
Persisting Smell and Taste Disorders in Patients Who Recovered from SARS-CoV-2 Virus Infection—Data from the Polish PoLoCOV-CVD Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodology
- (A)
- 0 points (asymptomatic/mild course)
- Asymptomatic course;
- Parainfluenza symptoms lasting no more than 3 days.
- (B)
- 1 point (mild course)
- Home isolation;
- Subjective patient rating of “1” on a scale of 0 to 3 points;
- Duration of symptoms—less than 7 days.
- (C)
- 2 points (moderate course)
- Subjective patient rating of “2” or “3” on a scale of 0 to 3 points;
- Duration of symptoms—7 to 14 days;
- Presence of dyspnoea and fever ≥ 38 °C.
- (D)
- 3 points (severe course)
- Hospitalisation with a diagnosis of: pneumonia, respiratory failure, intensive care unit treatment, ventilator support, thromboembolic complications during hospitalisation/home isolation;
- (a)
- Diagnosis of SARS-CoV-2 virus infection (in accordance with current guidelines of the Ministry of Health of the Republic of Poland);
- (b)
- Age ≥ 18 years;
- (c)
- Absence of contraindications to participating in the study;
- (d)
- Full recovery (resolution of acute clinical symptoms—at least 2 weeks after last symptoms);
- (e)
- Written consent to participate in the study.
2.2. Statistical Analysis
3. Results
Characteristics of the Study Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Hornuss, D.; Lange, B.; Schröter, N.; Rieg, S.; Kern, W.; Wagner, D. Anosmia in COVID-19 patients. Clin. Microbiol. Infect. 2020, 26, 1426–1427. [Google Scholar] [CrossRef] [PubMed]
- Wee, L.E.; Chan, Y.F.Z.; Teo, N.W.Y.; Cherng, B.P.Z.; Thien, S.Y.; Wong, H.M.; Wijaya, L.; Toh, S.T.; Tan, T.T. The role of self-reported olfactory and gustatory dysfunction as a screening criterion for suspected COVID-19. Eur. Arch. Otorhinolaryngol. 2020, 277, 2389–2390. [Google Scholar] [CrossRef]
- Vaira, L.A.; Deiana, G.; Fois, A.G.; Pirina, P.; Madeddu, G.; De Vito, A.; Babudieri, S.; Petrocelli, M.; Serra, A.; Bussu, F.; et al. Objective evaluation of anosmia and ageusia in COVID-19 patients: Single-center experience on 72 cases. Head Neck 2020, 42, 1252–1258. [Google Scholar] [CrossRef]
- Speth, M.M.; Singer-Cornelius, T.; Oberle, M.; Gengler, I.; Brockmeier, S.J.; Sedaghat, A.R. Olfactory dysfunction and sinonasal symptomatology in COVID-19: Prevalence, severity, timing, and associated character-istics. Otolaryngol. Head. Neck Surg. 2020, 163, 114–120. [Google Scholar] [CrossRef]
- Huart, C.; Philpott, C.; Konstantinidis, I.; Altundag, A.; Whitcroft, K.; Trecca, E.; Cassano, M.; Rombaux, P.; Hummel, T. Comparison of COVID-19 and common cold chemosensory dysfunction. Rhinology 2020, 58, 623–625. [Google Scholar] [CrossRef] [PubMed]
- Giacomelli, A.; Pezzati, L.; Conti, F.; Bernacchia, D.; Siano, M.; Oreni, L.; Rusconi, S.; Gervasoni, C.; Ridolfo, A.L.; Rizzardini, G.; et al. Self-reported olfactory and taste disorders in patients with severe acute respiratory coronavirus 2 infection: A cross-sectional study. Clin. Infect. Dis. 2020, 71, 889–890. [Google Scholar] [CrossRef]
- Klopfenstein, T.; Zahra, H.; Kadiane-Oussou, N.J.; Lepiller, Q.; Royer, P.-Y.; Toko, L.; Gendrin, V.; Zayet, S. New loss of smell and taste: Uncommon symptoms in COVID-19 patients on Nord Franche-Comte cluster, France. Int. J. Infect. Dis. 2020, 100, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Neto, D.B.; Fornazieri, M.A.; Dib, C.; Di Francesco, R.C.; Doty, R.L.; Voegels, R.L.; Pinna, F.D.R. Chemosensory Dysfunction in COVID-19: Prevalences, Recovery Rates, and Clinical Associations on a Large Brazilian Sample. Otolaryngol. Head Neck Surg. 2021, 164, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Kaye, R.; Chang, C.W.D.; Kazahaya, K.; Brereton, J.; Denneny, I.J.C. COVID-19 Anosmia Reporting Tool: Initial Findings. Otolaryngol. Head Neck Surg. 2020, 163, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Mastrangelo, A.; Bonato, M.; Cinque, P. Smell and taste disorders in COVID-19: From pathogenesis to clinical features and outcomes. Neurosci. Lett. 2021, 748, 135694. [Google Scholar] [CrossRef]
- Boesveldt, S.; Postma, E.M.; Boak, D.; Welge-Luessen, A.; Schöpf, V.; Mainland, J.D.; Martens, J.; Ngai, J.; Duffy, V.B. Anosmia—A clinical review. Chem. Senses 2017, 42, 513–523. [Google Scholar] [CrossRef]
- Kim, D.H.; Kim, S.W.; Kang, M.; Hwang, S.H. Efficacy of topical steroids for the treatment of olfactory disorders caused by COVID-19: A systematic review and meta-analysis. Clin. Otolaryngol. 2022, 47, 509–515. [Google Scholar] [CrossRef]
- Agyeman, A.A.; Chin, K.L.; Landersdorfer, C.B.; Liew, D.; Ofori-Asenso, R. Smell and taste dysfunction in patients with COVID-19: A systematic review and meta-analysis. Mayo Clin. Proc. 2020, 95, 1621–1631. [Google Scholar] [CrossRef]
- Rocke, J.; Hopkins, C.; Philpott, C.M.; Kumar, N. Is loss of sense of smell a diagnostic marker in COVID-19: A systematic review and meta-analysis. Clin. Otolaryngol. 2020, 45, 914–922. [Google Scholar] [CrossRef]
- Hura, N.; Xie, D.X.; Choby, G.W.; Schlosser, R.J.; Orlov, C.P.; Seal, S.M.; Rowan, N.R. Treatment of post-viral olfactory dysfunction: An evidence-based review with recommendations. Int. Forum Allergy Rhinol. 2020, 10, 1065–1086. [Google Scholar] [CrossRef] [PubMed]
- Regemorter, V.V.; Hummel, T.; Rosenzweig, F.; Mouraux, A.; Rombaux, P.; Huart, C. Mechanisms linking olfactory impairment and risk of mortality. Front. Neurosci. 2020, 14, 140. [Google Scholar] [CrossRef]
- Kohli, P.; Soler, Z.M.; Nguyen, S.A.; Muus, J.S.; Schlosser, R.J. The association between olfaction and depression: A systematic review. Chem. Senses 2016, 41, 479–486. [Google Scholar] [CrossRef]
- Pinto, J.M.; Wroblewski, K.E.; Kern, D.W.; Schumm, P.; McClintock, M.K. Olfactory dysfunction predicts 5-year mortality in older adults. PLoS ONE 2014, 9, e107541. [Google Scholar] [CrossRef]
- Hummel, T.; Whitcroft, K.L.; Andrews, P.; Altundag, A.; Cinghi, C.; Costanzo, R.M.; Damm, M.; Frasnelli, J.; Gudziol, H.; Gupta, N.; et al. Position paper on olfactory dysfunction. Rhinology 2017, 54, 1–30. [Google Scholar] [CrossRef]
- Doty, R. Handbook of Olfaction and Gustation, 3rd ed.; Wiley-Blackwell: Malden, MA, USA, 2015. [Google Scholar]
- Suzuki, M.; Saito, K.; Min, W.-P.; Vladau, C.; Toida, K.; Itoh, H.; Murakami, S. Identification of viruses in patients with postviral olfactory dysfunction. Laryngoscope 2007, 117, 272–277. [Google Scholar] [CrossRef]
- Bon, L.S.-D.; Konopnicki, D.; Pisarski, N.; Prunier, L.; Lechien, J.R.; Horoi, M. Efficacy and safety of oral corticosteroids and olfactory training in the management of COVID-19-related loss of smell. Eur. Arch. Otorhinolaryngol. 2021, 278, 3113–3117. [Google Scholar] [CrossRef]
- Parma, V.; Ohla, K.; Veldhuizen, M.G.; Niv, M.Y.; Kelly, C.E.; Bakke, A.J.; Cooper, K.W.; Bouysset, C.; Pirastu, N.; Dibattista, M.; et al. More than smell-COVID-19 is associated with severe impairment of smell, taste, and chemesthesis. Chem. Senses 2020, 45, 609–622. [Google Scholar] [CrossRef]
- Whitcroft, K.; Ezzat, M.; Cuevas, M.; Andrews, P.; Hummel, T. The effect of intranasal sodium citrate on olfaction in post-infectious loss: Results from a prospective, placebo-controlled trial in 49 patients. Clin. Otolaryngol. 2017, 42, 557–563. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE), the Scottish Intercollegiate Guidelines Network, (SIGN) and the Royal College of General Practitioners (RCGP). COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. NICE Guideline, No. 188. p. 35. Available online: https://www.ncbi.nlm.nih.gov/books/NBK567261/ (accessed on 18 December 2020).
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. WHO Clinical Case Definition Working Group on Post-COVID-19 Condition A Clinical Case Definition of Post-COVID-19 Condition by a Delphi Consensus. Lancet Infect. Dis. 2021, 22, e102–e107. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F.; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Garrigues, E.; Janvier, P.; Kherabi, Y.; Le Bot, A.; Hamon, A.; Gouze, H.; Doucet, L.; Berkani, S.; Oliosi, E.; Mallart, E.; et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J. Infect. 2020, 81, e4–e6. [Google Scholar] [CrossRef]
- Carvalho-Schneider, C.; Laurent, E.; Lemaignen, A.; Beaufils, E.; Bourbao-Tournois, C.; Laribi, S.; Flament, T.; Ferreira-Maldent, N.; Bruyère, F.; Stefic, K.; et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin. Microbiol. Infect. 2020, 27, 258–263. [Google Scholar] [CrossRef]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef]
- Desgranges, F.; Tadini, E.; Munting, A.; Regina, J.; Filippidis, P.; Viala, B.; Karachalias, E.; Suttels, V.; Haefliger, D.; Kampouri, E.; et al. PostCOVID19 Syndrome in Outpatients: A Cohort Study. J. Gen. Intern. Med. 2022, 37, 1943–1952. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Locatello, L.G.; Trotta, B.; Bruno, C.; Trotta, M.; Maggiore, G.; Rasero, L.; Caini, S.; Gallo, O. Systemic steroids may enhance recovery from loss of smell and taste in hospitalized coronavirus disease 2019 (COVID-19) patients: An observational study. Int. Forum Allergy Rhinol. 2021, 11, 1689–1693. [Google Scholar] [CrossRef]
- Hopkins, C.; Surda, P.; Whitehead, E.; Kumar, B.N. Early recovery following new onset loss of sense of smell during the COVID-19 pandemic—An observational cohort study. J. Otolaryngol.-Head Neck Surg. 2020, 49, 26. [Google Scholar] [CrossRef]
- Reden, J.; Mueller, A.; Mueller, C.; Konstantinidis, I.; Frasnelli, J.; Landis, B.N.; Hummel, T. Recovery of olfactory function following closed head injury or infections of the upper respiratory tract. Arch. Otolaryngol. Head Neck Surg. 2006, 132, 265–269. [Google Scholar] [CrossRef]
- Vaira, L.; Hopkins, C.; Petrocelli, M.; Lechien, J.; Cutrupi, S.; Salzano, G.; Chiesa-Estomba, C.; Saussez, S.; De Riu, G. Efficacy of corticosteroid therapy in the treatment of long- lasting olfactory disorders in COVID-19 patients. Rhinology 2021, 59, 21–25. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Living Guidance for Clinical Management of COVID-19: Living Guidance; World Health Organization (WHO): Geneva, Switzerland, 23 November 2021. [Google Scholar]
- Chudzik, M.; Babicki, M.; Kapusta, J.; Kołat, D.; Kałuzińska, Ż.; Mastalerz-Migas, A.; Jankowski, P. Do the Successive Waves of SARS-CoV-2, Vaccination Status and Place of Infection Influence the Clinical Picture and COVID-19 Severity among Patients with Persistent Clinical Symptoms? The Retrospective Study of Patients from the STOP-COVID Registry of the PoLoCOV-Study. J. Pers. Med. 2022, 12, 706. [Google Scholar] [CrossRef]
- Nishiura, H.; Kobayashi, T.; Miyama, T.; Suzuki, A.; Jung, S.-M.; Hayashi, K.; Kinoshita, R.; Yang, Y.; Yuan, B.; Akhmetzhanov, A.R.; et al. Estimation of the asymptomatic ratio of novel coronavirus infections (COVID-19). Int. J. Infect. Dis. 2020, 94, 154–155. [Google Scholar] [CrossRef]
- Spinato, G.; Fabbris, C.; Polesel, J.; Cazzador, D.; Borsetto, D.; Hopkins, C.; Rizzo, P.B. Alterations in Smell or Taste in Mildly Symptomatic Outpatients With SARS-CoV-2 Infection. JAMA 2020, 323, 2089–2090. [Google Scholar] [CrossRef]
- Boscolo-Rizzo, P.; Borsetto, D.; Spinato, G.; Fabbris, C.; Menegaldo, A.; Gaudioso, P.; Nicolai, P.; Tirelli, G.; Da Mosto, M.C.; Rigoli, R.; et al. New onset of loss of smell or taste in household contacts of home-isolated SARS-CoV-2-positive subjects. Eur. Arch. Otorhinolaryngol. 2020, 277, 2637–2640. [Google Scholar] [CrossRef]
- Home Care for Patients With COVID-19 Presenting with Mild Symptoms and Management of Their Contacts n.d. Available online: https://www.who.int/publications-detail/home-care-for-patients-with-suspected-novel-coronavirus-(ncov)-infection-presenting-with-mild-symptoms-and-management-of-contacts (accessed on 27 April 2020).
- Logue, J.K.; Franko, N.M.; McCulloch, D.J.; McDonald, D.; Magedson, A.; Wolf, C.R.; Chu, H.Y. Sequelae in Adults at 6 Months After COVID-19 Infection. JAMA Netw. Open 2021, 4, e210830. [Google Scholar] [CrossRef] [PubMed]
- Klein, H.; Asseo, K.; Karni, N.; Benjamini, Y.; Nir-Paz, R.; Muszkat, M.; Israel, S.; Niv, M.Y. Onset, duration and unresolved symptoms, including smell and taste changes, in mild COVID-19 infection: A cohort study in Israeli patients. Clin. Microbiol. Infect. 2021, 27, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Von-Bartheld, C.S.; Hagen, M.M.; Butowt, R. Prevalence of Chemosensory Dysfunction in COVID-19 Patients: A Systematic Review and Meta-analysis Reveals Significant Ethnic Differences. ACS Chem. Neurosci. 2020, 11, 2944–2961. [Google Scholar] [CrossRef]
- Yan, C.H.; Faraji, F.; Bs, D.P.P.; Ostrander, B.T.; DeConde, A.S. Self-reported olfactory loss associates with outpatient clinical course in COVID-19. Int. Forum Allergy Rhinol. 2020, 10, 821–831. [Google Scholar] [CrossRef]
- Lechien, J.R.; Journe, F.; Hans, S.; Chiesa-Estomba, C.M.; Mustin, V.; Beckers, E.; Vaira, L.; Riu, G.D.; Hopkins, C.; Saussez, S. Severity of Anosmia as an Early Symptom of COVID-19 Infection May Predict Lasting Loss of Smell. Front. Med. 2020, 7, 582802. [Google Scholar] [CrossRef]
- Printza, A.; Katotomichelakis, M.; Valsamidis, K.; Metallidis, S.; Panagopoulos, P.; Panopoulou, M.; Petrakis, V.; Constantinidis, J. Smell and Taste Loss Recovery Time in COVID-19 Patients and Disease Severity. J. Clin. Med. 2021, 10, 966. [Google Scholar] [CrossRef] [PubMed]
- Bull-Otterson, L.; Baca, S.; Saydah, S.; Boehmer, T.K.; Adjei, S.; Gray, S.; Harris, A.M. Post–COVID Conditions Among Adult COVID-19 Survivors Aged 18–64 and ≥65 Years—United States, March 2020–November 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 713–717. [Google Scholar] [CrossRef]
- Boscolo-Rizzo, P.; Polesel, J.; A Vaira, L. Smell and taste dysfunction after COVID-19. BMJ 2022, 378, o1653. [Google Scholar] [CrossRef]
- Wu, T.J.; Yu, A.C.; Lee, J.T. Management of post-COVID-19 olfactory dysfunction. Curr. Treat. Options Allergy 2022, 9, 1–18. [Google Scholar] [CrossRef]
- Hopkins, C.; Alanin, M.; Philpott, C.; Harries, P.; Whitcroft, K.; Qureishi, A.; Anari, S.; Ramakrishnan, Y.; Sama, A.; Davies, E.; et al. Management of new onset loss of sense of smell during the COVID-19 pandemic—BRS Consensus Guidelines. Clin. Otolaryngol. 2021, 46, 16–22. [Google Scholar] [CrossRef]
- Abdelalim, A.A.; Mohamady, A.A.; Elsayed, R.A.; Elawady, M.A.; Ghallab, A.F. Corticosteroid nasal spray for recovery of smell sensation in COVID-19 patients: A randomized controlled trial. Am. J. Otolaryngol. 2021, 42, 102884. [Google Scholar] [CrossRef] [PubMed]
- Pekala, K.R.; Chandra, R.; Turner, J.H. Efficacy of olfactory training in patients with olfactory loss: A systematic review and meta-analysis. Int. Forum Allergy Rhinol. 2016, 6, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Altundag, A.; Yıldırım, D.; Sanli, D.E.T.; Cayonu, M.; Kandemirli, S.G.; Sanli, A.N.; Duz, O.A.; Saatci, O. Olfactory Cleft Measurements and COVID-19-Related Anosmia. Otolaryngol. Head Neck Surg. 2021, 164, 1337–1344. [Google Scholar] [CrossRef]
- The WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group; Sterne, J.A.C.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; et al. Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar] [CrossRef] [PubMed]
- Mattos-Silva, P.; Felix, N.S.; Silva, P.L.; Robba, C.; Battaglini, D.; Pelosi, P.; Rocco, P.R.M.; Cruz, F.F. Pros and cons of corticosteroid therapy for COVID-19 patients. Respir. Physiol. Neurobiol. 2020, 280, 103492. [Google Scholar] [CrossRef]
- Torabi, A.; Mohammadbagheri, E.; Akbari Dilmaghani, N.; Bayat, A.-H.; Fathi, M.; Vakili, K.; Alizadeh, R.; Rezaeimirghaed, O.; Hajiesmaeili, M.; Ramezani, M.; et al. Proinflammatory cytokines in the olfactory mucosa result in COVID-19 induced anosmia. ACS Chem. Neurosci. 2020, 11, 1909–1913. [Google Scholar] [CrossRef]
- Rydzewski, B.; Pruszewicz, A.; Sulkowski, W.J. Assessment of smell and taste in patients with allergic rhinitis. Acta Otolaryngol. 2000, 120, 323–326. [Google Scholar]
- Nguyen, N.N.; Hoang, V.T.; Lagier, J.-C.; Raoult, D.; Gautret, P. Long-term persistence of olfactory and gustatory disorders in COVID-19 patients. Clin. Microbiol. Infect. 2021, 27, 931–932. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.K.J.; Han, R.; Zhao, J.J.; Tan, N.K.W.; Quah, E.S.H.; Tan, C.J.; Chan, Y.H.; Teo, N.W.Y.; Charn, T.C.; See, A.; et al. Prognosis and persistence of smell and taste dysfunction in patients with COVID-19: Meta-analysis with parametric cure modelling of recovery curves. BMJ 2022, 378, e069503. [Google Scholar] [CrossRef]
- Amer, M.A.; Elsherif, H.S.; Abdel-Hamid, A.S.; Elzayat, S. Early recovery patterns of olfactory disorders in COVID-19 patients; a clinical cohort study. Am. J. Otolaryngol. 2020, 41, 102725. [Google Scholar] [CrossRef]
- Karaarslan, F.; Güneri, F.D.; Kardeş, S. Postdischarge rheumatic and musculoskeletal symptoms following hospitalization for COVID-19: Prospective follow-up by phone interviews. Rheumatol. Int. 2021, 41, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.S.; Hichami, A.; Khan, N.A. Obesity and COVID-19: Oro-Naso-Sensory Perception. J. Clin. Med. 2020, 9, 2158. [Google Scholar] [CrossRef] [PubMed]
- Patel, Z.M.; DelGaudio, J.M.; Wise, S.K. Higher body mass index is associated with subjective olfactory dysfunction. Behav. Neurol. 2015, 2015, 675635. [Google Scholar] [CrossRef] [PubMed]
- Boscolo-Rizzo, P.; Tirelli, G.; Meloni, P.; Hopkins, C.; Madeddu, G.; De Vito, A.; Gardenal, N.; Valentinotti, R.; Tofanelli, M.; Borsetto, D.; et al. Coronavirus disease 2019 (COVID-19)-related smell and taste impairment with widespread diffusion of severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) Omicron variant. Int. Forum Allergy Rhinol. 2022, 3, 1–9. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Smell and Taste Disorders (n = 98) | No Smell and Taste Disorders (n = 2120) | p-Value * | Total (n = 2218) | |
|---|---|---|---|---|
| Age ** | 49.19 ± 14.68 | 54.01 ± 13.44 | <0.001 | 53.80 ± 13.53 |
| Women | 32 (32.65%) | 776 (36.60%) | 0.426 | 808 (36.43%) |
| Men | 66 (67.35%) | 1344 (63.40%) | 1410 (63.57%) | |
| Weight ** | 76.58 ± 15.64 | 79.75 ± 17.30 | 0.091 | 79.61 ± 17.24 |
| Height ** | 169.13 ± 8.38 | 169.11 ± 9.16 | 0.953 | 169.11 ± 9.13 |
| BMI < 30 | 76 (77.55%) | 1409 (67.77%) | 0.042 | 1485 (66.95%) |
| BMI ≥ 30 | 22 (22.45%) | 670 (32.23%) | 692 (31.20%) | |
| Number of comorbidities ** | 1.29 ± 1.44 | 1.70 ± 1.62 | 0.011 | 1.68 ± 1.62 |
| Comorbidities | 56 (57.14%) | 1513 (71.37%) | 0.002 | 1569 (70.74%) |
| Hypertension (HT) | 24 (24.49%) | 802 (37.83%) | 0.007 | 826 (37.24%) |
| Thyroid disease | 17 (17.35%) | 357 (16.84%) | 0.675 | 374 (16.86%) |
| Hyperlipidaemia | 14 (14.29%) | 426 (20.09%) | 0.158 | 440 (19.84%) |
| Diabetes mellitus (DM) | 11 (11.22%) | 219 (10.33%) | 0.773 | 230 (10.37%) |
| Coronary artery disease | 3 (3.06%) | 131 (6.18%) | 0.205 | 134 (6.04%) |
| Previous myocardial infarction (MI) | 1 (1.02%) | 64 (3.02%) | 0.001 | 65 (2.93%) |
| Heart failure | 0 (0.00%) | 26 (1.23%) | 0.270 | 26 (1.17%) |
| Venous thromboembolism | 1 (1.02%) | 23 (1.08%) | 0.951 | 24 (1.08%) |
| Asthma | 7 (7.14%) | 210 (9.91%) | 0.368 | 217 (9.78%) |
| COPD | 1 (1.02%) | 50 (2.36%) | 0.387 | 51 (2.30%) |
| Flu vaccinations in the previous season | 3 (3.06%) | 163 (7.69%) | 0.087 | 166 (7.48%) |
| Vaccination against COVID-19 (n = 697)/ (n = 23 for smell and taste disorders) | 17 (73.91%) | 477 (70.77%) | 0.744 | 494 (22.27%) |
| Smell and Taste Disorders (n = 98) | No Smell and Taste Disorders (n = 2120) | p-Value * | Total (n = 2218) | |
|---|---|---|---|---|
| Pandemic wave | ||||
| 2 | 67 (68.37%) | 1087 (51.27%) | 0.003 | 1154 (52.03%) |
| 3 | 21 (21.43%) | 733 (34.58%) | 754 (33.99%) | |
| 4 | 10 (10.20%) | 300 (14.15%) | 310 (13.98%) | |
| Course of COVID-19 | ||||
| 0 | 8 (8.16%) | 157 (7.48%) | 0.542 | 165 (7.44%) |
| 1 | 35 (35.71%) | 616 (29.33%) | 651 (29.35%) | |
| 2 | 25 (25.51%) | 580 (27.62%) | 605 (27.28%) | |
| 3 | 30 (30.61%) | 747 (35.57%) | 777 (35.03%) | |
| Home isolation | 95 (96.94%) | 1765 (83.25%) | <0.001 | 1860 (83.86%) |
| Hospitalisation without pneumonia | 0 (0.00%) | 33 (1.56%) | 0.213 | 33 (1.49%) |
| Hospitalisation with pneumonia | 1 (1.02%) | 278 (13.11%) | 0.004 | 279 (12.58%) |
| Hospitalisation with ICU | 0 (0.00%) | 19 (0.90%) | 0.346 | 19 (0.86%) |
| Symptoms during COVID-19 | ||||
| Temperature < 36.6 | 20 (20.41%) | 294 (13.87%) | 0.056 | 314 (14.16%) |
| Temperature < 37.5 | 23 (23.47%) | 477 (22.50%) | 0.822 | 500 (22.54%) |
| Temperature > 37.5 | 46 (46.94%) | 1132 (53.40%) | 0.210 | 1178 (53.11%) |
| Cough | 54 (55.10%) | 1360 (64.15%) | 0.068 | 1414 (63.75%) |
| Dyspnoea | 45 (45.92%) | 1014 (47.83%) | 0.711 | 1059 (47.75%) |
| Olfactory dysfunction | 10 (10.20%) | 205 (9.67%) | 0.816 | 215 (9.69%) |
| Taste dysfunction | 1 (1.02%) | 139 (6.56%) | 0.027 | 140 (6.31%) |
| Smell and taste disorders | 82 (83.67%) | 912 (43.02%) | <0.001 | 994 (44.82%) |
| Significant fatigue | 69 (70.41%) | 1555 (73.35%) | 0.520 | 1624 (73.22%) |
| Chest pain | 45 (45.92%) | 923 (43.54%) | 0.642 | 968 (43.64%) |
| Back muscle pain | 50 (51.02%) | 1115 (52.59%) | 0.760 | 1165 (52.52%) |
| Leg muscle pain | 48 (48.98%) | 907 (42.78%) | 0.225 | 955 (43.06%) |
| Headache | 59 (60.20%) | 1166 (55.00%) | 0.311 | 1225 (55.23%) |
| Arthralgia | 50 (51.02%) | 851 (40.14%) | 0.034 | 901 (40.62%) |
| Diarrhoea | 21 (21.43%) | 409 (19.29%) | 0.601 | 430 (19.39%) |
| Vomiting | 4 (4.08%) | 146 (6.89%) | 0.279 | 150 (6.76%) |
| Chills | 36 (36.73%) | 761 (35.90%) | 0.865 | 797 (35.93%) |
| Labile blood pressure values | 16 (16.33%) | 311 (14.67%) | 0.651 | 327 (14.74%) |
| Hearing dysfunction | 14 (14.29%) | 206 (9.72%) | 0.139 | 220 (9.92%) |
| Duration of symptoms (number of days) ** | 10.43 ± 5.49 | 10.73 ± 5.75 | 0.578 | 10.72 ± 5.74 |
| Number of symptoms ** | 8.87 ± 3.65 | 7.91 ± 3.61 | 0.018 | 7.95 ± 3.62 |
| The Whole Group | Propensity Score Matching | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI for OR | p-Value | OR | 95% CI for OR | |||||
| Lower Limit | Upper Limit | Lower Limit | Upper Limit | p-Value | |||||
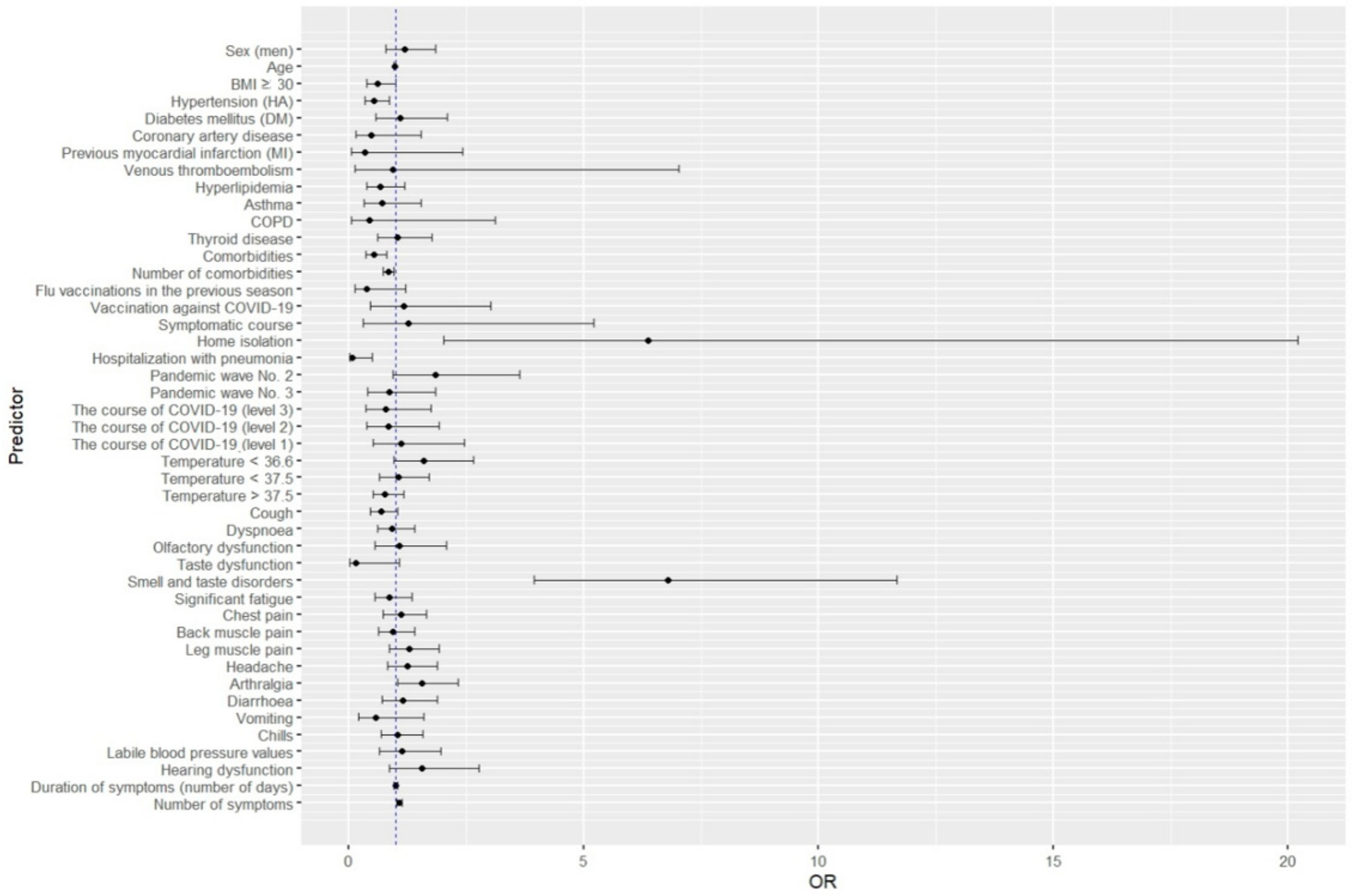
| Sex (men) | 1.191 | 0.774 | 1.833 | 0.427 | 0.913 | 0.521 | 1.600 | 0.751 | |
| Age | 0.973 | 0.959 | 0.987 | 0.001 | 0.998 | 0.979 | 1.017 | 0.857 | |
| BMI ≥ 30 | 0.609 | 0.375 | 0.987 | 0.044 | 0.659 | 0.356 | 1.220 | 0.185 | |
| Hypertension (HT) | 0.533 | 0.334 | 0.852 | 0.009 | 0.765 | 0.419 | 1.397 | 0.384 | |
| Diabetes mellitus (DM) | 1.098 | 0.577 | 2.087 | 0.777 | 1.367 | 0.559 | 3.338 | 0.493 | |
| Coronary artery disease | 0.479 | 0.150 | 1.534 | 0.215 | 0.407 | 0.054 | 3.063 | 0.383 | |
| Previous myocardial infarction (MI) | 0.331 | 0.045 | 2.412 | 0.275 | 0.000 | - | - | - | |
| Heart failure | 0.000 | - | - | - | 0.000 | - | - | - | |
| Venous thromboembolism | 0.940 | 0.126 | 7.032 | 0.952 | 1.112 | 0.139 | 8.932 | 0.919 | |
| Hyperlipidaemia | 0.663 | 0.373 | 1.179 | 0.161 | 0.864 | 0.427 | 1.746 | 0.683 | |
| Asthma | 0.700 | 0.320 | 1.529 | 0.371 | 0.835 | 0.322 | 2.160 | 0.709 | |
| COPD | 0.427 | 0.058 | 3.122 | 0.402 | 0.831 | 0.106 | 6.493 | 0.859 | |
| Thyroid disease | 1.036 | 0.607 | 1.770 | 0.896 | |||||
| Comorbidities | 0.535 | 0.355 | 0.807 | 0.003 | 0.625 | 0.374 | 1.045 | 0.073 | |
| Number of comorbidities | 0.833 | 0.720 | 0.963 | 0.014 | 0.837 | 0.696 | 1.007 | 0.059 | |
| Flu vaccinations in the previous season | 0.379 | 0.119 | 1.210 | 0.101 | 0.221 | 0.029 | 1.628 | 0.138 | |
| Vaccination against COVID-19 | 1.171 | 0.456 | 3.011 | 0.744 | 1.133 | 0.654 | 2.873 | 0.654 | |
| Symptomatic course | 1.255 | 0.301 | 5.222 | 0.755 | 2.031 | 0.268 | 15.389 | 0.492 | |
| Home isolation | 6.370 | 2.007 | 20.215 | 0.002 | 3.441 | 0.832 | 14.392 | 0.043 | |
| Hospitalisation without pneumonia | 0.000 | - | - | - | 0.000 | - | - | - | |
| Hospitalisation with pneumonia | 0.068 | 0.009 | 0.492 | 0.008 | 0.195 | 0.026 | 1..443 | 0.109 | |
| Hospitalisation with ICU | 0.000 | - | - | - | 0.000 | - | - | - | |
| Pandemic wave | 2 | 1.851 | 0.939 | 3.637 | 0.075 | 0.562 | 0.258 | 1.223 | 0.146 |
| 3 | 0.859 | 0.399 | 1.846 | 0.698 | 0.323 | 0.128 | 0.811 | 0.016 | |
| Course of COVID-19 | 3 | 0.788 | 0.355 | 1.752 | 0.361 | 0.682 | 0.272 | 1.708 | 0.546 |
| 2 | 0.846 | 0.374 | 1.912 | 0.622 | 0.690 | 0.271 | 1.753 | 0.595 | |
| 1 | 1.115 | 0.507 | 2.452 | 0.290 | 0.785 | 0.318 | 1.938 | 0.971 | |
| Temperature < 36.6 | 1.593 | 0.960 | 2.643 | 0.072 | 1.478 | 0.775 | 2.821 | 0.236 | |
| Temperature < 37.5 | 1.056 | 0.655 | 1.704 | 0.822 | 1.088 | 0.601 | 1.969 | 0.779 | |
| Temperature > 37.5 | 0.772 | 0.515 | 1.159 | 0.212 | 0.782 | 0.469 | 1.302 | 0.344 | |
| Cough | 0.686 | 0.456 | 1.031 | 0.070 | 0.794 | 0.474 | 1.330 | ||
| Dyspnoea | 0.926 | 0.617 | 1.390 | 0.711 | 0.982 | 0.587 | 1.639 | 0.943 | |
| Olfactory dysfunction | 1.062 | 0.543 | 2.074 | 0.861 | 1.067 | 0.468 | 2.440 | 0.875 | |
| Taste dysfunction | 0.147 | 0.020 | 1.062 | 0.057 | 0.000 | - | - | - | |
| Smell and taste disorders | 6.788 | 3.946 | 11.678 | 0.000 | 5.885 | 2.948 | 11.746 | <0.001 | |
| Significant fatigue | 0.865 | 0.554 | 1.348 | 0.521 | 0.791 | 0.449 | 1.388 | 0.413 | |
| Chest pain | 1.101 | 0.733 | 1.653 | 0.642 | 1.203 | 0.722 | 2.003 | 0.477 | |
| Back muscle pain | 0.939 | 0.626 | 1.408 | 0.760 | 1.139 | 0.681 | 1.906 | 0.618 | |
| Leg muscle pain | 1.284 | 0.856 | 1.925 | 0.227 | 1.713 | 1.026 | 2.864 | 0.039 | |
| Headache | 1.238 | 0.819 | 1.872 | 0.312 | 1.267 | 0.736 | 2.183 | 0.392 | |
| Arthralgia | 1.553 | 1.036 | 2.330 | 0.033 | 1.884 | 1.125 | 3.151 | 0.016 | |
| Diarrhoea | 1.141 | 0.696 | 1.871 | 0.601 | 1.128 | 0.691 | 2.341 | 0.438 | |
| Vomiting | 0.575 | 0.209 | 1.587 | 0.286 | 0.822 | 0.288 | 2.358 | 0.716 | |
| Chills | 1.037 | 0.681 | 1.578 | 0.866 | 1.059 | 0.629 | 1.783 | 0.827 | |
| Labile blood pressure values | 1.135 | 0.655 | 1.965 | 0.651 | 1.146 | 0.563 | 2.331 | 0.706 | |
| Hearing dysfunction | 1.549 | 0.864 | 2.776 | 0.142 | 1.694 | 0.822 | 3.487 | 0.153 | |
| Duration of symptoms (number of days) | 0.990 | 0.947 | 1.036 | 0.676 | 0.993 | 0.948 | 1.041 | 0.768 | |
| Number of symptoms | 1.076 | 1.017 | 1.138 | 0.011 | 1.087 | 1.012 | 1.167 | 0.021 | |
| The Whole Group | Propensity Score Matching | ||||||
|---|---|---|---|---|---|---|---|
| OR | 95% CI for OR | p-Value | OR | 95% CI for OR | |||
| Lower Limit | Upper Limit | Lower Limit | Upper Limit | ||||
| Comorbidities | 0.590 | 0.384 | 0.906 | 0.016 | --- | --- | --- |
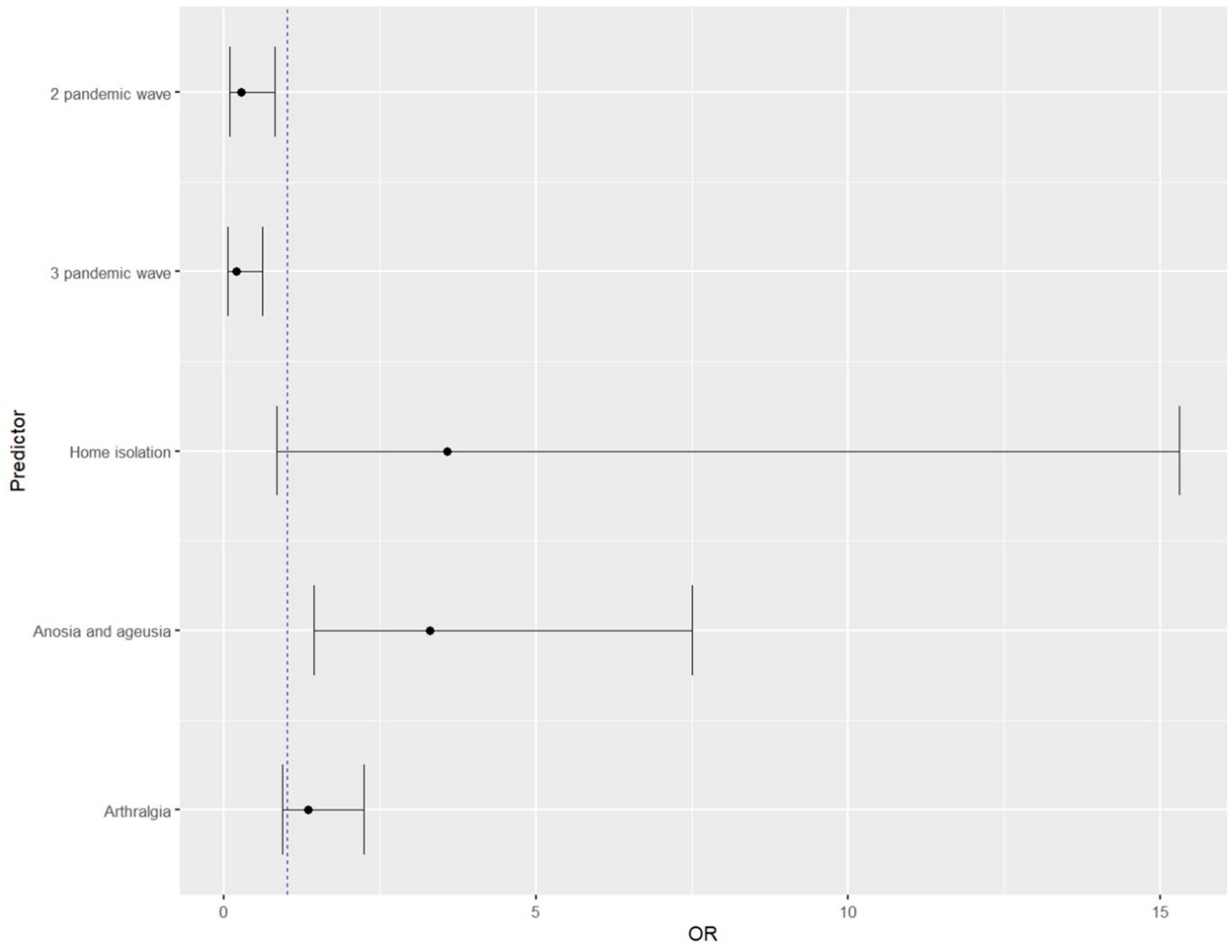
| Home isolation | 4.085 | 1.271 | 13.129 | 0.018 | 3.566 | 0.830 | 15.312 |
| Smell and taste disorders | 3.454 | 1.856 | 6.429 | 0.000 | 3.285 | 1.439 | 7.493 |
| Arthralgia | 1.519 | 0.996 | 2.318 | 0.052 | 1.341 | 0.930 | 2.231 |
| Pandemic wave 2 | --- | --- | --- | --- | 0.274 | 0.092 | 0.804 |
| Pandemic wave 3 | --- | --- | --- | --- | 0.187 | 0.057 | 0.608 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chudzik, M.; Babicki, M.; Mastalerz-Migas, A.; Kapusta, J. Persisting Smell and Taste Disorders in Patients Who Recovered from SARS-CoV-2 Virus Infection—Data from the Polish PoLoCOV-CVD Study. Viruses 2022, 14, 1763. https://doi.org/10.3390/v14081763
Chudzik M, Babicki M, Mastalerz-Migas A, Kapusta J. Persisting Smell and Taste Disorders in Patients Who Recovered from SARS-CoV-2 Virus Infection—Data from the Polish PoLoCOV-CVD Study. Viruses. 2022; 14(8):1763. https://doi.org/10.3390/v14081763
Chicago/Turabian StyleChudzik, Michał, Mateusz Babicki, Agnieszka Mastalerz-Migas, and Joanna Kapusta. 2022. "Persisting Smell and Taste Disorders in Patients Who Recovered from SARS-CoV-2 Virus Infection—Data from the Polish PoLoCOV-CVD Study" Viruses 14, no. 8: 1763. https://doi.org/10.3390/v14081763