Shehata, H.S.; Halfawy, A.A.; Shalaby, N.M.; Shehata, G.A.; Ali, A.M.; Elmazny, A.; Ahmed, S.M.; et al. Neurological Manifestations in a Cohort of Egyptian Patients with COVID-19: A Prospective, Multicenter, Observational Study. Brain Sci. 2022, 12, 74. [Google Scholar] [CrossRef]
- Wong-Chew, R.M.; Rodríguez Cabrera, E.X.; Rodríguez Valdez, C.A.; Lomelin-Gascon, J.; Morales-Juárez, L.; de la Cerda, M.L.R.; Villa-Romero, A.R.; Arce Fernández, S.; Serratos Fernandez, M.; Bello, H.H.; et al. Symptom cluster analysis of long COVID-19 in patients discharged from the Temporary COVID-19 Hospital in Mexico City. Ther. Adv. Infect. Dis. 2022, 9, 204993612110692. [Google Scholar] [CrossRef]
- Dickens, B.S.L.; Lim, J.T.; Low, J.W.; Lee, C.K.; Sun, Y.; Nasir, H.B.M.; Akramullah, F.A.B.M.; Yan, G.; Oon, J.; Yan, B.; et al. Simple “Rule-of-6” Predicts Severe Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2021, 72, 1861–1862. [Google Scholar] [CrossRef]
- Rinderknecht, M.D.; Klopfenstein, Y. Predicting critical state after COVID-19 diagnosis: Model development using a large US electronic health record dataset. NPJ Digit. Med. 2021, 4, 113. [Google Scholar] [CrossRef]
- Incerti, D.; Rizzo, S.; Li, X.; Lindsay, L.; Yau, V.; Keebler, D.; Chia, J.; Tsai, L. Prognostic model to identify and quantify risk factors for mortality among hospitalised patients with COVID-19 in the USA. BMJ Open 2021, 11, e047121. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Castellano, S.; Nasillo, V.; Ottomano, A.M.; Bergonzini, G.; Paolini, A.; Lusenti, B.; Milić, J.; De Biasi, S.; Gibellini, L.; et al. Monocyte Distribution Width (MDW) as novel inflammatory marker with prognostic significance in COVID-19 patients. Sci. Rep. 2021, 11, 12716. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Nasillo, V.; Luppi, M.; Tagliafico, E.; Trenti, T. Linking COVID-19, monocyte activation and sepsis: MDW, a novel biomarker from cytometry. EBioMedicine 2022, 75, 103754. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, H.K.; Mehra, M.R. COVID-19 illness in native and immunosuppressed states: A clinical–therapeutic staging proposal. J. Heart Lung Transplant. 2020, 39, 405–407. [Google Scholar] [CrossRef] [Green Version]
- Riva, G.; Nasillo, V.; Tagliafico, E.; Trenti, T.; Luppi, M. COVID-19: Room for treating T cell exhaustion? Crit. Care 2020, 24, 229. [Google Scholar] [CrossRef]
- Gibellini, L.; De Biasi, S.; Paolini, A.; Borella, R.; Boraldi, F.; Mattioli, M.; Lo Tartaro, D.; Fidanza, L.; Caro-Maldonado, A.; Meschiari, M.; et al. Altered bioenergetics and mitochondrial dysfunction of monocytes in patients with COVID-19 pneumonia. EMBO Mol. Med. 2020, 12, e13001. [Google Scholar] [CrossRef]
- Zhao, T.-S.; Zeng, H.-L.; Zhang, X.; Chen, X.; Jiang, W.-L.; Du, J.; Liu, H.-Y.; Zhao, J.; Yuan, Y.; Peng, X.-F.; et al. Neurological manifestations in COVID-19 patients and their application in predicting fatal disease: A retrospective cohort study. J. Microbiol. Immunol. Infect. 2021. in press. [CrossRef]
- Bungenberg, J.; Humkamp, K.; Hohenfeld, C.; Rust, M.I.; Ermis, U.; Dreher, M.; Hartmann, N.K.; Marx, G.; Binkofski, F.; Finke, C.; et al. Long COVID-19: Objectifying most self-reported neurological symptoms. Ann. Clin. Transl. Neurol. 2022. online ahead. [CrossRef]
- Deana, C.; Verriello, L.; Pauletto, G.; Corradi, F.; Forfori, F.; Cammarota, G.; Bignami, E.; Vetrugno, L. Insights into neurological dysfunction of critically ill COVID-19 patients. Trends Anaesth. Crit. Care 2021, 36, 30–38. [Google Scholar] [CrossRef]
- Vakili, K.; Fathi, M.; Hajiesmaeili, M.; Salari, M.; Saluja, D.; Tafakhori, A.; Sayehmiri, F.; Rezaei-Tavirani, M. Neurological Symptoms, Comorbidities, and Complications of COVID-19: A Literature Review and Meta-Analysis of Observational Studies. Eur. Neurol. 2021, 84, 307–324. [Google Scholar] [CrossRef]
- Wnuk, M.; Sawczyńska, K.; Kęsek, T.; Wrona, P.; Chatys-Bogacka, Ż.; Mazurkiewicz, I.; Drabik, L.; Jagiełła, J.; Szaleniec, J.; Czepiel, J.; et al. Neurological symptoms in hospitalised patients with COVID-19 and their association with in-hospital mortality. Neurol. Neurochir. Pol. 2021, 55, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Satici, C.; Asim, M.; Sargin, E.; Gursoy, B. Performance of pneumonia severity index and CURB-65 in predicting 30-day mortality in patients with COVID-19. Int. J. Infect. Dis. 2020, 98, 84–89. [Google Scholar] [CrossRef] [PubMed]
- García Clemente, M.M.; Herrero Huertas, J.; Fernández Fernández, A.; De La Escosura Muñoz, C.; Enríquez Rodríguez, A.I.; Pérez Martínez, L.; Gómez Mañas, S.; Iscar Urrutia, M.; López González, F.J.; Madrid Carbajal, C.J.; et al. Assessment of risk scores in Covid-19. Int. J. Clin. Pract. 2021, 75, e13705. [Google Scholar] [CrossRef] [PubMed]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Pawłowska, M.; Parczewski, M.; Piekarska, A.; Simon, K.; Tomasiewicz, K.; Zarębska-Michaluk, D. Management of SARS-CoV-2 infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of 31 March 2020. Pol. Arch. Intern. Med. 2020, 130, 352–357. [Google Scholar] [CrossRef] [Green Version]
- Hu, H.; Yao, N.; Qiu, Y. Predictive value of five early warning scores for critical novel coronavirus disease. Disaster Med. Public Health Prep. 2020, 1–8. [Google Scholar] [CrossRef]
- Aygun, H.; Eraybar, S. The role of emergency department triage early warning score (TREWS) and modified early warning score (MEWS) to predict in-hospital mortality in COVID-19 patients. Ir. J. Med. Sci. 2021, 1–7. [Google Scholar] [CrossRef]
- Kaeley, N.; Mahala, P.; Kabi, A.; Choudhary, S.; Hazra, A.; Vempalli, S. Utility of early warning scores to predict mortality in COVID-19 patients: A retrospective observational study. Int. J. Crit. Illn. Inj. Sci. 2021, 11, 163. [Google Scholar] [CrossRef]
- Meng, L.; Qiu, H.; Wan, L.; Ai, Y.; Xue, Z.; Guo, Q.; Deshpande, R.; Zhang, L.; Meng, J.; Tong, C.; et al. Intubation and Ventilation amid the COVID-19 Outbreak: Wuhan’s Experience. Anesthesiology 2020, 132, 1317–1332. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Li, X.; Marmar, T.; Xu, Q.; Tu, J.; Li, T.; Han, J.; Xu, D.; Shen, T. Cardiac Troponin I association with critical illness and death risk in 726 seriously ill COVID-19 patients: A retrospective cohort study. Int. J. Med. Sci. 2021, 18, 1474–1483. [Google Scholar] [CrossRef]
- Rostami, M.; Mansouritorghabeh, H. D-dimer level in COVID-19 infection: A systematic review. Expert Rev. Hematol. 2020, 13, 1265–1275. [Google Scholar] [CrossRef]
- Brieghel, C.; Ellekvist, P.; Lund, M.L.; Søborg, C.; Walsted, E.S.; Thomsen, J.J.; Biering-Sørensen, T.; Mohr, T.; Knop, F.K.; Ravn, P. Prognostic factors of 90-day mortality in patients hospitalised with covid-19. Dan. Med. J. 2021, 68, 1–9. [Google Scholar]
- Xiong, W.; Lu, L.; Zhang, B.; Luo, J.; Li, W.; He, L.; Sander, J.W.; Mu, J.; Zhu, C.; Zhou, D. Association of consciousness impairment and mortality in people with COVID-19. Acta Neurol. Scand. 2021, 144, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Morandi, A.; Rebora, P.; Isaia, G.; Grossi, E.; Faraci, B.; Gentile, S.; Bo, M.; Valsecchi, M.G.; Deiana, V.; Ghezzi, N.; et al. Delirium symptoms duration and mortality in SARS-CoV2 elderly: Results of a multicenter retrospective cohort study. Aging Clin. Exp. Res. 2021, 33, 2327–2333. [Google Scholar] [CrossRef] [PubMed]
- Syahrul, S.; Maliga, H.A.; Ilmawan, M.; Fahriani, M.; Mamada, S.S.; Fajar, J.K.; Frediansyah, A.; Syahrul, F.N.; Imran, I.; Haris, S.; et al. Hemorrhagic and ischemic stroke in patients with coronavirus disease 2019: Incidence, risk factors, and pathogenesis—A systematic review and meta-analysis. F1000Research 2021, 10, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Leven, Y.; Bösel, J. Neurological manifestations of COVID-19—An approach to categories of pathology. Neurol. Res. Pract. 2021, 3, 39. [Google Scholar] [CrossRef]
- Travi, G.; Rossotti, R.; Merli, M.; D’Amico, F.; Chiappetta, S.; Giussani, G.; Panariello, A.; Corradin, M.; Vecchi, M.; Raimondi, A.; et al. Neurological manifestations in patients hospitalized with COVID-19: A retrospective analysis from a large cohort in Northern Italy. Eur. J. Neurosci. 2021, 53, 2912–2922. [Google Scholar] [CrossRef] [PubMed]
- Goshtasbi, K.; Pang, J.; Lehrich, B.M.; Vasudev, M.; Birkenbeuel, J.L.; Abiri, A.; Kuan, E.C. Association Between Olfactory Dysfunction and Critical Illness and Mortality in COVID-19: A Meta-analysis. Otolaryngol.-Head Neck Surg. 2021, 1–5. [Google Scholar] [CrossRef]
- Moradzadeh, R.; Jamalian, S.M.; Nazari, J.; Kamali, A.; Sadeghi, B.; Hosseinkhani, Z.; Sofian, M.; Zamanian, M. Age-standardized mortality rate and predictors of mortality among COVID-19 patients in Iran. J. Educ. Heal Promot. 2021, 10, 169. [Google Scholar] [CrossRef]
- Amanat, M.; Rezaei, N.; Roozbeh, M.; Shojaei, M.; Tafakhori, A.; Zoghi, A.; Darazam, I.A.; Salehi, M.; Karimialavijeh, E.; Lima, B.S.; et al. Neurological manifestations as the predictors of severity and mortality in hospitalized individuals with COVID-19: A multicenter prospective clinical study. BMC Neurol. 2021, 21, 1–12. [Google Scholar] [CrossRef]
- Heldt, F.S.; Vizcaychipi, M.P.; Peacock, S.; Cinelli, M.; McLachlan, L.; Andreotti, F.; Jovanović, S.; Dürichen, R.; Lipunova, N.; Fletcher, R.A.; et al. Early risk assessment for COVID-19 patients from emergency department data using machine learning. Sci. Rep. 2021, 11, 4200. [Google Scholar] [CrossRef]
- De Souza, F.S.H.; Hojo-Souza, N.S.; de Oliveira Batista, B.D.; da Silva, C.M.; Guidoni, D.L. On the analysis of mortality risk factors for hospitalized COVID-19 patients: A data-driven study using the major Brazilian database. PLoS ONE 2021, 16, e0248580. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.Y.; Seon, J.Y.; Eun, B.L.; Koh, S.B.; Yoo, J.H.; Lee, W.Y.; Yum, H.K.; Yoon, S.J.; Oh, I.H.; Bae, S.C.; et al. Risk Factors of Outcomes of COVID-19 Patients in Korea: Focus on Early Symptoms. J. Korean Med. Sci. 2021, 36, e132. [Google Scholar] [CrossRef] [PubMed]
- Sundaramurthy, R.; Balasubramanian, S.; Ganesan, V.; Aggarwal, P.; Parvataneni, T.; Jyothi Ramachandran Nair, D.P.; Saravanan, R.P. Clinical and Laboratory Factors in Predicting Mortality Among COVID-19 RT-PCR Positive Patients: A Retrospective Observational Study From a Tertiary Care Center. Cureus 2021, 13, e19791. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Kong, W.; Yao, N.; Qiu, Y.; Yao, R. Prognostic value of three rapid scoring scales and combined predictors for the assessment of patients with coronavirus disease 2019. Nurs. Open 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nijman, G.; Wientjes, M.; Ramjith, J.; Janssen, N.; Hoogerwerf, J.; Abbink, E.; Blaauw, M.; Dofferhoff, T.; van Apeldoorn, M.; Veerman, K.; et al. Risk factors for in-hospital mortality in laboratory-confirmed COVID-19 patients in the Netherlands: A competing risk survival analysis. PLoS ONE 2021, 16, e0249231. [Google Scholar] [CrossRef]
- Wang, L.; Lv, Q.; Zhang, X.; Jiang, B.; Liu, E.; Xiao, C.; Yu, X.; Yang, C.; Chen, L. The utility of MEWS for predicting the mortality in the elderly adults with COVID-19: A retrospective cohort study with comparison to other predictive clinical scores. PeerJ 2020, 8. [Google Scholar] [CrossRef]
- Stachura, T.; Celejewska-Wójcik, N.; Polok, K.; Górka, K.; Lichołai, S.; Wójcik, K.; Krawczyk, J.; Kozłowska, A.; Przybyszowski, M.; Włoch, T.; et al. A clinical profile and factors associated with severity of the disease among Polish patients hospitalized due to COVID-19—An observational study. Adv. Respir. Med. 2021, 89, 124–134. [Google Scholar] [CrossRef]
- Hester, J.; Youn, T.S.; Trifilio, E.; Robinson, C.P.; Babi, M.-A.; Ameli, P.; Roth, W.; Gatica, S.; Pizzi, M.A.; Gennaro, A.; et al. The Modified Early Warning Score: A Useful Marker of Neurological Worsening but Unreliable Predictor of Sepsis in the Neurocritically Ill—A Retrospective Cohort Study. Crit. Care Explor. 2021, 3, e0386. [Google Scholar] [CrossRef]
- Salahuddin, H.; Afreen, E.; Sheikh, I.S.; Lateef, S.; Dawod, G.; Daboul, J.; Karim, N.; Gharaibeh, K.; Al-Chalabi, M.; Park, S.; et al. Neurological Predictors of Clinical Outcomes in Hospitalized Patients With COVID-19. Front. Neurol. 2020, 11, 1–8. [Google Scholar] [CrossRef]
- Park, J.; Kwon, Y.-S.; Kim, H.-A.; Kwon, D.-H.; Hwang, J.; Jang, S.-H.; Park, H.; Sohn, S.-I.; Choi, H.A.; Hong, J.-H. Clinical Implications of Neurological Comorbidities and Complications in ICU Patients with COVID-19. J. Clin. Med. 2021, 10, 2281. [Google Scholar] [CrossRef]
- García-Azorín, D.; Martínez-Pías, E.; Trigo, J.; Hernández-Pérez, I.; Valle-Peñacoba, G.; Talavera, B.; Simón-Campo, P.; de Lera, M.; Chavarría-Miranda, A.; López-Sanz, C.; et al. Neurological Comorbidity Is a Predictor of Death in Covid-19 Disease: A Cohort Study on 576 Patients. Front. Neurol. 2020, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kummer, B.R.; Klang, E.; Stein, L.K.; Dhamoon, M.S.; Jetté, N. History of Stroke Is Independently Associated with In-Hospital Death in Patients with COVID-19. Stroke 2020, 51, 3112–3114. [Google Scholar] [CrossRef] [PubMed]
- Gogu, A.E.; Motoc, A.G.; Stroe, A.Z.; Docu Axelerad, A.; Docu Axelerad, D.; Pârv, F.; Munteanu, G.; Dan, F.; Jianu, D.C. Clinical spectrum and neuroimagistic features in hospitalized patients with neurological disorders and concomitant coronavirus-19 infection. Brain Sci. 2021, 11, 1138. [Google Scholar] [CrossRef] [PubMed]
- Sze, S.; Pan, D.; Nevill, C.R.; Gray, L.J.; Martin, C.A.; Nazareth, J.; Minhas, J.S.; Divall, P.; Khunti, K.; Abrams, K.R.; et al. Ethnicity and clinical outcomes in COVID-19: A systematic review and meta-analysis. EClinicalMedicine 2020, 29–30, 100630. [Google Scholar] [CrossRef] [PubMed]
- Jarius, S.; Pache, F.; Körtvelyessy, P.; Jelčić, I.; Stettner, M.; Franciotta, D.; Keller, E.; Neumann, B.; Ringelstein, M.; Senel, M.; et al. Cerebrospinal fluid findings in COVID-19: A multicenter study of 150 lumbar punctures in 127 patients. J. Neuroinflamm. 2022, 19, 19. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Jain, R.; Dogra, S.; Krieger, P.; Lewis, A.; Nguyen, V.; Melmed, K.; Galetta, S. Cerebral Microbleeds and Leukoencephalopathy in Critically Ill Patients with COVID-19. Stroke 2020, 51, 2649–2655. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Death | Oxygen Therapy | ||||||
|---|---|---|---|---|---|---|---|
| All Patients n = 349 | No n = 316 | Yes n = 33 | p-Value | No n= 131 | Yes n = 218 | p-Value | |
| Demographics | |||||||
| Age (years) | 64 (51–77) | 62 (49–75) | 77 (73–84) | <0.001 | 58 (45–69) | 68.5 (55–79) | <0.001 |
| Age >75 years, n (%) | 101 (28.94) | 80 (25.31) | 21 (63.63) | <0.001 | 22 (16.79) | 80 (36.70) | <0.001 |
| Female sex, n (%) | 191 (54.72) | 173 (54.75) | 18 (54.55) | 0.982 | 85 (64.89) | 105 (48.17) | 0.002 |
| Comorbidities and treatment | |||||||
| Hypertension, n (%) | 209 (59.89) | 187 (59.18) | 22 (66.67) | 0.403 | 65 (49.62) | 144 (66.06) | 0.002 |
| Obesity, n (%) | 65 (18.62) | 58 (18.35) | 7 (21.21) | 0.688 | 20 (15.27) | 46 (21.10) | 0.178 |
| Smoking, n (%) | 54 (15.47) | 4 (14.92) | 7 (21.21) | 0.342 | 17 (12.98) | 37 (17.13) | 0.301 |
| Diabetes mellitus, n (%) | 90 (25.79) | 76 (24.05) | 14 (42.42) | 0.022 | 26 (19.85) | 64 (29.36) | 0.049 |
| Ischemic heart disease, n (%) | 59 (16.91) | 51 (16.14) | 8 (24.24) | 0.237 | 16 (12.21) | 43 (19.72) | 0.077 |
| Prior CNS disease, n (%) | 77 (22.06) | 56 (17.72) | 21 (63.64) | <0.001 | 17 (12.98) | 60 (27.52) | 0.002 |
| Stroke | 40 (11.46) | 27 (8.54) | 13 (39.39) | <0.001 | 10 (7.63) | 30 (13.82) | 0.079 |
| Dementia | 19 (5.44) | 16 (5.06) | 3 (9.10) | 0.332 | 0 (0.00) | 19 (8.76) | <0.001 |
| Parkinsonian syndrome | 7 (2.01) | 4 (1.23) | 3 (9.09) | 0.029 | 2 (1.53) | 5 (2.30) | 0.714 |
| Epilepsy | 13 (3.72) | 12 (3.80) | 1 (3.03) | 1.000 | 4 (3.05) | 9 (4.15) | 0.773 |
| CNS tumor | 8 (2.29) | 4 (1.27) | 4 (12.12) | 0.004 | 1 (0.76) | 7 (3.23) | 0.267 |
| Traumatic brain injury | 5 (1.43) | 3 (0.95) | 2 (6.06) | 0.072 | 1 (0.76) | 4 (1.84) | 0.654 |
| Asthma / COPD, n (%) | 20 (5.73) | 20 (6.33) | 0 (0.0) | 0.237 | 4 (3.05) | 17 (7.80) | 0.102 |
| Neoplasm, n (%) | 40 (11.46) | 31 (9.81) | 9 (27.27) | 0.027 | 6 (4.58) | 33 (15.14) | 0.002 |
| Chronic kidney disease stage 3, n (%) | 17 (4.87) | 12 (3.80) | 5 (15.15) | 0.039 | 3 (2.29) | 14 (6.42) | 0.121 |
| Immunosupressive treatment, n (%) | 18 (5.16) | 16 (5.06) | 2 (6.06) | 0.683 | 5 (3.82) | 13 (5.96) | 0.460 |
| First COVID-19 symptoms | |||||||
| Fever, n (%) | 207 (59.31) | 188 (59.49) | 19 (57.68) | 0.831 | 67 (51.15) | 141 (64.68) | 0.012 |
| Cough, n (%) | 219 (62.75) | 199 (62.97) | 20 (60.61) | 0.788 | 72 (54.96) | 147 (67.43) | 0.019 |
| Sore throat, n (%) | 44 (12.61) | 42 (13.29) | 2 (6.06)% | 0.405 | 24 (18.32) | 20 (9.17) | 0.013 |
| Loss of appetite, n (%) | 105 (30.09) | 100 (31.65) | 5 (15.15) | 0.071 | 39 (29.77) | 67 (30.73) | 0.849 |
| Dyspnea, n (%) | 178 (51.00) | 156 (49.37) | 22 (66.67) | 0.058 | 34 (25.95) | 145 (66.50) | <0.001 |
| Abdominal pain, n (%) | 67 (19.20) | 62 (19.62) | 5 (15.15) | 0.535 | 22 (16.79) | 46 (21.10) | 0.325 |
| Neurological symptoms and signs | |||||||
| Headache, n (%) | 130 (37.24) | 128 (41.69) | 2 (9.09) | 0.025 | 64 (49.23) | 67 (33.67) | 0.005 |
| Dizziness, n (%) | 78 (22.35) | 78 (25.41) | 0 (0.0) | 0.032 | 29 (22.31) | 50 (25.13) | 0.558 |
| Decreased mood, n (%) | 44 (41.26) | 143 (46.58) | 1 (4.76) | <0.001 | 58 (44.62) | 87 (43.94) | 0.904 |
| Memory or concetration difficulties, n (%) | 57 (16.33) | 50 (16.29) | 7 (31.82) | 0.063 | 20 (15.38) | 37 (18.59) | 0.452 |
| Fatigue, n (%) | 200 (57.31) | 193 (62.87) | 7 (33.33) | 0.007 | 77 (59.23) | 124 (62.63) | 0.536 |
| Visual disturbances, n (%) | 26 (7.45) | 24 (7.82) | 2 (9.52) | 0.677 | 13 (10.00) | 13 (6.57) | 0.260 |
| Decreased level of consciousness, n (%) | 57 (16.33) | 38 (12.06) | 19 (57.58) | <0.001 | 3 (2.29) | 54 (24.88) | <0.001 |
| Delirium, n (%) | 24 (6.88) | 16 (5.11) | 8 (25.0) | <0.001 | 2 (1.54) | 2 (10.23) | 0.002 |
| Seizures, n (%) | 8 (2.30) | 2 (0.63) | 6 (18.18) | <0.001 | 0 (0.0) | 8 (3.69) | 0.027 |
| Ataxia, n (%) | 6 (1.72) | 5 (1.61) | 1 (3.57) | 0.406 | 2 (1.54) | 4 (1.91) | 1.000 |
| Involuntary movements, n (%) | 16 (4.58) | 12 (3.81) | 4 (12.12) | 0.054 | 4 (3.05) | 12 (5.53) | 0.428 |
| Symptoms of stroke / TIA, n (%) | 35 (10.03) | 25 (7.91) | 10 (30.30) | <0.001 | 6 (4.58) | 29 (13.3) | 0.008 |
| Anosmia, n (%) | 73 (20.92) | 70 (22.80) | 3 (14.29) | 0.587 | 28 (21.54) | 45 (22.73) | 0.800 |
| Ageusia, n (%) | 89 (25.50) | 87 (28.34) | 2 (9.52) | 0.075 | 30 (23.08) | 59 (29.80) | 0.181 |
| Muscle weakness, n (%) | 160 (45.85) | 149 (48.22) | 11 (50.00) | 1.000 | 55 (42.31) | 106 (52.74) | 0.063 |
| Myalgia, n (%) | 122 (34.96) | 114 (37.13) | 8 (38.10) | 1.000 | 45 (34.62) | 78 (39.39) | 0.381 |
| Paresthesia, n (%) | 64 (18.34) | 61 (19.81) | 3 (14.29) | 0.776 | 29 (22.31) | 35 (17.59) | 0.290 |
| Diarrhea, n (%) | 92 (26.36) | 87 (27.53) | 5 (15.63) | 0.145 | 30 (22.90) | 63 (29.03) | 0.210 |
| Increased sweating, n (%) | 115 (32.95) | 110 (35.71) | 5 (20.00) | 0.13 | 37 (28.46) | 78 (38.42) | 0.062 |
| Blood pressure <90/60 mmHg, n (%) | 66 (18.91) | 48 (15.19) | 18 (54.55) | <0.001 | 13 (9.92) | 53 (24.31) | <0.001 |
| Heart rate (>100/min), n (%) | 105 (30.09) | 89 (28.16) | 16 (48.48) | 0.015 | 29 (22.14) | 78 (34.86) | 0.012 |
| High-risk NSS, n (%) | 77 (22.06) | 55 (17.57) | 22 (68.75) | <0.001 | 8 (6.15) | 69 (32.24) | <0.001 |
| Low-risk NSS, n (%) | 246 (70.49) | 238 (77.52) | 8 (38.1) | <0.001 | 101 (71.69) | 145 (73.60) | 0.402 |
| High-risk/absence of low-risk NSS, n (%) | 117 (35.78) | 100 (32.68) | 17 (80.95) | <0.001 | 33 (25.38) | 83 (42.53) | 0.017 |
| Hospital admission | |||||||
| Oxygen therapy, n (%) | <0.001 | - | - | ||||
| Not required | 131 (37.53) | 131 (40.82) | 0 (0.0) | 150 (68.80) | |||
| Nasal cannula | 150 (42.50) | 146 (46.20) | 4 (12.1) | 65 (29.81) | |||
| Non-re-breather mask | 65 (18.62) | 36 (11.40) | 29 (87.87) | 3 (1.37) | |||
| Non-invasive ventilation | 3 (0.86) | 3 (0.95) | 0 (0.0) | (0.0) | |||
| MEWS score, n (%) | <0.001 | <0.001 | |||||
| 0–2 | 330 (95.10) | 306 (97.14) | 24 (75.00) | 131 (100.0) | 198 (92.09) | ||
| ≥3 | 17 (4.90) | 9 (2.86) | 8 (25.00) | 0 (0.00) | 17 (7.91) | ||
| Laboratory tests | |||||||
| Troponin I (mg/dL) | 6.39 (3.24–16.41) | 5.80 (2.95–13.36) | 21.21 (11.53–39.53) | <0.001 | 4.02 (1.25–8.56) | 8.29 (4.39–20.27) | <0.001 |
| D-dimer (mg/L) | 0.72 (0.44–1.48) | 0.70 (0.43–1.39) | 1.23 (0.63–3.31) | 0.005 | 0.53 (0.31–1.17) | 0.86 (0.51–1.68) | <0.001 |
| Univariable Analysis | Multivariable Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Model A | Model B | Model C | ||||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age, decades | 2.08 (1.51–2.86) | <0.001 | 1.70 (1.11–2.61) | 0.016 | 1.68 (1.09–2.60) | 0.020 | 1.58 (1.02–2.45) | 0.041 |
| Prior CNS disease | 8.13 (3.78–17.47) | <0.001 | 5.26 (1.86–14.90) | 0.002 | - | - | - | - |
| Diabetes mellitus | 2.33 (1.11–4.86) | 0.025 | - | - | - | - | - | - |
| Chronic kidney disease stage 3 | 4.52 (1.49–13.76) | 0.008 | - | - | - | - | - | - |
| Neoplasm | 3.49 (1.47–8.08) | 0.004 | 4.64 (1.48–14.56) | 0.008 | 3.93 (1.14–13.59) | 0.031 | 4.83 (1.42–16.37) | 0.001 |
| High-risk neurological symptoms or signs | 10.32 (4.63–23.02) | <0.001 | 3.13 (1.11–8.84) | 0.031 | x | x | x | x |
| Low-risk neurological symptoms or signs | 0.18 (0.07–0.49) | <0.001 | x | x | 0.15 (0.05–0.48) | 0.001 | x | x |
| High-risk/or absence of low-risk neurological symptoms or signs | 8.76 (2.87–26.70) | <0.001 | x | x | x | x | 7.67 (1.94–30.20) | 0.004 |
| MEWS score (per point) | 2.08 (1.51–2.88) | <0.001 | 2.00 (1.30–3.04) | 0.001 | 2.25 (1.42–3.54) | <0.001 | 2.00 (1.29–3.10) | 0.002 |
| Troponin I (log) | 1.60 (1.25–2.05) | 0.002 | - | - | - | - | - | - |
| D-dimer (log) | 1.70 (1.26–2.28) | <0.001 | - | - | - | - | - | - |
| AIC | 127.21 | 104.75 | 104.73 | |||||
| The Wald test, (df), p-value | 36.02, (5), <0.001 | 27.10, (4), <0.001 | 25.73, (4), <0.001 | |||||
| AUC (95% CI) | 0.91 (0.87–0.95) | 0.89 (0.83–0.95) | 0.89 (0.83–0.95) | |||||
| The Hosmer–Lemeshow test p-value | 0.678 | 0.727 | 0.566 | |||||
| Univariable Analysis | Multivariable Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Model A | Model B | Model C | ||||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age, decades | 1.41 (1.2–1.62) | <0.001 | 1.21 (1.01–1.49) | 0.042 | 1.29 (1.08–1.54) | 0.005 | 1.24 (1.03–1.49) | 0.020 |
| Female sex | 0.51 (0.33–0.79) | 0.003 | 0.51 (0.29–0.91) | 0.023 | 0.51 (0.29–0.90) | 0.019 | 0.50 (0.28–0.87) | 0.018 |
| Prior CNS disease | 2.56 (1.42–4.62) | 0.002 | - | - | - | - | - | - |
| Hypertension | 1.96 (1.26–3.06) | 0.003 | - | - | - | - | - | - |
| Diabetes mellitus | 1.69 (1.01–2.84) | 0.048 | - | - | - | - | - | - |
| Neoplasm | 3.74 (1.52–9.18) | 0.004 | 3.85 (1.31–11.31) | 0.014 | 3.33 (1.15–9.64) | 0.027 | 3.46 (1.18–10.14) | 0.024 |
| High-risk neurological symptoms or signs | 7.26 (3.36–15.68) | <0.001 | 4.48 (1.88–10.68) | 0.001 | x | x | x | x |
| Low-risk neurological symptoms or signs | 0.80 (0.48–1.4) | 0.298 | - | - | x | x | x | x |
| High-risk/no low-risk neurological symptoms or signs | 2.16 (1.32–3.51) | 0.002 | x | x | x | x | 1.86 (1.01–3.46) | 0.049 |
| MEWS score | 5.01 (3.09–8,14) | <0.001 | 5.49 (3.05–9.74) | <0.001 | 5.78 (3.24–10.32) | <0.001 | 5.40 (3.03–9.62) | <0.001 |
| Troponin I (log) | 1.55 (1.26–1.92) | <0.001 | - | - | - | - | - | - |
| D-dimer (log) | 1.67 (1.30–2.15) | <0.001 | - | - | - | - | - | - |
| AIC | 299.33 | 303.45 | 301.21 | |||||
| The Wald test, (df), p-value | 55.35, (5), <0.001 | 48.14, (4), <0.001 | 64.03, (5), <0.001 | |||||
| AUC (95% CI) | 0.83 (0.79–0.87) | 0.80 (0.74–0.86) | 0.79 (0.75–0.83) | |||||
| The Hosmer–Lemeshow test p-value | 0.366 | 0.241 | 0.263 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drabik, L.; Derbisz, J.; Chatys-Bogacka, Z.; Mazurkiewicz, I.; Sawczynska, K.; Kesek, T.; Czepiel, J.; Wrona, P.; Szaleniec, J.; Wojcik-Bugajska, M.; et al. Neurological Prognostic Factors in Hospitalized Patients with COVID-19. Brain Sci. 2022, 12, 193. https://doi.org/10.3390/brainsci12020193
Drabik L, Derbisz J, Chatys-Bogacka Z, Mazurkiewicz I, Sawczynska K, Kesek T, Czepiel J, Wrona P, Szaleniec J, Wojcik-Bugajska M, et al. Neurological Prognostic Factors in Hospitalized Patients with COVID-19. Brain Sciences. 2022; 12(2):193. https://doi.org/10.3390/brainsci12020193
Chicago/Turabian StyleDrabik, Leszek, Justyna Derbisz, Zaneta Chatys-Bogacka, Iwona Mazurkiewicz, Katarzyna Sawczynska, Tomasz Kesek, Jacek Czepiel, Pawel Wrona, Joanna Szaleniec, Malgorzata Wojcik-Bugajska, and et al. 2022. "Neurological Prognostic Factors in Hospitalized Patients with COVID-19" Brain Sciences 12, no. 2: 193. https://doi.org/10.3390/brainsci12020193